
Abstract
Introduction:
Dialysis catheter-associated bacteremia in Intensive Care Units (ICUs) increases morbidity and mortality, prolongs hospital admission and increases admission costs. Taurolidine-Citrate-Heparin Locking Solution (TCHLS) is a catheter-locking solution with a broad antimicrobial activity against gram-positive and gram-negative bacteria and fungi. The aim of this study was to analyze the effect of systematic sealing of hemodialysis catheters in the ICUs of the Hospital Clínic de Barcelona on the incidence of hemodialysis catheter-related blood stream infections (CRBSI).
Material and methods:
CRBSI episodes of patients who underwent intermittent hemodialysis (IHD) during ICU admission were reviewed. TCHLS was established as a routine dialysis catheter sealing solution in the hospital ICUs in 2015. As a control group an historic pre-TCHLS group from 2010 to 2014 was used. The post-TCHLS period comprised from 2015 to 2018.
Results:
A total of 243 and 266 patients required IHD in the pre- and post TCHLS periods, respectively. The number of CRBSI in the pre-TCHLS period was 18 (7.43%) as compared to 9 (3.38%) in the post-TCHLS period (p = 0.043). All infections were from percutaneous catheters except for three catheters that were tunneled. There was no association between the location of the catheter and the incidence of CRBSI. The most frequent isolated microorganisms were Gram positive bacteria (48.38%), with a global predominance of Staphylococcus epidermidis (32.25%). There were no significant differences in the median days from the start of hemodialysis to the onset of bacteremia (23.5 days in pre-TCHLS group vs 21 days in the post-TCHLS). There were also no significant differences between the days of ICU stay in the CRBSI in both groups or in mortality, being the overall mortality of 65.9%.
Conclusions:
In our population, the systematic application of TCHLS in the sealing of dialysis catheters in critically ill patients reduces the incidence of CRBSI in ICUs.
Introduction
Catheter-related blood stream infections (CRBSI) are among the most frequent nosocomial infections, increasing morbidity and mortality. 1 In the ICU setting, the use of a central catheter is independently associated with a 6- fold increase in blood stream infections, and in the onset of bacteremia, a 2 to 3-fold increase in mortality. 2 The physiopathology starts with colonization of the skin, typically with Staphylococcus spp., but also with gram-negative bacteria and Candida spp. Later a biofilm is formed, with local exit site and tunnel infection, finally leading to bacteremia. 3
Different measures have been explored to prevent CRBSI. Within these strategies, the use of different lock solutions in the sealing of the catheter is on the rise. One of these lock solutions is based on the use of taurolidine. Taurolidine is an antimicrobial agent with broad activity against gram-positive and gram-negative bacteria, and also fungi. It has proved to have capacity of eradication of pathogens from the catheter biofilm.4,5
Several studies have been designed to assess the impact of using these lock solutions in the clinical setting, with promising results. It appears to decrease the incidence in CRBSI when a central venous catheter is used, including hemodialysis catheters.4–8 However, the studies centered in the effect of taurolidine in hemodialysis catheters are focused in chronic kidney disease patients with tunneled catheters, in which the sealing of the catheter with lock solutions is performed in the outpatient setting. There is a lack of knowledge about the role of taurolidine in patients that require intermittent hemodialysis during an admission in the ICU.
The aim of our work is to analyze the effect of systematic sealing of hemodialysis catheters (temporal or tunneled) in the ICUs of the Hospital Clínic of Barcelona on the incidence of blood stream infections associated with hemodialysis catheters.
Material and methods
Study design
We conducted a unicentric retrospective study that included all the patients admitted to the different Intensive Care Units (ICUs) of the Hospital Clínic of Barcelona with need of hemodialysis, from January 2010 to December 2018. The departmental ICUs in the Hospital included a Liver Critical Care Unit, Acute Cardiac Care Unit, Cardiac Surgery Unit, General Intensive Care Unit, Critical respiratory Care unit, and General Surgery Critical Care Unit.
The inclusion criteria were: patients over 18 years old who required renal replacement therapy (RRT), either acute or chronic, during ICU admission. Exclusion criteria were: patients that underwent RRT exclusively with continuous techniques or with use of arteriovenous fistula as vascular access. CRBSI as the cause for ICU admission was not considered for the analysis of its incidence.
In our center, the systematic sealing of acute hemodialysis catheters with Taurolidine-Citrate-Heparin Locking Solution (TCHLS) was introduced in 2015. For this reason, we used as a retrospective control group the patients treated with intermittent hemodialysis in the ICU before implantation of TCHLS, which constitutes the pre-TCHLS group between 2010 and 2014. The study group, post-TCHLS comprised from 2015 to 2018. Prior to this date, the sealing of the catheter was performed made with 5% heparin. The rationale of using taurolidine plus citrate and heparine was based on previous studies were use of taurolidine-citrate-heparine reduced the need for thrombolysis for mechanical dysfunction compared to taurolidine-citrate 9 Also, in previous studies from our group we observed that biofilm formation was reduced when using citrate compared with heparine. 10 Based on our these studies and our experience, we chose taurolidine-heparine and citrate option in order to reduce mechanical catheter dysfunction.
This study was approved by The Ethics Committee of our Institution. HCB/2022/0457 (25th of May 2022). Due to the characteristics of the study, patients did not sign informed consent.
Data recollection
Clinical, epidemiological, and microbiological variables were collected from the Electronic Health Records of our institution (SAP®). For every patient, sex, age on admission, admission cause, vascular access, isolated microorganism, date of isolation, and ICU/hospital length of stay was recorded.
Definitions
Patients with CRBSI were defined as those who had a hemodialysis catheter and presented with fever (>38°C) or local signs of infection with at least one positive blood cultures from a peripheral source and no other apparent source, with either positive semiquantitative (>15 CFU/catheter segment) culture, whereby the same organism (species and antibiogram) is isolated from the catheter segment and a peripheral source blood sample and a differential time to positivity (positivity of blood cultures obtained through the catheter ⩾120 min before those obtained from a peripheral vein). The blood cultures were obtained simultaneously via catheter and percutaneous peripheral vein. The diagnosis was confirmed by the Infectious Diseases Department of our Institution. Once CRBSI was diagnosed, the catheter was removed.
Statistics
The study variables are expressed as median and Interquartile range (IQR) because of their non-normal distribution. Categorical variables were expressed as an absolute value (n) and relative (%) frequency. p-Values less than 0.05 were considered significant. Group comparisons were made by chi squared test or Mann Whitney test for independent groups when appropriate. The statistical analysis was conducted using SPSS v.25 (SPSS Inc, Chicago, IL, USA).
Results
In the study period, 509 patients were included, 243 in the pre-TCHLS and 266 in the post-TCHLS (Figure 1). In the pre-TCHLS, median age was 64 years (53.22–74.16) and 151 (62.1%) were male. In the post-TCHLS the median age was 65 years (55.75–75) and 175 (65.8%) were male. The percentage of patients that had permanent vascular access was 11.1% and 16.2% in the pre-TCHLS and in the post-TCHLS, respectively. All the baseline characteristics are summarized in Table 1. All the long-term tunneled catheters were placed in jugular (27 in the pre-TCHLS period and 43 in the post-TCHLS period). As for non-tunneled catheters, 115 catheters were placed in femoral access and 101 in jugular access in the pre-TCHLS period and 143 in femoral access and 80 in the jugular access in the post-TCHLS period.
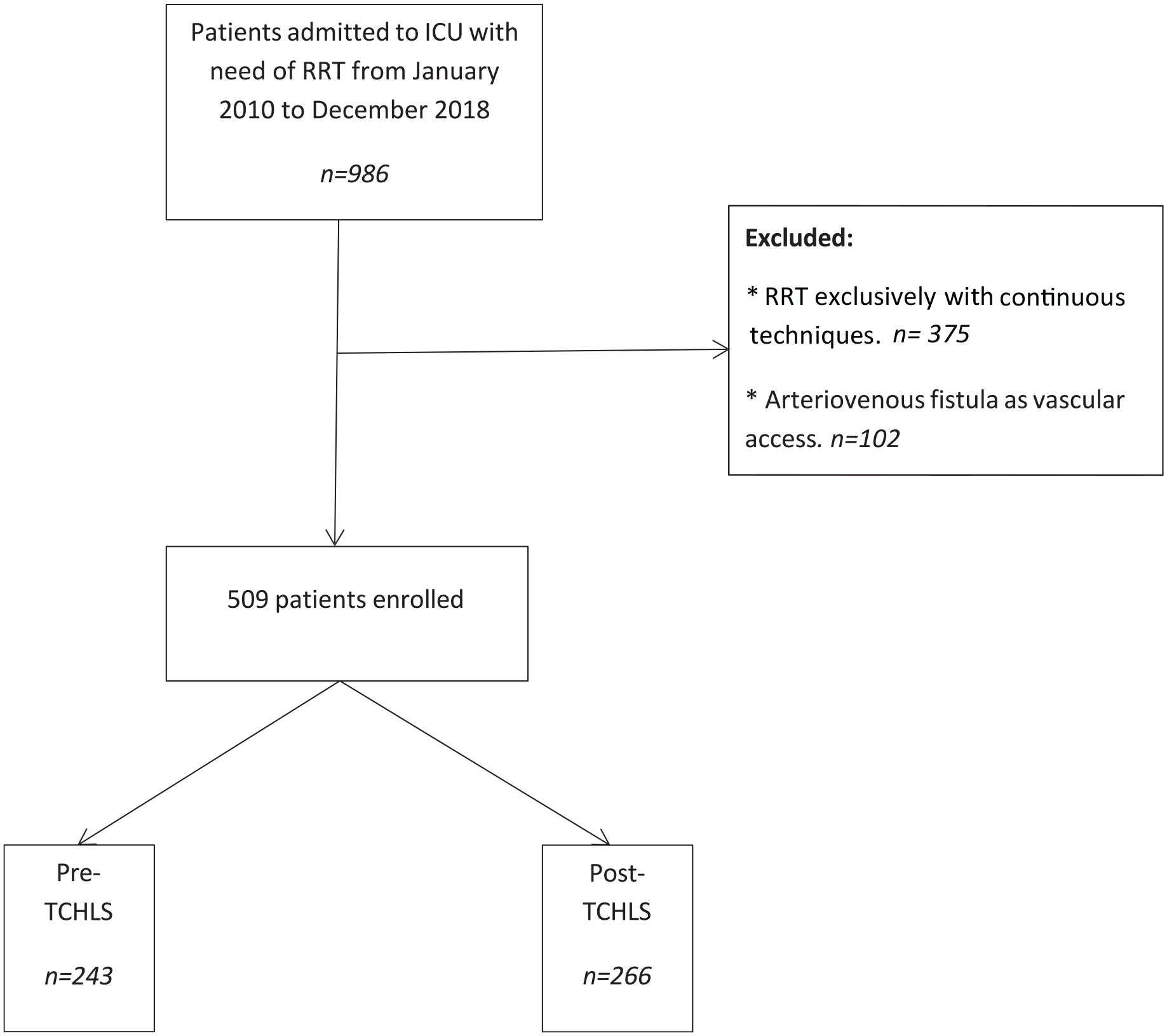
Flow diagram.
Baseline characteristics of the population.

RRT: renal replacement therapy; IHD: intermittent hemodialysis; ICU: intensive care unit; TCHLS: taurolidine-citrate-heparin locking solution.
A total of 27 CRBSI were found. Of these, 18 were pre-TCHLS (7.4%) and 9 were post-TCHLS (3.38%), with a statistically significant difference (p = 0.042) (Table 2). When we express the incidence per 1000 catheter days, it is 0.017 CRBS per 1000 catheter days in the Pre-TCHLS period and 0.008 per 1000 catheter days in the Post-TCHLS period, maintaing the tendency of bacteriemia reduction but losing statistical differences (p = 0.306).
Characteristics of the population with CRBSI.

ICU: intensive care unit; CRBSI: Catheter-related blood stream infections; TCHLS: Taurolidine-Citrate-Heparin Locking solution.
From the total of patients with CRBSI (n = 27), only three patients had tunneled catheters. As for the catheter site, femoral access was the most common site in patients with CRBSI in pre-TCHLS (61.1%) and jugular access in post-TCHLS (66.7%). As for tunneled catheters, only three suffered CRBSI (all in the pre-TCHLS) and all there were jugular catheters. Among non-tunneled catheters, CRBSI occurred in 11 femoral catheters and 4 jugular catheters in the Pre-TCHLS period and in 3 femoral catheters and 6 jugular catheters in the post-TCHLS period. If we analize catheter site, there were no difference between femoral and jugular site in both periods (p = 0.173) but when taking into account only non-tunneled jugular catheter site, there were more common in the post-TCHLS period.
Median days from first dialysis session in ICU to CRBSI diagnosis was 23.5 (11.5–52) in pre-TCHLS and 19 (11.5–24.5) in post-TCHLS without statistical differences (p = 0.348). Median ICU length of stay was 55 (18.5–162.25) days in pre-TCHLS and 30 (21–75) days in the post-TCHLS, without statistical differences (p = 0.705). There were also no significant differences in the mortality rate between both groups, being the overall mortality of 65.9%.
A total of 31 microorganisms were isolated. The most frequently isolated microorganism, regardless of the group, were gram-positive bacteria (48.38%), followed by gram-negative bacteria (29.03%) and finally species of the candida family (22.58%). Overall, the most frequent microorganism isolated was Staphylococcus epidermidis (32.25%). In two cases in the pre-TCHLS period, a combined infection was observed: Staphylococcus epidermidis and Serratia marcescens in one case and Enterococcus faecium and Pseudomonas aeruginosa in the other. No MRSA infection were reported.
The distribution of microorganisms types in pre-TCHLS and post-TCHLS are depicted in Table 3.
Microorganisms isolated in blood cultures in pre and post-TCHLS period.

TCHLS: taurolidine-citrate-heparin locking solution.
Discussion
Given the implications of catheter-related blood stream infections on morbidity and mortality, especially in critically ill patients, different measures destined to its prevention have been explored. 1 In this study, we focused on the impact of using TCHLS in the sealing of the hemodialysis catheters on preventing CRBSI in the ICU setting.
In our population, there was a reduction in incidence of CRBSI after the systematic sealing of the hemodialysis catheters was introduced. This resonates with the increasing evidence that supports the use of taurolidine as a locking solution.
Austin et al. 11 conducted an in vitro study that compared the characteristics of the biofilms of Escherichia coli and Staphylococcus epidermidis that formed in vascular catheters and the effect of different prophylaxis agents. Taurolidine was the most effective agent against the biofilm viability of E. coli and one of the most effective agents against S. epidermidis biofilm biomass. Also, citrate was found to be the most effective against the viability of S. epidermidis biofilm formation.
However, when it comes to preventing fungal biofilm formation, it seems that the results of the use of taurolidine are not so promising. Rosenblatt et al. 12 studied the effect of three different locking solutions: 30% citrate, taurolidine-citrate-heparin (THC) and nitroglycerin-citrate-ethanol (NiCE), in an in vitro model of catheter colonized by five different strains of Candida. Only the NiCE lock solution was able to eradicate all fungi biofilms. Citrate and THC failed to achieve the same results.
Therefore, a combination of taurolidine and citrate as a lock solution could constitute a resourceful alternative for prevention of bacterial CRBSI. In the clinical practice, Taurolidine as a lock solution has demonstrated to be effective preventing CRBSI in patients with intestinal failure receiving parental nutrition, 13 to halve the risk of central venous catheter (CVC)-related infections in oncology patients with long-term CVCs 14 and to reduce the totally implantable venous access port-related infections in cancer patients (ATAPAC trial). 15
Taurolidine as a locking solution has already been tested in chronic hemodialysis patients. In a previous study published by our group concluded that systematic use of a TCHLS to maintain the sterility of the tunneled central catheters lumen significantly reduced the incidence of CRBSI and improved the inflammatory profile of hemodialysis patients. 16 According with these results, Jiménez Hernández et al. studied the biofilm formation with different lock solutions in hemodialysis patients with tunneled cuffed catheters removed for non-infection-related reason. In this study, our group concluded that subgroup of patients under TCHLS obtained a significantly lower thickness and volume of biofilm formation studied by confocal and electron microscopy. 10 A quasi-experimental trial was conducted to determine if the effectiveness of taurolidine-citrate was similar to cefazolin-gentamicin as a locking solution. 17 They found that both antimicrobial agents were equally effective in preventing CRBSI, compared to their own incidence of CRBSI when they used heparin as a lock solution. However, the prevalence of oxacillin-resistant gram-positive strains in CRBSI was higher in the cefazolin/gentamicin group.
Our results resonate with the known literature presented above. We also found that TCHLS is effective in preventing CRBSI when applied as a lock solution in hemodialysis catheters in the critically ill patients. It is interesting to note that once the CRBSI occurred, the length of stay in the ICU, the isolated microorganisms and the mortality rates were similar in both groups regardless of whether a sealing solution was used or not. This could mean that although TCHLS is effective in preventing CRBSI, once the infections occur, the accompanying morbidity remains unchanged. Even though, as it is widely described in literature, an increase in mortality rate was observed when compared to overall cohort ICU mortality (33%, data not shown).
The main limitations of our study lie in the design for itself. It is an observational retrospective study, and even though we analyzed an extended period of time, the final number of patients with CRBSI is low. The low incidence of CRBSI even in the pre-TCHLS era may have made the preventive action of the lock with TCHL less evident, compared to settings where the incidence of CRBSi is higher. Also, because of this retrospective nature, the analysis by catheter/days should be taken with caution. Moreover, in 2009, Spain initiated the Bacteremia Zero Project (pBZ), a standardized intervention designed to mitigate bacteremia associated with CVC insertion and management. This intervention involves the implementation of six measures related to the insertion of the venous catheter: Adequate hand hygiene, application of Chlorhexidine in skin preparation, use of total barrier measures during the insertion of CVCs, preference for the subclavian vein as the placement site, removal of unnecessary CVCs and hygienic management of catheters. This intervention could explain the relative low event rates of infections.
From our study, we conclude that the systematic application of TCHLS in dialysis catheter sealing in critically ill patients can reduce the incidence of catheter-associated bacteremia in intensive care units. Controlled trials are needed to confirm our results and more studies are still needed to identify the best prophylactic locking therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.