To Compare the Safety and Outcomes of Ultrasound Guided Tunneled Dialysis Catheters Insertions with Or Without Flouroscopy
Konnepati Sushma, Manish Rathi, Jasmine sethi, Anupam lal, Raja Ramachachandran
PGIMER, Chandigarh
Introduction: Imaging guided tunneled dialyses catheter insertion is better than traditional landmark method due to fewer complications. Ultrasound guided insertion is safe and preferred method as proven by previous studies. However, there is a paucity of data regarding comprehensive outcomes in USG guided insertion with and without fluoroscopy.
Methods & Results: This is a single center RCT done in a tertiary hospital in North India. 149 were enrolled, 87 were randomized into Ultrasound guided insertion without fluoroscopy (Group A), and 62 were randomized into Ultrasound guided insertion with fluoroscopy (Group B). Outcomes were analyzed at baseline and at 1-month follow-up. However, the procedure time was the only significant result, which was less in the USG guided group with a significant p-value of 0.007.
Conclusion and Discussion: Our study is a RCT done in a tertiary care centre in north India, we compared complications of USG guided TDC insertion done with and without fluoroscopy. The primary outcome of our study was the successful placement of TDC, which was 100% in both groups. The parameters like the number of attempts for successful catheter placement, mean procedure time, and Ease of catheter insertion were compared between both groups, which is unique, and we believe this was a distinct contribution. Catheter-related infection was the most common complication overall reported in 14 participants (9.4 %), 11 from group A and three from group B, followed by hematoma formation(8.4%), and catheter slippage(3.4%) The mean procedure time was 41.26 minutes (SD 11.8) in group A, ranging from 15 to 75 minutes, and it was 47.74 minutes (SD 17.2) in group B ranging from 20 to 105 minutes. By applying the t-test(2-tailed), the p-value was 0.007 (<0.05), which was statistically significant. In group B, additional fluoroscopy use was time consuming attributed to aligning the participant in the correct position for better Imaging. Our study concluded that fluoroscopy has no additional advantage in reducing mechanical, infective, or thrombotic complications.
Snuff-box arteriovenous fistula creation by nephrologist as first-line access for hemodialysis initiation
Tauhidul Alam Choudhury, Abhishek Debnath
Dispur Hospitals, Guwahati, India
Introduction: The snuff-box arteriovenous fistula (SBAVF) is the most distal native vascular access. It provides a long segment of needling vessels and spares the proximal vessels for future use. We share our experience of snuff-box AVFs created by nephrologists for hemodialy- sis initiation in end-stage kidney disease.
Methods & Results: This prospective observational study evaluated 17 snuff-box AVFs created by a nephrologist for hemodialysis initiation with follow-up for three months or until maturation for six months from a single center in Nort East India. We included patients with suitable venous and arterial conditions on physical examinations. We excluded patients with abnormal anatomy and unsuitable venous or arterial conditions for AVF. The mean age was 45.94+12.10 years, with male to female ratio of 13:4. Two patients expired during the study period, one on day seven and another on day 30. Diabetes was present in 8(47%) patients, and hypertension was present in all patients. Type of anastomosis: End-to-side anastomosis in 5(29.5%) and side-to-side in12(70.5%) patients. We observed immediate patency in 17 (100%) and maturation in 15 (88.2%) patients.
Conclusion and Discussion: The advantages of SBAVF are that It provides a long segment of a vessel for needling and spares the proximal vessels for future use. The ability to effectively convert to wrist fistula in the event of snuff-box arteriovenous fistula failure provides longevity to native hemodialysis access [1].However, SBAVF is a technically challenging procedure and has higher probability of failure than other sites such as cubital [1]. The maturation of SBAVF varies from 50% up to 92% in the reported literature. The present study showed a maturation of 88.2%, comparable to other studies [2,3]. Vernekar RR et al. [3] from India reported successful SBAVF maturation of 92% in an observational study of 35 SBAVF (side-to-side anastomosis). A prospective cohort study [4] of 78 AVFs from Iran observed a maturation of 61%. They found no difference in maturation and patency between SBAVF and wrist AVFs. In a retrospective study [5] of 47 distal AVFs, the maturation failure was 47.2% for SBAVF and 50% for Wrist AVFs. Early complications of SBAVF is post-operative bleeding (3%) and thrombosis (3%) [1]. We avoided such complications as we had a small number of cases. The study’s drawbacks are a small number of patients and short follow-up. Conclusion: Snuff-box arteriovenous fistula is a good and valid option for first-line hemodialysis access in well-selected cases. The rate of successful maturation of SBAVF created by a nephrologist in our center is 88.2%.
References
1. Idrees M, Suthananthan A, Pathmarajah T, Sieunarine K. Snuffbox fistula - a first-line approach to haemodialysis: A review. J Vasc Access. 2020 Sep;21(5):554-563. doi: 10.1177/1129729819867817. Epub,
2. Ezelsoy M,Hasde A,Aslan M,Mavi M,Evaluation of Snuff-Box Arteriovenous Fistulas in Hemodialysis Patients .Turk J Vasc Surg 2015;24(1):013-017
3. Ritesh R. Vernekar 1, Vikram Prabha 2, * and Shashank D. PatilVascular Factors Affecting Outcomes of Snuffbox AV Fistula with Side-to-Side Anastomosis: A Single Institutional Observational Study:Nep
4. Iraj Nazari, Hossein Tajali, Saeedeh Majidi, Marjan Joudi, Farzaneh Pouya, Shiva Ghaderifar, Zahra Abbasi; Patency and Efficacy of Anatomical Snuffbox Arteriovenous Fistula Compared with Wrist Fistu5.Mokhtari S, Besancenot A, Beaumont M, Leroux F, Rinckenbach S, Salomon Du Mont L. Snuff-Box Versus Wrist Radiocephalic Arteriovenous Fistulas for Hemodial- ysis: Maturation Tend and its Affecting Fact,
AVF EXPERIENCE – Patient’s perspective
Sayli Prakash Jadhav, Jason Samuel, Neetu Dubey
Apex Kidney Care, Delhi
Introduction: Pain during cannulation of AVF is an inevitable sensation of every patient on HD treatment. Due to the complexity of this phenomenon, pain is the object of many multidisciplinary studies on the nature of pain.
Objectives: To measure intensity of pain during AVF cannulation as precisely as possible Encouraging conversation about fears and problems which they have related to AVF in order to improve healthcare, provide psychological support to patients and improve the environment for teamwork
Methods: The patients were delighted to take part in the survey. In order to get a true image of how they felt throughout the AVF cannulation, questions were created. We also asked patients if seeing the AVF during cannulation bothered them in any way or had an effect on their quality of life, in addition to just their impression of it. We used the Linkert’s scale and the pain scale to get the most accurate measurement possible.
Results: The survey included 100 patients, 44% female and 56% male with an average age of 52 years. The survey did not include patients with CVK. AVF was present in 96.5% of patients while only 3.5% have AVG. The average age of vascular access is 5 years. 16 patients use a local anesthetic.
Conclusion: According to the findings, it would be preferable to apply local anaesthetic on small patient groups. Additionally, it would be preferable to alter the technique of cannulation with ongoing cannulation changes in order to minimize the visibility of aneurysms, which negatively affects patients’ confidence. Any interchange of information relevant to a nursing patient is one step towards preventing and lowering issues. The survey, good communication, and empathy for patient problems all helped us increase cooperation and interpersonal relationships.
Acknowledgement
I am thankful to Sudhir Bagarao sir, for their expertise and assistance in statistical work. I would also want to thank Apex Kidney Care-ASDT.
References
1. Crespo R.Influence of bevel position of the needle on puncture pain in haemodialysis. J Eur Dial Transpl Nurs Assoc 1994; 4:21
2. Bali LK.(2005)Improving arteriovenous fistula cannulation skills. Nephrol Nurs J 32(6), 611 617, Ryner HC, Pisoni RL, Gillespie BW. Creation, cannulation and survival of arteriovenous fistulae: data from DOPPS. Kidney Int 2 00 3;63:323.
Successful thrombolysis of Arterio-Venous Graft (AVG) using r-TPA – A Case Report
Kamlesh Parikh, Ashwin Bhammar
MGM Medical college and Hospital Aurangabad
Introduction: A functioning vascular access is essential for effective delivery of hemodialysis and, understandably, lack of vascular access or complications developing in an existing vascular access are associated with significant patient morbidity. Thrombosis is one of the most common complications associated with autologous arteriovenous fistula (AVF) & AV graft for hemodialysis and often results in failure of AVF. Here we report, salvage of a thrombosed graft using early thrombolytic therapy (TT).
Methods & Results: 63-year-old, k/c/o diabetes mellitus developed ESRD in march 2020 Multiple AV fistula failure, blood stream infectious with perm cath, right internal jugular vein stenosis Surgeons attempted brachial artery to axillary vein graft twice, which eventually got occluded Left subclavian artery to subclavian vein NECKLACE graft done in 2022 with good blood flow and normal venous pressure. Patient went to native place in May,2023 and came with occluded graft. Thrombectomy attempted in OT successfully, on post operative day 1 – absent flow in graft. r-TPA given for 24 hours to patient, resulted in good flow. Venous stenosis later on dilated with drug eluting balloon.
Conclusion and Discussion: Vascular access is the “Achilles heel” of hemodialysis and absence or loss of vascular access is often associated with significant morbidity and mortality. Thrombosis is usually the consequence of some sort of anatomic abnormality, like stenosis, in the proximal venous segment; problems with the arterial segment account for only about 17% of AVF thrombosis, but systemic abnormalities in hemostasis like protein C and S deficiency, factor V Leiden, antiphospholipid antibodies, etc., may also contribute. For best results, treatment of thrombosis should start as early as possible. Delay in instituting treatment may result in extension of the thrombus, making subsequent intervention or surgical procedures more difficult and less successful. Delay in treating the thrombus also allows a longer period of contact between the thrombus and the vessel wall, making subsequent extraction of thrombus more traumatic to the vessel wall, which in turn could predispose to thrombotic events in the future. Most importantly, early resolution of the thrombo- sis may allow uninterrupted use of the same AVF for dialysis, avoiding intercurrent use of a venous catheter and attendant morbidity, like in our case. Treatment options available for thrombosed graft are: (1) percutaneous intervention with thrombectomy and angioplasty of any stenosis detected; (2) surgical thrombectomy; (3) declotting by mechanical techniques (dilatation and aspiration); (4) TT; and (5) combined mechanical declotting and TT. Only tPA is FDA approved for treatment of thrombosis in hemodialysis catheters (not AVF) in the. The available literature on the use of tPA reported a short-term patency of 90% or even more.Based on this, we felt that tPA probably offered better chances of success and decided to employ it in our case.
References
1. Hymohd J,shalansky K- efficacy of low dose alteplase for treatment of hemodialysis catheter occlusion- vascular access 2005:6, 76-82
2. Elyrich H, Walton T- alteplase versus urokinase in restoring blood flow in hemodialysis catheter thrombosis- Am J health syst pharm 2002; 54, 1437-1440,
3. Tissue plasminogen activator administration on patency of hemodialysis access cath- eter- ASKD 2000, 36,75-79,
Unusual complication of tunneled femoral hemodialysis catheter Vascular Access
Kshitija Girish Gadekar, Prashant Udgire, Saif Zil Kibriya, Rahul Tengse
MGM Medical college and Hospital Aurangabad
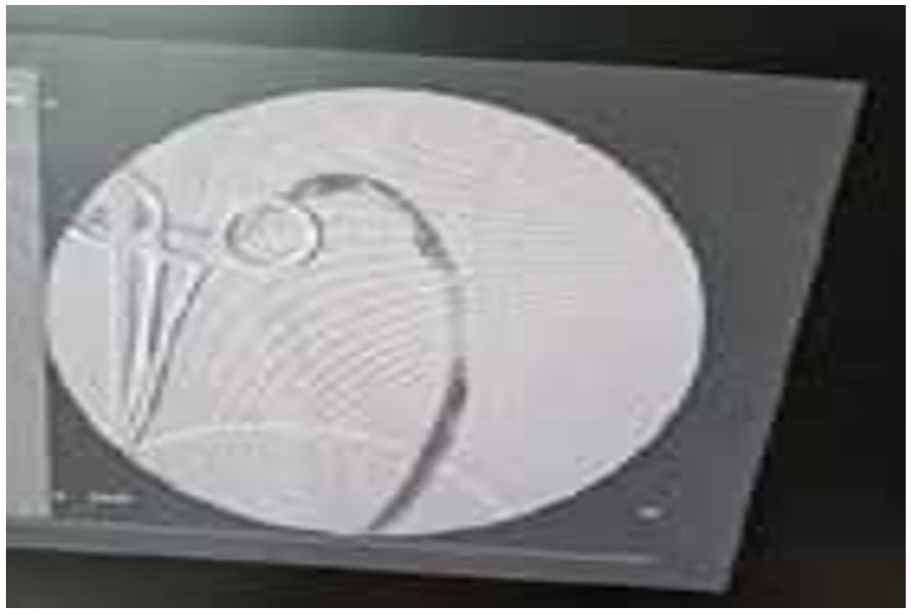
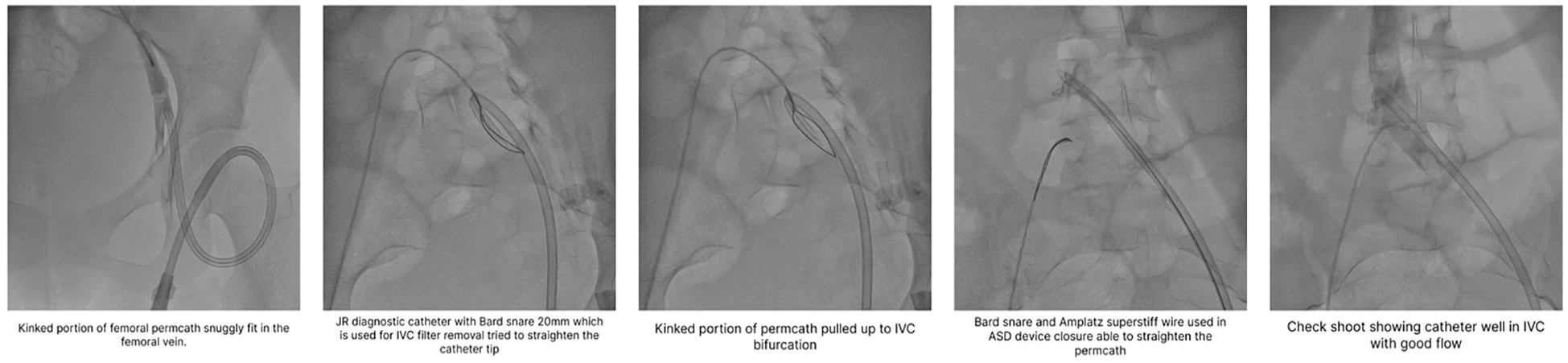
Introduction: This abstract presents an unusual case of an 18 years old young girl with ESRD due to lupus Nephritis, undergoing a tunneled femoral hemodialysis catheter insertion, where the catheter tip kinked during the procedure. The subsequent successful management of this complication is described.
Methods & Results: A tunneled femoral hemodialysis was chosen as the preferred access option due to limited vascular access alternatives. However, during the catheter insertion procedure, an unforeseen complication occurred when the catheter tip kinked and folded back on itself compromising its functionality and impeding successful catheterization.
Conclusion and Discussion: The catheter snuggly fit in the left femoral vein and was not unfolding even on withdrawing the catheter. Through the push-pull technique, a kinked portion of the permacath was pushed up to IVC bifurcation. Using a JR diagnostic catheter and Bard snare 20 mm used for IVC filter removal were used to straighten the tip which was unsuccessful. Then with the help of snare and Amplatz super stiff wire used in ASD device closure, the catheter tip was straightened well into the IVC, and flow was achieved. The successful resolution of this atypical complication highlights the importance of a multidisciplinary approach, technical expertise, and collab- oration between various medical specialties in managing complex catheter-related complications.
Acknowledgement
I express my sincere gratitude to Dr. Prashant Udgire (Interventional Cardiologist) and the entire team of Cath lab for their invaluable contribution.
Use of SǪ53 – “A Novel Biocide” in prevention of CLABSI Vascular Access
Shalini Priya, G Gireesh Reddy
Institute of Nephro-Urology, Bangalore
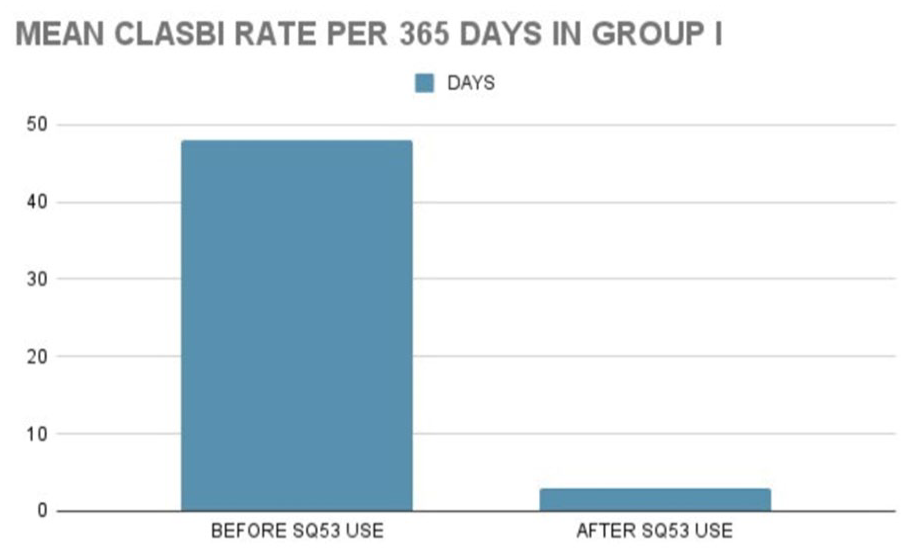
Introduction: CLABSI is the most frequent complication encountered in health care management of hemodialysis patients. SǪ53, a biocidal antimicrobial solution, is a novel therapeutic directed towards prevention of same. This study aims at calculating the reduction in rate of CLABSI per 365 catheter days after SǪ53 use.
Methods & Results: 146 patients were recruited in few multispecialty hospitals, requiring long term as well as short to medium term CVC. SǪ53 impregnated wipes were used initially during CVC insertion and subsequently for cleaning the catheter site and hubs every third day. The rate of CLABSI is per 365 catheter days after the use of SǪ53 was significantly low. SǪ53 was well tolerated by all patients. There was no incidence of skin irritation or hypersensitivity.
Conclusion and Discussion: The incidence of dialysis-related CLASBI is reported to be 2.5-5.5 cases per 1000 catheter days, or 0.9-2.0 episodes per patient-year. The risk of bacteremia is highest in haemodialysis patients using a CVC for vascular access, and increases in a linear fashion with the duration of catheter use. The 2 predominating sources of infection are believed to be extraluminal (from the skin during and following insertion) and intraluminal (from contaminated infusates or contaminated catheter hubs). The extra luminal source is the main port of entry of infections in India due to the higher bioburden in the environment as well as the lack of understanding about the precautions to be adhered to during line handling. Recommendations regarding the use of chlorhexidine gluconate (CHG) for skin preparation prior to insertion and in dressings/ sponges placed at the insertion site or as part of the dressing have largely successfully addressed the extraluminal source. Alcohol wipes have limited time of action. use of SǪ53, a novel, patented biocide antimicrobial solution is an adjunct to standard insertion and cleaning regimens. It is the only biocide driven antimicrobial available in the form of impregnated sterile packed wipes and ease of application of SǪ53 adds to the adherence rates.
References
1. Lee H, Manns B, Taub K, et al. Cost analysis of ongoing care of patients with end-stage renal
2. disease: The impact of dialysis modality and dialysis access. Am J Kidney Dis. 2002; 40:611-22
3. Marschall J, Mermel LA, Classen D et al. Strategies to prevent central line associated bloodstream infections in acute care hospitals. Infect Control Hosp Epidemiol. 2008; 29: S22-30
4. Cicaline S, Palmieri F, Petrosillo N. Clinical review: new technologies for prevention of intravascular catheter related infection. Crit Care. 2004; 8:157-62.
5. Garland JS, Buck RK, Maloney P, Durkin DM, Toth-Llyod S, Duffy M et al: Comparison of 10% povidone-iodine and 0.5% chlorhexidine gluconate for the prevention of peripheral intravenous catheter colon
Two Success Stories of Nephrologist As A 3600 Access Care Provider (Planning Creation, Surveillance And Vascular Access
Keerthi Krishnan, Sreedhara C G, Kishan A, Gireesh Reddy, Leelavathi, Mythri S
Institute of Nephro-Urology, Bangalore
Introduction: A good vascular access is often referred as a lifeline for a dialysis dependent patient. Here we present two case scenarios to highlight the role of Interventional Nephrologist in planning access creation, surveillance & salvage of Arteriovenous Fistula (AVF) so that patient inconvenience & high health care burden could be reduced.
Methods & Results: In the first case a 17-year-old boy with ESRD was referred to Vascular surgeon for AVF creation and he created Brachial-Cephalic AVF. Post three months of AVF creation patient developed mega fistula secondary to cephalic arch stenosis and also aneurysmal dilatations over AVF. Patient subsequently developed high output cardiac failure. At this point Nephrologist planned and created a radio cephalic fistula on the left forearm through which HD was successfully initiated.
Second case is of a 45-year-old male patient with ESRD caused by NSIAD abuse. Left radio cephalic fistula was attempted by surgeon but resulted in primary failure of the fistula. His Cephalic and Basilic venous system was deemed unfit for access creation. Then AVF creation was planned on right side but deferred as vascular mapping revealed heavily calcified artery in spite of patent veins. At this point interventional nephrologist anastomosed medial cubital vein with brachial artery on left so that patient would develop both cephalic and basilic venous outflows ensuring more vascular access options available in future and also reduced chances of high flow fistula due to distributed flow into the two veins. A successful AVF was later created but it developed a thrombus within 30 days. As the thrombus was of acute origin it was compressible and Nephrologist planned an endovascular procedure. Fistulogram revealed critical stenosis with decreased flows across the distal venous outflow portion of the AV fistula and Cephalic Arch which was successfully addressed by fluoroscopy guided angioplasty.
Conclusion: The above two cases highlight the advantage of the Nephrologist delivering a comprehensive and holistic care of vascular access. A well-trained Interventional Nephrologists is the best person to create and handle the vascular access in the best possible manner.
References
Lok CE, Huber TS, Lee T, et al; KDOQI Vascular Access Guideline Work Group. KDOQI clinical practice guideline for vascular access: 2019 update. Am J Kidney Dis. 2020;75(4)(suppl 2):S1-S164.
Symptomatic Central Venous Stenosis in Hemodialysis Patients Requiring Endovascular Intervention - A Case Series
Siri Chandana Gangasani, Ram Prasad, Jaya Kumar, Manikantan, Sandhya Suresh
Sri Ramachandra Institute of Higher Education and Research, Chennai
Introduction: Central Vein Stenosis (CVS) is a known complication in patients requiring Maintenance Hemodialysis (MHD) but symptomatic CVS requiring intervention is not so common. Here we present 3 cases of End Stage Renal Disease (ESRD) on MHD who developed CVS and under- went endovascular intervention.
Methods & Results: The study involves 3 patients with ESRD on MHD. Patients presented with chronic venous occlusion symptoms like swelling and pain of ipsilateral limbs. In view of suspicion of Central Vein Stenosis, CT Venogram done for the patients which showed stenosis of the central veins. Based on location and nature of the lesion different endovascular interventions were performed. Patients’ symptoms resolved and periodic follow-up was carried out to check vascular access patency and function.
Case1: 58-year-old male patient of ESRD on MHD via left brachiocephalic AVF presented with swelling of left arm.CT Venogram showed stenosis of brachiocephalic vein. Patient underwent successful balloon angioplasty of left brachiocephalic vein and HD continued through the same.
Case2: 56-year-old male patient of ESRD on MHD via left brachiocephalic AVF presented with progressive swelling of left arm. CT Venogram showed stenosis of central vein with partial thrombosis of axillary and subclavian veins. Patient underwent left brachiocephalic AVF ligation and new right radio cephalic AVF created for MHD. Symptoms resolved.
Case3: 44-year-old female patient of ESRD on MHD via right brachiocephalic AVF with history of multiple access failures, now presented with swelling and pain of right arm and breast. CT Venogram showed stenosis of right brachiocephalic vein. Patient underwent right brachiocephalic AVF ligation. Right IJV catheter placed as temporary access for HD and CAPD was planned. Patient’s symptoms improved.
Discussion & Conclusion: CVS is a serious issue in a hemodialysis patient. It is important to treat them but also to conserve the new created access. Endovascular intervention is the first treatment option for central venous obstruction. According to circumstances different interventional procedures are performed.
Acknowledgement
I would like to thank my professors Dr Ram Prasad, Dr Jayakumar, Dr Manikantan, Dr Sandhya Suresh for their guidance and patients for their cooperation.
References
1. Oguzkurt L, Tercan F, Yildirim S, Torun D. Central venous stenosis in haemodialysis patients without a previous history of catheter placement. Eur J Radiol. 2005;55:237–242. doi: 10.1016/j.ejrad.2004
2. Schwab SJ, Beathard G. The hemodialysis catheter conundrum: hate living with them, but can’t live without them. Kidney Int. 1999;56:1–17 Vascular Access Work Group. Clinical practice guidelines for vascular access. Am J Kidney Dis. 2006;48(Suppl 1):S248–S273
3. Miller GA, Friedman A, Khariton A, Preddie DC, Savransky Y. Access flow reduction and recurrent symptomatic cephalic arch stenosis in brachiocephalic hemodialysis arteriovenous fistulas. J Vasc Access,
4. YeatesK, ZhuN, VoneshE, TrpeskiL, BlakeP, FentonS. Hemodialysis and peritoneal dialysis are associated with similar outcomes for end-stage renal disease treatment in Canada. Nephrol Dial Transplant,
Femoral Tunnelled Cuffed Catheter (TCC) And Its Outcome in Indian ESRD patients
K Varalaxmi Shetty, Sreedhara C G, Kishan A, Gireesh Reddy, Mythri Shankardr Leelavati V, Umesh L, Shalini
Institute of Nephro-Urology, Bengaluru
Introduction: Though AV fistula is the best access for ESRD patients, TCC is the initial access in most ESRD patients. Although KDOGI guidelines suggest internal jugular vein and external jugular vein as preferred veins for tunneled catheter insertion but they are associated with Catheter related complications ultimately resulting in Stenosis/thrombosis of the central veins. Considering the above-mentioned points, an attempt was made to evaluate whether femoral tunneled catheters can be utilized as a bridge in the process of transition to permanent vascular access and as long-term vascular access in patients with multiple Vascular access failure and bilateral thoracic central venous occlusion (TCVO). This study aims to evaluate the technical feasibility and outcome of femoral TCC.
Methods & Results: This is an Open-label, Prospective study, conducted from Jan 2022 to June 13th 2023. All ESRD patients who underwent femoral TCC placement at Institute of Nephro-Urology, Bangalore centre were included. Around 36 patients were included in the study. Their demographic details, native kidney disease, length of tcc catheter, indication for TCC placement (as bridging access till AVF or permanent access in patients with multiple access failure) was categorised .
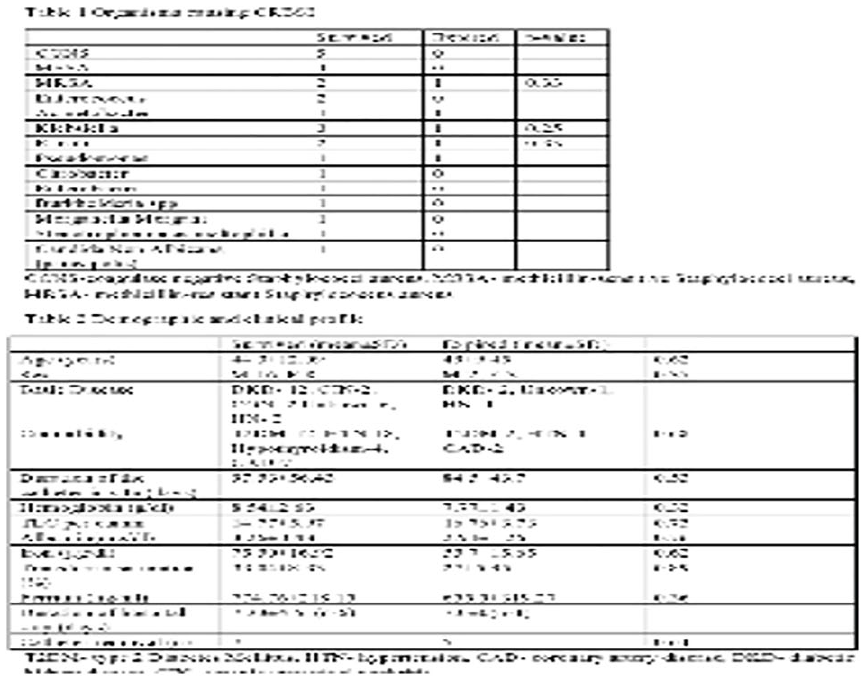
Conclusion and Discussion: Among 36 patients who underwent femoral TCC Placement, NKD -29 diabetic kidney diseases; 2ADPKD; 1 snake bite with cortical necrosis; 1chronic pyelonephritis; 1 c3 dominant GN; 1 IgA nephropathy; 1 TMA . Technical success was achieved in 100% of patients. Clinical success was achieved in 89%; Of these 5 patients had flow issue ( 2 patients within 1 month of TCC placement and 3 patients after 1 month ) however all 5 cases were managed with reteplase / heparin lock, none warranted catheter removal. Of 36 patients 5 patients were suspected to have CRBSI, 3 were culture negative 1 patient grown MRSA, Managed with antibiotic lock and catheter was salvaged, 1 grown MDR klebseilla with exit site infection in septic shock warranting catheter removal. Conclusions: From above results we can conclude that femoral TCC has favorable outcomes both in terms technical and clinical success when placed with right technique and timely intervened. The long-term outcomes will be mentioned in the subsequent period. Our study could be a basis for larger populations based Indian studies
Reference
1. Lok CE, Huber TS, Lee T, et al; KDOQI Vascular Access Guideline Work Group. KDOQI clinical practice guideline for vascular access: 2019 update. Am J Kidney Dis. 2020;75(4)(suppl 2):S1-S164
Does occluded Internal Jugular Vein (IJV) always mandate subclavian vein puncture or referral for more complex procedures? “Ultrasound (US)-guided Brachiocephalic Vein/Innominate Vein Hemodialysis Catheter placement”
Hemanth Kumar M K, Manas Ranjan Patel, Narayan Prasad
Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
Introduction: Central Venous Occlusion is common in hemodialysis patients with previous history of central venous catheters with a reported incidence of 26% in right IJV. US-guided brachiocephalic vein cannulation could be used as cost-effective and easier alternative to SCV or EJV or Contralateral IJV cannulation for catheter insertion in such patients
Methods & Results: In this case series of 10 patients with history of previous right IJV catheters, IJV occlusion was confirmed by Doppler USG. Supraclavicular short-axis out-of-plane or long-axis in-plane approach of BCV puncture was done by placing the 6-13MHz linear US probe just above the medial 1/3rd of clavicle and tilting the probe more caudally with 10-150 angulation. After confirming the patency of lower BCV and SVC by venogram, tunneled/non-tunneled dialysis catheters were inserted over guidewire.
Conclusion and Discussion: BCV central venous catheters have been described in infants and young children but their use in adults with IJV can be explored too. Innominate vein approach has been used only in 10% of cases with bilateral IJV thrombosis as compared to EJV approach in 14% of cases with patent SVC1. With use of optimal operator technique, 80-100% success rate for BCV puncture have been achieved in adults too with complication rates as low as 2.3%2,3. A comparative study even revealed BCV cannulation was associated with an estimated 62% lower odds of procedural difficulty compared to IJV4. However, a prospective- RCT revealed BCV approach was only non-inferior to IJV approach in those with patent IJV with regards to mean cannulation time, overall success rate and ease score of cannulation5. In our study, we avoided contralateral IJV approach or SCV approach as 6 of these patients already had a functioning non-mature AVF and 4 were awaiting AVF creation. We reported no complications. Hence, we suggest exploring BCV as a viable cost-effective option in those with Unilateral or Bilateral IJV thrombosis with patent central veins than FV or SCV or left sided approaches which are associated with higher rates of infection and thrombosis.
Acknowledgement
All Faculty and DM Residents of Dept. of Nephrology, SGPGI, Lucknow All Staff Nurse and Radiographers of Nephrology OT, SGPGI, Lucknow
References
1. Gouda ZE, Emara MM, Elbarbary HS, Koura MAA, Elarbagy AR. Studying alternative approaches for placement of cuffed hemodialysis catheters in hemodialysis patients with bilateral internal jugular vein occlusion. J Vasc Access. 2019 May;20(3):250-259. doi: 10.1177/1129729818794414. Epub 2018 Aug 24. PMID: 30141363.
2. Falk A. Use of the brachiocephalic vein for placement of tunneled hemodialysis catheters. AJR Am J Roentgenol. 2006 Sep;187(3):773-7. doi: 10.2214/AJR.04.1830. PMID: 16928944.
3. Moataz Fatthy, Tarek S. Abdelaziz, Mohamed A. Marie, Mohamed Abdelkawi, Tamer Abdel Tawab; Placing a Hemodialysis Catheter in Patients With Multiple Access Failure and Exhausted Usual Approachable Veins: Egyptian Single Center Experience.
4. Beccaria PF, Silvetti S, Lembo R, Landoni G, Monti G, Zambon M, Mamo D, Zangrillo A. The Brachiocephalic Vein as a Safe and Viable Alternative to Internal Jugular Vein for Central Venous Cannulation. Anesth Analg. 2018 Jul;127(1):146-150. doi: 10.1213/ANE.0000000000003357. PMID: 29683822.
5. Aydın T, Balaban O, Turgut M, Tokur ME, Musmul A. A Novel Method for Ultrasound-Guided Central Catheter Placement-Supraclavicular Brachiocephalic Vein Catheterization Versus Jugular Catheterization: A Prospective Randomized Study. J Cardiothorac Vasc Anesth. 2022 Apr;36(4):998-1006. doi: 10.1053/j.jvca.2021.06.010. Epub 2021 Jun 12. PMID: 34247928.
Role of Early Postoperative Doppler Ultrasonography in Prediction of AV Fistula Maturation Among Hemodialysis Patients: A Prospective Study
Akansha Umesh, Pooja prabhu, Mahesh E
M S Ramaiah Medical college
Background: The increasing prevalence of chronic kidney disease, coupled with advancements in the diagnosis and treatment of renal diseases and improvements in life expectancy, has led to a greater number of patients requiring hemodialysis. The preferred method of vascular access for hemodialysis is AV fistula formation; however, it is associated with a high rate of failure. In our prospective study, we focused on 40 patients scheduled for hemodialysis and utilized preoperative ultrasound vessel mapping as well as early postoperative ultrasound assessment on day 7 to establish criteria for predicting early fistula failure.
Method and Results: We employed preoperative ultrasound mapping to assess various factors such as cephalic vein diameter, compressibility, and color flow, as well as radial and brachial artery diameter, peak systolic velocity, and intimal wall calcification. Postoperatively, ultrasound examinations were conducted on day 7 and at 6 weeks to evaluate fistula blood volume and detect any complications. A significant association between fistula failure and factors such as cephalic vein diameter, brachial artery diameter, intimal vessel wall calcification, and comorbid conditions like diabetes mellitus was observed. Furthermore, the blood flow at day 7 was notably lower in the failure group compared to those with a functioning fistula and any fistula with blood flow <154 ml/min on day 7 may be predictive of early fistula failure.
Conclusion: Preoperative vessel mapping and early postoperative ultrasonography play a crucial role in patients who require AV fistula formation for hemodialysisand provide valuable information for selecting suitable vessels for successful fistula creation and enable early intervention to salvage a failing fistula after the surgery. By utilizing these, healthcare professionals can make informed decisions and take necessary steps to optimize the outcomes of AV fistula formation in patients undergoing hemodialysis.
Acknowledgement
Dr Madhuri - senior resident Radiology Dr Jhanavi - senior resident Radiology, M.S. Ramaiah Medical College and hospital
References
1. Michelle L. Robin, Tom Greene, Michael Allon, Laura M. Dember, Peter B. Imrey, Alfred K. Cheung et al.; Prediction of Arteriovenous Fistula Clinical Maturation from Postoperative Ultrasound Measurement,
2. Abd-Elmageed, M., Elsayed, B.F. & Elkholy, M.R. Role of early postoperative ultrasonography in prediction of AV fistula failure in hemodialysis patients. Egypt J Radiol Nucl Med 51, 95 (2020). https://doi.org/10.1186/s43055-020-00184-4
3. Patel P, Prabha V, Verneker RR, Nerli RB, Patel T, Ghagane SC. Role of color Doppler assessment in predicting outcomes of wrist Brescia-Cimino arteriovenous fistula creation: A single-center prospective study. Indian J Urol. 2023 Jan-Mar;39(1):33-38. doi: 10.4103/iju.iju_190_22. Epub 2022 Dec 29. PMID: 36824103; PMCID: PMC9942221.
Outcome of Reteplase Use In Management Of Dysfunctional Vascular Access In Indian ESRD Patients
Prasanna Bhat, Gireesh Reddy G, Sreedhar CG, Kishan A, Mythri S, Aathish MN, Ankitha R, Sairam B
Institute Of Nephr-Urology, Bangalore
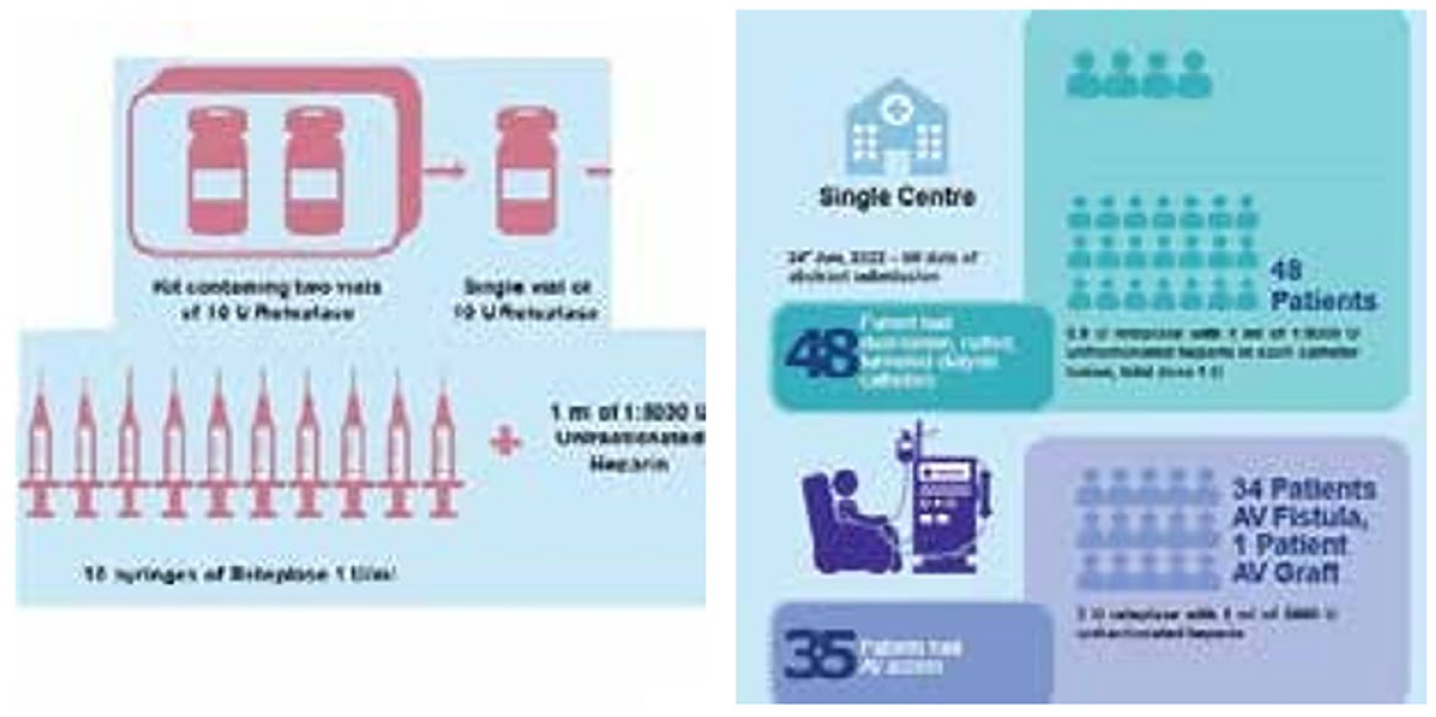
Introduction: In 2018, approximately 1,75,000 patients in the India were on maintainance hemo- dialysis (1). Failure of hemodialysis access is a major cause of morbidity and hospitalization in these patients. Reteplase has shown to re-establish patency with highest success rates 92% vs Tenecteplase 46% vs Alteplase 81% (2,3,4,5)
Methods & Results: Method: Around 48 patients had Dysfunctional TCC who underwent thrombolysis with 0.5U Reteplase with 5000u Heparin per port and 35 had thrombosed AV access who underwent thrombolysis with 5U Reteplase with 5000U Heparin. Among 48 catheter dysfunction cases which underwent thrombolysis with Reteplase, 98% patients had restored complete patency of catheter and underwent further Hemodialysis sessions without any flow issues. Among 35 cases of AV access thrombosis, 85% had complete restoration of flow
Conclusion and Discussion: Reteplase is clinically and cost wise an effective thrombolytic (roughly INR 700 for catheter dysfunction cases and RS 3500 for AVF thrombosis cases). From above results we can conclude that Reteplase could be used as a preferred thrombolytic for dysfunctional access other than Urokinase, Tenecteplase or Alteplase in both resourceful and resource constraint settings.
References
1. Lok CE, Huber TS, Lee T, et al. Kdoqi Clinical Practice Guideline For Vascular Access: 2019 Update. Am J Kidney Dis. 2020;75(4):s1
2. Castner D. The Efficacy of Reteplase in The Treatment of Thrombosed Hemodialysis Venous Catheters. Nephrol Nurs J 2001;28:403-10
3. Hilleman D, Campbell J. Efficacy, Safety, and Cost of Thrombolytic Agents for The Management of Dysfunctional Hemodialysis Catheters: A Systematic Review. Pharmacotherapy: The Journal of Human Pharmac
4. Falk A, Samson W, Uribarri J, Vassalotti JA. Efficacy of Reteplase in Poorly Functioning Hemodialysis Catheters. Clin Nephrol 2004;61:47-53
5. Hyman G, England M, Kibede S, Lee Willets G. The Efficacy And Safety of Reteplase for Thrombolysis of Hemodialysis Catheters at A Community and Academic Regional Medical Center. Nephrol Clin Pract 200
A heuristic roadmap for selection of configuration of cubital AV fistula based on observational study
Sameer Vilas Vyahalkar, Sameer Vyahalkar, Arif Hoda, Avinash Chaudhari, Pooja Binnani, Amar Kulkarni, Amit Nagarik
Dr D Y Patil Hospital, Navi Mumbai
Introduction: When radiocephalic AVF (RCAVF) isn’t feasible, the choice of next AVF varies according to the presence of adequate vessels and surgeon’s preference. Cubital region is the next commonly selected site for AVF creation. We propose a roadmap for selecting the next configuration after radiocephalic AVF based on our experience.
Methods & Results: Nephrologist-operated 174 AVFs over 3-year period, 72 (41.37%) were other than RCAVF; Gracz-29 (40.27%), brachio-basilic AVF (BBAVF) were 9 (12.5%) and brachio-cephalic AVF (BCAVF) were 22 (30.55%). 0ne-year outcomes of cubital AVFs were compared. Successful use of fistula for haemodialysis was observed in 86.2% of Gracz, 100% of BBAVF and 81.81% of BCAVF. Maturation of veins in arm was observed in Gracz group and BBAVF group and inadequate cephalic vein was observed preoperatively. Those with primary failure in Gracz group subsequently underwent BCAVF with successful outcome.
Conclusion and Discussion: We compared medium-term outcomes of three commonly employed types of cubital AVF. Cubital perforator v and median basilic v., when anastomosed to proximal radial artery or brachial artery, have the potential of arterialisation and maturation of cephalic v. and basilic v. of arm, as well as forearm veins, thus providing wider options of cannulation, reducing cannulation failure and preserving future access sites for AVF creation. We think that these two configurations should be preferred options before considering BCAVF. We propose a roadmap to proceed with selection of the site of AV fistula when RCAVF or PRA-MAVF are not feasible. This roadmap is based on the assumption of presence of the most common M or Y pattern of cubital veins, but when there is deviation from usual anatomical pattern, plan for AVF should be modified accordingly. In presence of high bifurcation of brachial artery, use of brachioulnar artery is more likely to result in SUFH than brachio-radial artery.
References
1. Fitzgerald JT, Schanzer A, Chin AI. Outcomes of upper arm arteriovenous fistulas for maintenance hemodialysis access. Arch Surg 2004;139(2):201-208
3. Elamurugan E, Hemachandar R. Brachiocephalic arteriovenous fistula for hemodialysis through the median antecubital vein. Indian Journal of Nephrology 2017;27(3):177-180
4. Pires L, Fonseca Jr A, Manaia J, Leite T, Babinski M, Chagas C. Comprehensive review of the superficial veins of the forearm from a historical, anatomical and clinical point of view. Italian Journal of Anatomy and Embryology 2019;124(2):142-152
An Observational Study on Tunnelled Cuffed Catheter Related Infection in A Tertiary Care Centre
Sweety Kakoti
Apollo Hospitals, Guwahati
Introduction: Tunnelled cuffed catheters (TCC) used for hemodialysis treatment are prone to infections, leading to complications and high mortality rates. Efforts to salvage TCC after bacteremia often result in recurrent infections, but comprehensive studies on confounding factors are lacking. Catheter-related infections pose a significant obstacle to long-term catheter use.
Methods & Results: An observational study of 6 months duration was performed at a tertiary care center in Northeast India, in patients on chronic HD using a tunnelled cuffed catheter and who had an episode of TCC related infection as per KDOǪI 2019 criteria. All the patients were observed for 6 months and outcomes were recorded.
Conclusion and Discussion: Among 55 patients with TCC-related bacteremia, follow-up data was available for 49. 53% were male and 47% were female. The majority had diabetes (96.36%), hypertension (92.73%) and 90.91% had both conditions. Most patients (94.54%) had an internal jugular catheter, while only 5.46% had a femoral catheter. Culture positivity occurred in 87.27% of cases, with Staphylococcus aureus (52.08%), Coagulase-negative staphylococci (20.83%), Enterococcus (22.92%), and Escherichia coli (4.17%) being the main pathogens. TCC removal was necessary in 27.27% of patients, while 52.73% were salvaged using IV antibiotics alone, and 20% required both IV antibiotics and antibiotic lock therapy. Mortality was observed in 3.63% of patients, and recurrent infection in 18.36%. Staphylococcus aureus infection significantly predicted treatment failure, with a nearly 6-fold higher risk in salvage attempts. Other factors associated with salvage failure included femoral TCC and the presence of both diabetes and hypertension. Tunnelled cuffed catheter (TCC) use poses infection risks with high morbidity and mortality. Salvage attempts post-bacteremia often lead to recurrent infections. Our study highlights the challenges and factors impacting TCC-related infections and treatment outcomes.
Acknowledgement
Dept. of Nephrology, Apollo Hospitals, Guwahati
References
1. Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, Abreo K, Allon M, Asif A, Astor BC, Glickman MH, Graham J, Moist LM, Rajan DK, Roberts C, Vachharajani TJ, Valentini RP; National Kidney Foundation. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. Am J Kidney Dis. 2020 Apr;75(4 Suppl 2):S1-S164. doi: 10.1053/j.ajkd.2019.12.001. Epub 2020 Mar 12. Erratum in: Am J Kidney Dis. 2021 Apr;77(4):551. PMID: 32778223.
2. MOKRZYCKI, MICHELE H.*,†,‡; SCHRO[Combining Diaeresis]PPEL, BERND*,†; GERSDORFF, GERO VON*,†; RUSH, HEATHER*,‡; ZDUNEK, MIROSLAW P.*,‡; FEINGOLD, ROBERT*,‡. Tunneled-Cuffed Catheter Associated Infections in Hemodialysis Patients Who Are Seropositive for the Human Immunodeficiency Virus. Journal of the American Society of Nephrology 11(11):p 2122-2127, November 2000. | DOI: 10.1681/ASN.V11112122
3. Mokrzycki MH, Zhang M, Cohen H, Golestaneh L, Laut JM, Rosenberg SO. Tunnelled haemodialysis catheter bacteraemia: risk factors for bacteraemia recurrence, infectious complications and mortality. Nephrol Dial Transplant. 2006 Apr;21(4):1024-31. doi: 10.1093/ndt/gfi104. Epub 2006 Jan 31. PMID: 16449293.
USG Guided AVF Plasty – Experience From A Tertiary Care Centre In South India
Athish M N
Institute Of Nephro-Urology, Bangalore
Introduction: An arteriovenous fistula is the access of choice for hemodialysis as it cost effective with better longevity and is not frequently infected. However, they are prone for stenosis and thrombosis thereafter, which needs definitive intervention to salvage the access for which USG is also an imaging option for the same.
Methods & Results: We reviewed 21 cases of UG-PTA which were done between September and December 2022. All Cases of access dysfunction except for central vein stenosis were included. All cases underwent an immediate screen and diameters were recorded and followed up at 3 and 6 months. Success was achieved in 91% of cases, with patency rates at 3 and 6 months being 82%. Complications included hematoma and vein rupture which could be conservatively managed
Conclusion and Discussion: Ultrasound guided interventions for AV fistulas is practical as fistulas are peripheral and easily accessible and therefore don’t need an operating room or fluroscopy guidance. In our study common lesions encountered were juxta anastomotic and outflow stenosis causing thrombosis of AV Access. Longest duration of use of the AVF before needing intervention was 2 years and shortest duration was 2 weeks, emphasizing the need for good surgical technique. 80% patients had Diabetes, 15% had concomitant IHD and all patients suffered from hypertension, probably as a component of CKD. 66 % patients had DKD as the basic disease, correlating with vascular complications in diabetes mellitus. All accesses were on the left upper limb, with 48 % being BCF’s, 28 % being RCF’s, 19% being BBAVF and one Brachio-Axillary AV graft. We had 1 hybrid procedure as well. The procedure is a safe and effective method to treat stenosed and thrombosed accesses. It is safer with regard to exposure to radiation as well. However, it is labor intense, needing a dedicated team to salvage precious accesses and definite outcomes of prospective studies are needed to ascertain the long-term outcomes of this procedure and the access benefits it provides to the patient.
References
1. Wakabayashi M, Hanada S, Nakano H, et al. Ultrasound-guided endovascular treatment for vascular access malfunction: results in 4896 cases. J Vasc Access 2013; 14: 225-30
2. Kumar S, Mahajan S, Patl SS, et al. Ultrasound-guided angioplasty for treatment of peripheral stenosis of arteriovenous fistula– a single-center experience. J Vasc Access 2017; 18: 52-6 Dariusz Szewczyk, Piotr Andziak, Krzysztof Bojakowski et al. Ultrasound-guided angioplasty of dialysis fistulas in renal transplant patients- J Vasc Miniinv 2019; 14 (4): 532- 537
3. Gorin DR, Perrino L, Potter DM, et al. Ultrasound-guided angioplasty of autogenous arteriovenous fistulas in the office setting. J Vasc Surg 2012; 55: 1701-5
4. Napoli M, Prudenzano R, Russo F, Antonaci AL, Aprile M, Buongiorno E. Juxta-anastomotic stenosis of native arteriovenous fistulas: surgical treatment versus percutaneous transluminal angioplasty. JVA,
Translumbar Dialysis Catheter - A Savior In Multiple Access Failure
Introduction: Access to hemodialysis in India for ESRD patients and their longetivity has increased tremendously with government support. Same time, this increases the prevalence of patients with vascular access issues. Here we report patient with exhausted vascular access in whom Translumbar IVC Permcath insertion (TLDC) was done as a life saving measure.
Methods & Results: 58-year female with diabetic ESRD with hemodialysis vintage of 6 years was switched to CAPD in view of multiple access failure. After one year patient had refractory peritonitis, which led to removal of CAPD catheter. Attempts at alternate access was futile. As a last resort, TLDC inserted by interventional radiology using gunsight technique for infrarenal IVC access and a 40 cm hemodialysis catheter (BARD glide path) tunneled along lateral abdominal wall. Flow was adequate.
Conclusion and Discussion: Long-term haemodialysis requires an effective vascular access. End-stage renal disease patients are faced with very limited options when they occlude all usable extremity and central veins.
Translumbar HD catheters are essentially long, tunneled dialysis catheters that are inserted through the skin and muscles of the back, advanced into the abdominal portion of the IVC and positioned in the right atrium. This technique was first reported by Lund et al in 1995. Though the translumbar approach eliminates traditional complications such as pneumothorax and inadvertent arterial punctures, this access is also not problem free. Rates of infection and thrombosis are comparable to those with other access sites. The catheter patency rate at 3,6,12 months were 43%, 25% and 7% respectively in a study by Liu et al. The main complication reported were poor flow(40%) and infections (36%). One unique complication noted was retroperitoneal hemorrhage and fibrosis. In our patient 350ml/min flow was supported, no retroperitoneal bleed and discharged in stable condition with aspirin and warfarin. Thus TLDC might offer a relatively safe and effective dialysis access option for patients with limited central venous access. However, additional studies are needed to estimate the long-term patency and safety in this high-risk population.
Acknowledgement
Barnard Institute of Interventional Radiology
Anatomical variants and insertion of tunnelled/ non tunnelled dialysis catheters
Introduction: Internal jugular vein is the most preferred temporary/permanent vascular access for emergency hemodialysis. Cognizance of the anatomical variations of neck vasculature, although rare, can help prevent procedure related complications. Here we describe incidental detection of persistent left superior vena cava (PLSVC).
Methods & Results: Case-1 is presented as 45/M, with secondary fistula failure underwent right jugular TCC insertion uneventfully. However, during first dialysis, he developed palpitations due to new onset atrial fibrillation. 2DEcho revealed persistent left SVC. Symptoms worsened during next dialysis necessitating TCC removal. Case-2 was 48/ F, needed non-tunnelled jugular HD catheter for initiation of emergency dialysis. Post procedure Xray showed abnormal position of catheter tip, CT scan revealed catheter tip in coronary sinus. 2DEcho confirmed presence of persistent left SVC.
Conclusion and Discussion: The presence of PLSVC has important clinical implications, because dialysis catheter insertion may precipitate cardiac conduction abnormalities especially during dialysis. Arrhythmias can be caused by persistence of embryological pacemaker tissue located along the posterior cardinal vein and/or dilated coronary sinus. It can manifest as atrial fibrillation/flutter, tachyarrythmias or bradyarrythmias. These patients may require placement of pacemaker or defibrillator and ideally these patients need to be dialysed under cardiac monitoring. Secondly, PLSVC may be associated with a variety of other congenital malformations of heart and great vessels, such as cor triatriatum, atrial septal defect, bicuspid aortic valve and coarctation of aorta, especially in the absence of right sided superior vena cava. There are reports of association of PLSVC with complications like cardio respiratory arrest during dialysis, pericardial effusion and thrombus formation. In patients with PLSVC, it is generally recommended to avoid TCC. Thus we would like to highlight the significance of thorough pre and post procedure evaluation during tunnelled/non tunnelled dialysis catheter insertion.
References
1. Corîci OM, Gașpar M, Mornoș A, Iancău M. Cardiac Arrhythmias in Patient with Isolated Persistent Left Superior Vena Cava. Curr Health Sci J. 2017 Apr-Jun;43(2):163-166. doi:10.12865/CHSJ.43.02.10. Epub 2017 Jun 29. PMID: 30595873; PMCID: PMC6284175.
2. Goyal, S.K., Punnam, S.R., Verma, G. et al. Persistent left superior vena cava: a case report and review of literature. Cardiovasc Ultrasound 6, 50 (2008).
3. Kute VB, Vanikar AV, Gumber MR, Shah PR, Goplani KR, Trivedi HL. Hemodialysis through persistent left superior vena cava. Indian J Crit Care Med. 2011 Jan;15(1):40-2. doi:10.4103/0972-5229.78223. PMID: 21633545; PMCID: PMC3097541
Unconventional use of nitroglycerine in a failing AVF
Kajal Vijay Darandale, Tushar Dighe
Deenanath Mangeshkar hospital, Pune
Introduction: Transdermal nitroglycerine (NTG) administration may have a beneficial effect in the creation of an AVF by increasing blood flow through the access and by inhibiting platelet aggregation. We evaluated the hemodynamic effects of transdermal NTG on AVF with reduced blood flow in two patients
Methods & Results: Two patients with chronic kidney disease on maintenance hemodialysis through AVF for more than 6 months were chosen. As NTG cream and patch were unavailable, 0.5% of NTG per gram of cream was made with easily available moisturizing cream. The cream was applied locally 24 hrs prior to dialysis in a dose of thrice a day. After a week of application of the cream blood flow through the AVF was checked.
Conclusion and Discussion: Significant increase in blood flow observed after a week of application from 150 ml/ min (prior to application of NTG) to 250 ml/ min( post NTG application). We concluded that local application of 5 % NTG cream is a safe and effective method of improving blood flow through AVF.
References
1. Hemodynamic effect of transdermal ermal glyceryl trinitrate on newly constructed arteriovenous fistula; Emin Baris Akin, Omer Tapcu, Hasan Ozcan, Sadik Ersoz, Suat aytac, Erdal Anadol; Pmid : 12205547,
2. Facilitated intravenous access through local application of nitroglycerine ointment; R J Roberge, M Kelly, T C Evans; Ann Emerge Med, 1987 may;16(5):546-9
Losing of Hydrophilic guide wire(Glidewire) jacket: A rare procedural complication - Identification and methods for its safe removal
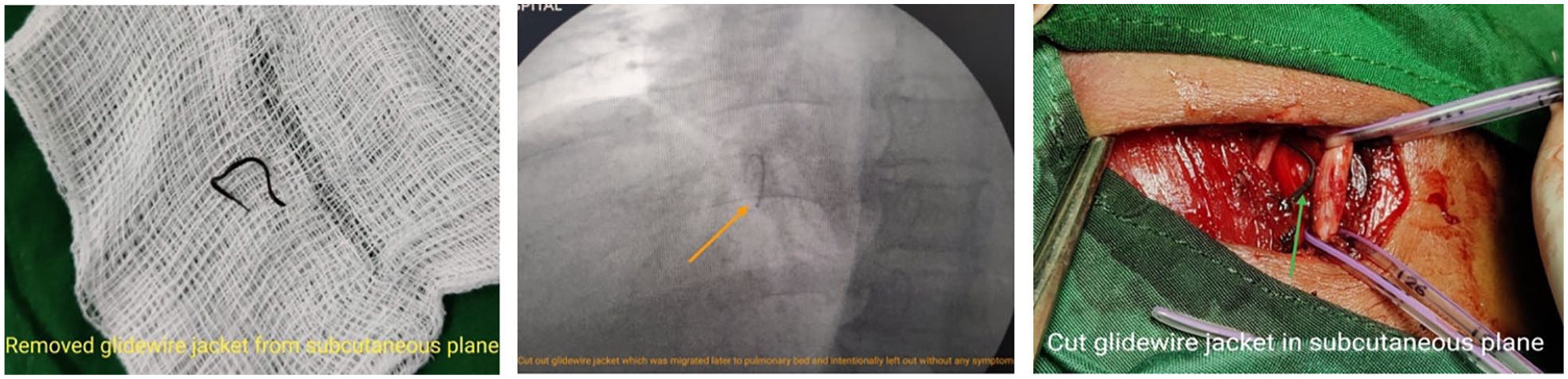
Introduction: Glidewire is a very useful tool for difficult passage of insertion of central venous catheter, fistuloplasty, angiogram and other procedures requiring seldinger technique. Glidewire complications may occur such as kinking, knotting and fracture, which may lead to severe complications like embolization, removal of it may also cause vessel damage
Methods & Results: We report 3 different cases of Glidewire fracture and entrapment of jacket into central vein, from Muljibhai Patel Urological Hospital, Nadiad, from which, 1 case of successful removal using snare-loop under fluoroscopic guidance, 1 case of removal via subcutaneous incision and 1 case of intentionally left out fractured jacket into pulmonary artery bed without any symptoms. All 3 patients recovered without any complications.
Conclusion and Discussion: Glidewire consists of hydrophilic coating and polyurethane jacket with nitinol core alloy. Breakage or fracture of the guide wire during insertion, negotiation or withdrawal can cause complications including myocardial perforation, pulmonary embolism, arrhythmias, sepsis, endocarditis and even cardiac arrest. When resistance is felt during insertion or withdrawal of the guidewire, force should not be applied to the guidewire and care should also be exercised when passing the tissue dilator over the guidewire to avoid stripping. All accessories should be properly examined before and after the procedure to recognize any lost part. Stripped glide wire fragments can be safely removed percutaneously under fluoroscopic guidance. The most commonly used techniques are snare-loop or basket catheter, other consist of open vascular surgery in case of failed/ not approachable fractured part via snare loop or basket catheter.
Acknowledgement
I would like to thank Department of Nephrology, Muljibhai Patel Urological Hospital, for the help required for this report preparation.
References
1. Garg R, Ramaiah VK, Chouhan RS. Damaged guidewire by the introducer needle tip while inserting central venous catheter in subclavian vein by supraclavicular approach. Saudi J Anaesth 2010; 4: 210-212
2. Polos PG, Sahn SA. Complication of central venous catheter insertion: fragmentation of a guidewire with pulmonary artery embolism. Crit Care Med 1991; 19: 438-440. PMID: 1999111
3. Carpentier JP, Braz da Silva J, Choukroun G. Formation of a knot in a J spiral metallic guide: a complication of the Seldinger method. Cah Anesthesiol 1991; 39: 277-278. PMID: 1933528
4. Han HS, Jeon YT, Na HS, Hwang JY, Choi EJ, Kim MH. Successful removal of kinked J-guide wire under fluoroscopic guidance during central venous catheterization -A case report-. Korean J Anesthesiol 201
5. Wang HE, Sweeney TA. Subclavian central vcenous catheterization complicated by guidewire looping and entrapement. J Emerg Med 1999; 17: 721-724. PMID: 10431965
Immediate clinical Success of Transluminal Angioplasty In Hemodialysis Access Related Complications
Introduction: Arteriovenous fistulae (AVF) for hemodialysis (HD) are prone to development of multiple complications, which can lead to nonfunctioning of the fistula. We report outcomes of endovascular management for dysfunctional HD AVF.
Methods & Results: 35 patients on maintenance haemodialysis underwent transluminal angioplasty at Indraprastha apollo new delhi. The clinical signs of the adequacy of vascular access, including a continuous palpable thrill with minimal or no pulsatility; no complaint of prolonged bleeding time after needle removal and no complaints while puncturing the access site were considered as an indicator of clinical success. The resumption of normal HD for a minimum of 1 session was considered as clinical success
Conclusion and Discussion: In the present study, the clinical success rate immediately after the procedure was 97% Khan T et al., reported that the clinical success of the procedure in their study was around 92%(1). Yadav et al., reported an overall clinical success was noted in 81.7% of cases (2)
References
1. Khan T, Bhat M, Shah OA, Choh NA, Maqsood S, Shera TA. Percutaneous Transluminal Angioplasty of Dysfunctional Hemodialysis Vascular Access: Can Careful Selection of Patients Improve the Outcomes? 2022
2. Yadav N, Gamanagatti S, Sharma R, Aggarwal SK, Bansal VK, Kandasamy D, et al. Outcomes of Endovascular Therapy for Salvage of Hemodialysis Arteriovenous Fistulae. J Clin Interv Radiol ISVIR. 2021;142–,
Immediate Anatomic Success Of Transluminal Angioplasty In Hemodialysis Access Related Complications
Introduction: Patients with chronic kidney failure whose life depends on routine hemodialysis, need good hemodialysis access. Arteriovenous fistula (AVF) is prone to stenosis. The best treatment for the problem of AVF stenosis is by percutaneous transluminal angioplasty whose immediate anatomic outcomes were analyzed in this study
Methods & Results: 35 patients on maintenance haemodialysis underwent transluminal angioplasty at Indraprastha Apollo Hospital, New Delhi. The angiographic inclusion criteria was a morphological evidence of stenosis of more than 50%. Anatomical success was a less than 30% residual stenosis and restoration of normal flow on post procedure angiogram. Angiography followed by angioplasty was successful in 34 (97.14%) participants and only 1 participant did not meet the criteria for the anatomic success
Conclusion and Discussion: Angiography followed by angioplasty was effective in 34 (97.14%) out of 35 of the participants and just one individual did not fulfil the criteria for the anatomic success immediately after the procedure. Tan TL et al., reported an anatomical success rate of 100% among their participants (1). Khan T et al., reported that the anatomical success in their study was 98% with only one patient in whom they were unable to cross the stenosis with the guidewire (2). Saleh et al., reported that anatomical success was achieved in 144 (96.6%) patients (3). Yadav N et al., reported that anatomical success were noted in 95% participants (4). Aktas A et al. (5) found an anatomical success rate of 97.2%
Acknowledgement
Special thanks to my coauthors who happen to be my teachers and guides both in nephrology and in real life.
References
1. Tan TL, May KK, Robless PA, Ho P. Outcomes of endovascular intervention for salvage of failing hemodialysis access. Ann Vasc Dis. 2011;4(2):87–92.
2. Khan T, Bhat M, Shah OA, Choh NA, Maqsood S, Shera TA. Percutaneous Transluminal Angioplasty of Dysfunctional Hemodialysis Vascular Access: Can Careful Selection of Patients Improve the Outcomes? 2022
3. Saleh M, Ibrahim M, Ali H. Outcomes of balloon angioplasty for failing upper extremity dialysis access. Egypt J Surg 2020;39(3)
4. Yadav N, Gamanagatti S, Sharma R, Aggarwal SK, Bansal VK, Kandasamy D, et al. Outcomes of Endovascular Therapy for Salvage of Hemodialysis Arteriovenous Fistulae. J Clin Interv Radiol ISVIR. 2021;142,
5. Aktas A, Bozkurt A, Aktas B, Kirbas I. Percutaneous transluminal balloon angioplasty in stenosis of native hemodialysis arteriovenous fistulas: technical success and analysis of factors affecting postprocedural fistula patency. Diagn Interv Radiol. 2015 Mar-Apr;21(2):160-6. doi: 10.5152/dir.2014.14348. PMID: 25698092; PMCID: PMC4463311.
Anastomotic Pseudoaneurysm of Arteriovenous Fistula in Hemodialysis Patients Having Non-Cuffed Catheters as Vascular Access
Arif Anwarul Hoda, Sameer Vyahalkar, Avinash Chaudahri
Dr D Y Patil Hospital, Navi Mumbai
Introduction: Vascular access (VA) is one of the most important part of hemodialysis (HD). Not only is the access vital for the patient on HD, but also it is vulnerable to complications. We hereby report our experience on the incidence of anastomotic pseudoaneurysm of AVF (PA-AVF).
Methods & Results: Cohort study based on retrospective analysis of three-year data of case-series of PA-AVF occurring in first six months after AV fistula creation for hemodialysis. Among the 283 AV fistula surgeries (215 distal forearm radio-cephalic AVF and 68 brachial artery or cubital region AVF), 7 patients (2.4%) developed PA-AVF within 1 to 8 weeks after AV fistula surgery. Over-extended dependence on non-cuffed hemodialysis (HD) catheter was a common factor among patients developing this complication.
Conclusion and Discussion: Our observations suggest that infections are primarily responsible for anastomotic PAs of the AVF occurring within the first few months of surgery. Both wound infection and CRBSI are common sources of infection in this population. Diagnosis of CRBSI should be actively sought in patients who are undergoing HD through HD catheters and are planned for AVF surgery. VA surgery must not only be avoided in the presence of infections but also until CRBSI is completely treated and bacteremia ruled out. At the same time, a high degree of vigilance is necessary for the early diagnosis and management of CRBSI to avoid infected PA of AVF after AVF surgery in catheter-dependent patients. The role of timely AVF creation to avoid or minimize catheter dependence cannot be overemphasized.
Acknowledgement
We would like to thank Dr. Suhas Bendre, Dr. K.N. Bhosale, and Dr. Sandeep Verma – CVTS
References
1. Tal MG, Ni N. Selecting optimal hemodialysis catheters: Material, design, advanced features, and preferences. Tech Vasc Interv Radiol 2008;11:186-91
2. Lee T, Mokrzycki M, Moist L, Maya I, Vazquez M, Lok CE, et al. Standardized definitions for hemodialysis vascular access. Semin Dial 2011;24:515-24.
3. Kumar A, Jha MS, Singla M, Gupta N, Raina P, Dubey D, et al. Radio-median cubital/radiocephalic arteriovenous fistula at elbow to prevent vascular steal syndrome associated with brachiocephalic fistula
Catheter related right atrial thrombus (CRAT) in patient on maintenance haemodialysis
Ajit Kumar Dash
TNMC & BYL Nair Ch. Hospital, Mumbai
Introduction: CRAT is a serious complication of central venous cannulation. It is associated with triple-lumen catheters for chemotherapy, intravenous fuids or parenteral nutrition,and hemodialysis catheters. CRAT has severe consequences leading to pulmonary embolism, infection with septic emboli, arrhythmias. Few case reports are available on this topic which limits the strength of our inferences.
Methods & Results: 61-year-old male with CKD on MHD for 4 months through right IJV TCC. Presented with fever on hemodialysis. Diagnosed as CRBSI, started IV antibiotics. Blood cultures s/o VRE while 2D echocardiography revealed RA mass measuring 20 X 23 mm. The catheter was removed and temporary hemodialysis catheter was inserted. Fever persisted despite 3 weeks of treatment with sensitive antibiotics. Repeat 2D echocardiography revealed persistent mass. Patient continued to deteriorate in the form of septic shock and was started on inotropes with antibiotics being stepped up. Patient was planned for surgical removal of cardiac mass; however, relatives refused this treatment option. Patient succumbed to severe sepsis about 4 weeks after his hospital admission.
Conclusion and Discussion: Incidence of CRAT is reported to be 5.4% in haemodialysis patients .There are two different types of right atrial thrombi: Type A which are highly mobile thrombi that are found in structurally normal atria and Type B thrombi that are attached to the atrial wall and are found in structurally abnormal atria or in the presence of foreign bodies, like a catheter.The CRAT presented here is Type B thrombus which has a reported incidence of 14 % for pulmonary embolism and has a mortality rate of 18.3% in dialysis patients. The mechanism of catheter-associated thrombus formation is repeated mechanical trauma to the atrial wall caused by the movement of the catheter tip due to the movement of the heart. Infection creates a thrombogenic environment or alternatively the thrombosis may serve as a nidus for colonization and bacteraemia. CRAT, should be suspected in all dialysis patients on tunnelled and untunnelled catheters. Thus, 2D echocardiography should be done as a screening in all dialysis patients presenting with CRBSI. Catheter removal should be the first step in the management of a CRAT followed by either anti-coagulation or surgical thrombectomy. Co-morbidity is likely to remain an important issue in the choice of treatment.
Reference
1. Ross P Jr, Ehrenkranz R, Kleinman CS, Seashore JH. Thrombus associated with central venous catheters in infants and children. J Pediatr Surg. 1989 Mar;24(3):253-6. doi: 10.1016/s0022-3468(89)80006-5. PMID: 2496218.
AV fistula outflow stenosis- an under-recognized entity
Tusti Kumari, Smita Patil, Atim Pajai, Ajit Dash, Kalpana S M
TNMC & BYL Nair Ch. Hospital, Mumbai
Introduction: Arteriovenous (AV) fistulas are usually the first choice for vascular access in those undergoing HD, as they are more durable and have decreased risk for infection in comparison with AVGs or venous catheters. A complication of AVFs is significant outflow stenosis or obstruction which can be treated with Percutaneous Angioplasty.
Methods & Results: We present a constellation of 3 cases of juxta AVF outflow stenosis treated with PTA. An elderly male, CKD on MHD with Right elbow brachio-basilic fistula as access for 2 years presented with ipsilateral upper limb swelling with difficulty cannulation for hemodialysis. Fistulogram revealed 3.6mm narrowing in basilic vein in mid arm and AVF was seen draining through other collaterals. Post PTA flow across improved across stenosed segment, with PSV improved from 270cm/s to 378cm/s.
Conclusion and Discussion: An elderly female, c/o ADPKD on MHD with left forearm AVF for 3 years presented with access failure which on examination was found to have poor flow through AVF. Fistulogram showed focal severe (>90%) short segment stenosis of cephalic vein. She was taken up for balloon angioplasty. Post procedure flow improved with PSV of 275cm/s. One year later AV fistula is having good flow on dialysis. Another young male, k/c/o CKD on MHD since Feb 2023, with access as TCC. Later left forearm BCF was created which was showing non maturation even after 2 months of surgery which later on fistulogram was found to have cephalic vein narrowing and managed with balloon venoplasty, following which flow across AVF improved. Patient is now receiving dialysis with AVF. AV fistula outflow stenosis a not so rare complication can be seen in both short term and long term. Role of clinical examination of access and AVF surveillance plays important role for planning early and appropriate treatment thus avoiding secondary AVF failures. While short term management with angioplasty has shown promising results recurrence and restenosis still form major challenges and use of drug eluting balloons has been in research in last few years.
References
1. Sarala S, et al Cephalic Arch Stenosis: Location of Stenosis in Indian Hemodialysis Patients. Indian J Nephrol. 2018 Jul-Aug;28(4):273-277
2. Risk Factors of Arteriovenous Fistula Stenosis of Patients with Maintenance Hemodialysis Meiling Gao and Jing Wang; Evidence-Based Complementary and Alternative Medicine Volume 2022
Introduction: Central venous catheter placement is often requiring in patients needing renal replacement therapy. Catheter dysfunction due to thrombotic occlusion is a potential serious problem often resulting in catheter removal needing further access placement hospitalisation adding to cost and increased morbidity
Methods & Results: 53-year-old female k/c/o type 2 DM and HTN for 15 years. Initially started on HD with temporary catheter-initiated PD, developed peritonitis, reinitiated on HD, developed catheter dysfunction with blood flow of 200 ml/min. After ruling out catheter displacement and confirming clot in situ she was given tPA Alteplase as per protocol.
Conclusion and Discussion: Thrombolysis using local installation of various thrombolytic agents can be tried to salvage these HD CV catheters especially in patients who are having difficulty in achieving permanent access
Acknowledgement
This case report wouldn’t have been possible without the guidance of my consultants and seniors and lab technicians and patient and their attendants
Where there is a Will there is a way”: Case Reports and Discussion of Etiologies, Diagnosis and Treatment Strategies in CKD patients with access site failures secondary to insertion of TCC
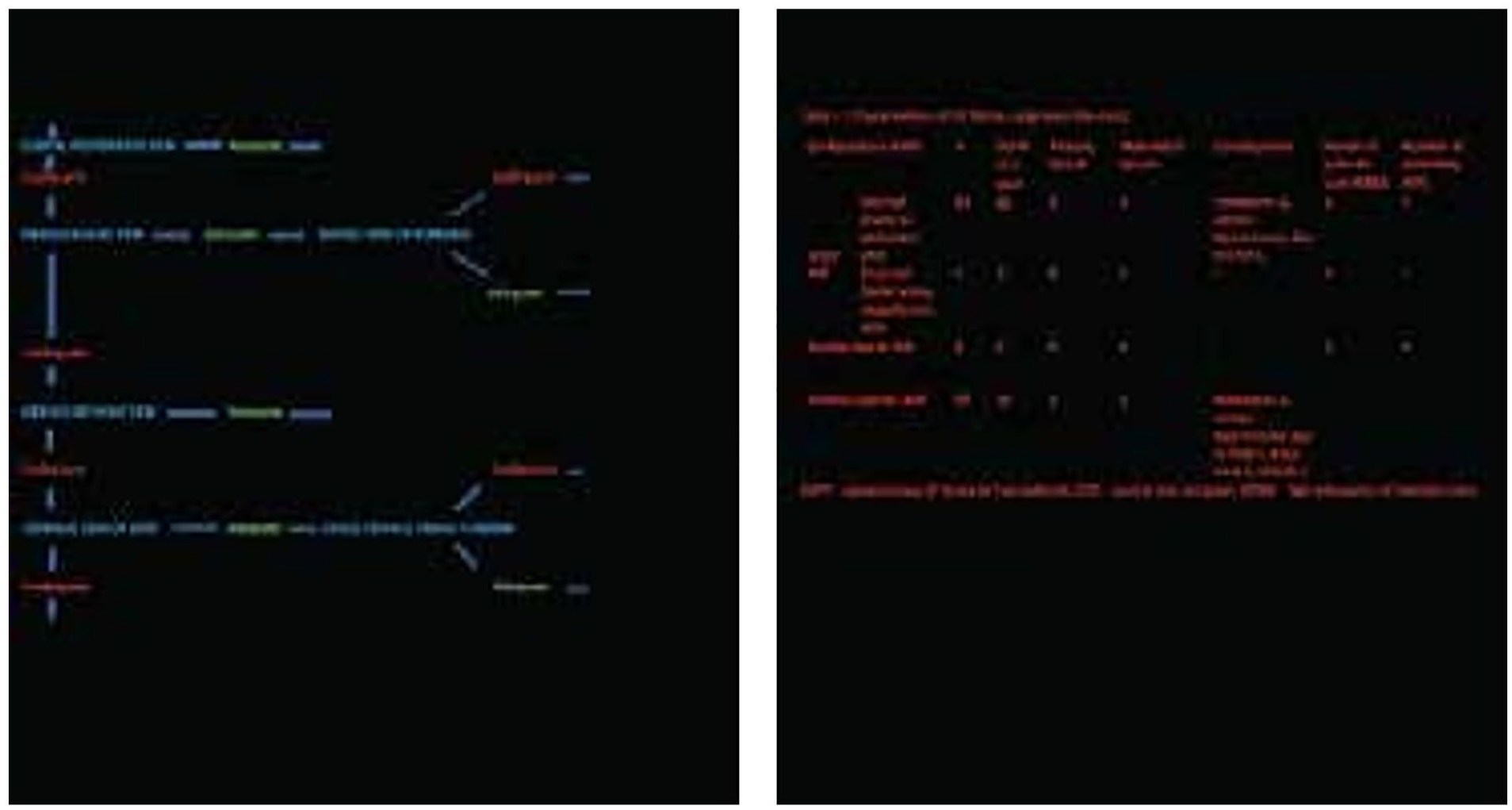
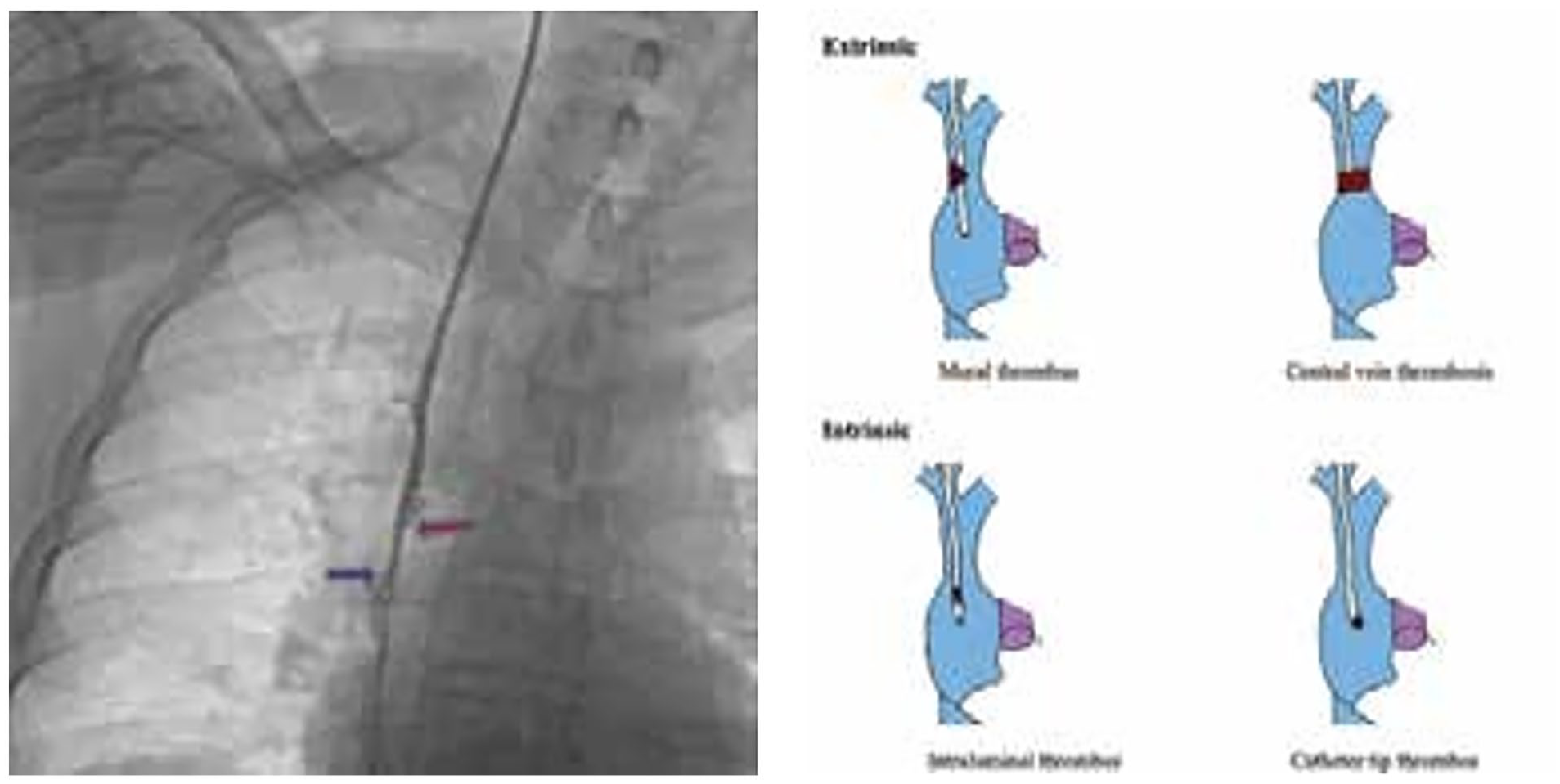
Introduction: Tunneled Cuffed Catheters (TCC’s) are silicon or polycarbonate-polyurethane copolymer based wide bore dual lumen catheters which are commonly used for the initiation of hemodialysis in CKD patients. One of the important long-term complications associated with TCC insertion is development of the central vein thrombosis which can be extrinsic / intrinsic
Methods & Results: A retrospective descriptive study was performed; a total of 25 CKD patients with prior TCC placement, from June 2022 to February 2023, presented with signs & symptoms of the central vein stenosis / occlusion / thrombosis leading to inadequate HD. 15 patients had extrinsic causes and 10 patients had intrinsic causes of the central vein occlusion leading to TCC failure. All 25 patients were successfully recanalized & TCC restored for HD.
Conclusion and Discussion:
Aims and Objectives - 1. To understand the etiology and establish the diagnosis of central vein thrombosis / occlusion / stenosis secondary to the TCC placement 2. To explore few possible ways for central vein recanalization in patients with access site failures, in order to continue hemo-dialysis Access site failures secondary to insertion of TCC (Tunneled Cuffed Catheter) are commonly seen and encountered in CKD patients. This can have various causes which needs quick attention and treatment. The goal of treatment should be restoration of the access for HD through the native site if possible. Because of the complexity of these cases, a team approach involving trained interventional radiologist and nephrologists would be beneficial and serve to improve patient care. In our short study, all 25 CKD patients had access site failures and efforts were made to restore the primary access site for the continuation of the HD. This report illustrates the common causes associated with access site failures and few ways to treat them in order to benefit the patient for the restoration of the access site and continuation of HD.
Acknowledgement
1. Dr. Anagha R Joshi, Prof & HOD, Department of Radiology, LTMG Hospital 2.Dr Mayuri Trivedi, Prof & HOD, Department of Nephrology, LTMG Hospital
References
1. Varughese S, Abraham G. Chronic kidney disease in India: A clarion call for change. Clinical Journal of the American Society of Nephrology. 2018 May 7;13(5):802-4,
2. Miller LM, Clark E, Dipchand C, Hiremath S, Kappel J, Kiaii M, Lok C, Luscombe R, Moist L, Oliver M, MacRae J. Hemodialysis tunneled catheter-related infections. Canadian journal of kidney health and,
3. El Khudari H, Ozen M, Kowalczyk B, Bassuner J, Almehmi A. Hemodialysis catheters: update on types, outcomes, designs and complications. InSeminars in Interventional Radiology 2022 Feb (Vol. 39)
4. Napalkov P, Felici DM, Chu LK, Jacobs JR, Begelman SM. Incidence of catheter-related complications in patients with central venous or hemodialysis catheters: a health care claims database analysis.
5. BM Beigi AA, Sharifi A, Gaheri H, Abdollahi S, Esfahani MA. Placement of long-term hemodialysis catheter (permcath) in patients with end-stage renal disease through external jugular vein. Advanced biomed,
Right External Jugular Vein and Left Internal Jugular vein as Alternative Access for Right Internal Jugular vein for Tunneled Dialysis Catheter: A Prospective Comparative Study
Vineet Behera, G Shanmugraj, Rohith KP, Prabhat C
INHS Asvini, Mumbai
Right internal jugular vein (RIJV) is the commonest site for tunneled dialysis catheter (TDC). After exhaustion of RIJV, left internal jugular vein (LIJV), right external jugular vein (REJV), or other veins, may be used. This prospective study compared the clinical profile and outcomes of TDC in REJV vs LIJV.
A prospective non-randomized single center study included ESRD patients on with TDC, with exhausted RIJV while patients with SVC occlusion, or unwilling were excluded. Patients with patent REJV/ right BCV underwent REJV TDC. Patients with occluded REJV/ right BCV underwent LIJV TDC. Primary outcome was cumulative catheter patency (insertion to removal of TDC), while secondary outcomes was primary catheter patency (insertion to TDC catheter dysfunction) and CRBSI. Appropriate IEC approval and patient consent was obtained.
Fifty patients were included in study with 23 (46%) in REJV arm and 27 (54%) LIJV arm, with mean age 48.6±4.5 years, 28 (56%) males, 24 (48%) diabetes; mean duration of RIJV 178.6±34.5 days (similar in both groups). Primary outcome of catheter removal occurred in 10 (37%) in LIJV arm and in 04 (17.3%) in REJV arm (HR 0.67, 95% CI: 0.62-0.97, p=0.008); while cumulative patency was 262.6±39.5 days in LIJV arm and 335.6±49.5 days in REJV arm (p=0.04). Amongst LIJV and REJV, catheter dysfunction needing attention was seen in 14(51.8%) and 6(26%) (HR 0.79, 95% CI: 0.72-1.32, p=0.02); while CRBSI was seen in 7(25.9%) and 4(17.3%) (HR 0.92, 95% CI: 0.42-1.44, p=0.3), respectively. The factors predisposing to cumulative catheter patency were studied using Cox proportional hazards model, and duration of previous dialysis catheter (HR 2.24, 95% CI: 1.42-3.72, p=0.02) and central vein thrombosis (HR 1.89, 95% CI: 1.33-4.32, p=0.04), were statistically significant. Conclusion: Rt EJV access is superior to left IJV as an alternate insertion route for TDC in patients of ESRD on hemodialysis with exhausted RIJV.
Predictors For Patency of Access After 1 Year Of Initiation On Hemodialysis In Elderly
Aiswarya Kosaraju, Ramprasad E, Sandhya Suresh
Sri Ramachandra Institute of Higher Education and Research Centre
The demography of the global population is changing recently. Elderly population has increased and their incidence in ESRD registries worldwide is on rise. The optimal vascular access for elderly patients remains a challenge due to difficult balance between risks and benefits in a population with increased comorbidity and decreased survival.
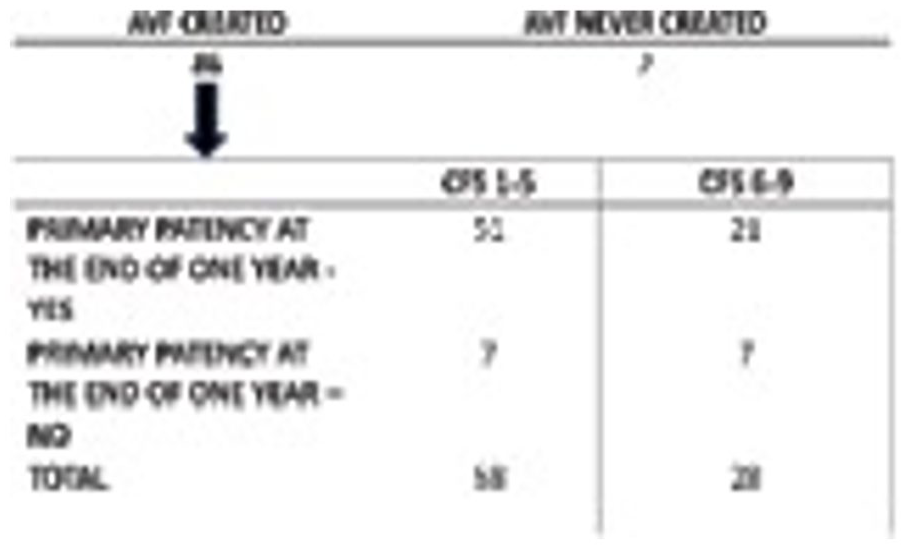
This is an observational study done in Sri Ramachandra University, Chennai over a period of one year. 88 Ederly patients ( >65 years ) who were initiated on long term Hemodialysis(HD) were studied. Frailty was assessed according to CFS (Clinical Frailty score). Majority of patients had high CFS. At the end of 1-year, Primary Patency and Secondary Patency was estimated. Higher rate (50%) of Access Failure was seen with CFS >6.
A well-functioning VascularAccess is crucial for good HD. Elderly patients are usually affected by comorbidities like Diabetes, Coronary Artery Disease(CAD), etc that can impair the outcome of the access. Increased age has been associated with non-maturing fistula with more than doubling of the risk in those age >65 years(1). The reported prevalence of frailty in patients with HD varies widely, ranging from 21% to 73%(2,3). Patients with higher CFS score(>5) had higher risk of access failure (25%) at 1 year compared to those with lower CFS score (12%, p = 0.211), although the difference was not significant. However it was noted that even the group with moderate and severe frailty had primacy patency rate of 75% of their first AV access at one year. Therefore, this data suggests that higher degrees of Frailty does not preclude the placement of an AV access.
Primary Patency at one year did not corelate with CAD, DM, biochemical values like Calcium, Phophorus and albumin. Higher degrees of Uremia was associated with greater risks of Access Failure. In conclusion, Frailty is associated with poor dialysis vascular access outcomes. Further research should focus on the assessment and interventions for frailty to optimize the process of caring for dialysis vascular access portals.
Acknowledgement
I would like to thank all the patients that have cooperated in the study and my Head of Department Ramprasad and guide Dr Sandhya Suresh.
References
1. Lok CE, Allon M, Moist L, Oliver MJ, Shah H, Zimmerman D. Risk equation determining unsuccessful cannulation events and failure to maturation in arteriovenous fistulas (REDUCE FTM I) J Am Soc Nephrol
2. Bao Y, Dalrymple L, Chertow GM, et al. Frailty, dialysis initiation, and mortality in end-stage renal disease. Arch Intern Med. 2012;172:1071–1077
3. Lee SY, Yang DH, Hwang E, et al. The prevalence, association, and clinical outcomes of frailty in maintenance dialysis patients. J Ren Nutr. 2017;27:106–112,
Outcome Of Central Venoplasty and Fistuloplasty In A Tertiary Care Centre In Eastern India
Introduction: Access crisis is the Achilles heel of dialysis in ESRD patients. Central vein stenosis (CVS) and AVF failure are common and negatively impact the quality of dialysis and quality of life in CKD patients. Here we report the outcome of central venoplasty and fistuloplasty in our centre.
This was a retrospective observational study done from January’21 to October 22. Minimum follow up-6 months. Central venoplasty was preceded with venography. Right/left common femoral and venous limb of fistula were used as access, sometimes ipsilateral internal jugular vein is also used as third access. arterial limb preferably radial artery used as access for fistuloplasty. Total 38 primary venoplasty and 5 secondary interventions performed, fistuloplasty performed in 21 cases.
In cases of CVS 42.1% patients had tunneled catheter, 52.6% had AVF and 5.3% had temporary catheter. 73.7%patients had access failure, 26.3% had upper limb swelling. mean dialysis vintage-1.87yrs. 73.7% had CRBSI episodes of >3. Mean duration to develop CVS-34.5m(SD-13.6m). For central venoplasty-32(84.2%) were successful and 15.8% failed. Restenosis developed in 7 (18.4%). These cases had multiple collaterals, long segment chronic thrombus in venography, presented late (>3 months), had T2DM and hypertension. Mean duration to develop restenosis-105.3d(SD-53.6 d). minor bleeding occurred in 15.8%, profuse bleeding-5.3%, stent placement was done in 2 patients for venous rupture and recurrent stenosis.1 patient died immediate post procedure due to stent migration and sudden cardiac death. 21 patients undergone Fistuloplasty. RCF -57.14%, BCF -28.57%, BBF-14.28%. Mean patency of AVF-1.03Y. Fistuloplasty was successful in 85.7% and 3 failed having long segment narrowing, extensive collaterals, very late presentation, had diabetes and hypertension. Mean fistula flow volume-110.4(SD79ml/min(preprocedure),738ml/min(SD-244.9 ml/min)(post-procedure). Restenosis- 4 cases. mean duration to develop restenosis -104.5d. secondary fistuloplasty-3 cases. minor bleeding occured in 6 cases, venous rupture in 2 and radial artery pseudoaneurysm in 1 case.
This outcome analysis suggests, for CVS and AVF failure, endovscular procedures have good outcome, cost and restenosis remain the main limiting factor.
Acknowledgement
Department of radiology, ipgmer and sskm hospital.
References
1. Cuthbert GA, Lo ZJ, Kwan J, Chandrasekar S, Tan GWL. Outcomes of Central Venoplasty in Haemodialysis Patients. Ann Vasc Dis. 2018 Sep 25;11(3):292-297. doi: 10.3400/avd.oa.18-00025. PMID: 30402178; PMCID: PMC6200608.
2. Ozyer U, Harman A, Yildirim E, Aytekin C, Karakayali F, Boyvat F. Long-term results of angioplasty and stent placement for treatment of central venous obstruction in 126 hemodialysis patients: a 10-year single-center experience. AJR Am J Roentgenol. 2009 Dec;193(6):1672-9. doi: 10.2214/AJR.09.2654. PMID: 19933663.
3. Ibrahim, Hilman; Muradi, Akhmadu; and Limianto, Eka A. (2021) "Outcomes of Percutaneous Transluminal Angioplasty for Central Vein Stenosis in Hemodialysis: A Literature Review," The New Ropanasuri Journal of surgery.
Endoluminal balloon dilatation procedure for removal of a stuck tunneled cuffed haemodialysis catheter
Vivek Kothandaraman Koushik, Venkatesh Rajkumar
Apollo Hospitals, Chennai
Introduction: About 1% of tunnelled catheters may not be amenable to regular removal techniques and are labelled as stuck tunnelled catheters. Normally TCCs are removed by dissecting the dacron cuff to release the subcutaneous portion. Attempted forceful removal can lead to TCC fragmentation, embolization, central vein or right atrial tear.
Methods & Results: A 70 year female with myeloma and ESRD on HD through right IJ palindrome TCC for the past 7 years developed a CLABSI due to Pseudomonas. Planned TCC removal at bedside. Endoluminal balloon dilatation was considered for stuck catheter. A 5mm balloon through one of the limbs of the TCC but failed to pass through. TCC was cut close to exit and balloon was inserted, then dilated freeing the TCC from its adhesions. TCC removed.
Conclusion and Discussion: This technique prevented the patient from undergoing general anaesthesia/ major surgery and also the significant cost incurred during such surgery. The highlights of this case were that an endoluminal balloon dilatation was done through the exit site without neck dissection and a coronary wire and balloon used but even a low profile balloon could have been used.
Reference
Hong J.H. A breakthrough technique for the removal of a hemodialysis catheter stuck in the central vein: endoluminal balloon dilatation of the stuck catheter. J Vasc Access.2011;12(4):381–384.
Minimally invasive surgical removal of Tunnelled cuffed catheter (TCC) associated Right atrial clot: A report of 3 cases
Sudharshan Karthikeyan, Venkatesh Rajkumar
Apollo Hospitals, Chennai
Introduction: Majority of Catheter related right atrial thrombus (CRAT) are small, asymptomatic and are incidentally detected by Transthoracic or Transoesophageal ECHO. There is paucity of literature about the potentially fatal complication of CRAT in dialysis patients, and the optimal management is controversial
Methods & Results: Here we report 3 patients of end stage renal disease (ESRD) on regular hemodialysis with a TCC who all had evidence of Catheter related blood stream infection (CRBSI) with TEE showing thrombus. These patients were managed with broad spectrum IV Antibiotics. Infected clot retrieval via Right mini thoracotomy was performed on all 3 patients with removal of TCC. All these patients had good post-operative outcomes with better hemodynamic stability, shorter hospital stay, less bleeding risk
Conclusion and Discussion: CRAT is commonly noted in the IVC and RA junction. Differentiating thrombus from vegetation is important but difficult, hence early management with IV Antibiotics is crucial. Management options include catheter directed therapy (CDT), Surgical thrombectomy, systemic anticoagulation and thrombolysis. Early open surgical intervention is indicated when there are high risk features such as infected thrombi, large thrombus >5-6cms, multiple thrombi, failed anticoagulation therapy and thrombus extension with pulmonary embolism. Patients with ESRD are at a high risk of surgical complications but here we report good post operative outcomes for all patients with this approach of minimally invasive right mini thoracotomy for infected clot retrieval hence highlighting its importance in CRAT
References
1. Nasir Hussain, Paul Eric Shattuck et al, "Large Right Atrial Thrombus Associated with Central Venous Catheter Requiring Open Heart Surgery", Case Reports in Medicine, vol. 2012, Article ID 501303
2. David Ferreira, Anthony Le et al, "Surgical Management of Right Atrial Mass Associated with a Vascular Access Catheter", Case Reports in Cardiology, vol. 2020, Article ID 4590147, 3 pages, 2020.
Comparison of Taurolock solution with Heparin as lock solution of tunnelled catheter
Manzoor Ahmad Parry, Hamad Jeelani
Ministry of Health, Oman
Background: The use of dialysis catheters can result in catheter-related infections, which is a significant side effect that can lead to higher rates of hospitalization, morbidity, and mortality.1-3 Instead of heparin lock solution, use of citrate-taurolidine lock solution can lower the occurrence of catheter-related infections.4 This study was done to evaluate Citrate-taurolidine lock solution for decreasing catheter related infections.
Material and Methods: This retrospective study included 89 patients who received hemodialysis for at least 6 months via tunnelled catheter. The patients who received Taurolock (a solution of 1.35% taurolidine, 4% citrate, and 500 units/ml of heparin) were compared with patients who received Heparin lock solution (5000 IU/ml) for catheter related infection and catheter dysfunction. Patients were excluded from the study if they had previous catheter related infection, or if they had positive blood cultures within two weeks of Catheter placement.
Results: Out of 89 patients included in this study, 47 patients received Heparin lock solution and 42 patients received Taurolock lock solution. Over a period of 7560 catheter days, 1 patient in Taurolock group developed catheter related infection, while as over a period of 8140 catheter days 5 patients had catheter related infection in Heparin group, corresponding to 0.13 and 0.61 episodes of catheter related infections per 1000 catheter days respectively (an incidence rate ratio of 0.21, 95% confidence interval 0.04 to 0.54, P= 0.029). Catheter dysfunction rates were significantly less in Taurolock group compared to Heparin lock solution (1.05 vs 4.88/1000 catheter days). Also, two patients required removal of catheter in heparin group while as no patient required removal of catheter in Taurolock group.
Conclusion: Our study demonstrates higher incidence of catheter-related infections in the Heparin group compared to Taurolock solution and a significantly higher effectiveness of Taurolock solution in preventing catheter dysfunction over Heparin.
References
1. Butterly DW, Schwab SJ. Dialysis access infections. Current opinion in nephrology and hypertension. 2000 Nov 1;9(6):631-5.
2. Zhang J, Li RK, Chen KH, Ge L, Tian JH. Antimicrobial lock solutions for the prevention of catheter-related infection in patients undergoing haemodialysis: study protocol for network meta-analysis of randomised controlled trials. BMJ open. 2016 Jan 1;6(1):e010264.
3. Oliver MJ, Callery SM, Thorpe KE, Schwab SJ, Churchill DN. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: a prospective study. Kidney international. 2000 Dec 1;58(6):2543-5.
4. Liu H, Liu H, Deng J, Chen L, Yuan L, Wu Y. Preventing catheter-related bacteremia with taurolidine-citrate catheter locks: a systematic review and meta-analysis. Blood purification. 2014;37(3):179-8
Outcome of Tunnelled Haemodialysis Catheter-Related Bloodstream Infections
Catheters are used in roughly 60-80% of patients at the time of initiation and 25-30% of all prevalent patients as a bridge to permanent vascular access.[1] The present study investigates the causative organisms and the survival outcome of tunneled catheter-related bloodstream infections (CRBSI) in hemodialysis patients.
It was a retrospective cross-sectional study carried out in a tertiary care hospital in north India. It included adult (>18 years) ESRD patients diagnosed with HD CRBSIs between January 2020 to December 2022. The diagnosis of CRBSI was based on the clinical presentation of fever, chills and/or hypotension and any of the following two criteria: 1. Same organism recovered from percutaneous blood culture and from semi-quantitative roll-plate culture (>15 colony forming units) of the catheter. Out of 54 suspected cases of CRBSI, 35 cases of infection were reported in 29 subjects. In our study, the incidence of CRBSI was 6.67 episodes per 1000 catheter days. Gram-positive and gram-negative organisms were reported in 18 and 16 patients respectively (table 1). A non-significant trend of higher mortality was seen in gram-negative infections, (p-value 0.162). No significant differences in demographic or biochemical variables were seen in surviving and non-surviving subjects (table 2). The long-term duration of tunnelled catheter stay was a uniform feature in both groups of patients. 94% (34) of patients reported chills during dialysis sessions whereas fever was reported by 85% (30) of subjects. Infections resulted in catheter removal in 12 subjects while the rest of the infections were managed with intravenous antibiotics and antibiotic locks.
In hemodialysis patients with a catheter as vascular access presenting with fever, the first differential diagnosis is CRBSI. Higher mortality associated with rising gram-negative infections should be kept in mind. The catheter can be salvaged in most patients without severe infection.
Reference
1. Allon M. Dialysis catheter-related bacteremia: treatment and prophylaxis. Am J Kidney Dis. 2004 Nov;44(5):779-91. PMID: 15492943,
Rescue Therapy of An Irretrievable Tunneled Cuffed Hemodialysis Central Venous Catheter
Introduction: Tunneled cuffed hemodialysis catheters have protected effective long-term alternatives in patients who have exhausted or failed other vascular access options (1,2). Long term catheter use can lead to serious sequelae of infection, thrombosis, central vein stenosis and mechanical dysfunction (3). Rarely, catheters can become firmly adhered to a vessel.
Methods & Results: A 33-year-old female with ESRD with a 5-year dialysis vintage. She had complicated vascular access history and had left sided IJV TCC as vascular access which was in situ since last 2 years. She was admitted with CRBSI and poor flow from arterial port of Left IJV TCC. TCC removal procedure revealed catheter stuck to a vessel wall and required surgical removal along with part of SVC which was reconstructed with autologous pericardial patch.
Conclusion and Discussion: Stuck catheter is a rare complication but its frequency will very likely increase in the future. The catheter adherence to the vessel wall should be recognized as a serious complication. In such cases, forceful traction can cause vascular injury, or fracture of the catheter. In cases of indwelling catheters for extended periods, appropriate preparation should be made in anticipating this complication during removal- this may include forewarning the anesthesiologist regarding a potentially longer procedure, ensuring necessary endovascular and imaging equipment is available, and the access to a cardiothoracic surgery. Prophylactic catheter exchange should be considered to avoid such serious complication.
References
Rayner, H. C. & Pisoni, R. L. Te increasing use of hemodialysis catheters: evidence from the DOPPS on its significance and ways to reverse it. Semin Dial. 23, 6–10 (2010)
Aitken, E. L. et al. Te use of tunneled central venous catheters: inevitable or system failure? J Vasc Access. 15, 344–350 (2014)
Little MA, O’Riordan A, Lucey B et al. A prospective study of complications associated with cuffed, tunneled hemodialysis catheters. Nephrol Dial Transplant 2001; 11: 2194–2200
Miller LM, MacRae JM, Kiaii M, et al. Hemodialysis tunneled catheter noninfectious complications. Can J Kidney Health Dis. 2016; 3:2054358116669130
Forneris G, Savio D, Ǫuaretti P, Fiorina I, Cecere P, Pozzato M, Trogolo M, Roccatello D: Dealing with stuck hemodialysis catheter: state of the art and tips for the nephrologist. J Nephrol 2014
Comparative Study of Kt/V In Various Hemodialysis Machines
Mohammed Saif, Shaikh Jason Samuel, Neetu Dubey
Apex Kidney Care Hospital, Delhi
Introduction: To determine the comparison of various hemodialysis machines based on Kt/V, cumulative blood volume and blood flow rate.
Methods & Results: It is to relate the cumulative blood volume and Kt/V on various hemodialysis machines, to relate the impact of blood flow rate on Kt/V in various hemodialysis machines and to relate the dialysis duration on Kt/V in various hemodialysis machines.
Conclusion and Discussion: The sample size of the study is 1500 hemodialysis sessions. The equipments used were Hemodialysis machines like Fresenius medical care (4008 S NG) Nipro (Surdial 55 plus) and BBraun (Dialog+ plus), the dialyzer’s surface area used were 1.6 m2, 1.7 m2, F7 HPS, F8 HPS, F4 HPS and DORA. The mean Kt/V is low in BBraun hemodialysis machine. The Kt/V drops as number of dialyzer reuse increases. Hence Kt/V is directly proportional to blood flow rate and cumulative blood volume.
Acknowledgement
I am thankful to Sudhir Bagarao sir, for their expertise and assistance in statistical work. I would also want to thank Apex Kidney Care-ASDT.
References
1. Miskulin D, Bragg-Gresham J, Gillespie BW, Tentori F, Pisoni RL, Tighiouart H, et al. Key comorbid conditions that are predictive of survival among hemodialysis patients.
2. National Kidney Foundation. KDOǪI Clinical Practice Guideline for Hemodialysis Adequacy:2015 update. Am J Kidney Dis. 2015;66(5):884–930. doi:10.1053/j.ajkd.2015.07.015.
3. Sternby J, Daugirdas JT. Theoretical basis for and improvement of Daugirdas’second generation formula for single-pool Kt/V. Int J Artif Organs. 2015;38(12):632–637. doi:10.5301/ijao.5000456.
Ipos Renal: Tool To Unveil Common But Undetected Symptom Burden To Enhance Patient Care And Health Outcomes In Chronic Kidney Disease
Md Samiul Akhtar, Manisha Sahay, Kiranmai Ismal
Osmania Medical College & General Hospital, Hyderabad
Introduction: Renal failure is a chronic disease that can seriously affect quality of life (ǪOL) [1-3]. ǪOL has become an important indicator of healthcare, patient experience, and measure of effectiveness in end stage kidney disease (ESKD)[4].
Patients receiving maintenance hemodialysis experience significant symptom burden that is often undetected and hence under-treated.
Methods & Results: Patient scores were collated from responses of 97 CKD patients undergoing maintenance hemodialysis at Osmania General Hospital by using IPOS-renal patient version. The average age of the patient was 44.30 ±11.59. There were 61 males (62.8%) and 36 female (37.2%) patients. Results showed Difficulty in Sleeping 50%, Pain 47.6%, Weakness or lack of energy 45.2%, Poor mobility 30.9%, anxiety 59% and depression 43% and 22% of participants unable to share their feelings with family/friends.
Conclusion and Discussion: ǪOL is defined as “An individual perception of their position in life in the context of culture and value system where they live, and in relation to their goals, expectations, standards, and concerns [4].” Patients with CKD may experience a negative impact on their ǪOL, due to anxiety that can appear before and during the treatment [1]. Loss of freedom, dependence on caregiver, disruption of marital, family, and social life; and reduced or loss of financial income negatively affect ǪOL [5]. In this study, our aim was to evaluate the ǪOL of patients with ESKD undergoing maintenance hemodialysis (MHD). Difficulty in sleeping (50%) followed by Pain (47.6%) and weakness or lack of energy (45.2%) was 3 major physical symptom burdens. Anxiety (59%) was the most common psycho- logical as well as overall most common symptom burden. The evaluation of the ǪOL in CKD patients undergoing hemodialysis showed that it was relatively compromised. IPOS review highlighted the areas of concern for CKD patients, routinely not identified and hence under-treated which may support healthcare professionals when measuring and managing the potential symptoms burden associated with CKD and referral to various services such as chronic pain clinic, physiotherapist and social worker to help patients.
Acknowledgement
I am extremely grateful to Dr. Prof Manisha Sahay (HOD) and Dr. Prof Kiranmai Ismal for continuous motivation and guidance to conduct the present study.
References
1. Theofilou PA. The impact of socio demographic and psychological variables on quality of life in patients with renal disease: Finding of a cross sectional study in Greece. World J Nephrol Urol 2012;
2. Ginieri Coccossis M, Theofilou P, Synodinou C, Tomaras V, Soldatos C. Ǫuality of life, mental health and health beliefs in haemodialysis and peritoneal dialysis patients: Investigating differences
3. Theofilou P. Ǫuality of life in patients undergoing hemodialysis or peritoneal dialysis treatment. J Clin Med Res 2011;3:1328.
4. Ravindran, et al.: Assessment of quality of life among end stage renal disease patients undergoing hemodialysis in Indian population; 2020 Indian Journal of Palliative Care.
5. Sathvik BS, Parthasarathi G, Narahari MG, Gurudev KC. An assessment of the quality of life in hemodialysis patients using the WHOǪOL BREF questionnaire. Indian J Nephrol 2008;18:141 9,
Primary Caregiver Burden Between In-Center Hemodialysis And Home Hemodialysis
Gargi Ajay Khanvilkar, Jason Samuel, Neetu Dubey
Apex Kidney Care, Delhi
Introduction: The main aim of the study is to identify the primary care giver burden for in center HD and home HD.
Methods & Results: 100 caregivers of in-center hemodialysis patients and 50 home hemodialysis patients from AKC, were assessed by using Burden assessment scale questionnaire. Based on the questionnaires we assessed the burden levels of caregivers in 3 ratings. 1- Not at all, 2- A little, 3- A lot. The result for the questionnaires is based on the rating scale from 1 to 5. The level of burden is 15% for home hemodialysis and 35% for in-center hemodialysis.
Conclusion and Discussion: The questionnaires are categorized into personal, social, financial, psychological and clinical implications (for home HD). The high level of caregiving stress is experienced by hemodialysis primary caregivers and has a negative impact on their quality of life. It is advised that more consideration be given to the requirements of caregivers and that they receive enough social, economic, physical, and psychological counseling.
Acknowledgement
I am thankful to Sudhir sir for his expertise and assistance in statis- tical work. I would also want to thank AKC-ASDT.
References
1. Fekete C. Caregiver Burden. In: Wright JD, editor. International Encyclopedia of the Social & Behavioral Sciences (Second Edition). Oxford: Elsevier; 2015
2. Alvarez-Ude F, Valdés C, Estébanez C, Rebollo P; FAMIDIAL Study Group. Health-related quality of life of family caregivers of dialysis patients. J Nephrol. 2004 Nov-Dec;17(6):841-50. PMID: 155
Depression In Dialysis Patients
Priyanka Muthukrishnan Yadav, Jason Samuel, Neetu Dubey
Apex Kidney Care, Delhi
Introduction: Regular dialysis will alter the patient’s daily routine and have an effect on their biopsychological quality of life for the majority of renal patients. Even without depression, life with dialysis is difficult. The early diagnosis and treatment and have an effect on ǪOL of dialysis patients.
Methods & Results: The research survey was carried out in the form of anonymous generic questionnaires. The Yesavage depression scale was used for the evaluation. 100 patients were involved at our AKC dialysis centers in Mumbai. We evaluated the level of depression overall as well as the level of individual patients and divided them into three groups. 65% do not suffer 23% are mild and 11% have severe Depression.
Conclusion and Discussion: One of the issues is that severe kinds of depression (11%) are challenging to identify objectively if the patient refuses to acknowledge it. This is reflected in the behavior of these patients and their lack of Cooperation with medical staff. The research’s findings have undergone further analysis, and they will be used as one of the foundations for incorporating this problem into the integrated care concept’s strategy and as a result, raising the standard of care offered at the facility. The investigation verified that there is depression at our dialysis facility. Our recommendation is to implement early mental health screening for new dialysis patients in order to raise the standard of healthcare.
The regular screening must involve the use of structured questionnaires. As part of multidisciplinary care, we also advise a psychologist to visit the center frequently. Patients have difficulty visiting psychiatric facilities outside of the dialysis center, according to experience. Patient non-cooperation will be reduced because to early detection and consistent team support, but the standard of living for dialysis patients will also increase.
Acknowledgement
I am thankful to Sudhir Bagarao sir, for his expertise and assistance in statistical work. I would also want to thank AKC-ASDT.
References
1. Havins WN, Massman PJ, Doody R. Factor structure of the Geriatric Depression Scale and relationships with cognition and function in Alzheimer’s disease. Dement Geriatr Cogn Disord. 2012;34(5-6):360-72. doi: 10.1159/000345787. Epub 2012 Dec 13. PMID: 23235472.
2. Alden D, Austin C, Sturgeon R. A correlation between the Geriatric Depression Scale long and short forms. J Gerontol. 1989 Jul;44(4):P124-5. doi: 10.1093/geronj/44.4.p124. PMID: 2738314.
Early Renal Artery Rupture – A Rare But Devastating Complication Post Kidney Transplant Early Renal Artery Rupture – A Rare But Devastating Complication Post Kidney Transplant
Selvin Sundar Raj Mani, Athul Thomas, Manish Lalwani, Sudhindra J, Suceena Alexander, Santosh Varughese, Vinoi George David
Christian Medical College, Vellore
Introduction: Immediate Vascular complications are rare in kidney transplant. In this case report, we describe a rare case of early arterial rupture post kidney transplant.
Methods & Results: A 36 years old live related ABO compatible kidney transplant recipient developed Pseudomonas sepsis on day 5. On post operative day 6, she developed sudden onset abdominal pain with hemorrhagic drain output of 2 liters. On exploration, she had necrotic defect in the graft arterial wall with active bleeding requiring removal and storage in HTK solution. After stabilization, she underwent successful repeat left iliac fossa kidney transplantation. However, she succumbed to ventilator associated pneumonia.
Conclusion and Discussion: Immediate vascular complication is uncommon (1.3%) following kidney transplant. The complications include vascular kinking, torsion renal artery or vein thrombosis. Renal artery rupture is a rare life-threatening complication, mostly described in the literature as either case report or case series. It is mostly caused by infection followed by surgery related complication. Common organisms described in the literature include Staphylococcus aureus, Candida, Klebsiella or Pseudomonas which may be either donor derived infection, urosepsis or catheter related infections. Early institution of antimicrobial therapy may prevent such complication. High clinical suspicion is warranted to identify arterial rupture.
Warning symptoms include abdominal discomfort, sudden increase in drain output and new onset hypotension. Treatment usually involves emergency exploration and achievement of hemostasis. Graft may be salvaged and repeat transplantat can be attempted at a later stage. Our patient, despite salvage of the graft succumbed to a hospital acquired infection. To summarize, rupture of a graft artery is a potentially devastating complication which may result in graft loss and even death. Prompt recognition and emergency exploration is crucial.
References
1. Dimitroulis D, Bokos J, Zavos G, Nikiteas N, Karidis NP, Katsaronis P, Kostakis A. Vascular complications in renal transplantation: a single-center experience in 1367 renal transplantations and review of the literature. Transplant Proc. 2009 Jun;41(5):1609-14. doi: 10.1016/j.transproceed.2009.02.077. PMID: 19545690.
2. Lin YH, Liao CH, Jiang BJ, Chen TH. Early renal arterial rupture and arterial pseudoaneurysm in graft kidneys from the same deceased donor. Ci Ji Yi Xue Za Zhi. 2018 Oct-Dec;30(4):250-254. doi: 10.4103/tcmj.tcmj_180_17. PMID: 30305791; PMCID: PMC6172893.
3. Tavakkoli M, Zafarghandi RM, Taghavi R, Ghoreifi A, Zafarghandi MM. Immediate Vascular Complications After Kidney Transplant: Experience from 2100 Recipients. Exp Clin Transplant. 2017 Oct;15(5):504-508. doi: 10.6002/ect.2016.0057. Epub 2016 Dec 2. PMID: 27915961.
Assessment of nutritional status of dialysis patients in routine clinical practice
Krishnapriya Vadlapatla, Bharat V Shah
Global Hospital, Mumbai
Introduction: Nutrition among dialysis patients, a common predictor of mortality, is assessed comprehensively by Subjective Global Assessment (SGA) score, which is time consuming and not practical to follow in routine clinical practice. We studied a more pragmatic tool- the Simple Objective Assessment (SOA) and have compared its performance with SGA.
Methods & Results: 54 adult patients who were on hemodialysis for at least 6 months with no active infection or malignancy were included and their nutritional status was assessed by SGA and SOA scoring systems. SGA score consists of 7 variables, while the SOA score consists of change in weight and serum albumin over 6 months as parameters. There was good correlation between the two scoring methods with an R value of 0.85.
Conclusion and Discussion: Periodic assessment of nutritional status is important in hemodialysis patients. Most widely accepted method is SGA. However, this is time consuming, needs dedicated personnel and not practical in routine clinical practice. Our study shows that SOA using delta weight and delta albumin over 6 months provides as good information as SGA (R 0.85) and is easy to implement in routine clinical practice.
Acknowledgement
I am extremely grateful to my mentor Dr Bharat Shah and Nutrition specialist Dr Zamrudd Patel for helping and guiding me throughout the project.
References
1. Tapiawala. S, Vora.H, Patel.Z, Badve.S and Shah.B. Subjective Global Assessment Of Nutritional Status Of Patients With Chronic Renal Insufficiency And End Stage Renal Disease On Dialysis. 2006. JAPI;
2. Piratelli.C.M and Junior.R.T. Nutritional Evaluation Of Stage 5 Chronic Kidney Disease Patients On Dialysis. 2012. Sao Paulo Med J;30 (6): 1516-3180.
Study Of Sleep Apnea in Patients on Hemodialysis at A Tertiary Care Centre
Irawati Rajiv, Waghmare Dash, Sudhiranjan, Amjadkhan Pathan, Ashay Shingare Deshpande, Rushi Bahadur M M, Ashwin Patil
Jaslok Hospital and Research Centre, Mumbai
Introduction: The prevalence of sleep apnea in ESRD patients is reported to be 50%-80%, higher than the general population.(1-5) Sleep apnea, a modifiable risk factor, contributes to the cardiovascular morbidity and mortality in dialysis patients. This study aims to determine the prevalence of sleep apnea in hemodialysis patients at our Centre.
Methods & Results: This study was a cross-sectional, observational study, over one year involving 54 patients. All the patients were on maintenance hemodialysis for at least three months. Patients with underlying condition affecting results of polysomnography test were excluded. All patients underwent polysomnography and 2D-echocardiography. The prevalence of sleep apnea was found to be 72.3%. Majority of the patients were asymptomatic. Weight and BMI were not found to risk factors. Results summary in Table 1.
Conclusion and Discussion: Sleep apnea was prevalent in 72.3% of patients in this study. The traditional risk factors for sleep apnea in the general population were not seen in the hemodialysis population in this study and majority of the patients diagnosed with sleep apnea were asymptomatic for the same. Sleep apnea and its severity were associated with older age and there was no association of sleep apnea with weight, BMI, gender predisposition, diabetes mellitus or hypertension. Majority of the patients with sleep apnea had mild disease in this study (51.3% of the patients with sleep apnea). A greater number of patients with sleep apnea had left ventricular hypertrophy and pulmonary hypertension as compared to the patients without sleep apnea. Sleep apnea is underdiagnosed in the ESRD population group. The current study intends to gauge the prevalence of sleep apnea in hemodialysis population which is often missed, although it is a modifiable risk factor amenable to intervention. Early diagnosis of sleep apnea can help in reducing the adverse cardiovascular risk in hemodialysis patients which is the major cause of increased mortality in this population. A high index of suspicion and a low threshold for diagnosis should be kept for diagnosing the disease.
Acknowledgement
I would like to thank Dr Susheel Bindroo, Consultant department of Respiratory medicine and my colleagues, Shaurya Mehta and Harsh Shah for their support.
References
1. Hanly P. Sleep disorders and end-stage renal disease. Curr Opin Pulm Med. 2008;14(6):543-550.
2. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230-1235
3. West SD, Nicoll DJ, Stradling JR. Prevalence of obstructive sleep apnoea in men with type 2 diabetes. Thorax.
6. Huang Z, Tang X, Zhang T, Ǫiu S, Xia Z, Fu P. Prevalence of sleep apnoea in non-dialysis chronic kidney disease patients: A systematic review and metaanalysis. Nephrology (Carlton). 2019;24(10):1041-1
Peritoneal dialysis associated peritonitis - A study of clinical features and predictors of outcome
Sairam B, Sreedhara C G, Kishan A, Mythri Shankar, Gireesh Reddy, Leelavathi V, Umesha LS, halini
Institute of Nephro-Urology, Bangalore
Introduction: Peritoneal dialysis (PD)-related peritonitis is a major risk factor for drop out of patients on continuous ambulatory PD (CAPD) and automated PD (APD). 1 There have been few studies investigating risk factors that could predict the outcome of these infections. 2 Aim of this study is to identify clinical and
Methods & Results: All patients with PD-associated peritonitis cared for at the Institute of Nephrourology, Banglore, from 2014 to 2021 were retrospectively studied. A total of 53 episodes occurring in 41 patients were evaluated. The average age was 44 years and 50% were men. More than half of the cases were culture negative. Twenty-three complicated episodes were noted including 16 catheter removals and 4 deaths. Exit site infections, drug-resistant organisms and low albumin were potential risks.
Conclusion and Discussion: Exit site infections, multi-drug resistant organisms and low serum albumin were potential risks factors for complicated peritonitis and may be used to distinguish high risk cases. 50% culture negativity despite using automated methods has been described in previous studies. Likewise our study also shows predominance of gram negative peritonitis in accordance with other Indian studies with similar results. Though survival rate was similar to other Indian studies catheter removal rates were slightly higher compared to other studies. This may be because of the patient factors and delay in seeking health care facility. Also the number of government facilities offering Peritoneal dialysis is low compared to hemodialysis.
References
1. Ǫuintanar Lartundo JA, Palomar R, Dominguez-Diez A, Salas C, Ruiz-Criado J, Rodrigo E, et al. Microbiological profile of peritoneal dialysis peritonitis and predictors of hospitalization. Adv Perit,
2. Krishnan M, Thodis E, Ikonomopoulos D, Vidgen E, Chu M, Bargman JM, et al. Predictors of outcome following bacterial peritonitis in peritoneal dialysis. Perit Dial Int 2002;22:573–81.
3. Gupta S, Muralidharan S, Gokulnath, Srinivasa H. Epidemiology of culture isolates from peritoneal dialysis peritonitis patients in Southern India using an automated blood culture system to culture
4. Prasad N, Gupta A, Sharma RK, Prasad KN, Gulati S, Sharma AP, et al. Outcome of gram-positive and gram-negative peritonitis in patients on continuous ambulatory peritoneal dialysis: A single-center
5. Keithi-Reddy SR, Gupta KL, Jha V, Sud K, Singh SK, Kohli HS, et al. Spectrum and sensitivity pattern of gram-negative organisms causing CAPD peritonitis in India. Perit Dial Int 2007;27:205-7.,
Introduction: Indigenous medication usage is widely prevalent in the Indian subcontinent. Lack of strict regulations in the manufacturing process of indigenous medications has resulted in instances of dangerously high levels of heavy metal contaminants causing toxic effects. We report a case of heavy metal toxicity due to indigenous medication usage.
Methods & Results: Case Report: A 31-year-old male, who is a known case of End Stage Renal Disease on Maintenance Hemodialysis for 2 years, presented with involuntary movements of the upper limbs followed by reduced level of consciousness. He also developed 1 episode of generalized tonic-clonic seizure. Neuroimaging was normal. On probing, his wife revealed that the patient has been taking multiple over-the-counter indigenous medicines with the hope of renal recovery.
Conclusion and Discussion: In view of suspected metabolic encephalopathy and the history of indigenous medication intake, a serum heavy metal screening was done which revealed elevated arsenic level - 6.27 ug/L (Normal <5ug/L).
Analysis of the indigenous medicines revealed high arsenic level in the medicine ‘Smritisagar Ras’ (11233mg/kg). The patient was managed conservatively with multiple sessions of hemodialysis, following which his sensorium improved. The patient was discharged without any neurological sequelae. Indigenous medications, especially the use of Indian Ayurvedic medicines is prevalent globally. There have been multiple reports of heavy metal toxicity associated with the use of these medicines, with toxicological analysis showing high levels of heavy metal contaminants, lead being the commonest, followed by mercury and arsenic. Acute arsenic toxicity in humans manifests as gastrointestinal and neurological symptoms. Chronic arsenic toxicity affects all the systems with prominent dermatological manifestations. Having high volume of distribution and renal mode of elimination, chelation is the mainstay of treatment in patients with preserved renal function. In anuric patients, extracorporeal blood purification aids in the removal of arsenic, with chelation helping in containing the heavy metal to the vascular compartment.
References
1. Mikulski MA, Wichman MD, Simmons DL, Pham AN, Clottey V, Fuortes LJ. Toxic metals in ayurvedic preparations from a public health lead poisoning cluster investigation. Int J Occup Environ Health. 2017
2. Pinto B, Goyal P, Flora SJ, Gill KD, Singh S. Chronic arsenic poisoning following ayurvedic medication. J Med Toxicol. 2014 Dec;10(4):395-8. doi: 10.1007/s13181-014-0389-0. PMID: 24696169; PMCID: PMC4,
3. Hsiao,CY., Gresham, C. & Marshall, M.R. Treatment of lead and arsenic poisoning in anuric patients – a case report and narrative review of the literature. BMC Nephrol 20, 374 (2019). https://doi.org/
4. Shivam Gujarathi, Surender, Sahil Sharma; Analysis of heavy metals in herbal products and their impact on human health. AIP Conference Proceedings 3 February 2023; 2558 (1): 020057. https://doi.org/10
5. Saper RB, Phillips RS, Sehgal A, Khouri N, Davis RB, Paquin J, Thuppil V, Kales SN. Lead, mercury, and arsenic in US- and Indian-manufactured Ayurvedic medicines sold via the Internet. JAMA. 2008 Aug,
Effect of intestinal dialysis using polyethylene glycol on fluid balance and thirst in maintenance hemodialysis patients: A comparative study
Puneet Bhuwani
Wockhardt Hospital, Mumbai
Introduction: High Inter-dialytic weight gains (IDWG) and Hyperkalemia have been associated with adverse outcomes like poor quality of life and high mortality. Thirst remains an unsolved problem in Haemodialysis (HD) patients.
Methods & Results: A Prospective Interventional based comparative single center study was conducted. 35 anuric patients on weekly thrice HD were studied for 4 consecutive dialysis weeks. Before the mid-week dialysis day of week 3, Patients received 2L polyethylene glycol solution. The primary end points were change in mean relative IDWG and change in mean subjective thirst feeling as measured on Visual analog scale (VAS) with secondary endpoints being change in small molecule clearance.
Conclusion and Discussion: There was significant reduction in IDWG after the therapy from 3 ± 0.81liters to 2.35 ± 0.72 (P=0.002). The therapy also reduced the % IDWG BW from 5.1 ± 1.7% to 4.15 ± 1.6% (P=0.017). No change in thirst was seen i.e. 6.16 ± 0.66, 6.14 ± 0.64, 6.16 ± 0.65 (P=0.986). A multivariate linear regression did not reveal any effect of age, gender and co-morbidities on the reduction of IDWG. The therapy achieved a significant Urea, Creatinine and Potassium reduction of 8.23%, 8.13% and 8.33% respectively with an increase in sodium levels by 0.86%. This modality reduced the IDWG, was found to be a potent treatment modality for hyperkalemia but did not affect thirst sensation even after consumption of 2 Litre solution.
References
1. Ifudu O, Uribarri J, Rajwani I, Vlacich V, Reydel K, Delosreyes G, Friedman EA. Relation between interdialytic weight gain, body weight and nutrition in hemodialysis patients. Am J Nephrol. 2002 Jul-Aug;22(4):363-8. doi: 10.1159/000065228. PMID: 12169869.
2. López-Gómez JM, Villaverde M, Jofre R, Rodriguez-Benítez P, Pérez-García R. Interdialytic weight gain as a marker of blood pressure, nutrition, and survival in hemodialysis patients. Kidney Int Suppl. 2005 Jan;(93):S63-8. doi: 10.1111/j.1523-1755.2005.09314.x. PMID: 15613071.
3. Foley RN, Herzog CA, Collins AJ; United States Renal Data System. Blood pressure and long-term mortality in United States hemodialysis patients: USRDS Waves 3 and 4 Study. Kidney Int. 2002 Nov;62(5):1784-90. doi: 10.1046/j.1523-1755.2002.00636.x. PMID: 12371980.
4. Saran R, Bragg-Gresham JL, Rayner HC, Goodkin DA, Keen ML, Van Dijk PC, Kurokawa K, Piera L, Saito A, Fukuhara S, Young EW, Held PJ, Port FK. Nonadherence in hemodialysis: associations with mortality, hospitalization, and practice patterns in the DOPPS. Kidney Int. 2003 Jul;64(1):254-62. doi: 10.1046/j.1523-1755.2003.00064.x. PMID: 12787417.
5. Kalantar-Zadeh K, Regidor DL, Kovesdy CP, Van Wyck D, Bunnapradist S, Horwich TB, Fonarow GC. Fluid retention is associated with cardiovascular mortality in patients undergoing long-term hemodialysis. Circulation. 2009 Feb 10;119(5):671-9. doi: 10.1161/CIRCULATIONAHA.108.807362. Epub 2009 Jan 26. PMID: 19171851; PMCID: PMC2773290.
Hematological Abnormalities In Prevalent Hemodialysis Patients At A Government Run Stand-Alone Dialysis Unit- A Retrospective Observational Study
Delfia Sweetlin J, Prasanna Bhat, Sairam B, Aathish,Sreedhar C G, Kishan A
Institute Of Nephro-Urology, Bangalore
Introduction: Hematological abnormalities were well described in patients with CKD. However, there is a paucity of knowledge about these abnormalities in prevalent hemodialysis populations who are already on maintenance hemodialysis. This study aims at analyzing hematological abnormalities in prevalent hemodialysis patients attending a Government run stand-alone hemodialysis unit.
It is a retrospective observational study conducted between April-June 2023. 181 Patients’ baseline characteristics like hemoglobin, RBC indices, total leucocyte count, platelet count and iron profile were collected.
Further anemia was sub-categorized into mild, moderate and severe. Also, we sub-categorized iron deficiency as functional or absolute iron deficiency based on ferritin and transferrin saturation in the study population. The mean age of our study population is 47±13, with male to female sex ratio of 7:3, and Diabetic kidney disease (40%) was the leading cause of ESRD in our study. Hypertension (98%) was the most common comorbidity in this study. The majority of our study population had an arterio-venous fistula (93%) as access for hemodialysis and also 82% of patients were getting dialysis three times a week. Our study results showed anemia in 97% of the study population, of which 76% of patients had moderate anemia. We noticed thrombocytopenia in 20% of patients, further abnormality in total leucocyte count was least common among the
Conclusion and Discussion: Despite patients receiving erythropoietin and I.v iron therapy in the study population, the anemia burden (97%) is still high and most of them had normocytic normochromic anemia and the degree of anemia was moderate, whereas thrombocytopenia is the second most common hematological abnormality noted in the study population.
References
1. shastry I, Belurkar S. The spectrum of red blood cell parameters in chronic kidney disease: A study of 300 cases. J Appl Hematol 2019; 10:61-6,
2. Elsayed Azab, A., & M. Alshoukry, A.B (2023). Prevalence of anemia and variations of hematological parameters among anemic hemodialysis patients in the Tripoli region. Global journal of cardiovascular,
3. Conjeevaram A, Anupama YJ, Vincent L, Sastry NB, Siddini V, Revanasiddappa M, Srinivasa S, Thimmegeowda AB, Kulkarni MJ, Patil VS. Clinico-Epidemiological Profile of Dialysis Services in Karnataka, India - A Multicentric Exploratory Study. Indian J Nephrol. 2022 May-Jun;32(3):223-232. doi: 10.4103/ijn.IJN_94_21. Epub 2022 Mar 23. PMID: 35814317; PMCID: PMC9267092.
4. Study of Hematological Profile in Chronic Renal Failure Patients on Hemodialysis in a Tertiary Care Hospital Ruc hi Khadayate1, Piyush Sahu2, Shilpi Sahu3, Siddhi Karale4, International Journal of Health Sciences and Research (www.ijhsr.org) 1 Vol.10; Issue: 12; December 2020
NPCR And MIS To Assess Protein Energy Wasting in Chronic Kidney Disease Patients On Maintenance Hemodialysis And Its Associated Factors In A Semi Urban Tertiary Care Center
Tirunelveli Medical College, Tirunelveli, Tamil Nadu
Introduction: Patients with chronic kidney disease have muscle wasting, sarcopenia, and cachexia that contribute to frailty and morbidity. The present study assessed the prevalence of protein-energy wasting in dialysis dependent chronic kidney disease population and evaluated the diagnostic validity of nPCR and MIS in diagnosing the protein-energy wasting.
Methods & Results: All patients above 18 years undergoing dialysis for more than 3 months in a tertiary care centre without any active infection or malignancy were included in our study. Anthropometric measurements, dietary assessment, blood investigations were collected. Protein-energy wasting was assessed by International Society of Renal Nutrition and Metabolism 2008 criteria. Diagnostic validity of n PCR and MIS to predict the protein-energy wasting was estimated by area under the curve, sensitivity, specificity accuracy statistics
Conclusion and Discussion: A total of 146 patients were studied. The prevalence of protein energy wasting was 56.8 %. Protein energy wasting was significantly associated with socioeconomic status, hospitalisation days and catheter days. Normalised Protein Catabolisation Rate had the highest sensitivity (90.4%) for predicting protein energy wasting. Malnutritional Inflammatory Score had the highest area under the curve (0.858), specificity (82.5%) and accuracy (82.2%). Mid upper arm circumference, Dialysis Malnutrition Score and Albumin were also found to be significant predictors of protein energy wasting. Lack of advanced equipment in suburban and rural centres to detect protein energy wasting in India, can be overcome by using the various stand-alone and combination nutrition assessment tools which has been validated in the present study. Figure Legend Figure 1: significant associations of PEW Figure 2: Prevalence of PEW by various assessment tools
Acknowledgement
We would like to acknowledge and thank the Staff Nurses, Dialysis Technicians and Dialysis Students of the Department of Nephrology,TVMCH
References
1. Carrero JJ, Thomas F, Nagy K, Arogundade F, Avesani CM, Chan M, Chmielewski M, Cordeiro AC, Espinosa-Cuevas A, Fiaccadori E, Guebre-Egziabher F, Hand RK, Hung AM, Ikizler TA, Johansson LR, Kalantar-Zadeh K, Karupaiah T, Lindholm B, Marckmann P, Mafra D, Parekh RS, Park J, Russo S, Saxena A, Sezer S, Teta D, Ter Wee PM, Verseput C, Wang AYM, Xu H, Lu Y, Molnar MZ, Kovesdy CP. Global Prevalence of Protein-Energy Wasting in Kidney Disease: A Meta-analysis of Contemporary Observational Studies From the International Society of Renal Nutrition and Metabolism. J Ren Nutr. 2018 Nov;28(6):380-392. doi: 10.1053/j.jrn.2018.08.006. PMID: 30348259.
2. Ishfaq Rashid, Aamir Bashir, Pramil Tiwari, Sanjay D’Cruz, Shivani Jaswal, Estimates of malnutrition associated with chronic kidney disease patients globally and its contrast with India: An evidence based systematic review and meta-analysis,Clinical Epidemiology and Global Health,Volume 12, 2021,100855,ISSN 2213-3984, https://doi.org/10.1016/j.cegh.2021.100855.
3. Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, Chauveau P, Cuppari L, Franch H, Guarnieri G, Ikizler TA, Kaysen G, Lindholm B, Massy Z, Mitch W, Pineda E, Stenvinkel P, Treviño-Becerra A, Wanner C. A proposed nomenclature and diagnostic criteria for protein-energy wasting in acute and chronic kidney disease. Kidney Int. 2008 Feb;73(4):391-8. doi: 10.1038/sj.ki.5002585. Epub 2007 Dec 19. Erratum in: Kidney Int. 2008 Aug;74(3):393. Trevinho-Becerra, A [corrected to Treviño-Becerra, A]. PMID: 18094682.
4. Ikizler TA, Burrowes JD, Byham-Gray LD, Campbell KL, Carrero JJ, Chan W, Fouque D, Friedman AN, Ghaddar S, Goldstein-Fuchs DJ, Kaysen GA, Kopple JD, Teta D, Yee-Moon Wang A, Cuppari L. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am J Kidney Dis. 2020 Sep;76(3 Suppl 1):S1-S107. doi: 10.1053/j.ajkd.2020.05.006. Erratum in: Am J Kidney Dis. 2021 Feb;77(2):308. PMID: 32829751.
5. Qin A, Liu X, Yin X, Zhou H, Tang Y, Qin W. Normalized Protein Catabolic Rate Is a Superior Nutritional Marker Associated With Dialysis Adequacy in Continuous Ambulatory Peritoneal Dialysis Patients. Front Med (Lausanne). 2021 Jan 12;7:603725. doi: 10.3389/fmed.2020.603725. PMID: 33511142; PMCID: PMC7835658.
A Single Center Prospective Observational Study To Compare Clinical And Biochemical Parameters And Ǫuality Of Life In End Stage Renal Disease Patients Undergoing Conventional Haemodialysis (HD) Vs Those Hemodiafiltration (HDF)
Yogesh Kumar Gaury
Asian Institute of Nephrology and Urology, Hyderabad
Introduction: Uraemia is a pathological condition caused by the retention of solutes that are normally excreted by the kidneys. This study looks into comparison of effects of HDF to that of Conventional HD on clinical parameters, biochemical parameters and quality of life end points over an observation period of 12 months.
Methods & Results: Single center study Conducted in the Department of Nephrology at Asian Institute of Nephrology and Urology, Banjara hills, Hyderabad from April 2020 to October 2021(12months) Patients were dialyzed thrice-weekly, with a 4-hour schedule, either post or pre dilutional HDF (as per hemodynamic stability and tolerance of patient) using a Fresenius 5008 console and polysulfone high-flux filter (FX60 and FX80) and HD using Fresenius 4008 console – MIDDLE FLUX NIPRO M dialyzer Clinical parameters including age,
Conclusion and Discussion: We conclude that: 1. There is better control of interdialytic weight gain, pre-dialysis SBP, lower requirement of number of antihypertensive drugs, lower weekly EPO requirement and lower phosphate binders in patients undergoing thrice weekly 4-hour HDF than to patients undergoing thrice weekly 4-hour conventional HD. 2. There is improved anaemia control, lower weekly EPO requirement in patients undergoing thrice weekly 4-hour HDF than to patients undergoing thrice weekly 4-hour conventional HD. 3. Hyperphosphatemia is better controlled in ESRD patients undergoing thrice weekly 4-hour HDF than to patients undergoing thrice weekly 4-hour conventional HD. 4. There is a need for monitoring of serum albumin and calcium levels in patients on HDF as our study showed lower serum albumin and calcium levels in ESRD patients undergoing thrice weekly 4-hour HDF than to patients undergoing thrice weekly 4-hour conventional HD. 5. ESRD patients on HDF have better control of uremic symptoms, cognitive function, sleep and physical health when compared with HD patients, using KDǪOL SF 36 questionnaire, 6. There is low mortality in ESRD patients undergoing thrice weekly 4-hour HDF.
Acknowledgement
Dr. Mulpuru venkateshwar rao, Dr. Srikanth gundlapalli, Dr. Sujeeth reddy bande
References
1. von Albertini B, Miller JH, Gardner PW, Shinaberger JH. High-flux hemodiafiltration: under six hours/week treatment. Trans Am Soc Artif Intern Organs. 1984;30:227-31. PMID: 6533889.
2. Panichi V, Rizza GM, Paoletti S, Bigazzi R, Aloisi M, Barsotti G, Rindi P, Donati G, Antonelli A, Panicucci E, Tripepi G, Tetta C, Palla R; RISCAVID Study Group. Chronic inflammation and mortality in haemodialysis: effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol Dial Transplant. 2008 Jul;23(7):2337-43. doi: 10.1093/ndt/gfm951. Epub 2008 Feb 27. PMID: 18305316.
3. Ward RA, Schmidt B, Hullin J, Hillebrand GF, Samtleben W. A comparison of on-line hemodiafiltration and high-flux hemodialysis: a prospective clinical study. J Am Soc Nephrol. 2000 Dec;11(12):2344-2350. doi: 10.1681/ASN.V11122344. PMID: 11095657.
4. Hays RD, Kallich JD, Mapes DL, Coons SJ, Carter WB. Development of the kidney disease quality of life (KDQOL) instrument. Qual Life Res. 1994 Oct;3(5):329-38. doi: 10.1007/BF00451725. PMID: 7841967.
5. Patrier L, Dupuy AM, Granger Vallée A, Chalabi L, Morena M, Canaud B, Cristol JP. FGF-23 removal is improved by on-line high-efficiency hemodiafiltration compared to conventional high flux hemodialysis. J Nephrol. 2013 Mar-Apr;26(2):342-9. doi: 10.5301/jn.5000150. Epub 2012 Apr 27. PMID: 22573526.
Assessment of nutritional status in patients on hemodialysis using handgrip strength - A prospective, observational study in Indian Population
Makbool Ali Agharia, Dhawal Dalal, Jyotsna Zope, Ankit Mody
Bhaktivedanta Hospital and Research Institute, Mumbai
Protein-energy wasting (PEW) is a common complication in patients with chronic kidney disease (CKD) on maintenance hemodialysis. This research work aimed to study the utility of handgrip strength (HGS) as a simple, rapid, bedside test to assess the nutritional status in patients with chronic kidney disease (CKD) on hemodialysis.
The primary objective of this study was to determine the correlation between the handgrip strength (HGS) and the Malnutrition-Inflammation Score (MIS) in patients with chronic kidney disease (CKD) on hemodialysis. Adult patients with CKD on maintenance hemodialysis at a tertiary care hospital were included in this study.HGS was measured using the Jamar hydraulic hand dynamometer in the non-fistula arm of the patients. The MIS tool was used to obtain the MIS for each patient.
This study found a significant negative correlation between HGS and MIS of the patients (P<0.0001). The mean HGS in males was significantly greater than that in females. The findings of our study suggest that there is a significant negative correlation between the handgrip strength and the malnutrition inflammation score of patients with chronic kidney on hemodialysis. This negative correlation exists irrespective of the age and gender of the patients. Thus handgrip strength can be used as a simple, bedside test to assess the nutritional status of patients with chronic kidney disease (CKD) on hemodialysis. The findings of our study suggest that handgrip strength should be used more frequently for the assessment of the nutritional status of patients in clinical practice.
Vagaries of CKD with coagulopathy and its compadres “An interesting case”
Urvashi Khan
Dharamshila Narayana Hospital, Delhi
Introduction: Chronic kidney disease patients have increased rates of bleeding as well as thrombosis. Fibrinogen and platelets combine to generate a mature clot, but in CKD platelets are dysfunctional.
Methods & Results: We present a rare case of 87-year-old male patient who is a known case of ESRD secondary to diabetic nephropathy on maintenance hemodialysis. He had recently been treated with oral steroids for Bullous pemphigoid. Patient presented with multiple spontaneous ecchymosis spots involving trunk and upper thigh. His lab investigations revealed isolated aPTT rising up to 128 seconds despite being on heparin free dialysis. Further evaluation revealed his factor 8 level to be reduced to <0.7%.
Conclusion and Discussion: With this case we would like to bring it into highlight that Acquired Haemophilia A can be suspected in patients presenting with symptoms of bruises without hemarthrosis and without the history of bleeding. Isolated aPTT elevation with normal PT should raise high suspicion of Acquired Haemophilia A.
Acknowledgement
This case report would have been not possible without the exceptional support of my professors, my colleagues, my parents, staff and patient’s attendant.
Reference
1. Binet Ǫ, Lambert C, Sacré L, Eeckhoudt S, Hermans C. Successful management of acquired hemophilia a associated with bullous pemphigoid: a case report and review of the literature. Case Reports in Hema,
Sarcopenia in end stage renal disease patients on maintenance hemodialysis. Hemodialysis
P D Hinduja hospital and Medical Research center, Mumbai
Introduction: Sarcopenia is a progressive skeletal muscle disorder involving the accelerated loss of muscle mass and strength, associated with increased adverse outcomes like falls, poor ǪOL, frailty, and mortality.(1) Prevalence of sarcopenia in dialysis population varies from 4% to 63%.(2) However, the prevalence of sarcopenia in Indian dialysis population remains uncertain.
Methods & Results: The aim of the study was to estimate the prevalence of sarcopenia in MHD patients. 70 adult MHD patients who fulfilled the criteria were enrolled in this cross-sectional study. Bio-impedance spectroscopy, hand grip dynamometry and a 4-meter walk test were employed to evaluate muscle mass, strength and function respectively. Asian Working Group for Sarcopenia (AWGS) criteria were used for defining sarcopenia. The prevalence of sarcopenia was 25.71% in the study population.
Conclusion and Discussion: 70 dialysis patients (mean age 55.3 years) were evaluated using Appendicular skeletal muscle index (ASMI), hand grip strength (HGS) and gait speed (GS) for assessing muscle mass, muscle strength and physical performance respectively. As per AWGS criteria, the prevalence of probable sarcopenia (low ASMI), sarcopenia (low ASMI + low HGS), and severe sarcopenia (low ASMI + low HGS + low GS) was 11.43%, 25.71%, and 7.1% respectively. Prevalence in male and female patients was 26.92% and 25% respectively. Various studies have reported the prevalence varying between 4% to 63%. (2,3) High prevalence of sarcopenia in dialysis patients emphasizes the importance of increased clinical awareness and nutritional status assessment. Outpatient tools like body composition analysis (BIA) and hand grip strength (Hand dynamometer) should be employed for early diagnosis of sarcopenia. Sarcopenia is associated with increased morbidity, mortality and poor quality of life. Early diagnosis is important to employ necessary measures to prevent the progression of the same.
References
1. Brown, J.C.; Harhay, M.O.; Harhay, M.N. Sarcopenia and mortality among a population-based sample of community-dwelling older adults. J. Cachexia Sarcopenia Muscle 2016, 7, 290–298.
2. Kim, J.K.; Choi, S.R.; Choi, M.J.; Kim, S.G.; Lee, Y.K.; Noh, J.W.; Kim, H.J.; Song, Y.R. Prevalence of and factors associated with sarcopenia in elderly patients with end-stage renal disease.
3. Clin. N, Doaa SE Zaky, Amany M. Abdallah, Prevalence of Sarcopenia among Hemodialysis Patients in a University Hospital, Cairo, Egypt, International Journal of Prevention and Treatment, Vol. 8 No. 2, 2019, pp,
Percutaneous USG guided glue (N-butyl cyanoacrylate) injection in post renal biopsy bleeding. Hemodialysis
Gopinath Venkatesan, Venkatesh Rajkumar
Apollo hospitals, Chennai
Bleeding is the primary complication of kidney biopsy. A meta-analysis revealed that PRC transfusion required in 1.6% of patients following biopsy, Intervention and nephrectomy required in 0.3% & 0.01% respectively. Although Interventional procedures are there, still bleeding following biopsy in borderline kidneys and high-risk patients is the nightmare for most of the Nephrologists. Here we have used glue injection intraprocedural to arrest the bleeding following biopsy.
We have done 20 (native & Allograft) kidney biopsies for various indications. Biopsy was done under real time ultrasonogram with 18 G biopsy needle. All patients had high risk factor for bleeding such as elevated serum creatinine, mild thrombocytopenia, echogenic kidneys, anemia, hypertension. All of them had bleeding immediately after the procedure, which was evidenced by the color Doppler. Doppler revealed hematoma with active bleeding and pseudoaneurysms in some patients. N butyl cyanoacrylate (glue) was injected along the biopsy track under USG guidance to arrest the bleeding.
Results After injection of the glue, bleeding was stopped immediately and none of the patients had further bleeding during the follow up period of minimum 24 hours. All of them were discharged in stable condition after 24 hours of monitoring. None of our patients had hypotension, drop in hematocrit and they did not require PRC transfusion or interventional procedure. Conclusions Intraprocedural use of N butyl cyanoacrylate in high-risk biopsy patients following the procedure prevents gross hemorrhage and avoids unwanted hospitalization for biopsy related complications.
Efficacy And Safety of Oral Alendronate Therapy On Bone Mineral Density In Patients On Mhd
Sudhir Mehta
MMIMSR, Ambala, Haryana
Bisphosphonate therapy improves BMD and lowers the fracture risk in general population. The prevalence of low BMD and osteoporosis increases with greater severity of CKD. The large randomized trials excluded patients with known renal dysfunction. Only post hoc studies on the subjects with an estimated eGFR lower than 60 have shown that the fracture reduction was similar to subjects with a normal eGFR. This study was done to evaluate efficacy and safety of bisphosphonates in subjects on MHD.
150 patients of CKD stage 5D were randomized to placebo versus 35 mg of alendronate, taken once a week for 12 months. There was improvement in mean T score, Z score and BMD at level of lumbar spine, femur neck and total hip at 6 and 12 months in patients on DEXA scan, who received oral alendronate compared to controls.
A total of 150 patients of CKD stage 5D with T score < -1SD on DEXA scan were enrolled for the study. 32.5% were female and 67.5% were male. There was improvement in mean T score, Z score and BMD at level of lumbar spine, femur neck and total hip at 6 and 12 months in patients, who received oral alendronate compared to controls. This change in mean of T score, Z score and BMD was statistically significant between two groups at 6 and 12 months. Difference in mean ALP value was significant at 12 months between two groups. There was statistically significance difference in mean PTH level between control and cases at 12 months (P=0.047). Our study demonstrated the efficacy and safety of antiresorptive therapy in patients on regular MHD. Low-dose alendronate, administered for longer duration, appears to be well tolerated in CKD 5D patients without major adverse effects. The BMD, T-scores and Z score declined in the placebo group over 12 months, while there was improvement in the treatment group, suggesting a bone-preserving effect of alendronate. There were no major adverse effects of therapy except for mild GIT intolerance.
Study of Incidence of Intradialytic Hypotension in Patients on Maintenance Hemodialysis in a Tertiary Care Centre in India
Dr Vajed Rahim Mogal
MGM Medical college and superspeciality hospital, Aurangabad
Introduction: Hypotension is quite common during hemodialysis & despite significant improvements of hemodialysis techniques in the recent years; the frequency of recurrent episodes intradialytic hypotension has remained unchanged. Intradialytic hypotension (IDH) is a serious complication and a major risk factor of increased mortality during hemodialysis (HD). However, predicting the occurrence of intradialytic blood pressure (BP) fluctuations clinically is difficult. The goal of our study was to assess the prevalence of IDH and to identify patients and treatment factors associated with its presence.
Methods & Results:
Material and Methods: This is a prospective observational study conducted at the tertiary care center in western region of Maharashtra, India from 1/6/2020 to 30/06/202 (12 months), 200 subjects who were on maintenance hemodialysis (4 hours/3 per week) observed over 12months. Vital statistics, co morbidities, estimated dry weight, pre and post dialysis weight, interdialytic weight gain and medications were recorded. Diet history including salt and water intake were recorded. Complete Blood Count and Iron studies were recorded.
Conclusion and Discussion: Intradialytic hypotension was found in 19% of subjects (38 patients). Incorrectly assessed ideal body weight was found to be the commonest cause of intradialytic hypotension. Volume assessment and adjusting the ideal body weight was found to be central to the problem of preventing intradialytic hypotension. This study concludes that intradialytic hypotension is a common phenomenon, even in a tertiary care center. Preventive strategies should be developed in each unit to decrease the future risk for intradialytic hypotension in specific patients.
References
1. Chiang CE, Wang TD, Li YH, Lin TH, Chien KL, Yeh HI, et al. Hypertension committee of the Taiwan Society of cardiology. J Formos Med Assoc 2010;109:740e73.
2. Aftab R, Khan A, Adnan A, Sulaiman S, Khan T. Efficacy of Losartan in the management of post-dialysis euvolemic hypertension (HELD-Trial): a single-Blind Randomized control Trial. Sci Rep 2016;6:36592.
Case report on imbalance in balancing chamber of hemodialysis machine. Hemodialysis |
A 27 year old female k/c/o CKD 5D on 3/week MHD with dialysis vintage of 8 months, on her one routine maintenance HD session she developed hypotension within 1 hour of dialysis session because of excess UF removed above the targeted goal due to imbalance in balancing chamber.As per HD machine total UF removed was 1.3 kg but there was 3.1 kg weight reduction as compared to her pre HD weight on weighing scale. HD machine was serviced by service engineer and found problem in balancing chamber (screws broken down) and its valve was faulty. In our case, excess amount of UF was removed via drain as there was no obvious leakage seen. Hence never override the test run and should run test each time before initiating any patient on HD. Post HD weight discrepancy with UF goal removed should raise the concern of imbalance in balancing chamber.