
Abstract
Introduction:
According to current guidelines Totally Implantable Venous Access Devices (TIVADs) require regular maintenance (i.e. flushing with 0.9% Sodium Chloride solution) when not in use. Existing evidence suggests that extending flushing intervals up to 12 weeks does not compromise catheter function, but longer intervals or omitting flushes require more research.
Methods:
To facilitate a future randomized controlled trial (RCT), various methods were evaluated for assessing functional (CINAS classification, vacutainer filling time (VFT)), microbial (tip culture, swabs), radiological (linogram), and macroscopic (visual inspection) changes in TIVADs after a 12-weekly maintenance regimen. TIVADs from 70 patients were assessed upon TIVAD removal.
Results:
Concerns over the perceived invasiveness of the linogram resulted in only 36% of eligible patients eventually consenting to participate in the trial. Eighty-six percent had normal TIVAD function, with an average VFT of 23 s/10 mL (SD 5 s/10 mL). Linograms were aberrant in 15% of patients, but the majority of anomalies did not correlate with visible thrombus on inspection or functional issues. No positive microbial cultures were found.
Conclusions:
The primary end point of any future research on TIVAD maintenance should primarily be focused on the functionality of the TIVAD. The CINAS classification effectively standardizes reporting of TIVAD functionality. Although VFT offers a precise measurement of aspiration function, optimal target values remain unclear and clinical relevance might be limited in a functional TIVAD. The added value of a linogram seems to be negligible. An RCT trial comparing 12-weekly TIVAD maintenance versus no maintenance would be invaluable for both patients and health care providers. Clinical Trials register (NCT03948958).
Introduction
Long-term central venous access is crucial for administering vesicant medications and facilitating frequent blood draws for oncology patients. Long-term central venous access can be provided by the implantation of a Totally Implantable Venous Access Device (TIVAD). TIVADs offer safe central venous access, while allowing patients to remain relatively unburdened between treatments, thanks to their subcutaneous chamber implantation. During treatment, TIVAD should be flushed with 0.9% Sodium Chloride solution before and after every use to flush out drug or blood remains. Medication precipitation and blood clotting may lead to internal lumen obstruction of the TIVAD which result in functional problems.1–3 When TIVADs are no longer in use, regular flushing is still advised to preserve patency. Manufacturers recommend TIVAD flushing at least every 4 weeks if no treatment is given. 4 This 4-weekly TIVAD maintenance involves port access with a non-coring needle, verifying functionality, and performing a pulsatile flush and lock with 10 mL of a 0.9% Sodium Chloride solution. 2 The optimal interval between TIVAD maintenance procedures to prevent catheter occlusion is unclear. Current literature supports intervals of up to 12 weeks, although the evidence level is low. 5
The clinical impact of TIVAD flushing regimens on functionality and complications is well studied, but little is known about the underlying physical changes in and around a TIVAD. Our study aims to explore functional, microbial, radiological, and macroscopic factors at the time of TIVAD removal under a 12-week maintenance regimen and also focuses on the usefulness of these tests for future research.
Methods
This prospective, observational study aimed to evaluate the functional, microbial, radiological, and macroscopic parameters as well as patient-reported outcomes at TIVAD removal. The study was conducted at University Hospital Leuven (UHL), Belgium between July 2019 and July 2022. Eligibility criteria included patients scheduled for elective TIVAD removal, aged ⩾18 years, who had not used their TIVAD for therapeutic purposes in the past 365 days, were Dutch-speaking, and capable of providing informed consent. Patients with symptoms of infection, such as fever or chills following the last flushing procedure, were excluded.
Demographic data (age and gender) and details of TIVAD insertion were collected, such as indication for insertion, TIVAD specifications (type, size), implantation technique (vein and body side), and history of TIVAD-related complications (thrombosis, infection, malfunction).
Prior to removal, the TIVAD was accessed using a 20 Gauge non-coring needle, and functionality was assessed using the Catheter INjection and ASpiration (CINAS) classification, with scores of 1 (easy), 2 (difficult), or 3 (impossible) for both injection and aspiration. 6 For normally functioning catheters (IN1AS1), the vacutainer filling time (VFT, i.e. the time required to fill a dry 10 mL Vacutainer® tube) was recorded. 7 In cases of abnormal function (IN2/3, AS2/3), attempts were made to restore functionality through repeated needle puncture, positional changes, and flushing (without using thrombolytics), after which a final CINAS score was documented.
Catheter tip position was assessed on X-ray and a linogram was performed in order to visualize device damage, chamber filling defects, tip thrombosis, and excessive fibroblastic sleeve formation. Tip thrombosis was defined as a filling defect in the vessel and/or a contrast jet deflecting from the catheter’s long axis, and excessive fibroblastic sleeve as contrast flowing retrogradely along the catheter. One research team member evaluated all linograms (GM). Linograms were omitted in patients with renal dysfunction (eGFR < 30 mL/min/1.73 m², or eGFR < 45 mL/min/1.73 m² with risk factors for contrast-induced acute kidney injury), pregnancy, iodine allergy, or known catheter damage/obstruction.
At removal, TIVADs were macroscopically evaluated followed by a photographic documentation of the catheter and port chamber (septum and interior). TIVAD chambers were classified as clean, as having a visible film (i.e. a thin layer of precipitate), or as containing sludge. Two research team members assessed the port chambers independently (MJ and YP). Cultures of the catheter tip and swabs of the port chamber content were analyzed for microbial contamination.
After port removal, patients completed a self-developed Patient Reported Experiences at Port removal (Leuven PREP) questionnaire, covering their experiences with TIVAD insertion, dwell time, and removal. These results will be reported in a separate publication.
Given the anticipated diversity in the patient population, 100 patients were included in the study. No sample size calculation was performed due to the study’s descriptive and explorative nature. Statistical analysis was conducted using SPSS (IBM v29), with categorical variables presented as frequencies and percentages, and continuous variables as medians and quartiles (Q1–Q3).
This study received approval from the UZL Ethics Committee (S62321) and was registered on Clinical Trials register (NCT03948958).
Results
Five hundred and 58 patients were screened, of whom 278 met the eligibility criteria. Of these, 178 patients refused participation, resulting in a final cohort of 100 patients. Seventy of the 100 included patients who adhered to a tri-monthly flush regimen and 30 patients either flushed at longer irregular intervals (n = 18) or did not flush their TIVAD at all (n = 12). Because our primary goal was to evaluate patients under a 3-monthly maintenance interval, 70 patients who adhered to a 3-monthly flushing regimen were included in the analysis. Patient and TIVAD characteristics are detailed in Table 1.
Patient demographics.
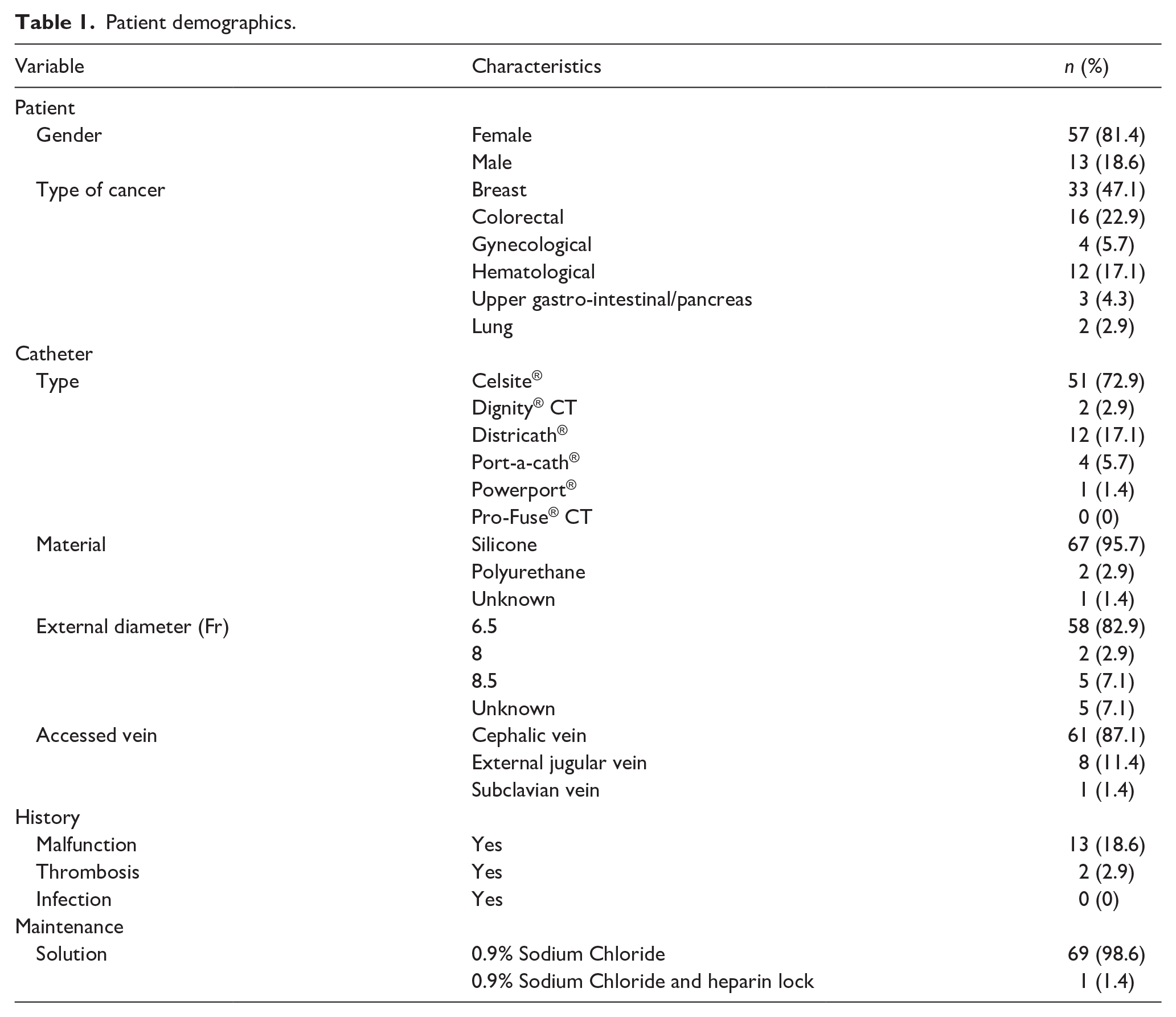
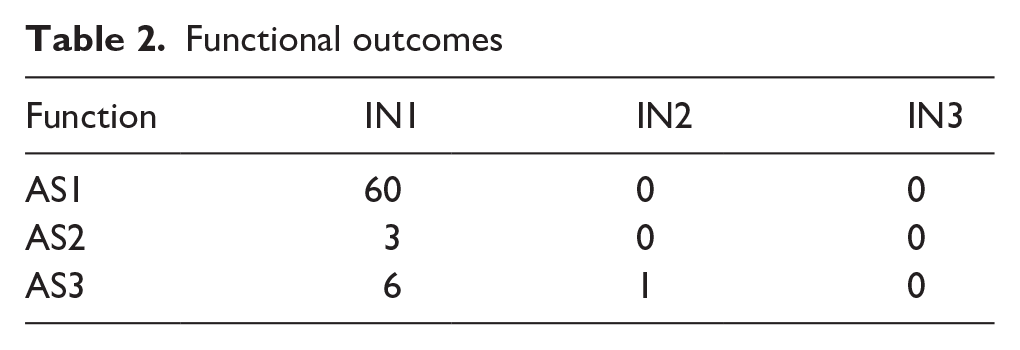
The median age was 62 years (54–69 years). In all cases the indication for TIVAD insertion was chemotherapy administration. All TIVADs were implanted in the infra-clavicular region. The median dwell time since implantation was 1827 days (1192–2224 days). The median time since last maintenance was 53 days (19–89 days). Sixty patients out of 70 (85.7%) had a normal catheter function (IN1AS1), of whom fifty-six directly after Huber needle puncture and another four patients after supplementary simple measures: that is, after new needle puncture (n = 2) or positional adjustments and flushing (n = 2). No complete occlusion (IN3AS3) was detected. Of the remaining ten patients, nine had aspiration problems [IN1AS2 (n = 3), IN1AS3 (n = 6)] and one patient had both injection and aspiration problems [IN2AS3]. Among thirteen patients with a history of port malfunction, three (23%) had an abnormal function (IN1AS3) at removal. The mean VFT was 23 s/10 mL (SD 5 s/10 mL) in patients with an initially normal catheter function (IN1AS1). Functional evaluation results are summarized in Table 2.
Functional outcomes
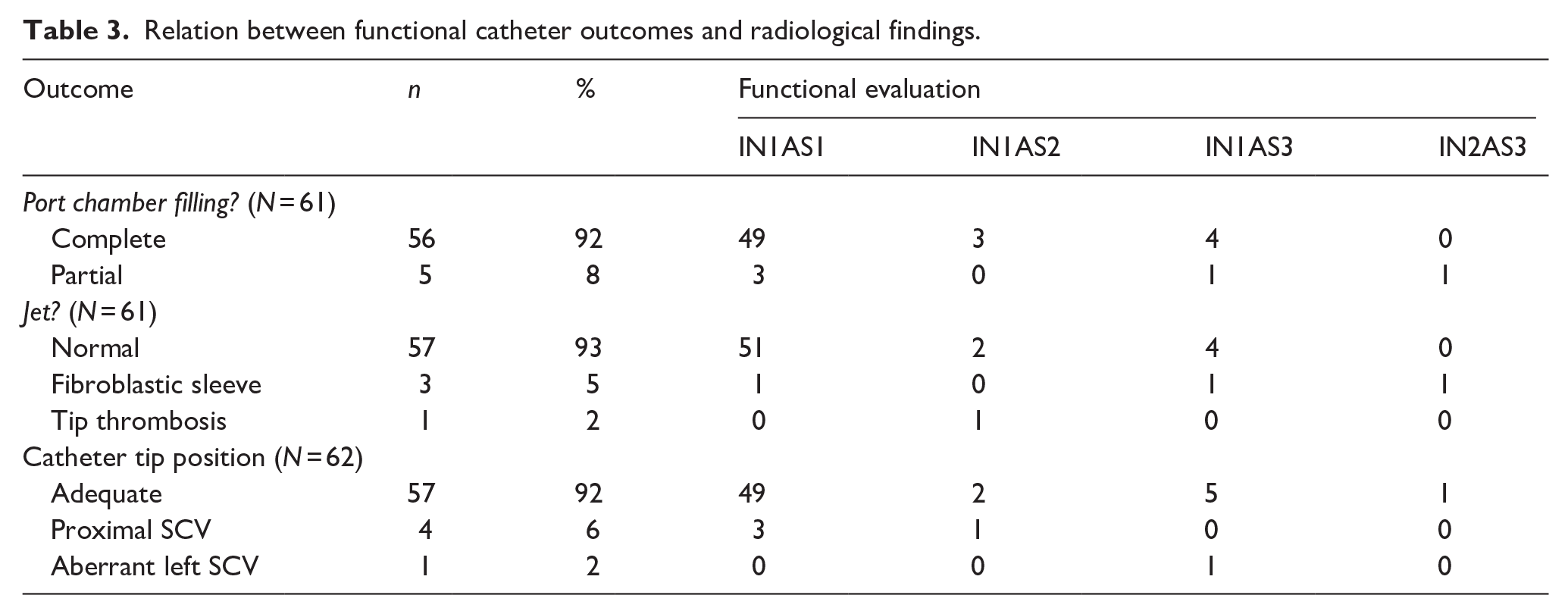
A complete linogram was performed in 61 patients of 70 patients. The linogram was omitted in nine patients, due to contrast allergy (n = 8) and catheter damage associated with contrast leakage (n = 1). In the latter only the tip position could be evaluated. The catheter tip was properly positioned in 57 patients (92%), either in the distal third of the superior vena cava or the right atrium. In other cases the tip was positioned in the proximal superior vena cava (n = 4, 6.5%) or an aberrant left superior vena cava (n = 1, 1.5%). Partial port chamber filling was observed in five cases (8.2%). An aberrant jet was visible in four patients (6.6%), three showed a fibroblastic sleeve and one a small tip thrombus (maximum diameter of 9 mm; Figure 1). Radiological evaluation results are summarized in Table 3.
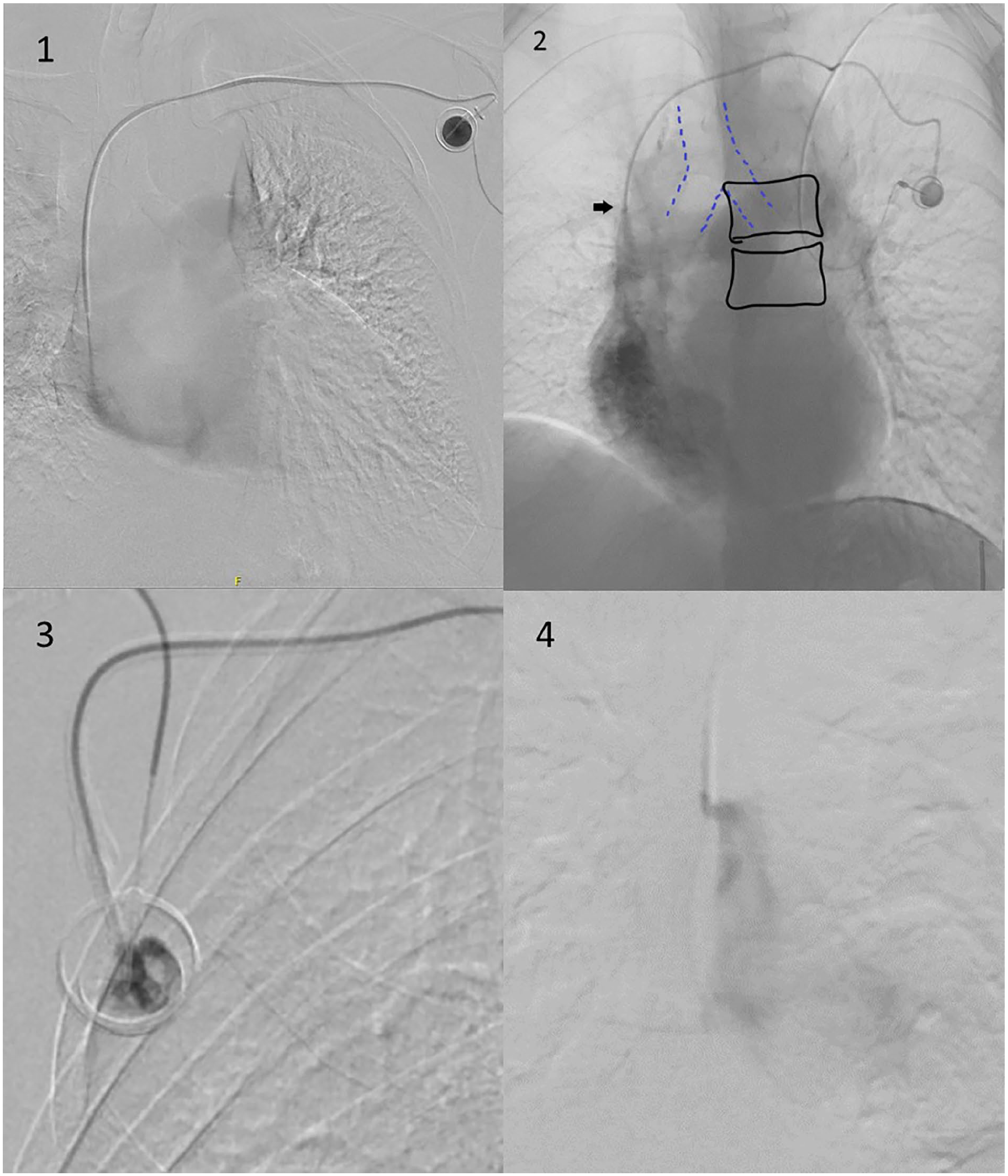
TIVAD radiological evaluation: (1) normal contrast jet, good tip position, (2) references for TIVAD tip position evaluation, carina (Dotted line), vertebrae (full line), tip position (arrow), (3) TIVAD chamber filling defect, and (4) abberant contrast jet caused by tip thrombus.
Relation between functional catheter outcomes and radiological findings.
All TIVAD chambers were surgically removed. In two cases, catheters had to be partially left in situ due to strong adherence to the vein wall which resulted in catheter breaking during extraction. Both instances involved 8.5 Fr Celsite TIVADs with silicone catheters, placed in the cephalic vein via a venous cut-down technique, and in situ for 12 and for 16 years.
All TIVAD chambers were swabbed internally for culture. Tip culture was omitted in two cases due to incomplete catheter removal. All cultures were negative.
Macroscopic inspection of all removed TIVADs revealed visible “contamination” in 28 chambers (40%). This included a visible layer of precipitate at the bottom of the inner chamber in 27 cases (38.6%) and sludge within the chamber in 1 case (1.4%; Figure 2).
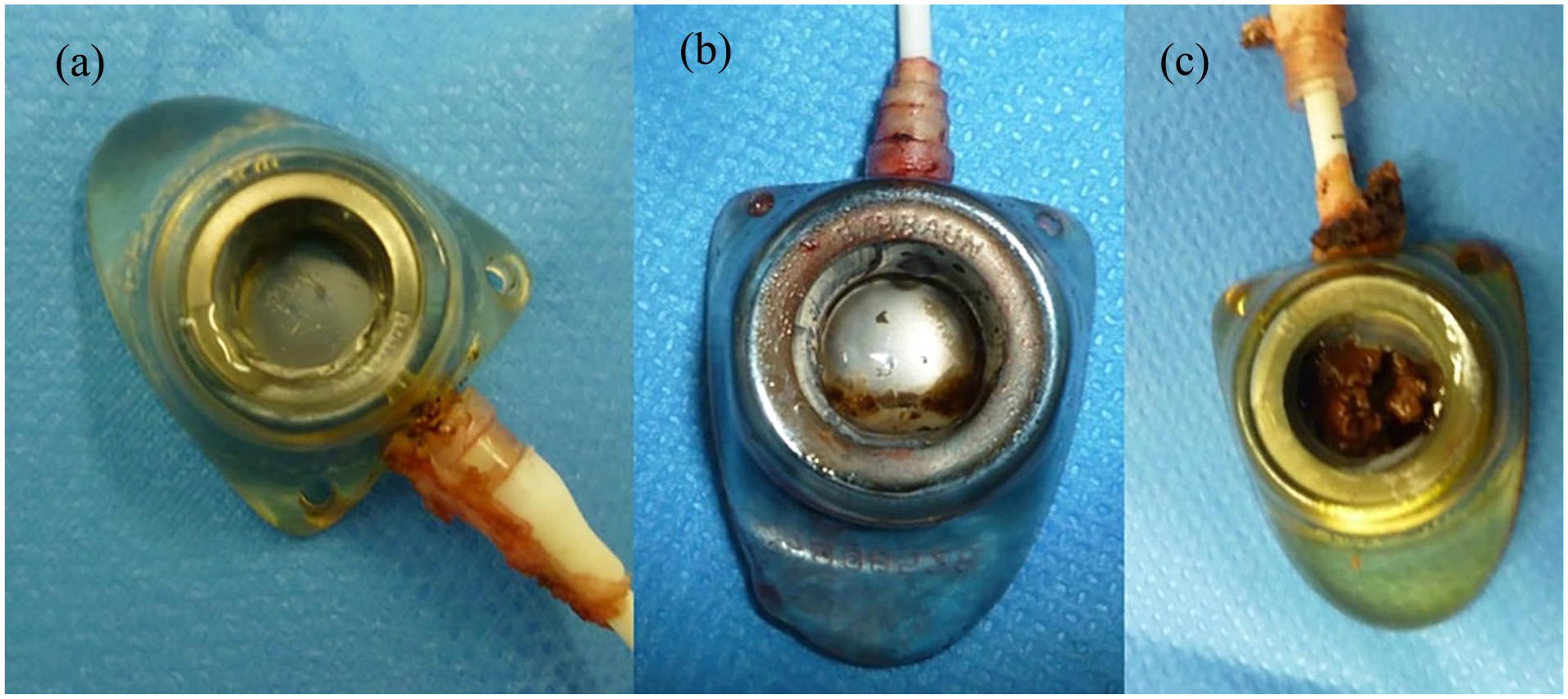
Visual TIVAD chamber inspection: (a) clean, (b) visible layer of precipitate, and (c) sludge.
Discussion
TIVAD are widely used to assist in the treatment of oncology patients. When treatment is completed the TIVAD can be retained for a variable amount of time, depending on the estimated risk of disease relapse. When TIVADs are retained, it is unclear whether they should be flushed to preserve their patency and, if so, at which frequency. Literature on TIVAD maintenance intervals supports intervals of up to 12 weeks, 8 with low evidence; due to small study sample sizes, retrospective study design, varying flushing intervals, different flushing volumes and locking solution and patient populations. Moreover, the non-standardized way of reporting complications and functional outcomes across trials precludes a definitive conclusion on the optimal flushing interval.
We performed a pilot study to evaluate functional outcomes and different techniques to explore TIVAD function under a 12-week maintenance regimen, as well as the resulting physical changes in and around TIVADs.
In this study 30% of patients did not adhere to the prescribed 3-monthly maintenance regimen. Ignatov et al. 9 also reported a compliance of 40% to a monthly flushing regimen, whereas Kuo et al. 10 reported low compliance to a monthly maintenance regimen, but high compliance with a 3-monthly maintenance regimen parallel to a 3-monthly oncology follow-up consultation. This suggests that patients may perceive the prescribed maintenance regimen as having a logistical burden compared to the perceived benefit. Therefore, the underlying mechanisms of non-compliance should be further examined and taken into account before deciding on any type of TIVAD maintenance regimen.
Preserving catheter functionality is the primary motivation for TIVAD maintenance. The incidence of functional problems during maintenance procedures varies significantly in literature, ranging from 1% to 47%.10–13 Unfortunately, comparing functional outcomes is challenging because the definition of functionality is often ambiguous and varies greatly among studies. Most studies focus solely on complete occlusion (IN3AS3) as principal complication, which represented only 1.4% of patients in our study. This finding confirms prior studies, suggesting that a maintenance interval of 3 months results in a low complete occlusion rate.4,5,9–21 However, other functional issues are often overlooked. Difficult injection abilities can result in frequent injection pump alarms or slower drug infusion, potentially leading to treatment delays or suboptimal drug delivery, whereas aspiration difficulties can create uncertainty regarding the needle’s position, which is particularly problematic when administering vesicant drugs. The CINAS classification, first proposed by Goossens et al., 6 offers a dependable method for assessing various types of catheter function with minimal inter-observer variability. This adequate, standardized reporting system for catheter functionality should be advocated for future comparative research.
The VFT was developed as a standardized method to quantify blood aspiration time through TIVADs, which may proof useful in a research context. 7 Interestingly, the mean VFT in our study was 24 s with mostly 1.6 mm internal diameter catheter compared to 19 s in the initial published results for catheters with a 1.1 mm internal diameter. 7 This difference is probably related to the difference in timing of the procedure namely at insertion in the initial study versus at removal in the current study. One hypothesis might be that biofilm accumulation in the internal catheter lumen, may lead to a reduction in the internal diameter and/or might change the shear stress on fluid passing through the catheter. 22 The definition of an impeded withdrawal function, suggested as “the inability to fill a Vacutainer® tube of 10 ml within 20 seconds,” should probably be further examined together with its clinical relevance. In a clinical context, the CINAS is probably sufficient a standardized assessment of TIVAD function.
Several malfunction protocols are available to resolve functional TIVAD issues. They outline measures that vary from simple manipulations (e.g. moving an arm or repositioning the needle) to the use of thrombolytics. 15 A meta-analysis by da Costa et al. 23 demonstrated an 84% success rate in restoring function in occluded long-term venous access devices through thrombolytics. However, despite the effectiveness of malfunction protocols, the burden and cost associated with the administration of thrombolytics may limit their use in study protocols on TIVAD maintenance. In our study, functional problems could be resolved without thrombolytics in 28% of cases (4 out of 14 patients). Given the high success rate of malfunction protocols with thrombolytics one can further argument to omit TIVAD maintenance.
A linogram has been proposed as a method to assess the presence of precipitates and thrombosis in the TIVAD chamber. 24 While radiological imaging showed abnormal chamber filling in five cases in our study, after removal, macroscopic examination revealed visible sludge in only one of these TIVADs, which questions the accuracy of a linogram to assess presence of TIVAD chamber debris. Needle bevel orientation during linogram could be a possible explanation for this discrepancy. Guiffant et al. studied the effects of Huber needle bevel orientation and found that positioning the needle opening toward the chamber exit creates a low-flow zone behind the needle. If the bevel is directed toward the chamber exit during a linogram, stasis of the locking fluid behind the needle could ensue, leading to an apparent filling defect. 3
A linogram can also visualize extraluminal alterations at the catheter tip, such as a thrombus at the tip or a fibroblastic sleeve around the catheter tip. 25 In our study, an abnormal contrast jet was shown in four patients, although functional issues arose in only three of them.
Thus, visualized abnormalities on linogram do not always correspond to functional impairments. Furthermore, many patients refused inclusion into our study, because they perceived the linogram to be an invasive procedure. Therefore, less invasive and more precise imaging techniques are needed to optimize the detection of fibroblastic sleeve formation and tip thrombosis. Enhanced ultrasound modalities, along with greater experience in TIVAD insertion, have improved visualization of thrombosis and sleeve formation along the catheter, though the catheter tip remains difficult to assess.26,27
Chou et al. reported on 434 removed TIVAD and found visible contamination in 56.9% of TIVAD chambers. They also identified “injection chamber blood clot” and “injection chamber biofilm” as two separate problems, respectively in 22.1% and 34.8% of TIVAD. 14 Yet, despite the use of a similar maintenance regimen, visual inspection of the TIVADs in our study revealed clear occlusive sludge in only 1 (1.4%) and a film in 27 (38.6%). The presence of a biological film lining the implant can be explained by an almost instant protein adsorption to biomaterial surfaces, followed by an inflammatory response and formation of foreign body giant cells. The course of this foreign body reaction on the inside of catheters has not been elucidated yet, but this biofilm does not lead to infectious complications nor functional problems. 28 However, the presence of a blood clot or substantial precipitate in the TIVAD chamber may lead to functional problems due to obstruction of the needle internally or chamber exit. We hypothesize that blood clot presence in the chamber is probably related to inadequate TIVAD flushing rather than to the frequency of maintenance. However our study precludes conclusions about the correlation of maintenance practices with these events due to the exclusion of TIVADs removed for complications, such as infection or thrombosis.
Although our TIVAD maintenance procedure is for years already 3 months, 30 patients admitted that they extended the procedure. The analysis of these 30 patients is performed separately and may be found in the supplementary data. Given the explorative nature of the study, no impact of the smaller sample size is expected on the results. The data regarding adherence to the flushing regimen were self-reported and not always verifiable. Therefore, for the other 70 patients, it remains uncertain how many patients may have responded in a socially desirable manner, potentially indicating compliance with the 3-month maintenance when they did not actually adhere to it.
Conclusion
Although TIVAD maintenance is prescribed by manufacturers, it represents a substantial burden for patients, health care staff and society, without proof in preserving TIVAD function. Furthermore, current evidence in literature on the optimal timing of TIVAD maintenance is low and scarce.
Our study reports a clear evaluation of functional, microbial, radiological, and macroscopic factors at the time of TIVAD removal under a 12-week maintenance regimen. These results have not been reported before in literature. Furthermore, we have evaluated the use of different examination strategies such as CINAS, VFT, linogram, providing crucial information for planning future research on TIVAD maintenance.
In our opinion, the primary end point of any future research on TIVAD maintenance should primarily be focused on the actual TIVAD functionality, because this has the highest direct clinical relevance. Research would greatly benefit from an international consensus on the definitions of functionality, preferably using an easy scoring system, such as the CINAS score. A current gap, a RCT comparing 12-weekly TIVAD maintenance versus no maintenance would be invaluable for both patients and health care providers.
Footnotes
Acknowledgements
We acknowledge the vast amount of previous research and support by Prof. M. Stas, who had an important role in preparation of this study. We acknowledge the use of Chat GPT4.0 in revision of the text.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by “BBraun chair for research on vascular access.”
Ethical approval
This study received approval from the UZL Ethics Committee (S62321) and was registered on Clinical Trials register (NCT03948958).
Consent to participate
Requirement for informed consent to participate has been waived by the relevant Ethics Committee.