
Abstract
Background:
The criteria for vascular access (VA) selection in pediatric hemodialysis (HD) population has changed over time until the current patient-centered approach using the individualized Life-Plan. We analyzed the type of VA used by incident and prevalent end-stage kidney disease (ESKD) pediatric patients (pts) treated with HD in Catalonia.
Method:
Data from the Catalan Renal Registry of ESKD pts under 18 years of age undergoing kidney replacement therapy (KRT) were examined for a 22-year period (1997–2018).
Results:
ESKD children starting KRT through HD decreased progressively from 55.6% (1997–2001) to 38.2% (2012–2018) and, conversely, there was an increase in pts starting KRT by preemptive kidney transplantation (KT) from 28.9% to 42.6% between the same periods (for both comparisons, p = 0.007). Most ESKD pts started HD by fistula (AVF) from 1997 to 2001 (56.5%) but this percentage decreased over time and no AVFs were used to start HD in children from 2012 to 2018. Likewise, the percentage of children starting HD by tunneled catheter increased progressively from 8.7% to 72.2% between the same periods (for both comparisons, p < 0.001). Regarding prevalent ESKD pts, children on HD decreased from 34.9% in 1997 to 4.7% in 2018 and, conversely, pts with a functioning kidney graft increased from 62.8% to 92.4% during the same periods (for both comparisons, p < 0.001). There was a progressive decrease in the percentage of children dialyzed by AVF from 100% in 1997 to 0% in 2018 (p < 0.001). The KT rate increased from 5.4 per million population (pmp) in 1997 to 17.1 pmp in 2018 (p = 0.007). The median time on HD prior to the first KT progressively decreased to 6.6 months (2014–2018).
Conclusion:
The high KT rate was a determining factor in choosing the VA type in the incident and prevalent pediatric population treated with HD in Catalonia.
Keywords
Introduction
According to the current approach, the choice of dialysis access at a given time in the life of each end-stage kidney disease (ESKD) patient must be made in the context of the patient’s individualized Life-Plan, which must take into account the modalities of kidney replacement therapy (KRT) available.1,2 This is especially important in the pediatric ESKD patient, who will have to live with the kidney disease throughout his/her life. 3 A child with ESKD may need to be treated with all modalities of KRT successively throughout their Life-Plan, that is, peritoneal dialysis (PD), hemodialysis (HD), and kidney transplantation (KT), not necessarily in this order. For this reason, the dialysis access of each pediatric patient must be planned considering both the immediate type of treatment and future options for KRT. 4
Regarding HD treatment for adult population, the approach for vascular access (VA) selection has changed successively during the last decade, from the initial “Fistula First,” followed by “Catheter Last” and, finally, the current patient-centered approach of “Patient First” according to the ESKD Life-Plan. 2 This paradigm shift, included in the latest update of the KDOQI Guideline, 4 should also be applied to the pediatric population. Adapting a statement from this Guideline 4 to pediatric patients, the decision about any VA creation or placement should be made according to each child’s overall ESKD Life-Plan.
The main purpose of this study was to analyze the VA profile used by incident and prevalent pediatric ESKD patients treated with HD in Catalonia, Spain.
Method
The Renal Registry of Catalonia
The data source used for this study is the Renal Registry of Catalonia, an autonomous community of Spain with a population of 7,543,825 million residents in 2018. 5 It is a mandatory population registry that collects information on all patients receiving KRT in Catalonia. Once these data have been processed, an annual statistical report and several specific analyses are prepared to present and disseminate the results obtained. All active cases on 31 December are updated yearly.
Patients
We conducted a retrospective and observational study of ESKD patients under 18 years of age undergoing KRT for a 22-year period (1997–2018). Children with ESKD pre-dialysis or on KRT by PD or HD in Catalonia were included on a priority waiting list program for KT. Four types of VA were considered: arteriovenous fistula (AVF), arteriovenous graft, tunneled central catheter (TCC), and non-tunneled catheter.
This study followed the principles of the World Medical Association Declaration of Helsinki, was approved by the Catalan Registry follow-up commission, made up of representatives of all the Nephrology Departments of Catalonia, and it relied only on the official database. As data were retrospectively obtained from the Catalan Registry, informed consent and institutional ethics board review were not required for this study.
Statistical analysis
Data analysis was performed using the STATA software version 13 (StataCorp, College Station, TX, USA). Values were expressed as percentage, median, mean ± standard deviation, and per million of population (pmp) as appropriate.
We used the paired samples t-test and its nonparametric analog Wilcoxon Test to evaluate differences in related means. The chi-squared test was used to assess associations between qualitative variables.
Statistical significance was defined as p < 0.05.
Results
Modality of KRT used by incident ESKD pediatric patients
The modality of KRT used by incident ESKD pediatric patients has changed significantly over time in Catalonia (Figure 1). The percentage of children who started KRT through HD decreased progressively from 55.6% during the 1997–2001 period to 38.2% throughout 2012–2018. Conversely, the percentage of children who started KRT by using preemptive KT showed an increase of 28.9% to 42.6% between the same periods (for both comparisons, p = 0.007).

Modality of kidney replacement therapy used by incident end-stage kidney disease pediatric patients in Catalonia during four periods of time. Black, white, and green represent hemodialysis, peritoneal dialysis, and preemptive kidney transplantation, respectively.
In 2018, 18 children started KRT (12.8 pmp) by using preemptive KT (n = 8, 44.4%), PD (n = 5, 27.8%), or HD (n = 5, 27.8%).
Characteristics of incident pediatric patients starting HD therapy
From 1997 to 2018, 112 ESKD pediatric patients started KRT by using HD. Their characteristics are shown in Table 1.
Characteristics of incident pediatric patients starting HD therapy (1997–2018).
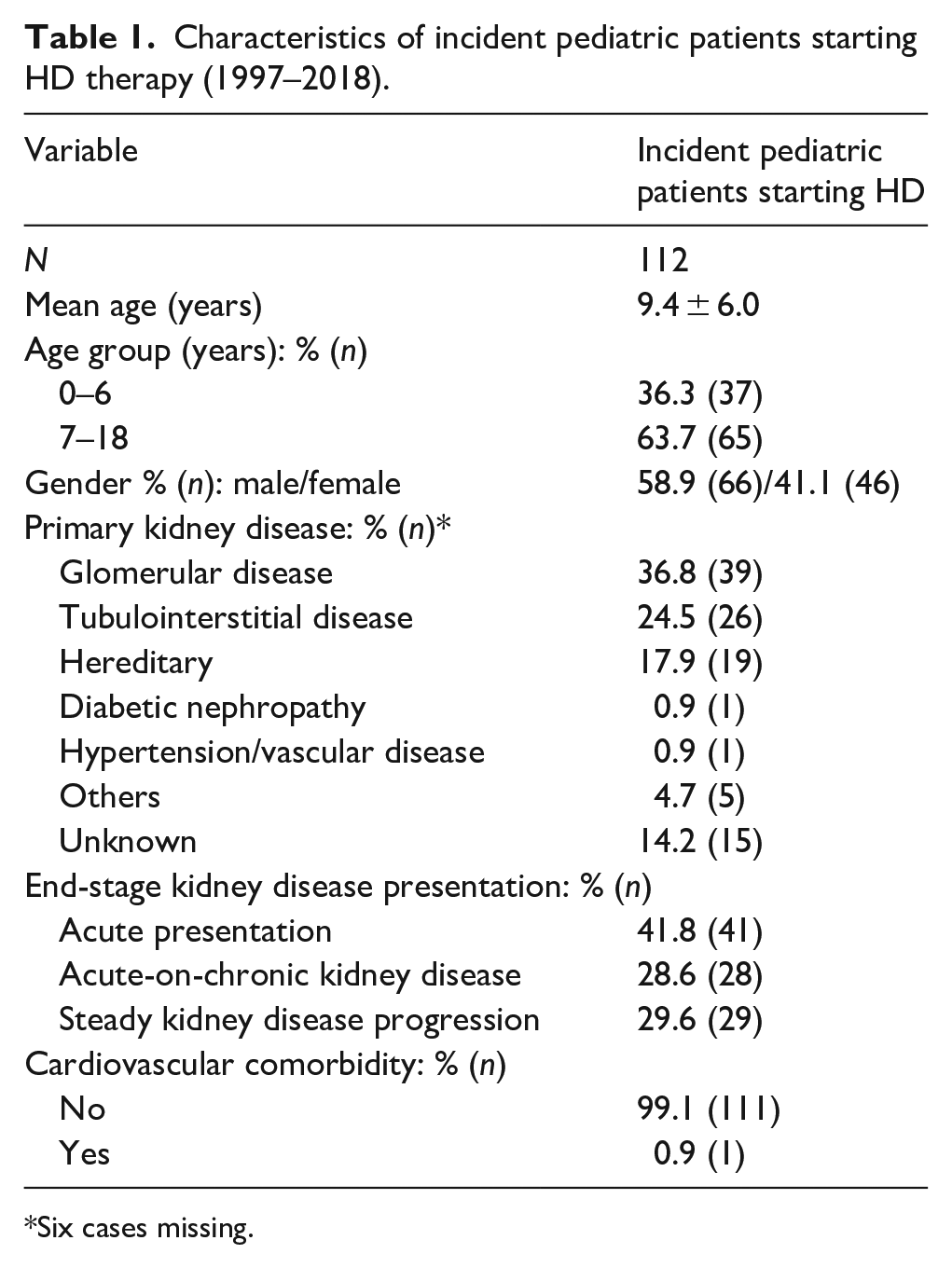
Six cases missing.
Vascular access profile of incident pediatric patients starting HD therapy
Most children started HD through an AVF during the 1997–2001 period (56.5%) but this percentage decreased over time and no children initiated HD using an AVF during the 2012–2018 period (p < 0.001). Likewise, the percentage of patients starting HD through a TCC increased progressively from 8.7% to 72.2% between the same periods (p < 0.001). No significant changes over time were recorded regarding non-tunneled catheter utilization, which dropped from 34.8% (1997–2001) to 27.8% (2012–2018) (p = 0.57). No children used an arteriovenous graft for starting HD during the study period.
Vascular access of incident pediatric HD patients depending on age and kidney disease presentation
Table 2 shows the dialysis access used for incident HD pediatric patients considering two age groups (0 –6 years and 7–18 years) and all forms of kidney disease presentation.
Hemodialysis access used for incident pediatric patients (n = 112) depending on age group and kidney disease presentation (1997–2018).
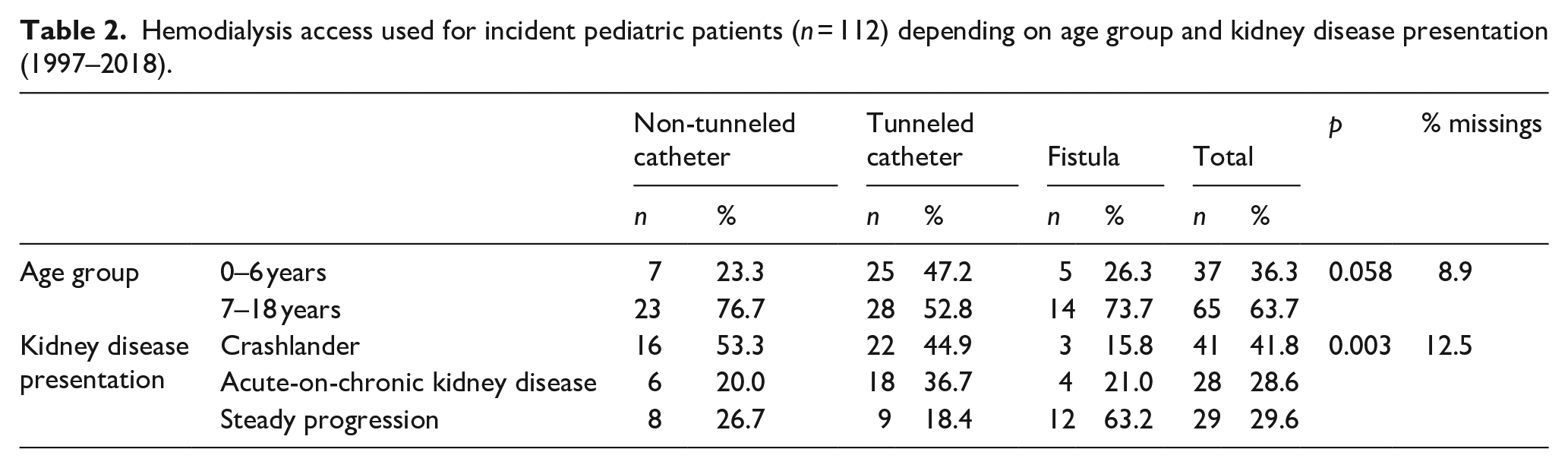
Compared with older children, there was a clear predominance of TCC over non-tunneled catheter and AVF for starting HD in incident patients within the age bracket from 0 to 6 years (67.5%, 25/37).
In addition, the VA mainly used to initiate HD in children differed according to kidney disease presentation. AVF was used for patients with steady kidney disease progression (41.4%, 12/29) and TCC for acute (crash-landers) and acute-on-chronic kidney disease presentation (53.6% 22/41 and 64.3% 18/28, respectively).
Modality of kidney replacement therapy used by prevalent ESKD pediatric patients
The KRT modality using by prevalent ESKD pediatric patients also changed over time in Catalonia (Figure 2). The percentage of prevalent patients on HD decreased from 34.9% (n = 15, mean age 13.5 years) in 1997 to 4.7% (n = 5, mean age 11.6 years) in 2018 (p < 0.001). Conversely, that of prevalent children with a kidney graft rose from 62.8% (n = 27, mean age 13.7 years) to 92.5% (n = 98, mean age 11.2 years) over the same period (p < 0.001). During the 2008–2018 period, more than 80% of prevalent pediatric patients on KRT were at home with a functioning kidney graft (Figure 2).
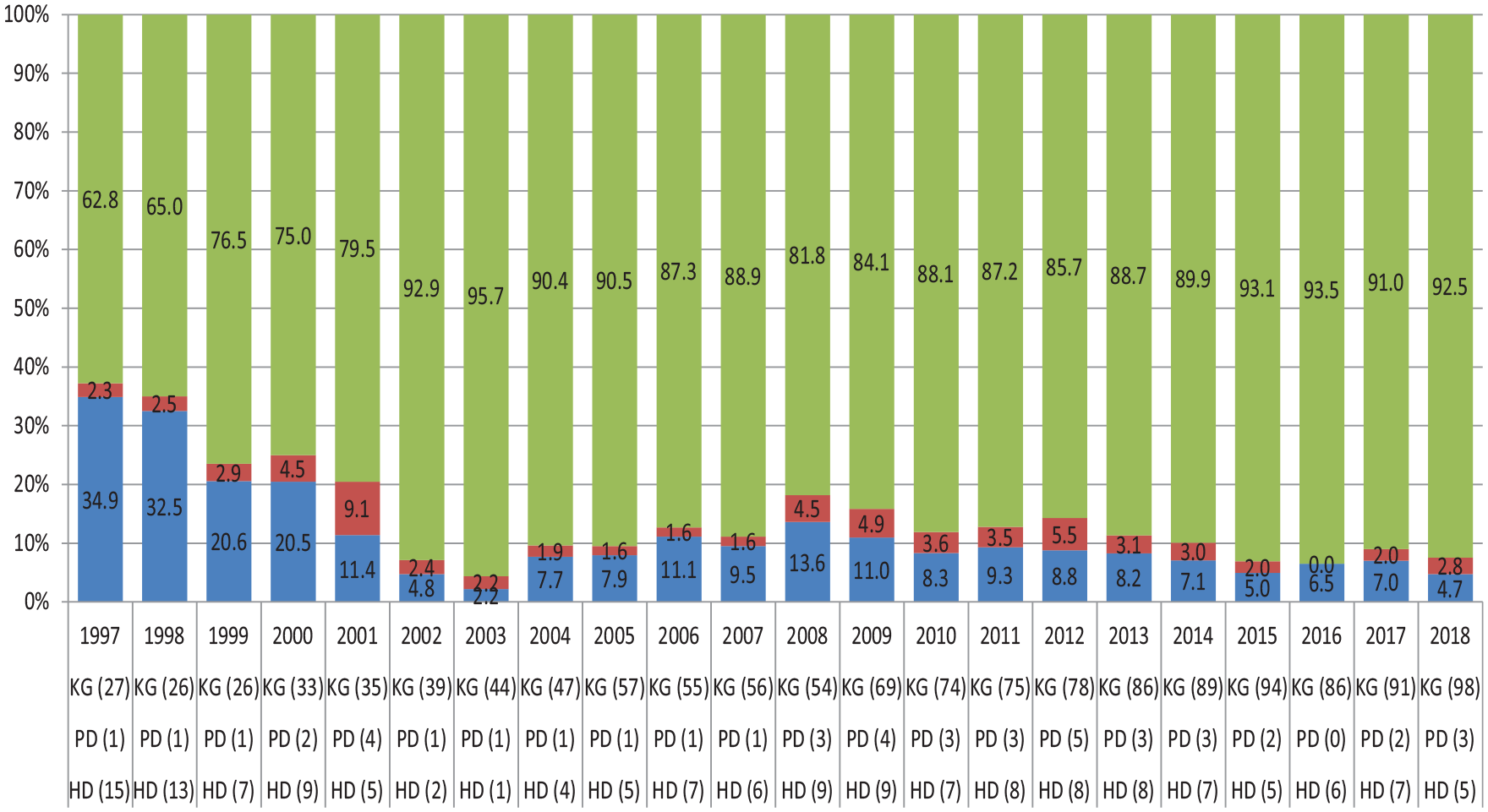
Modality of kidney replacement therapy used by prevalent end-stage kidney disease pediatric patients from 1997 to 2018. Blue, red, and green represent hemodialysis (HD), peritoneal dialysis (PD), and functioning kidney graft (KG), respectively.
Vascular access profile of prevalent pediatric patients on HD
As we can see in Figure 3, the percentage of children dialyzed through an AVF plummeted from 1997 (100%) to 2018 (0%) (p < 0.001). All prevalent pediatric HD patients were dialyzed through a catheter in 2018. No children were dialyzed by an arteriovenous graft during the study period.
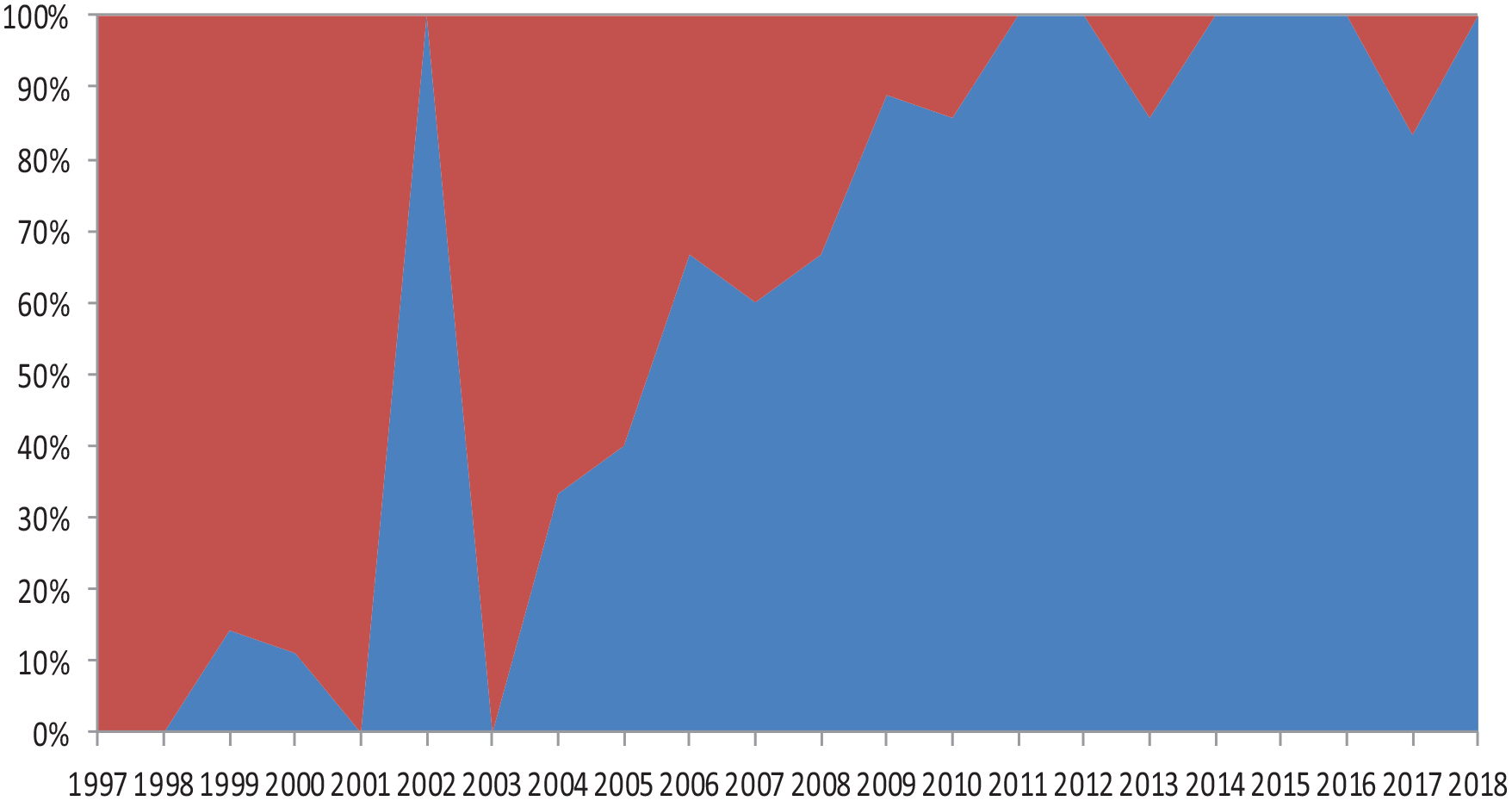
Vascular access profile of prevalent pediatric patients on hemodialysis from 1997 to 2018. Red and blue represent fistula and catheter, respectively.
KT activity for pediatric patients in Catalonia
There has also been a significant rise in the KT rate, which increased from 5.4 pmp (n = 6) in 1997 to 17.1 pmp (n = 24) in 2018 (p = 0.007). The median time on HD prior to the first KT went down from more than 15 months before 2002 to less than 9 months after 2002 (p < 0.001) and was the shortest during the 2014–2018 period (6.6 months) (Figure 4).
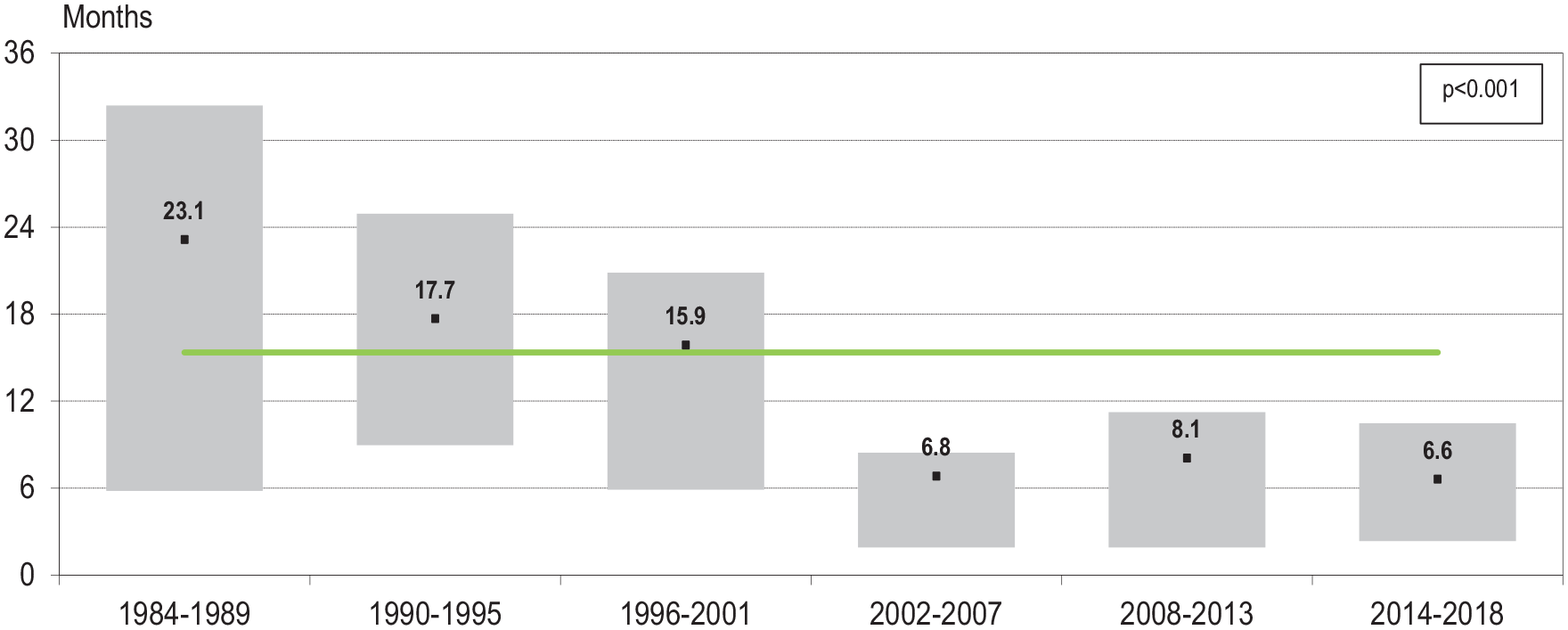
Median time on hemodialysis prior to the first pediatric kidney transplantation in Catalonia considering six periods of time. The solid green line corresponds to the overall median in months.
Discussion
The KRT modality used by incident and prevalent pediatric patients has changed significantly over time in Catalonia. As a result, more than 85% of prevalent children were kidney graft carriers and over 40% of incident patients started KRT through a preemptive KT during the last period considered (2012–2018). On the one hand, this high percentage of prevalent children living with a functioning kidney graft in Catalonia are in keeping with data reported by other Registries.6,7 On the other hand, our results regarding the change of KRT modality used by incident pediatric patients over time contrasts with those published in these.6–8 Indeed, data from Europe (2007–2016), the USA (2010–2020), and Australia and New Zealand (2015–2020) showed that around 20% of incident children started KRT with preemptive KT and this percentage, unlike Catalonia, remained constant over time, with no changes.6–8
In addition to KRT modality, the VA profile of the pediatric population treated with HD also radically changed over time in Catalonia. Since 2012, AVF practically disappeared as the VA in the incident and prevalent patients on HD and almost all children were dialyzed through a catheter. The same trend was reported by other Registries.9,10 In this regard, the systematic review of HD in children by Chanchlani et al. 11 including 54 studies (8751 patients) stratified according to the era of publication, showed an arteriovenous access predominance in studies from 1990 to 2000, but a catheter predominance in the periods 2001–2010 and 2011–2019. There are several factors associated with catheter use, such as late nephrology referral, acute or acute-on-chronic ESKD presentation, young age and/or small vessel size due to technical difficulties for AVF creation, stress caused by AVF needling and/or needle phobia, short waiting time (<1 year) to KT and acting as “a bridge mode” awaiting start of PD technique or AVF maturation.9–12
In this study, we have reviewed the VA used by incident pediatric patients on HD according to their age and the form of ESKD presentation. Although TCC was by far the main VA used for incident HD patients between 0 and 6 years-old, it is noteworthy that, despite their anatomical limitations for AVF creation related to small vessels size, more than 10% of these children started HD with an AVF, a percentage closer to that reported by the ESPN/ERA-EDTA Registry (14.3%). 10 As in the adult population, 13 AVF was the predominant VA for children with a steady rate of kidney disease progression, which gave time for AVF creation and maturation.
The main explanation for the change in VA type used for children in our study should be sought in a significant decrease in time on HD before receiving a kidney graft due to a rise in KT activity over time in Catalonia. Data from the Catalan Registry showed that the overall number of KT performed in Catalonia went up from 560 (74.0 pmp) in 2012 to the historical maximum of 773 (101.7 pmp) in 2018. 14 In fact, this current KT activity is a determining factor on VA profile for both adult and pediatric patients on HD in Catalonia:
- Adults. High KT activity contributes to the increase in the percentage of adult patients with an adverse clinical profile and low rate of mature AVF treated within the HD Units. On the one hand, young adults on HD with a preserved vascular network are more likely to be dialyzed through an AVF and, at the same time, to be on the kidney transplant waiting list for receiving a kidney graft. These adults disappear from the HD Unit after a reasonable time period and are likely to be found at home with a functioning kidney graft in regions with high KT activity, such as Catalonia. On the other hand, elderly prevalent HD patients with a high burden of cardiovascular comorbidity will remain inside the HD room and treated through a TCC and with very little or null probability of receiving a kidney graft. 15
- Children. The median waiting time for receiving the first KT was 6.6 months for pediatric HD patients in Catalonia over the last 5 years of the study (2014–2018) and it was the main reason for TCC placement instead of AVF creation. In fact, TCC acts as a “short-term bridge” between two different KRT modalities: HD and KT. 10 Our results are in line with those reported in the 14-year retrospective study by Merouani et al. 16 including 78 pediatric patients from Quebec, that showed significant VA changes after implementing a pediatric priority allocation policy for deceased-donor kidneys: comparing pre- (1997–2004, n = 41) and post- (2004–2011, n = 37) implementation periods, they showed a significant reduction in waiting time on the transplant list (from 413.5 to 89 days), a significant decrease in time on HD (from 705 to 349.5 days) and a drop in AVF prevalence from 83% to 40% of patients (p = 0.002). In addition, the VA profile shift recorded in our study is in accordance with the consensus document by the European Society for Paediatric Nephrology Dialysis Working Group suggesting the use of a TCC for starting HD, instead of an AVF, where a short period on HD is anticipated before KT. 3
AVF creation is the best vascular access option for starting HD in incident pediatric patients with a long-term forecast on HD and low probability of receiving a kidney graft.12,17 This approach avoids all potential side effects of a TCC.3,9,17–19 Catheter-associated infection and malfunction are the main complications reported, both leading to a catheter exchange rate of 0.32–3 per patient-years. 19 In addition, central venous stenosis development, related to long-term TCC placement, may compromise future AVF creation.3,9,18,19 Although AVF placement in young low-weight children is a technical challenge, successful AVF creation has been demonstrated in these patients using microsurgery techniques.19–21
This study has a series of weaknesses inherent in any study performed completely using patients’ data from a population registry database, because the variables used are restricted in number and can have low clinical specificity. Despite the limited number of patients included, the long duration of the study period (22 years) allows us to analyze the results from an optimal perspective in order to draw conclusions about VA evolution among children on HD in Catalonia.
In summary, high KT rate was a determining factor in choosing the VA type in the incident and prevalent pediatric population treated with HD in the region. The VA profile of children on HD has radically changed over time: since 2012, AVF has practically disappeared and almost all children were dialyzed through a catheter due to the short waiting time on HD before receiving a kidney graft in Catalonia.
Footnotes
Author contributions
The paper was revised critically for important intellectual content and given final approval for publication by all the authors. JC was involved in the analysis and interpretation of data, statistical processing and design of figures. RR-T made substantial contributions to the conception and design of the work, data interpretation, as well as writing and reviewing the article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.