
Abstract
Background:
Centrally inserted central venous catheters (CICCs) are commonly placed in critically ill patients who require a central venous catheter (CVC). Recently, peripherally inserted central venous catheters (PICCs) have been widely used on general wards. However, the safety of PICCs in critically ill patients remains unclear.
Method:
We conducted a retrospective observational study at a mixed intensive care unit (ICU). Adult patients (⩾18 years) who were emergently admitted to the ICU and underwent CVC insertion between April 2019 and March 2021 were enrolled. We compared the safety of PICCs and CICCs. The primary outcome was the overall rate of catheter-related complications, including bloodstream infections, thrombosis, insertional trauma, catheter malfunction, and accidental removal. We used a stabilized inverse probability weighting (sIPW) model to estimate the effects of PICC use.
Results:
A total of 239 CVCs (PICCs, 53; CICCs, 186) were inserted into 229 patients. Although the severity of illness did not differ significantly between the groups, the length of hospital stay and mean indwelling catheter duration were significantly longer in the PICC group. There was no significant intergroup difference in the overall rate of catheter-related complications (PICC: 9.4% vs CICC: 3.8%; odds ratio [OR]: 2.65; 95% confidence interval [CI]: 0.63–10.2, p = 0.145), and there were 7.7 and 9.0 complications per 1000 catheter days in the PICC and CICC groups, respectively (hazard ratio [HR]: 0.61; 95% CI: 0.14–2.65, p = 0.513). After adjustment using the sIPW model, PICC use was not found to be associated with a reduction in catheter-related complications (adjusted OR: 3.10; 95% CI: 0.90–10.7; adjusted HR: 0.53; 95% CI: 0.14–1.97).
Conclusion:
We found no significant differences in catheter-related complications between patients treated using CICCs and those treated using PICCs after emergency ICU admission. Our findings imply that PICCs may be an alternative to CICCs in critically ill patients.
Introduction
Central venous catheters (CVCs) are commonly inserted into critically ill patients to administer fluids and drugs, including sedatives, analgesics, and vasopressors. However, the use of centrally inserted central venous catheters (CICCs) is associated with serious complications (e.g. vascular injury, pneumothorax, and hemothorax), especially when the internal jugular vein or subclavian vein is punctured. 1 In addition, critically ill patients often have limited CVC puncture sites because of trauma, burns, unexposed skin surfaces (e.g. due to the wearing of a cervical collar, surgical sites being covered by a dressing), and medical devices (e.g. extracorporeal membrane oxygenation [ECMO] devices and dialysis catheters). Therefore, a greater range of CVC puncture sites would be desirable for managing these patients.
In recent years, peripherally inserted central venous catheters (PICCs) have been widely used for long-term intravenous therapy on general wards. 2 PICCs can be inserted more safely than CICCs; that is, with a lower risk of serious mechanical complications, possibly because they are used to puncture superficial veins, including the basilic vein. Thus, PICCs may also be a safer alternative to CICCs for critically ill patients.
Although, theoretically, PICC use reduces the risk of mechanical complications during insertion, the risk of other complications associated with CVCs also needs to be assessed. A retrospective study conducted in a medical intensive care unit (ICU) found no differences in the rates of infection or thrombosis between patients treated with PICCs and those treated with CICCs. However, there were differences in the severity of illness between the two groups, making it difficult to generalize these findings to all patients. 3 It remains unclear whether PICC use would decrease the overall rate of catheter-related complications, including infections and thrombosis, among critically ill patients.
Based on current evidence, clinical practice guidelines cannot make suggestions regarding the use of PICCs in critically ill patients.4,5 The aim of this study was to investigate whether the use of PICCs rather than CICCs in critically ill patients decreases the risk of catheter-related complications.
Method
Trial design and setting
This was a retrospective observational study conducted in a mixed ICU in Japan. This study was approved by the ethics committee of the JA Hiroshima General Hospital.
We collected data from medical records and included adult patients (⩾18 years) who were emergently admitted to the ICU and underwent CVC insertion between April 2019 and March 2021. Patients who underwent scheduled ICU admission (e.g. for elective cardiac surgery) were excluded. Patients in whom CVCs were inserted prior to their ICU admission or more than 24 h after their ICU admission were also excluded. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement. 6
Catheter type and insertion technique
We inserted the CICCs (Covidien Japan, Tokyo; SMAC™ plus, triple lumen, outer diameter: 2.5 mm) and PICCs (BD Japan, Osaka; Power PICC®, 4 Fr double lumen) with maximal barrier precautions and under real-time ultrasound guidance at the bedside. During cannulation, the basilic or brachial vein was selected for PICC insertion, and the internal jugular, subclavian, or femoral vein was selected for CICC insertion. We used 1.0% alcohol/chlorhexidine gluconate solution with 79% ethanol as an antiseptic for skin disinfection. The final tip position was confirmed on a bedside chest X-ray.
Both PICCs and CICCs were inserted by the attending physician or a resident. In each case, the type of CVC used and punctured vein were decided by the attending physician.
Data collection and outcomes
We collected data regarding the following factors: age, sex, body mass index (BMI), severity of illness (the Acute Physiology and Chronic Health Evaluation III [APACHE III] score 7 and Sequential Organ Failure Assessment [SOFA] score), 8 the updated Charlson Comorbidity Index (CCI), 9 indwelling catheter duration, length of ICU stay, length of hospitalization, and in-hospital mortality. All CVCs were followed until they were removed, the timing of which was decided by the treating physicians. The primary outcome was the rate of catheter-related complications, which were defined as the occurrence of one or more of the following: a central line-associated bloodstream infection (CLABSI), which was defined using the Centers for Disease Control and National Healthcare Safety Network reporting definitions 10 ; catheter-related deep vein thrombosis (CRDVT), which was defined as the presence of clinical findings such as swelling or pain in the upper extremities and the presence of upper extremity deep venous thrombosis (DVT), as determined by venous duplex ultrasonography (ultrasonographic studies for CRDVT were only performed in symptomatic patients); insertional trauma, including pneumothorax, hemothorax, and arterial puncture, which was defined as any such condition that required a surgical procedure (e.g. chest drainage or vascular repair); a catheter malfunction, which was defined as when a catheter did not allow adequate blood flow; and accidental removal, which was defined as unscheduled CVC removal.
Statistical analysis
Data are expressed as medians with interquartile ranges or absolute values with corresponding percentages, as appropriate. Baseline characteristics were compared between the CICC and PICC groups. Continuous variables were compared using the Student’s t-test or Mann‒Whitney U test, according to the data distribution. Dichotomous variables were analyzed using Fisher’s exact test. We also applied stabilized inverse probability weighting (sIPW) to calculate adjusted odds ratios (ORs), adjusted hazard ratios (HRs), and 95% confidence intervals (CIs) for the patients in the PICC group relative to those in the CICC group for the primary outcome. Covariables that were expected to be associated with disease severity in ICU patients (i.e. age, sex, BMI, the updated CCI, the SOFA score, the APACHE III score, and ICU stay length) were included in the sIPW models.
Logistic regression analysis and Cox proportional hazards regression analysis were performed to estimate the effect of PICC use on the overall rate of catheter-related complications. We defined death before CVC removal as a competing event. All statistical tests were two-sided, and p-values of <0.05 were defined as indicating statistical significance.
All statistical analyses were performed with EZR (version 1.55; Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (version 4.1.2; The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R Commander (version 2.7-1) designed to add statistical functions that are frequently used in biostatistics. 11
Results
During the 2-year study period, a total of 239 CVCs were inserted into 229 patients (10 patients had two eligible CVCs inserted; Figure 1). Overall, 53 (22.2%) were PICCs, and 186 (77.8%) were CICCs. The basic clinical characteristics of these patients are shown in Table 1. One hundred and fifty-seven patients (65.7%) were male, and the median age of the patients was 72 years (interquartile range [IQR]: 64–81). There were no significant differences between the PICC and CICC groups with regard to age, sex, BMI, the updated CCI, the SOFA score, the APACHE III score, ICU stay length, or in-hospital mortality (Table 1). However, the PICC group had a longer median hospital stay (32.0 vs 26.0 days; p = 0.042) and a longer median indwelling catheter duration (9.0 vs 3.0 days; p < 0.001) than the CICC group.
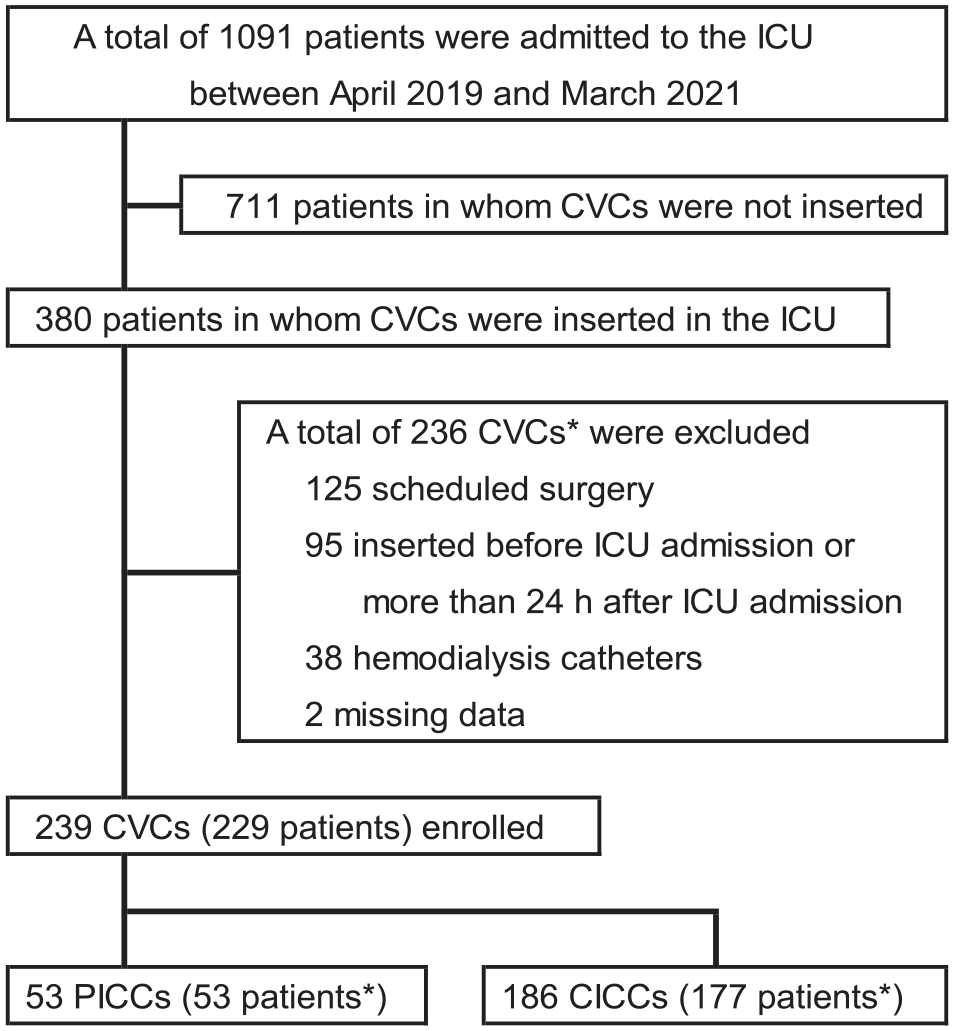
Flow chart of patient selection.
Characteristics of the two groups.
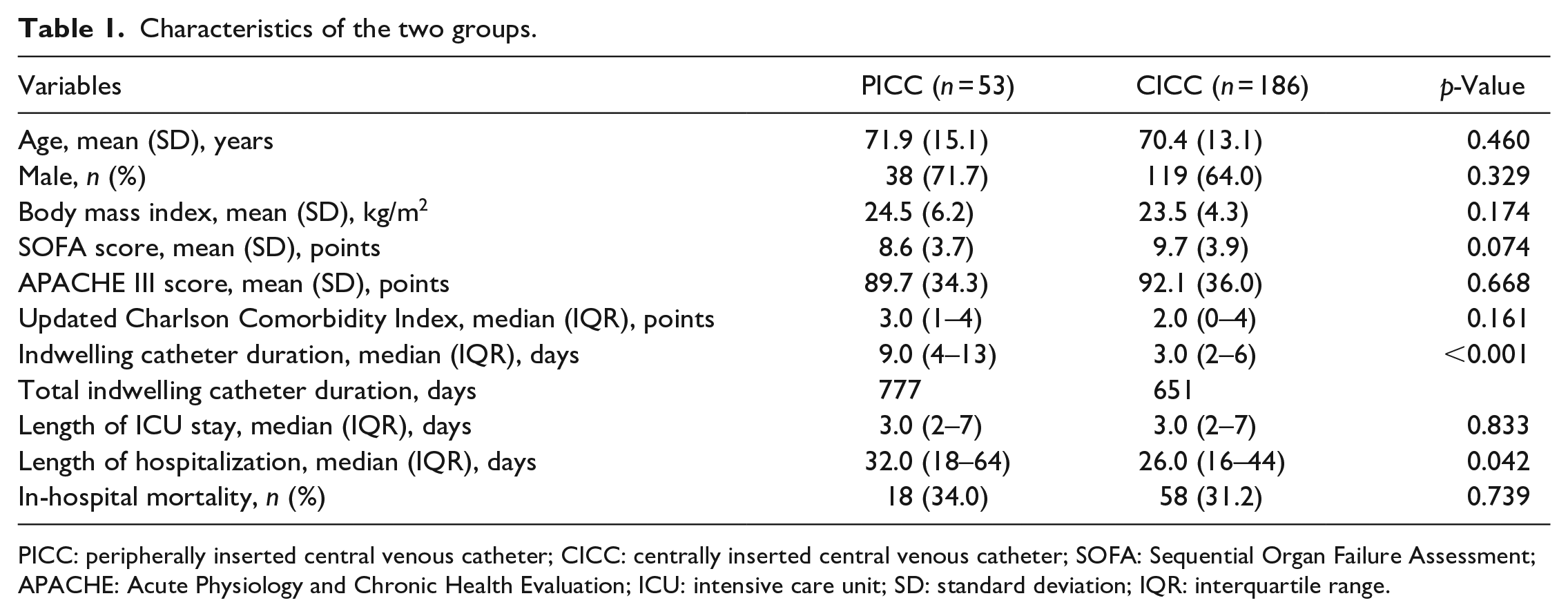
PICC: peripherally inserted central venous catheter; CICC: centrally inserted central venous catheter; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation; ICU: intensive care unit; SD: standard deviation; IQR: interquartile range.
There were 12 catheter-related complications (5.0%; Table 2). There was no significant intergroup difference in the overall rate of catheter-related complications (PICC: 5 (9.4%) vs CICC: 7 (3.8%), OR: 2.65 [95% CI: 0.63–10.2], p = 0.145), and there were 7.7 and 9.0 complications per 1000 catheter days in the PICC and CICC groups, respectively (HR: 0.61 [95% CI: 0.14–2.65], p = 0.513).
Primary outcomes of patients in the PICC and CICC groups.
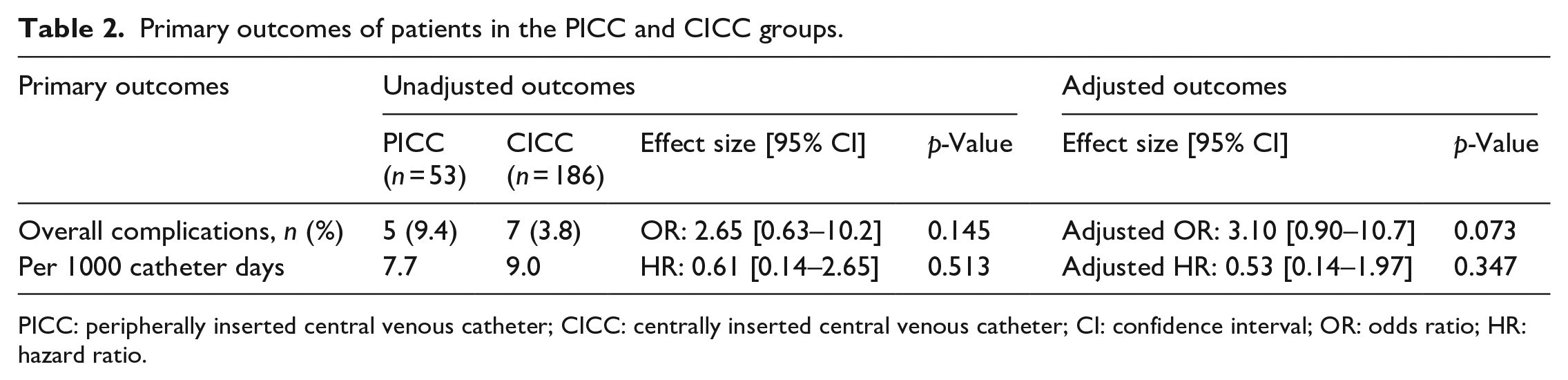
PICC: peripherally inserted central venous catheter; CICC: centrally inserted central venous catheter; CI: confidence interval; OR: odds ratio; HR: hazard ratio.
sIPW was performed, resulting in there being 49.4 patients in the PICC group and 168.8 patients in the CICC group. After adjustments were made using the sIPW model, the standardized difference was less than 10% for all variables, indicating that the two groups were generally well balanced (Table 3). The adjusted OR for the PICC group compared with the CICC group was 3.10 [95% CI: 0.90–10.7], and the adjusted HR was 0.53 [95% CI: 0.14–1.97] (Table 2).
Baseline characteristics of the two groups before and after sIPW.
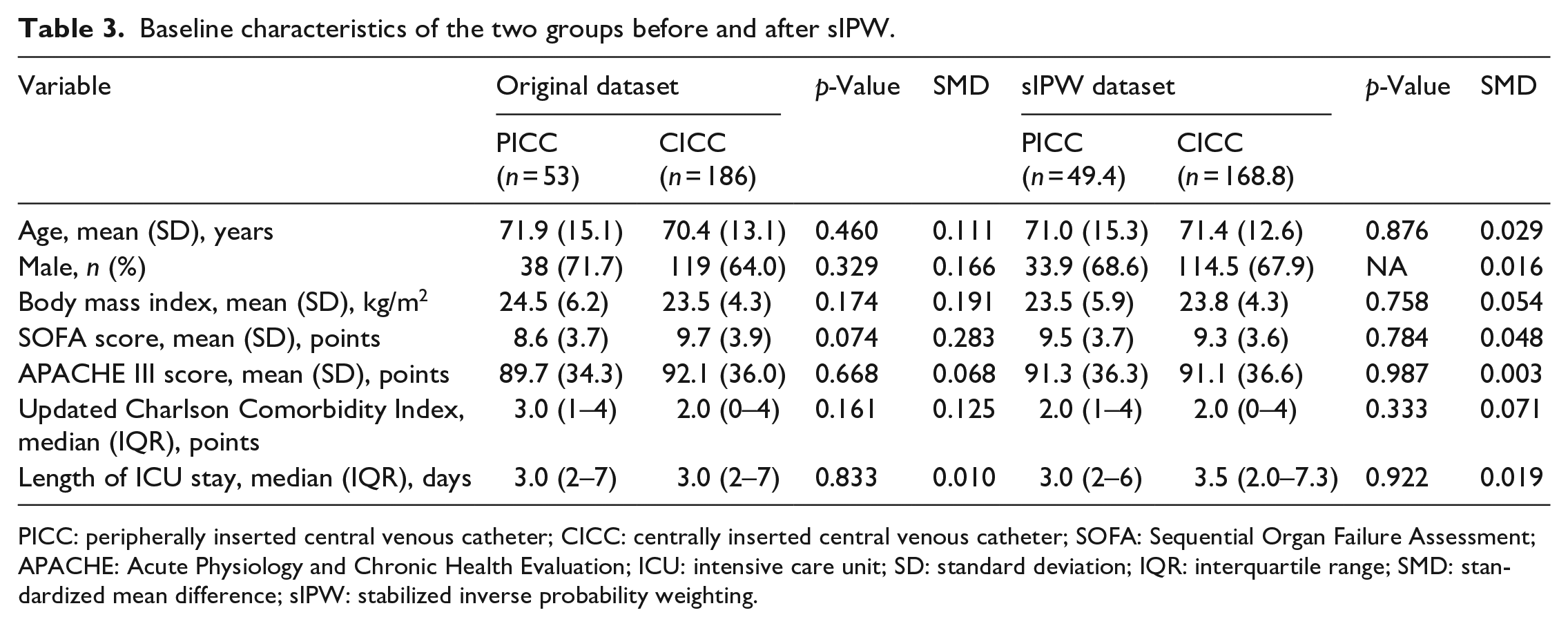
PICC: peripherally inserted central venous catheter; CICC: centrally inserted central venous catheter; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation; ICU: intensive care unit; SD: standard deviation; IQR: interquartile range; SMD: standardized mean difference; sIPW: stabilized inverse probability weighting.
Catheter malfunction only occurred in the PICC group (two patients). In both cases, the cause was catheter obstruction, and the PICCs were promptly removed. There were no significant differences between the two groups in the rates of any of the examined complications: CLABSI (PICC: two patients; CICC: one patient); accidental removal (PICC: one patient; CICC: six patients). There were no cases of air emboli associated with accidental removal. None of the patients in either group experienced CRDVT or insertional trauma. Further details of the complications are presented in Table 4.
Details of the catheter-related complications.
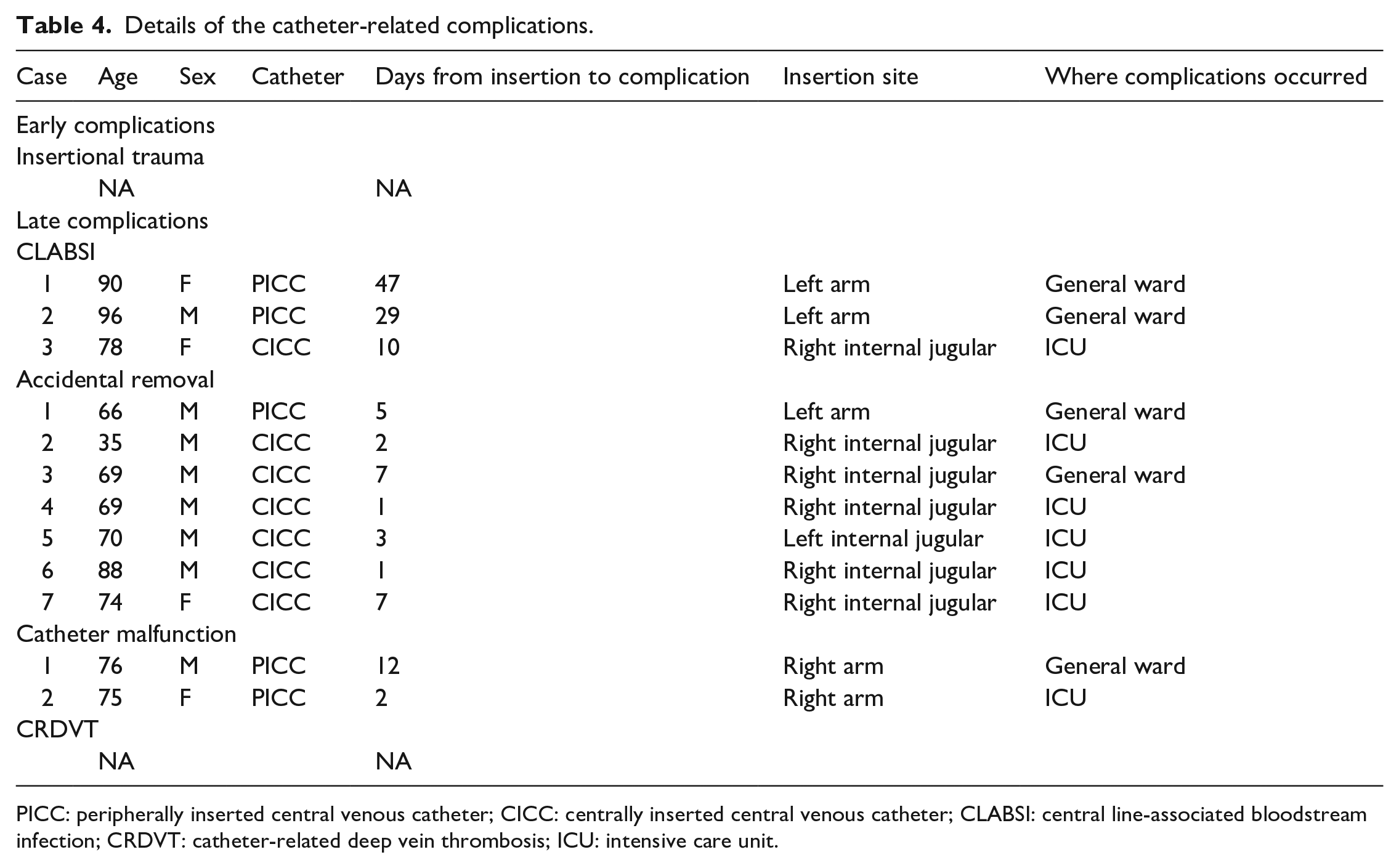
PICC: peripherally inserted central venous catheter; CICC: centrally inserted central venous catheter; CLABSI: central line-associated bloodstream infection; CRDVT: catheter-related deep vein thrombosis; ICU: intensive care unit.
Discussion
We included all CVCs that were inserted after an emergent ICU admission during the study period and compared the patients who had PICCs inserted with those who had CICCs inserted using sIPW models. There were no differences in patient characteristics that could be related to the severity of illness, but both the length of the hospital stay and the indwelling catheter duration were significantly longer in the PICC group than in the CICC group. Nevertheless, there was no significant difference in the overall rate of catheter-related complications between the PICC and CICC groups after adjustments were made using sIPW, which indicated that the prespecified covariables were well balanced.
Previous studies about PICCs have mainly focused on general ward patients and outpatients, with only a minority of studies involving ICU patients. In addition, the studies that did examine critically ill patients had some limitations, such as regarding the type of ICU or the severity of illness. It has been suggested that PICCs can be used as an alternative to CICCs among critically ill patients, 12 although this suggestion was only supported by evidence with low certainty. A randomized controlled trial conducted in a neurointensive care unit demonstrated that there was no difference in the number of cases of any complication between the PICC and CICC groups. 13 However, the patients in the latter study may have been experiencing consciousness deficits, paralysis, and/or indications or contraindications for anticoagulation therapy, which may have affected the prevalence of complications. In a retrospective study of medical ICU patients, there was no significant difference in the rate of CLABSI or CRDVT between the PICC and CICC groups. 3 However, significant differences in disease severity and the indwelling catheter duration were observed between the two groups, and mechanical complications, such as insertional trauma, were not examined. Thus, there are several concerns about the generalizability of the findings of these studies to critically ill patients. Our study, which was performed in a mixed ICU and adjusted for the severity of illness, solves these limitations, and its findings are highly likely to be generalizable to critically ill patients.
The guidelines recommend avoiding PICCs in ICU patients to reduce the risk of CLABSI, based on the finding that both PICC and CICC use are associated with a similar risk of CLABSI in hospitalized patients. 5 However, another study found that most cases of CLABSI occurred after ICU discharge. 14 A longer indwelling catheter duration may increase the risk of complications such as infections and thrombosis. 1 In our study, PICCs were kept in place for longer than CICCs, despite the patients in these groups having diseases of similar severity. Furthermore, the ORs for complications in the PICC group tended to be higher, while the HRs were lower, than those seen in the CICC group. These findings imply that a longer indwelling catheter duration may increase the risk of complications associated with PICCs, resulting in the risk of such complications being higher for PICCs than for CICCs, even if the complications risk is generally considered to be lower in patients treated with PICCs. Prospective studies with standardized CVC removal criteria are warranted to compare these two types of catheters.
There was a trend toward a higher frequency of accidental removal in the CICC group than in the PICC group, although this difference was not significant, possibly because of the small number of these events (Table 4). Lorente et al. 15 reported that there were no significant differences in the incidence of accidental catheter removal between four central venous access sites (peripheral, jugular, subclavian, and femoral), but suggested that the insertion of CVCs into the internal jugular vein may be associated with higher risk. In our study, accidental removal also tended to occur more frequently after internal jugular placement and less frequently after placement in the peripheral veins. Notably, most of the accidental removals occurred in the ICU. PICCs may be chosen for critically ill patients who are at a higher risk of accidental removal, since the interruption of drug administration is associated with serious adverse events in such patients. Furthermore, PICC use is associated with a low risk of air embolization, even after accidental removal.
Our study demonstrated that the overall rate of catheter-related complications did not differ between the PICC and CICC groups. The main advantage of PICCs is that they are associated with a lower risk of complications during insertion. Since some critically ill patients have coagulopathy or receive anticoagulation therapy, PICCs may be a safer alternative for such patients. However, the insertion technique used for PICCs may be more difficult than that used for CICCs because PICCs are inserted into smaller target veins. A longer CVC insertion procedure may lead to the delayed administration of medication. However, it was recommended that vasopressors can be administered peripherally for rapid initiation, 16 and most drugs can also be administered through a peripheral vein for short periods of time. A retrospective cohort study of septic shock patients in an ICU showed that the vascular access team were able to insert PICCs more quickly than CICCs for initial resuscitation. 17 In addition, obesity and critical illness may not be associated with the duration of the PICC insertion procedure. 18 PICC insertions performed using appropriate techniques may not take longer than CICC insertions. Thus, the duration of the PICC insertion procedure may not have a significant clinical impact, even during the resuscitation of patients in shock. In addition, when appropriate insertion techniques were employed PICC use was found to be associated with a low risk of thrombosis and CLABSI.12,19 Thus, it may be preferable to use PICCs rather than CICCs in critically ill patients.
Our study had several limitations. First, the inferences that could be drawn from our findings were limited by the small sample size and the uncontrolled bias introduced by the retrospective nature of the study. Although the patients were not randomized to the groups, and the type of CVC used was decided by the attending physician, the updated CCI, SOFA score, and APACHE III score did not differ between the groups. In addition, we did not find any significant differences after performing adjustments using sIPW. However, due to the small sample size we could not show that CICCs and PICCs are associated with equivalent risks of catheter-related complications. To verify our findings, larger multi-center prospective studies are warranted. Second, we could not collect asymptomatic DVT cases retrospectively. Previous studies demonstrated that PICC use was associated with an increased risk of upper extremity DVT, especially in ICU patients. 20 If we had screened all of the patients for upper extremity DVT, we may have found an increased number of DVT cases. However, pulmonary emboli due to upper extremity DVT occurred less frequently than pulmonary emboli due to lower extremity DVT. 21 In addition, it was reported that asymptomatic CVC-related thrombosis does not require treatment. 22 Therefore, a potential increase in the risk of asymptomatic upper extremity DVT may not be a crucial issue, and the lack of data on asymptomatic DVT may not be a serious limitation. Finally, we must mention procedural limitations. PICC is not suitable for intravenous fluid resuscitation due to its high flow resistance. Therefore, during resuscitation, we resolved the problem administering large volumes of fluid via peripheral venous access and vasopressors via PICC. We mainly checked the positions of the catheter tips using bedside X-rays obtained after the procedure, although recent guidelines recommend intra-procedural confirmation (e.g. echocardiography and intracavitary electrocardiography). 23 However, no complications due to catheter tip position were observed in this study. We are used to inserting PICCs and encountered few technical or psychological barriers to PICC insertion, even in emergency situations. Since the use of PICCs in critically ill patients is not as widespread as the use of CICCs in such patients, the generalizability of our findings is unclear.
Conclusion
We found no significant differences in the rate of catheter-related complications between patients that underwent CICC insertion and those that underwent PICC insertion after emergency ICU admission. Our findings imply that PICCs are a suitable alternative to CICCs in critically ill patients. Further interventional research is warranted to provide more robust findings.
Footnotes
Author contributions
TM designed the study, acquired the data, performed the statistical analyses, and interpreted the data. MS interpreted the data, advised on the statistical analyses, and edited the manuscript. KY reviewed and edited the study. The first draft of the manuscript was written by TM, and all of the authors commented on previous versions of the manuscript. All of the authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the ethics committee of the JA Hiroshima General Hospital (No 21-42). The requirement for informed consent was waived, and an opt-out recruitment method was employed.
Guarantor
MS.