
Abstract
Background:
During the COVID-19 pandemic, Poland saw a surge in interest in midline catheters (MCs) and Long Peripheral Catheters (LPCs) for intravenous therapy. Before this, MCs were not extensively utilised in the country, and there was no formally established Polish vascular access team. MCs, which have been used for years in many countries, are now becoming increasingly common in Poland. This study aimed to analyse the use of MCs in a 3-year perspective of their introduction in daily clinical practice based on a nurse-led Vascular Access Team (VAT).
Methods:
The records of adult patients who received intravenous therapy with 727 MCs and 293 LPCs from January 2021 to December 2023 at the University Clinical Centre of the Medical University of Warsaw were analysed.
Results:
The main indication for cannulation was expected intravenous therapy over 5 days (81.66%, n = 833), of which 71.37% (n = 728) of patients in this group had concomitant difficult intravenous access (DIVA). Over 6 years, centrally inserted central catheters (CICCs) inserted due to DIVA were reduced from n = 108 in 2017 to n = 18 in 2023. The end of intravenous therapy was the reason for the removal of 64.6% of catheters (n = 659), including death and switch to CICCs as well. Complications leading to premature removal accounted for 31.2%, such as: occlusion (14.6%), patient self-removal (7.1%) and thrombosis (3.43%).
Conclusions:
The introduction of MCs as a possible option for peripheral venous access reduces the use of CVCs. Developing MCs programmes should be based on investing in staff competencies, which increases success rates. The nurses and physicians should be trained in infusion care to achieve better results in the use of MCs and LPCs. Increasing the competence of nurses in Poland is necessary for the implementation of full-service and top-level functioning of VAT.
Keywords
Introduction
Intravenous therapy, which includes administering medications ranging from hydration solutions to lifesaving drugs through the intravenous route, is a widely practised yet invasive procedure across the globe. Avoiding complications related to this therapy is a collective challenge for medical teams. 1 During the COVID-19 pandemic, Poland saw a surge in interest in midline catheters (MCs) and long peripheral catheters (LPCs) for intravenous therapy. Before this, MCs were not extensively utilised in the country, and there was no formally established Polish vascular access team. MCs are another option for peripheral venous access alongside the commonly used short peripheral catheters (SPCs) and LPCs. They are particularly suitable for patients who are scheduled to receive intravenous therapy for more than 5 days, particularly with difficult intravenous access (DIVA).2 –5 MCs are inserted under ultrasound guidance into the peripheral veins of the arm using the Direct Seldinger Technique or its variations (Accelerated and Modified). The tip of the catheter according to current recommendations is placed at the level of the axilla in the upper arm despite the fact that studies are emerging which use the ‘midclavicular’ position.5,6 MCs are defined as peripheral device, because the tip is not located in the superior vena cava or in the right atrium. 6 The qualification of patients by nursing staff to obtain appropriate intravenous access, especially under ultrasound guidance, reduces the number of failed attempts with SPC and reduces the number of central venous catheters (CVC).7,8 MCs, which have been used for years in many countries, are now becoming increasingly common in Poland. 9 This study aimed to analyse the use of midline catheters in a 3-year perspective of their introduction in daily clinical practice based on a multidisciplinary nurse-led Vascular Access Team at the Medical University of Warsaw (VAT).
Material and methods
Study number AKBE/284/2023 was acknowledged by the Bioethics Committee. The observational study was retrospective in nature. The records of adult patients who received intravenous therapy with 727 MCs and 293 LPCs from January 2021 to December 2023 at the University Clinical Centre of the Medical University of Warsaw by the Vascular Access Team were analysed.
Vascular access team
The interdisciplinary nurse-led team consists of ten nurses and three anaesthesiologists. MCs use started during the COVID-19 pandemic and was established by the nursing team. After 2 years of operation, the VAT was established as an official unit of the hospital in early 2023. This was the first VAT in Poland to start functioning in a structured, previously unknown way. Over 3 years, procedures and standards of practice were created, as well as a system of support and supervision for the nurses and physicians. The way the VAT functioned and the operating procedures and standards were created based on the Infusion Therapy Standards of Practice issued by the Infusion Nurses Society (INS). 5
Functioning of the VAT
The nursing team is responsible for the qualification of patients, performs the procedure for insertion of SPCs, USG-SPCs, LPCs and MCs on an elective and emergency basis, periodically observes patients with inserted MCs, conducts staff training and responds to telephone calls in the event of complications. The VAT operates during hospital daytime duty. The induction of new VAT members is based on mentoring so that the candidate can safely acquire the relevant competencies (the operators performed 20 cannulations under the guidance of a procedure supervisor).
Nurses’ qualifications
By 2020 in Poland, nurses were only implementing SPCs. The establishment of the first VAT, additionally based on nurses, was a national phenomenon. The first nurses in our team were trained during a university course. Due to the numerous controversies regarding competence, the authors approached national consultants, who expressed the opinion that peripheral cannulation with various techniques (including ultrasound) was within the scope of nurses’ qualifications, as long as they had the knowledge and skills after completing their bachelor’s degree. Currently non-governmental organisations or equipment suppliers in Poland provide education in this field, but these programmes do not confer official accreditation or competence.
Patient qualification
Ward teams pre-qualified patients and completed an electronic MC order sheet. The VAT finalises the decision to insert a MC after conducting a patient interview and physical examination. Qualification was made based on three criteria: (a) predicted DIVA assessed by the A-DIVA scale (>4 points) or (b) two unsuccessful attempts at peripheral catheter insertion and/or (c) expected intravenous therapy more than 5 days.5,10 The suitability for MC is also based on administering compatible, non-irritant (pH = 5–9; <600 mOsm/l) and non-vesicant drugs.5,6 Based on the Manrique-Rodríguez et al. publication it can be determined which ‘low risk’ and ‘moderate risk’ medications can be safely administered by MCs. 11 Moreover, many antibiotics such as vancomycin are ‘red flag’ and hospital protocols for the use of MCs should include this. 12 The appropriateness of the type of access should be re-evaluated as the treatment plan changes.
Performing the procedure
Safe Insertion of Peripherally Inserted Central Catheters (SIP) was adopted to perform the procedure. 13 After obtaining the patient’s informed consent for the procedure, an ultrasound examination of the arm veins was performed using a 10.0 MHz linear probe. Once the optimal puncture site was selected (vein/catheter ratio <33%), cannulations were carried out in an accessible dedicated VAT room and in the case of epidemiologically isolated reason at the patient’s bedside. The recommended of maximal barrier precautions: mask, cap, sterile gown, sterile gloves, long sterile cover for the ultrasound probe, wide sterile field were used. 6 Cannulation was performed using the Seldinger technique with the polyurethane catheters with an integrated extension line 10–25 cm Smartmidline Vygon sets (with stainless steel guidewire for 3 and 4 Fr and nitinol guidewire for 2 Fr). A disposable tape measure was used to determine the correct length of the catheter. Depending on the result of the measurement of the potential distance from the axillary line, an appropriate catheter length was chosen. All catheters were inserted according to the procedure described, but due to European recommendations on the proper indication and use of peripheral venous access devices (the ERPIUP consensus) recommended terminology, they were divided into MCs (>15 cm) and LPCs (10–12 cm). 6 LPCs 8–10 cm (PUR or PEBA) dedicated to DIVA and shorter therapy are not included in the analysis. According to hospital procedure based on INS Standards, the catheter tip was placed at level of axilla. 5 The catheters were secured with the adhesive securement device and transparent dressing.
Data collection
The operator filled in a cannulation and observation chart. The VAT was available for consultation for 12 h on a dedicated telephone number, and despite the daily assessment of all patients in case of complications, the VAT personally assessed the possible causes. Associated complications were recorded whenever the VAT was informed of their presence by ward team. The results of complications should be carefully analysed and interpreted.
Staff education
During the 3 years of MCs use at the centre, there is ongoing education of the medical staff on the implementation of procedures and clinical management following the Infusion Therapy Standards of Practice (new local protocols have been created with detailed guidelines for practice). 5 The bundle for catheter maintenance includes sealing the exit site with a sterile, semi-permeable, transparent dressing. The dressing must be replaced every 7 days or earlier if required. During the dressing change, the adhesive securement device and needle-free connector are changed, and the exit site is disinfected with a single application of 2% chlorhexidine in 70% isopropyl alcohol. Furthermore, the bundle requires that the NFCs be scrubbed vigorously before accessing the line with 70% isopropyl alcohol for at least 15 s or using the disinfecting port protectors when the catheter is not in use. Last but not least the devices must be flushed with 0.9% saline using the pulsed technique.5,6 Due to significant staff turnover, the education programme is ongoing, especially in wards where managers report the need to train new staff.
Statistical analysis
The following statistical tests and methods were used for statistical analysis: Mann-Whitney U, Chi-square, Spearman’s Rho and Kruskal-Wallis. During the statistical verification of the collected material, the significance level of the obtained results was taken as p < 0.05. The incidence of complications was calculated using percentages and episodes per 1000 catheter days. The statistical package IBM SPSS Statistics 29 was used to perform the calculations.
Results
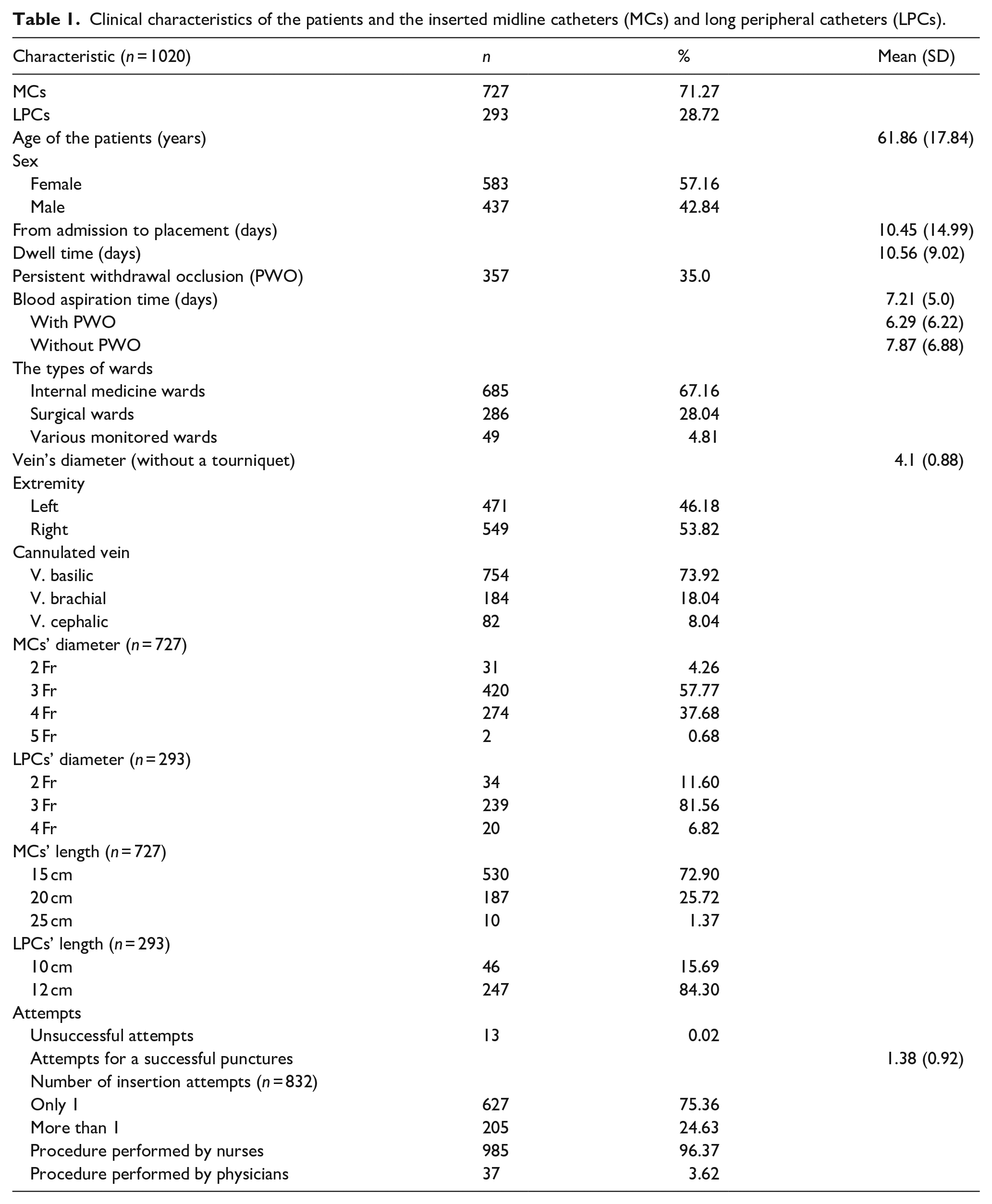
The cannulation and follow-up charts of 1033 midline catheters inserted by the VAT between January 2021 and December 2023 were analysed. 1020 patients were included in the analysis (13 cannulations were unsuccessful and were excluded from further analysis). The main indication for cannulation was expected intravenous therapy over 5 days (81.66%, n = 833), of which 71.37% (n = 728) of patients in this group had concomitant DIVA. Intravenous therapy via catheters was possible for an average of 10.56 days (SD 9.02). Clinical characteristics of the patients and the inserted MCs are shown in Table 1.
Clinical characteristics of the patients and the inserted midline catheters (MCs) and long peripheral catheters (LPCs).
Until 2017, only SPCs, USG-SPCs and centrally inserted central catheters (CICCs) were available at the University Clinical Centre of the Medical University of Warsaw. Subsequently, SPCs started to be inserted under ultrasound guidance by the emergency nursing team, and in the era of the COVID-19 pandemic, nurses began to introduce MCs. Over 6 years, CICCs inserted due to DIVA (as the single indication, even for peripheral drugs) were reduced from n = 108 in 2017 to n = 18 in 2023 (Figure 1). Figure 2 presents the CICC introduced in total (for all indications). There was a marked decrease in CICC insertion in late 2019 and early 2020, the time of the COVID-19 pandemic, when patients requiring total parenteral nutrition or chemotherapy did not present to the hospital due to organisational difficulties of health facilities and lockdown.
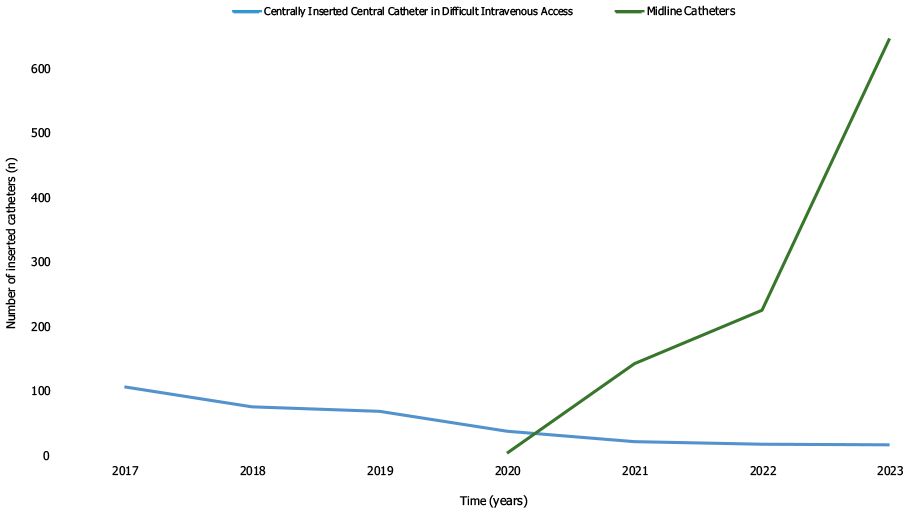
Centrally Inserted Central Catheters inserted due to DIVA and Midline Catheters.
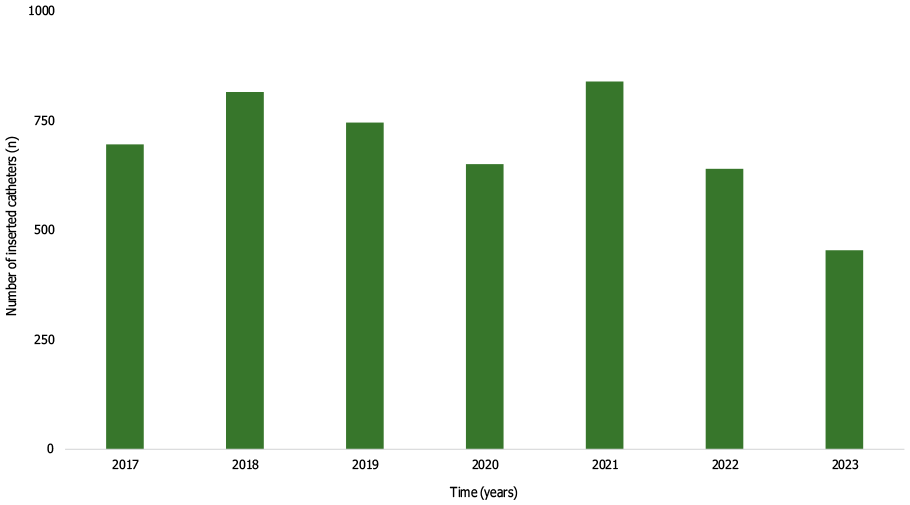
Total Centrally Inserted Catheters.
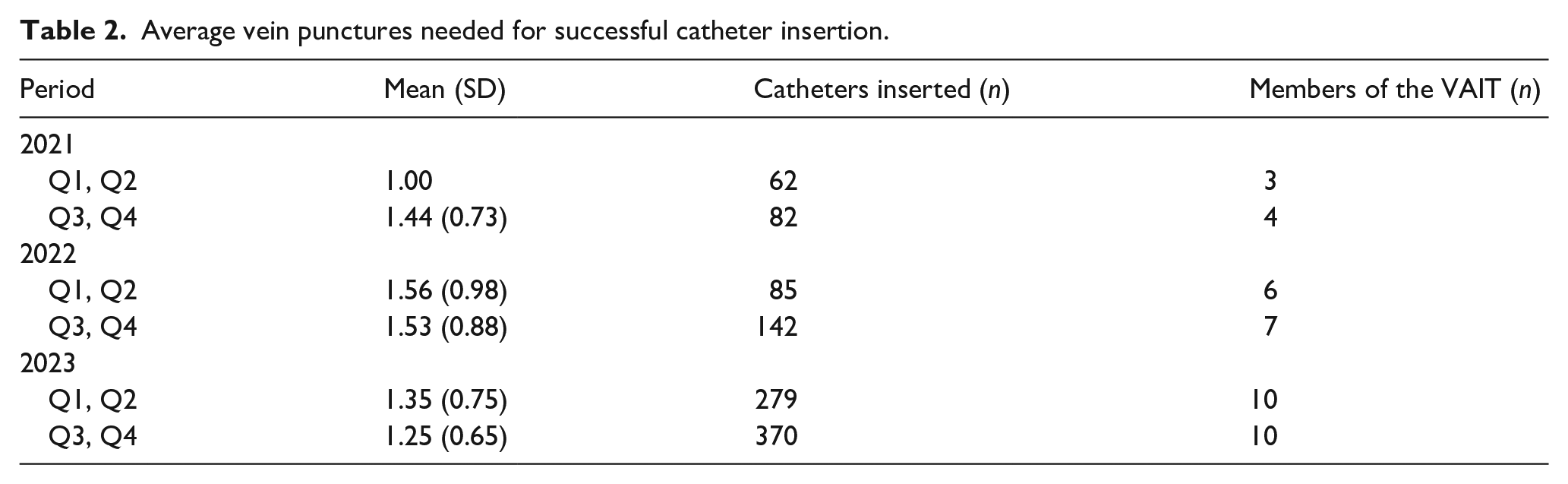
In 2022, nurses to the VAT were recruited, which affected the average vein puncture needed to achieve success (Table 2).
Average vein punctures needed for successful catheter insertion.
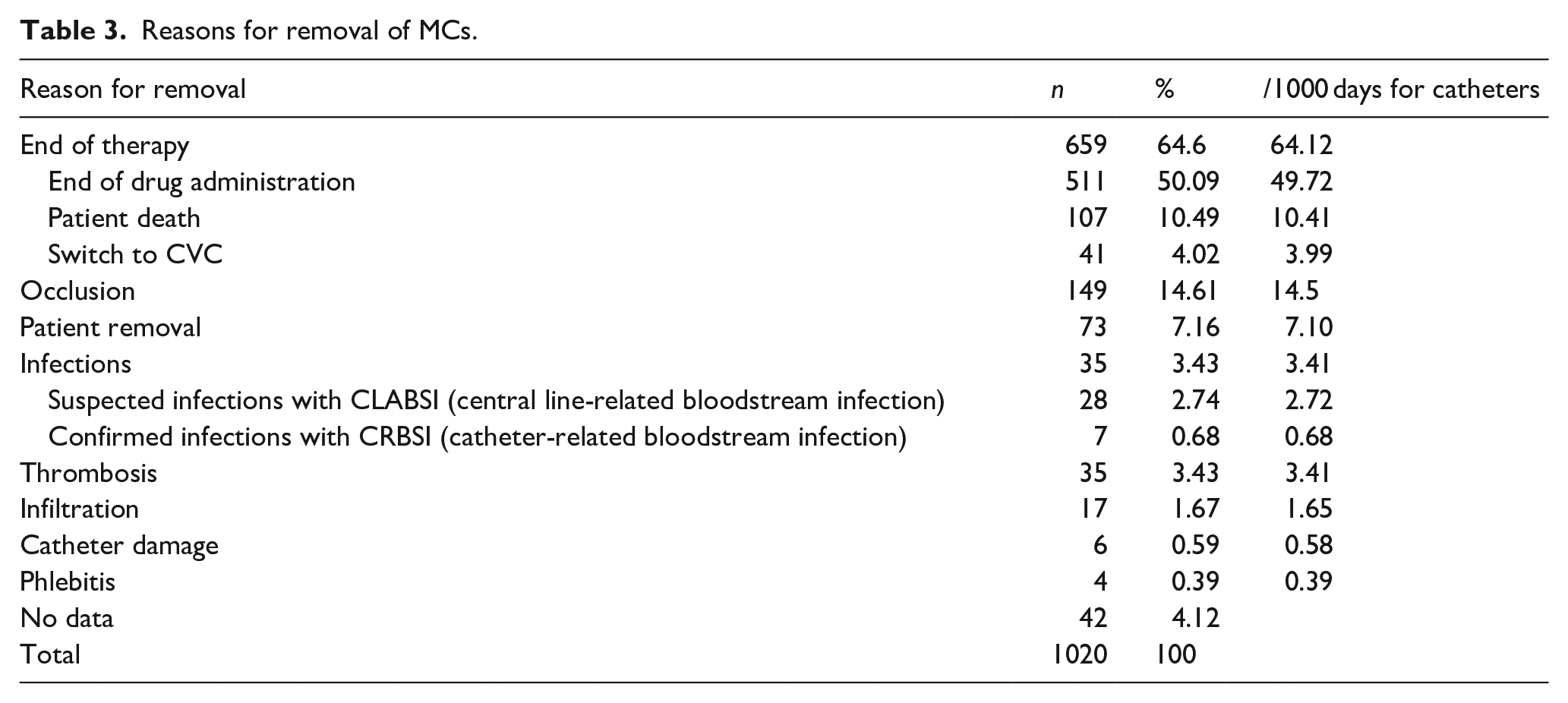
The end of intravenous therapy was the reason for the removal of 64.6% of catheters (n = 659), including death and switch to CVC as well (Table 3). Complications leading to premature removal accounted for 31.2%, such as: occlusion (14.6%), patient self-removal (7.1%) and thrombosis (3.43%) (Table 3). Figure 3 shows the reasons for catheter removal due to catheter occlusion and end of therapy at 3 years.
Reasons for removal of MCs.
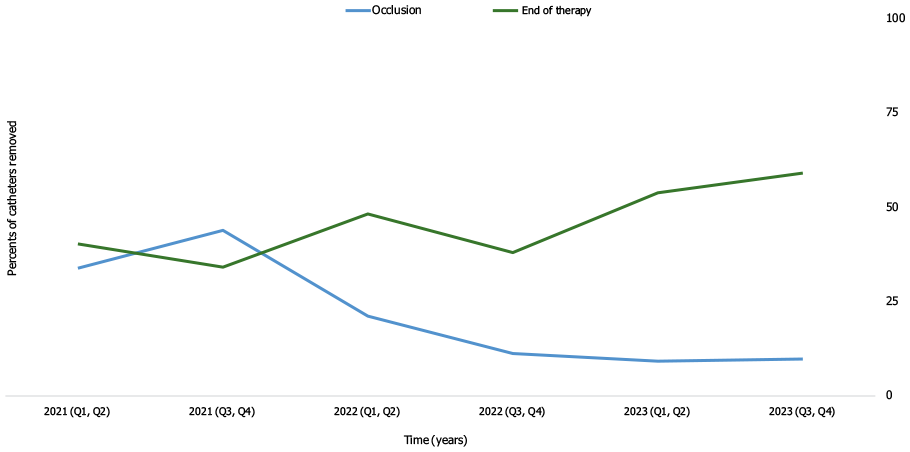
Reason for removal: end of therapy and occlusion
Limitations
This study had several limitations. First, it was a retrospective review of medical records. The type of data collection changed during the registry, which contributed to variables partially missing data in variables in the analysed sample. It was not until mid-2023 that it was possible to introduce an electronic patient registration system. The VAT operates from Monday to Friday, so some needed cannulation were carried out over the weekend by the on-call anaesthetist or emergency nurse. There were instances where the ward team removed the MCs and then passed this information to the VAT. Thus, there was no opportunity to assess the catheter to look for the cause of the catheter failure that was the reason for removal. This may have impacted noting the wrong reason for MCs removal, particularly in differentiating between occlusion and the occurrence of fibroblastic sheath phenomenon or vein thrombosis without clinical signs. Though the definitions of the different types of peripheral catheters have now been systematised due to the accepted indications and method of implantation of MCs with lengths of 10 and 12 cm, we included them in the analysis. The position of the catheter tip was the same and they differed in length rather than technique or material and at the time of the analysis the definitions had not yet been systematised. The LPCs described in the recommendations of the INS and the ERPIUP5,6 we use for DIVA when it is not technically possible to insert SPCs and the expected duration of therapy is shorter than for MCs or unknown. The main determinant for adopting the definition was the catheter insertion site (Dawson’s green zone), the tip location typical of MC (with the tip terminating at the level of the axilla) and to avoid confusion between the results reported, the length of the catheter.5,6,14 We still do not have peripherally inserted central catheters (PICCs) available at the hospital, but qualification for the right access was adopted on the specific criteria described in the methods and MC was selected if and only if compatible solutions were for peripheral veins.
Discussion
We conducted the first analysis of the solution introduced in the hospital in 2021. Despite the implementation of the infusion bundle of care, we noted unsatisfactory results in clinical practice. 15 Unfortunately, it is difficult to refer to national work, as infusion nursing in Poland is just developing and there is a lack of needs for more research in this area. Implementing new solutions based on standards and consistently introducing all their elements may result in improved outcomes. Education of health providers, mainly in terms of patient qualification and proper infusion care, can increase patient satisfaction and safety.5,16 The establishment of VAT can benefit not only the selection, implementation of the appropriate intravenous access and education but also the quality management process, particularly in settings where infusion care is only one of many staff tasks.17,18 In 2021, the team performed effective 92% cannulation of the time, and this rate increased to 98.2% in the present study. 15 However, other authors report efficacy rates of 99.4%–99%.19 –21 This is perhaps due to the learning curve, as the results consider a 3-year period, particularly the first year in which operators were gaining experience in a completely new type of access in the country. IV therapy via MCs could be administered for longer compared to the first and third year of operation, demonstrating the effectiveness of ongoing staff training. 15 However, therapy was provided for an average of 10.5 days, which is still less compared to the 14.9 or 21.82 days described by other authors.19,22 This may be related to the still insufficient level of nursing care in Poland and the further need to develop education in this area.
Indications
At the centre, MCs started to be inserted mainly as an alternative to inserting CICCs due to DIVA (for compatible peripheral drugs when DIVA was the only indication), and in 2021, this indication accounted for 83%. Thanks to the developed training programme for healthcare providers, results improved in several areas, especially in those where knowledge and practical skills that do not require changes in the hospital’s organisational policy predominate. During the period analysed, more patients were qualified based on the expected duration of treatment (81.6%) rather than DIVA alone, which was the main indication in 2021; after 3 years DIVA alone – 17.7%. Johnson et al. report this indication at 32.6%, although it should be remembered that 71.3% of patients whose first indication in our centre was extended intravenous therapy had difficult intravenous access. 23 Days waiting placement was reduced by 4 days compared to 2021 (10.4 vs 15 days). However, there is still a need to emphasise early, procedurally compliant qualification to achieve the result reported by the Rosich-Soteras et al. (mean = 0.13; 0–4 days). 22 Despite creating a team based on scientific research, the competence of nurses in Poland is limited to the implantation of peripheral accesses and many other restrictions that do not allow them to use their full potential. Our centre still does not use PICCs, although many patients could benefit from such a solution and perhaps the acquisition of such competence would allow not only the introduction of MC when it is not necessary to use CICC alone (when compatible peripheral therapy is used), but also PICC when it would be more appropriate than CICC. The introduction of PICCs in hospitals not using it will possibly avoid the potential, and still unknown in the early days of VATs, problem of using MCs to administer drugs labelled ‘high risk’ (due to a change in the patient’s treatment plan). 11
Team experience building
Team building is based on mentoring, which brings benefits in the form of controlled competence acquisition. 24 This is important, especially when the VAT’s personal development is dynamic. This arrangement has resulted in the safe introduction of new members who have been successful in introducing ultrasound-guided vascular accesses. The number of attempts over 3 years decreased from 1.44 to 1.25 despite the introduction of new practitioners who were able to gain relevant experience and aim for efficiencies similar to other authors, where the average was 1.0 (Table 2). 21 It appears that the different average than reported in the literature may be due to hospital policies that do not allow VAT to operate 24/7 according to guidelines, resulting in cannulations sometimes being performed by less experienced practitioners or lacking support from those least experienced in VAT. 5 In addition to the implantation itself, the choice of the correct catheter size and tip location may impact the occurrence of complications.19,25 In relation to the techniques described in the literature and the widespread use of a catheter with 3 Fr or 2 Fr in our centre, it indicates the need to teach the VAT team the pseudo-tunnelling technique, which will avoid the introduction of CICCs for peripheral therapy in patients with small veins in the arms.26,27 The development of further skills and competences indicates the need for responsible training of nurses in the introduction of PICC in the similarity of other European countries.28 –30 The introduction of VATs has well-known benefits, but in the results we have described, the most important is the reduction in the introduction of CICCs due to DIVA and probably through the provision of training a general increase in awareness, which should be analysed in the future. Perhaps the reduction in the cost of care will allow infusion care to be further developed in our country in a similar way to others.
Complications
Complication comparison is problematic due to the different definitions of midline catheters and tip location adopted by the authors of the articles. In the Qin KR survey, the majority of respondents consider that LPCs and MCs should be primarily differentiated based on the location of the tip. 31 Only recently have the definitions been clarified by ERPIUP. 6 However, most authors use the definition of MCs as a catheter >15 cm placed in the axilla or midclavicular position.19,32,33 Currently INS and ERPIUP described MCs inserted in the middle third of the arm and with the tip at level of axilla.5,6 Nevertheless, as the ERPIUP described the tip of MC inside the chest (‘midclavicular’ location) in Europe are still used. 6 This tip location in thrombosis can result in more serious complications than in thrombosis in the veins of the arm. 6 The MCs tip appears to be appropriately positioned distal to the axillary fold to reduce the risk of complications from the catheter tip crossing the joint and potentially less complications from thrombosis relative to its position in the thoracic tract.5,6 More studies are needed to determine the location of the catheter tip leading to longer catheter indwelling time and the incidence of other complications due to different outcomes.34,35 In some works, shorter catheters appear, but they are made of polyurethane and are treated as MCs.36,37 Despite the adoption of the definition by the expert panel in clinical practice, it is not always applicable, as not only the length, but also the material, the place and method of insertion and the position of the tip determine the type of access (e.g. in short patients with 15–20 cm catheters may be too long, resulting in insertion of the tip in the currently not recommended ‘midclavicular’ position and as LPCs and MCs should be primarily differentiated by tip location).5,31 The problem of universal definitions was described by Fabiani et al. 38 Regardless of this, uniform definitions should be used, for example, based on catheter length, which is recommended by ERPIUP, in order to properly compare results and draw appropriate conclusions.
Long time to pre-qualified patients by ward staff and low rate of catheter’s indwelling time, despite improvement is still unsatisfactory, which indicates a continuing need for training of doctors and nurses in the implementation of vascular access selection strategies. This may have been because for many patients, after numerous attempts to insert SPCs over the years and multiple diseases (oncology, diabetes and nephrology), the MC was a ‘last chance’ before obtaining CVC, for which there was no clear indication. MCs were used to terminate intravenous therapy in 64.6%, which was associated not only with complications during use but also with self-removal, death or switch to CVC. Even more accurate and earlier qualifications may allow better results similar to other authors.23,37 Complications leading to premature removal accounted for 31.2% compared to 41% in 2021. 15 Other authors report complication rates in the range of 8%–38%.10,23,39 –41 However, education on proper infusion care reduced the complication rate of catheter occlusion from 36% to 14.6% during the analysed period. 15 Tran et al. report a similar rate of catheter occlusions (17%), although there are papers where it occurred in only 2.6%–3.8%.23,38,39 In an RCT study comparing MCs and PICCs, occlusion was only 2% for midline catheters. 40 If on one hand Persistent Withdrawal Occlusion (PWO) occurred in 35%, which is similar to the 36.5% reported by Gidaro et al., on the other hand, is higher than the one reported in Hitchcock’s study. The authors speculate that the high rate of PWO may have been influenced by the incorrect use of NFCs, despite training and the implemented standard of practice. 42 Appropriate use of NFCs may influence the occurrence of PWO and this area and the practice of nurses using them in practice should be examined. 43 In further practice, PWO due to fibroblastic sleeve should be reported. Microbiologically confirmed infections accounted for 0.68% of the causes of removal. Unfortunately, for 28 catheters, the ward team decided to remove the catheter without microbiological confirmation, which was ultimately not the cause of the developing infection. In the study by Frondizi et al. the authors noted 3.2/1000 catheter days, but in the meta-analysis of Lu et al. only 0.58% (40/6900) and of Chen and Liang 0.59% (43/7079).44 –46 This is an important area that needs to be developed, firstly to further minimise the possibility of infection (some authors reported no infection or at 0.3% in their analyses) and secondly to reduce the number of catheters removed prematurely.10,40,41 Thrombosis occurred in 3.43% of cases similar to other work (0%–4.1%).10,23,39 –41,47 The incidence of phlebitis with MCs phlebitis has been reported for 1.67% and in other works it occurs at the level of 1.9%–3.4%.10,48 We suspect that some of the different results cited in the discussion are due to the highly different level of infusion care and its organisation in different parts of the world. In contrast, others are objective and depend mainly on the implantation technique, which is similar. Moreover, restrictive maintain the appropriate catheter-to-vein ratio may have resulted in a low rate of complications unrelated to infusion care. 49
Conclusions
The introduction of MCs as a possible option for peripheral venous access reduces the use of CVCs. Developing MCs programmes should be based on investing in staff competencies, which increases success rates. Lack of appropriate hospital policies does not allow for the fully effective use of new solutions. The nurses and physicians should be trained in proper choice and infusion care to achieve better results in the use of MCs. Increasing the competence of nurses in Poland is necessary for the implementation of full-service and top-level functioning of VAT.
Footnotes
Acknowledgements
The authors thank the University Clinical Centre of the Medical University of Warsaw teams for their contributions and assistance in this work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: None of the Authors are employed or receive a financial benefit from the use of the equipment in clinical practice by any equipment distributing company, also none of the Authors received compensation for conducting this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Study number AKBE/284/2023 was acknowledged by the Bioethics Committee of the Medical University of Warsaw.