
Abstract
This article reports a critically ill patient with extremity fractures caused by a traffic accident. Given the severity of the patient’s condition and the specific nature of the fractures, after a thorough evaluation of the fracture sites, a midline catheter was placed in the affected side’s upper arm through ultrasound guidance as a vascular access solution. The catheter was safely retained for 63 days, completing the entire treatment cycle without any related complications, providing stable and reliable vascular access support for the patient’s overall treatment. This case demonstrates the feasibility of using midline catheters in critically ill patients with extremity fractures, offering new perspectives and references for the selection of vascular access in these patients.
Introduction
With the development of industrialization, the incidence of traumatic fractures caused by falls from height, traffic accidents, and construction site accidents has been increasing annually. Extremity fractures are the most common type of traumatic fracture in these patients. 1 Due to the severity of their condition, patients often require vascular access devices (VADs) for fluid resuscitation, medication administration, and nutritional support. 2 VADs refer to various catheters that enter the bloodstream for medical purposes, which are crucial life-saving channels for critically ill patients. 3
Some scholars have pointed out that vascular access devices (VADs) are classified into “Peripheral Venous Access Devices (PVADs), Central Venous Access Devices (CVADs), and Totally Implantable Venous Access Devices (TIVADs).” PVADs include: Short Peripheral Catheter (SPC) for lengths less than 6 cm, Long Peripheral Catheter (LPC) for lengths between 6 and 15 cm, and Midline Catheter (MC) for lengths greater than 15 cm. CVADs include: Peripherally Inserted Central Catheter (PICC), Centrally Inserted Central Catheter (CICC), and Femoral Inserted Central Catheter (FICC). TIVADs include: PICC-port and FICC-port. 4
However, there are few reports on the placement of midline catheters in the affected side of critically ill patients with extremity fractures.
On December 21, 2023, the patient was admitted to the neurology ICU due to a traffic accident that resulted in altered consciousness (GCS E1V1M4 6 points, MRS 4 points, NHISS score 40). Upon admission, full-body CT scans revealed severe cranial injury, including right frontal and temporal lobe hemorrhages, right frontal epidural hematoma, subdural hematomas beside the falx cerebri and cerebellum, traumatic subarachnoid hemorrhage, fractures of the left temporal, left zygomatic arch, and multiple fractures of the body, including left clavicle, left ribs, right pelvis, and left femur. Severe trauma is often associated with a high risk of deep vein thrombosis (DVT), especially in patients with lower extremity and pelvic fractures, where the risk of venous thromboembolism (VTE) is the highest.5,6
The patient’s condition was critical and required immediate intravenous medication treatment. Given that the peripheral veins were not palpable, ultrasound guidance was used to place the vascular access. Difficult Intravenous Access (DIVA) refers to cases where special interventions are needed to establish and maintain peripheral venous access. 7 Currently, DIVA patients are not considered to necessarily require central access, as they may benefit from ultrasound-guided insertion of peripheral intravenous catheters. 8
Based on the patient’s venous condition, the severity of the trauma, the fracture sites, and the associated thrombotic risk, a decision was made, after consultation with the attending physician, to insert a 4F single-lumen silicone midline catheter into the right upper arm’s basilic vein under ultrasound guidance, with the catheter tip positioned in the right subclavian vein. The catheter was successfully inserted on December 21, 2023, and the patient was transferred to orthopedics on January 23, 2024. The catheter continued to be used, and on January 26, 2024, the patient was transferred to the rehabilitation department. The catheter remained functional and in use until February 22, 2024, when it was successfully removed after 63 days.
It is worth noting that the use of a single-lumen midline catheter positioned in the subclavian vein for long-term use in critically ill patients, relying solely on one single-lumen catheter to complete the entire treatment process, is extremely rare. Therefore, this case has certain clinical value, and the review of related literature supports this approach (Figures 1–4).
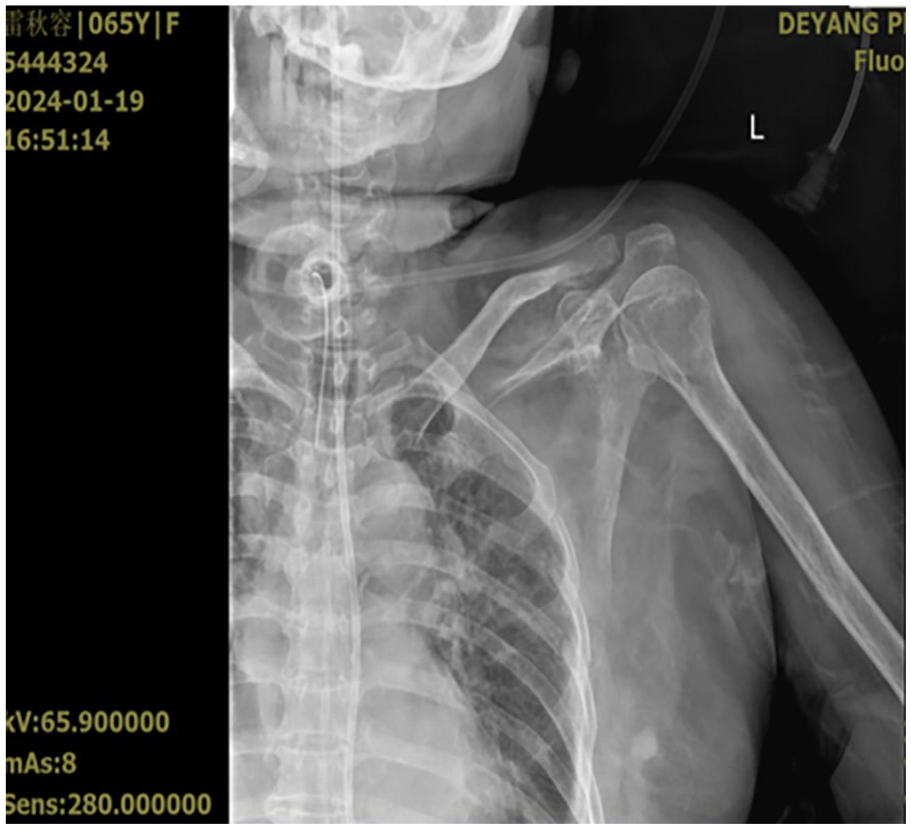
Comminuted fracture of the lateral segment of the left clavicle and fracture of the left third-fifth ribs.
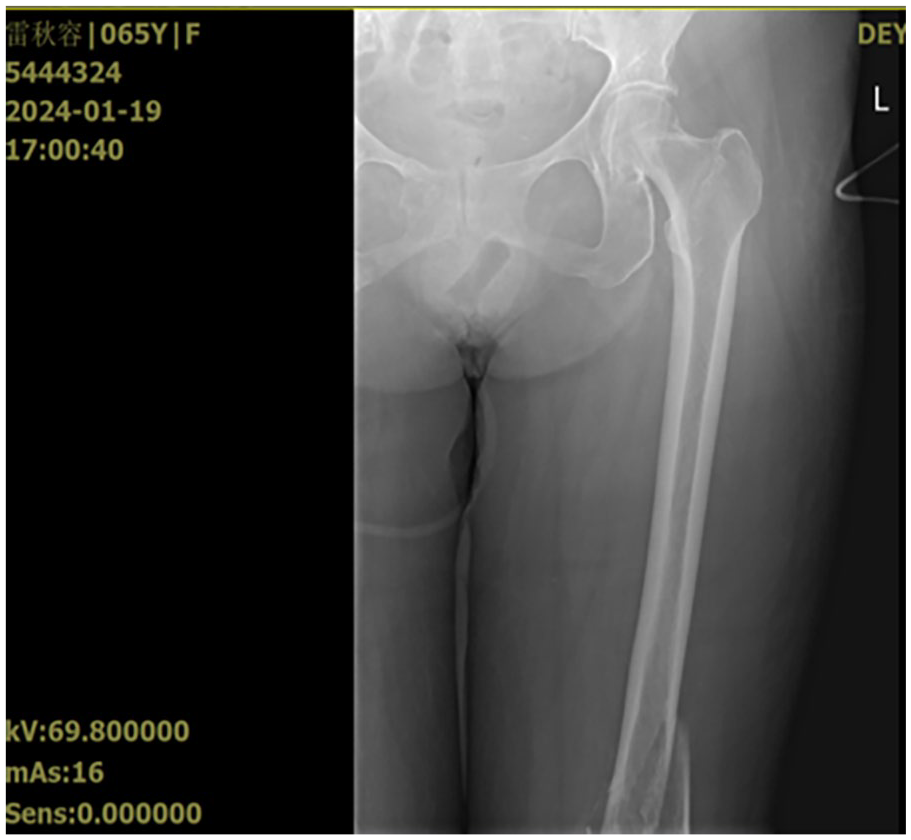
Comminuted fracture of the lower end of the left femur.
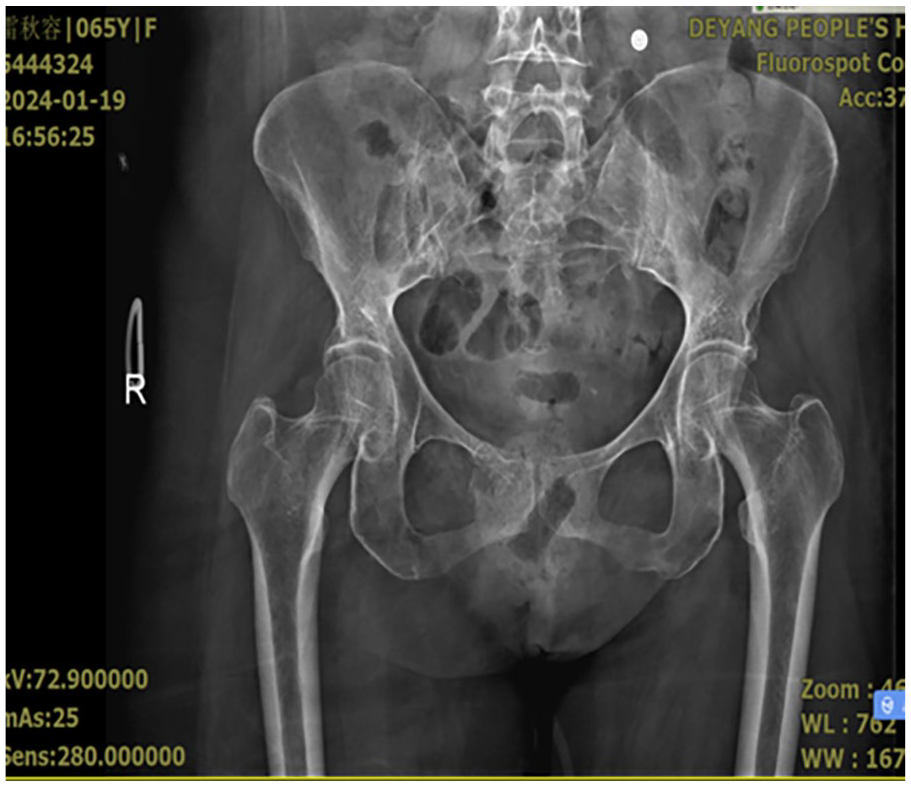
Fracture of the right pubic symphysis, right subpubic branch.

Fracture of the middle part of the right ulnar radius.
Case description
A 65-year-old female patient was admitted on December 21, 2023, due to altered consciousness caused by a traffic accident. Upon admission, full-body CT revealed severe cranial trauma, closed chest and abdominal injuries, and multiple fractures: including left clavicle acromial fracture, multiple rib fractures, right femoral head fracture, right radius and ulna fractures, and left femoral distal fracture. Given the critical condition and specific nature of the fractures, after fully assessing the fracture sites, a 4F single-lumen silicone catheter (28 cm, 2 cm exposed, 27 cm arm circumference on the punctured side) was placed in the right upper arm’s cephalic vein under ultrasound guidance. The catheter tip was located in the same-side subclavian vein. The patient was treated with invasive mechanical ventilation, mannitol + glucose + human serum albumin for dehydration treatment, meropenem for infection control, propofol for sedation, and butorphanol for pain relief. Blood vessel activity was maintained, and nutrition, seizure prevention, and electrolyte balance were supported with intravenous medications. The patient was relatively stable and transferred to the orthopedic department for further treatment on January 23, 2024. On January 26, 2024, the patient was transferred to rehabilitation and continued treatment until the catheter was removed on February 22, 2024, after 63 days of use.
Discussion
Importance of innovative vascular access selection
In critically ill patients with extremity fractures, traditional vascular access is often challenged by trauma and limb swelling. Choosing an effective and durable alternative solution is crucial. Proper pre-placement assessment is key to success. 9 This case demonstrates the effectiveness and safety of midline catheters in critically ill patients with extremity fractures. The successful retention of the midline catheter for 63 days in this patient reflects the strategy’s ability to maintain stable vascular access while effectively supporting the overall treatment process.
Comprehensive assessment of fracture sites and access selection
Patients with lower extremity and pelvic fractures have the highest risk of venous thromboembolism (VTE).5,6 Given the uniqueness of this case, it was crucial to assess the fracture sites and their impact on surrounding tissues when selecting vascular access. The orthopedic team comprehensively considered the fracture type, location, and the potential impact on vascular access when developing the treatment plan. This holistic evaluation of the patient’s condition and local injuries helped select the optimal vascular access solution and offers valuable insight for managing similar cases.
Clinical significance and future research directions
The successful implementation of this case provides a new perspective for the treatment of critically ill patients with extremity fractures. Future multicenter studies should focus on the effects and complication rates of midline catheters in patients with different types of fractures and injuries, providing more comprehensive reference data for clinical practice. Additionally, with the advancement of modern medical technology, exploring more suitable vascular access options for critically ill patients will be an important direction for future research.
Conclusions
The following conclusions can be drawn based on our findings:
(1) Midline catheters can be used as an alternative solution for vascular access in critically ill patients with extremity fractures.
(2) The duration of midline catheter placement should be determined jointly based on the patient’s clinical needs, venous conditions, and catheter function.
(3) Future research should further explore the long-term effects and complication rates of midline catheters in patients with different types of extremity fractures, providing more comprehensive and systematic reference data for clinical practice.
Footnotes
Acknowledgements
The authors are grateful to the patient for providing basic information.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Natural Science Subjects of Sichuan Nursing Vocational College, Grant/Award Number: 2024ZRY38.
Ethical approval
The trial was well-received by the Deyang People’s Hospital Ethics Committee and approved by the study hospital with the review lot number 2023-03-003-K01.