
Abstract
Purpose:
To assess the accuracy and safety of intracardiac electrocardiography (IC-ECG) in positioning catheter tips for Totally Implantable Venous Access Device (TIVAD) placement.
Methods:
This study conducts a retrospective analysis of patient data collected from The Affiliated Suzhou Hospital of Nanjing Medical University. Patients were categorized into two groups based on the method used for catheter tip positioning: the IC-ECG group and the X-ray group. Propensity Score Matching (PSM) is employed to balance the baseline characteristics of the two groups in a 1:2 ratio. The primary outcomes of interest are the ideal position rate of the TIVAD tip and the incidence of complications. Additionally, multivariable logistic regression analysis will be utilized to identify risk factors associated with complications. The area under the ROC curve (AUC) will be calculated to evaluate the diagnostic performance of the detection methods.
Results:
During the period from January 2023 to June 2024, a total of 493 adult oncology patients received TIVAD. After applying PSM, 465 patients were included in the retrospective analysis, comprising 221 males (47.5%) and 244 females (52.5%), with a mean age of 62.6 years. The ideal position rates for the catheter tips were 150 cases (96.8%) in IC-ECG group and 301 cases (97.1%) in X-ray group (p = 0.834). The distance from the catheter tip to the carina was measured at 1.60 ± 0.356 and 1.41 ± 0.34 vertebral body units, respectively (p < 0.01). The overall complication rates were comparable between the two groups. Multivariate logistic regression analysis indicated that BMI is an independent risk factor for TIVAD-related complications (OR = 0.437, 95% CI: 0.319–0.563, p < 0.001). The ROC curve analysis revealed that the area under the curve (AUC) for BMI was 0.926 (95% CI: 0.886–0.926, p < 0.001).
Conclusion:
Intracardiac electrocardiography (IC-ECG)-guided catheter tip positioning for TIVAD placement has demonstrated accuracy, feasibility, and safety. Given its potential to reduce radiation exposure, improve safety, and offer cost-effectiveness, IC-ECG presents a promising method for catheter tip positioning in TIVAD procedures. Based on these advantages, IC-ECG could be considered a preferable method in clinical practice.
Keywords
Introduction
Totally Implantable Venous Access Device 1 (TIVAD) are extensively utilized in the clinical management of cancer patients. A long-term follow-up study indicates that TIVAD are safe for this population 2 and demonstrate superior cost-effectiveness and a reduced incidence of complications compared to Peripherally Inserted Central Catheter (PICC) over the long term. 3 The accurate positioning of the TIVAD catheter tip is essential to mitigate catheter-related complications, including malfunction, thrombosis, vascular and valve erosions, and arrhythmias. In medical practice, the position of the TIVAD tip is frequently determined using intraoperative fluoroscopy. While effective, fluoroscopy presents specific risks, including repeated radiation exposure for patients undergoing frequent procedures, which may contribute to cumulative radiation effects. Additionally, fluoroscopy lacks real-time feedback on catheter tip positioning, potentially leading to suboptimal placements. Previous research has identified the optimal tip position as being between the lower one-third of the superior vena cava and the junction with the right atrium, 4 which can be delineated on chest X-ray as being located 0.8–2.4 vertebral body unit (VBU) from the carina. 5 Intracardiac electrocardiography (IC-ECG) has been demonstrated to be a safe and effective alternative for catheter tip positioning in PICC procedures,6–8 IC-ECG offers several advantages: it eliminates radiation exposure, provides real-time feedback during the procedure, and has been associated with higher positioning accuracy.9,10 However, there is limited data regarding its application in TIVAD cases. Therefore, this study aims to implement the IC-ECG-guided catheter tip positioning method in TIVAD procedures and evaluate its safety and accuracy compared to traditional fluoroscopic guidance.
Materials and method
This study involved a retrospective analysis of patient data collected from The Affiliated Suzhou Hospital of Nanjing Medical University. The study cohort consisted of adult cancer patients who underwent TIVAD placement between January 2023 and June 2024. We employed Propensity Score Matching (PSM) to match 155 patients who had catheter tip positioning guided by IC-ECG (IC-ECG group) with 338 patients who underwent chest X-ray positioning (X-ray group) in a 1:2 ratio, resulting in two groups with comparable baseline characteristics. It is important to note that the Ethics Committee of The Affiliated Suzhou Hospital of Nanjing Medical University reviewed and approved this study in accordance with ethical standards. Since this research involved retrospective data collection, informed consent from patients was not required.
Surgical procedures
All procedures were performed in the operating room under local anesthesia. The internal jugular vein or axillary vein was selected as the target for venous access. Following successful venous puncture under ultrasound guidance, a guidewire was inserted through the puncture needle and advanced 10–15 cm, with placement in the superior vena cava confirmed by either ultrasound or fluoroscopy. The catheter was then advanced through a peel-away sheath into the lower one-third of the superior vena cava. The position of the catheter tip was verified intraoperatively using fluoroscopy or intracardiac electrocardiography (IC-ECG).
The IC-ECG technique involves using the catheter tip as a “moving intracardiac electrode.” The catheter was filled with saline, and a syringe was attached to a metal wire with a blunt needle at its tip. The opposite end of the wire was connected to the ECG electrodes by an assistant. The catheter was advanced slowly while monitoring the changes in the ECG P wave. When the ascending limb of the P wave reached maximum amplitude without a negative P wave, the catheter tip was considered to be in the optimal position. Postoperatively, patients with IC-ECG-guided catheter tip placement underwent chest X-ray (CXR) to confirm the catheter tip position and the integrity of the TIVAD.
Data compilation and definitions
A comprehensive retrospective review of the patients’ medical records was conducted, including demographic data such as age, gender, surgical duration, and complications. Complications were defined as any re-interventions required to address clinical issues, such as infections, thrombosis, or dislocation related to TIVAD implantation. Complications were specifically defined as those occurring within the first 30 days following the procedure. Additionally, the distance from the catheter tip to the carina was measured in vertebral body unit (VBU). This measurement was documented by an experienced interventional physician and a radiologist, with any discrepancies resolved through discussion. A TIVAD tip positioned between 0.8 and 2.4 VBU from the carina 5 was classified as being in the ideal position.
Statistical analysis
All data were processed and analyzed using RStudio for Windows. Quantitative data following a normal distribution were presented as mean and standard deviation (SD; mean ± SD), with a t-test used for comparisons between two samples. Qualitative data were expressed as frequency (n) and percentage (%), with either the Chi-square test or Pearson’s Chi-squared test with Yates’ continuity correction applied as appropriate. Multivariate logistic regression analysis was conducted to identify risk factors associated with TIVAD-related complications. Optimal cutoff values for continuous variables were determined using receiver operating characteristic (ROC) curves, and the area under the curve (AUC) was calculated to assess diagnostic performance. A p-value of <0.05 was considered statistically significant.
Result
A total of 493 adult cancer patients who underwent TIVAD placement between January 2023 and June 2024 were identified. After Propensity Score Matching (PSM), 465 patients were included in the retrospective analysis, comprising 221 males (47.5%) and 244 females (52.5%), with a mean age of 62.6 years. The cohort included 120 cases of breast cancer (25.8%), 84 cases of lung cancer (18.1%), and 64 cases of gastric cancer (13.8%), among others. All patients underwent ultrasound-guided puncture of the target vein in real-time, with the majority (422 cases, 90.8%) accessing the right-sided veins; a smaller proportion accessed the left side, primarily associated with right-sided breast cancer and enlarged right cervical lymph nodes. The average surgical duration was 31.9 ± 5.51 min. Based on the method used for catheter tip positioning, patients were divided into the IC-ECG and X-ray groups. As shown in Table 1, after PSM, the differences in BMI were balanced, and the baseline characteristics were comparable between groups.
Comparison of characteristics between the X-ray and IC-ECG groups in the overall population and the propensity score-matched population.
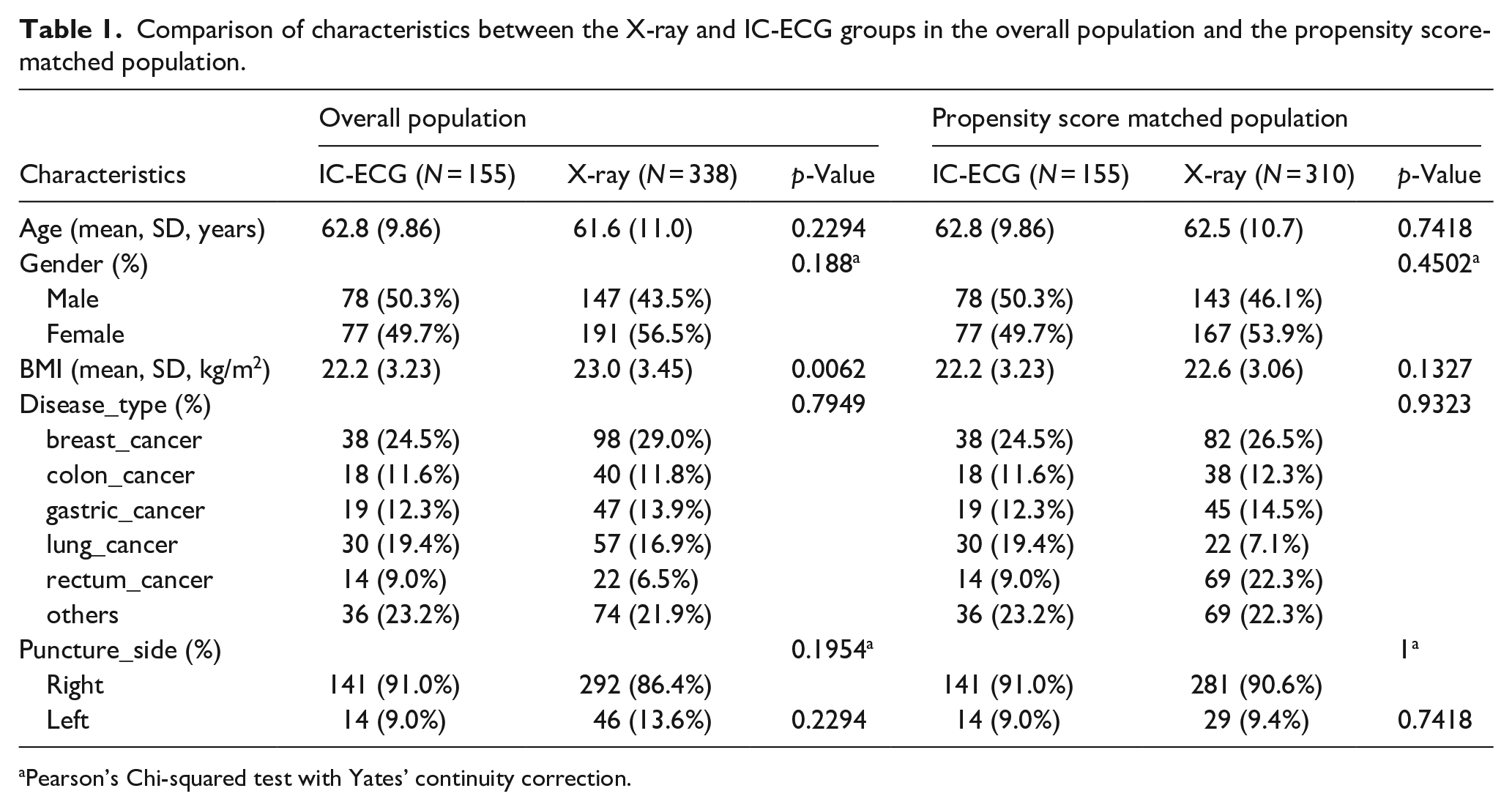
Pearson’s Chi-squared test with Yates’ continuity correction.
In the X-ray and IC-ECG groups, catheter tip positions were determined using intraoperative fluoroscopy and intracardiac electrocardiography, respectively. The ideal position was achieved in 150 cases (96.8%) and 301 cases (97.1%), respectively. The mean distance from the catheter tip to the tracheal carina was 1.60 ± 0.356 and 1.41 ± 0.34 vertebral body units (p < 0.01). Complications occurred in 15 cases (4.8%) in the X-ray group and 7 cases (4.5%) in the IC-ECG group, with the primary complications being local infection, thrombosis, and catheter-related bloodstream infection. Additionally, the average surgical times were 29.7 min for the X-ray group and 33.0 min for the IC-ECG group (p < 0.01), as shown in Table 2.
Primary outcome indicators.
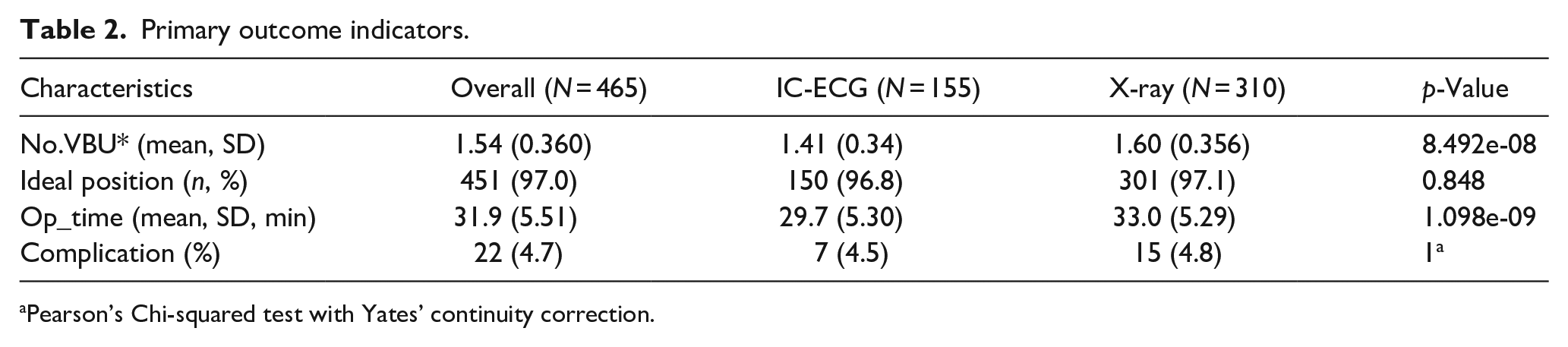
Pearson’s Chi-squared test with Yates’ continuity correction.
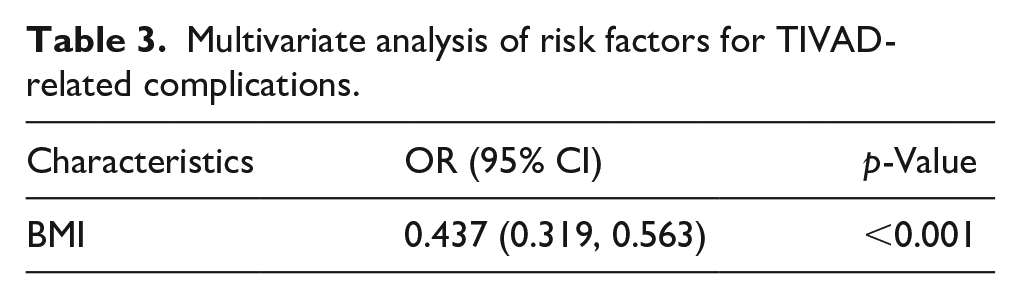
The overall incidence of complications was comparable between the two groups. Multivariate logistic regression analysis, as shown in Table 3, identified BMI as an independent risk factor for TIVAD-associated complications (OR = 0.437, 95% CI: 0.319–0.563, p < 0.001). ROC curve analysis in Figure 1 showed an area under the curve (AUC) for BMI of 0.926 (95% CI: 0.886–0.926, p < 0.001).
Multivariate analysis of risk factors for TIVAD-related complications.
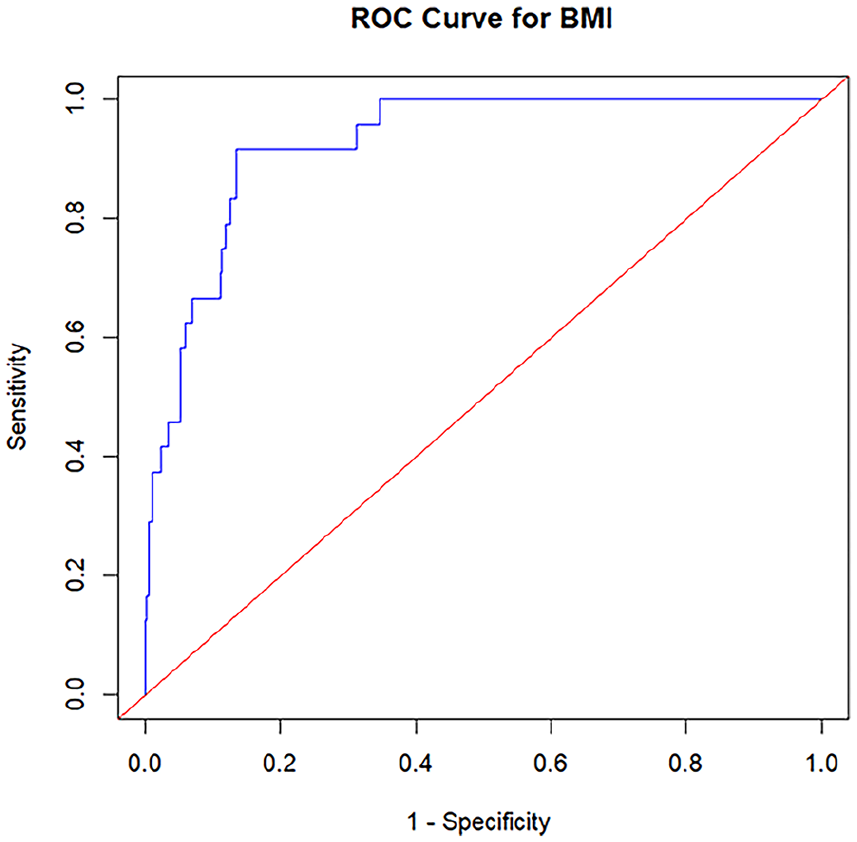
ROC curve of BMI. The AUC of BMI was 0.926 (95% CI: 0.886–0.926, p < 0.001).
Discussion
With the increasing use of TIVAD in clinical practice, precise catheter tip positioning has become crucial for long-term functionality. Although the carina is widely used as a reference point during intraoperative fluoroscopy, 11 this method increases specific risks, particularly repeated radiation exposure for both healthcare providers and patients, raising concerns about cumulative radiation effects. Healthcare workers performing frequent procedures may face long-term occupational risks, such as an increased likelihood of radiation-induced malignancies, underscoring the need for safer alternatives. In recent years, accumulating evidence suggests that non-fluoroscopic techniques for catheter positioning provide a safe alternative.12–14
Previous studies have demonstrated that IC-ECG provides reliable safety and accuracy for positioning peripherally inserted central catheters (PICC).6,7,9 The primary advantage of this technique is its ability to monitor catheter tip position in real time, reducing dependence on traditional imaging methods and thus minimizing radiation exposure. In addition to improving safety, IC-ECG has been shown to be a cost-effective method compared to X-rays, as it eliminates the need for intraoperative and postoperative imaging, which can substantially reduce procedural expenses. These savings are particularly relevant in resource-limited settings, where the high cost of fluoroscopic equipment and maintenance can be prohibitive. 9 Accordingly, this study proposes using IC-ECG to guide the accurate placement of TIVAD catheter tips.
A noteworthy clinical finding is the higher accuracy of IC-ECG in identifying the optimal catheter tip position compared to X-ray methods when using trans-esophageal echocardiography (TEE) as the gold standard.15–17 Studies have shown that IC-ECG offers superior precision in determining the ideal location within the lower third of the superior vena cava, reducing the risks of complications such as arrhythmias or catheter migration. This improvement further supports IC-ECG as a safer, more reliable, and economically advantageous option for TIVAD implantation. 9
According to previous studies,12,18–20 BMI is a known risk factor influencing postoperative complications related to TIVAD. To address this, we applied the Propensity Score Matching (PSM) method to balance baseline characteristics, particularly BMI. We assessed the accuracy and safety of IC-ECG-guided catheter tip placement during TIVAD implantation. The results showed no significant difference in achieving the ideal position between the IC-ECG group and the X-ray group (150 cases (96.8%) vs 301 cases (97.1%), p = 0.848), aligning with previous findings. 14 The accuracy of IC-ECG may be influenced by various factors, including the precision of the IC-ECG equipment, the judgment of the surgical operator, and the medium through which the cardiac signals are conducted. Previous studies 21 have demonstrated that 5.45% and 10% sodium chloride solutions are significantly superior to 0.9% sodium chloride solution in terms of the derived rate of stable intracardiac ECG, the occurrence rate of characteristic P waves, and the time required for catheter tip localization. However, compared to the X-ray group, the IC-ECG group had fewer VBUs from the catheter tip to the tracheal carina (1.41 ± 0.34 vs 1.60 ± 0.356, p < 0.001), which may be attributed to patient positioning. This finding aligns with earlier studies, 22 which demonstrated that transitioning from a supine to an upright position can lead to cranial migration of the catheter tip, with an average shift of 19.34 ± 11.95 mm. All patients in the X-ray group were positioned supine during the procedure, whereas those in the IC-ECG group were upright postoperatively. These results indicate that the retraction distance of the catheter tip is acceptable and remains within the ideal positioning range. Therefore, we conclude that the IC-ECG-guided method for TIVAD catheter tip positioning is accurate. We propose that routine postoperative chest X-rays may not be necessary, potentially reducing healthcare costs and radiation exposure.
The overall incidence rate of TIVAD-related complications in this study was 4.7% (22/465), consistent with previous research findings.23,24 Given the known impact of BMI on postoperative complications, the PSM method was applied to ensure balanced baseline characteristics between the two groups. The complication rates were comparable between the X-ray group and the IC-ECG group (4.5% vs 4.8%, p = 1.0). This indicates that IC-ECG-guided TIVAD placement is safe in the short term and does not lead to a higher incidence of complications. However, this may be influenced by the shorter follow-up period, which could limit the detection of potential long-term complications; therefore, extended follow-up is warranted. Overall, the safety profile of IC-ECG for catheter tip positioning in TIVAD is acceptable. The IC-ECG method can be considered a viable alternative to the standard fluoroscopic technique for catheter tip positioning. When combined with its cost-effectiveness and comparable safety, IC-ECG represents a viable alternative to fluoroscopy for catheter tip positioning in clinical practice.
Additionally, multivariate analysis indicated that BMI is an independent risk factor for TIVAD-related complications (OR = 0.437, 95% CI: 0.319–0.563, p < 0.001), consistent with previous studies. 25 In our practice, we observed that patients with a lower subcutaneous fat layer are more prone to infections and poor wound healing post-implantation; therefore, TIVAD placement is not recommended for patients with extreme thinness. In contrast, Liu et al. 12 and Haslik et al. 26 reported that being overweight or obese can substantially increase the thickness of the subcutaneous fatty layer covering TIVADs, which may impede accurate positioning and puncture of the port system. Consequently, further research is warranted to better understand the relationship between BMI and TIVAD-related complications.
This study has several limitations that should be acknowledged. First, it is a single-center retrospective study with a relatively small sample size, and some data were unavailable. Second, the shortened follow-up period may have limited the assessment of adverse events, which could potentially escalate over a longer monitoring duration. Additionally, patient satisfaction was not systematically evaluated. To enhance the accuracy and standardization of the IC-ECG method, future research could explore a quantitative approach to monitoring P wave changes.
Conclusion
IC-ECG-guided catheter tip positioning for TIVAD placement has demonstrated accuracy, feasibility, and safety. Given its potential to reduce radiation exposure, improve safety, and offer cost-effectiveness, IC-ECG presents a promising method for catheter tip positioning in TIVAD procedures. Based on these advantages, IC-ECG could be considered a preferable method in clinical practice.
Footnotes
Acknowledgements
We appreciated clinical departments for data support to the manuscript.
Availability of data and materials
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy agreements and ongoing research. However, they are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This research study was conducted retrospectively from data obtained for clinical purposes. This study was approved by the Ethics Committee of The Affiliated Suzhou Hospital of Nanjing Medical University.
Informed consent
We obtained informed consent for all patients. All methods were performed in accordance with the relevant guidelines and regulations.