
Abstract
Dear Editor,
Anatomical knowledge often lies dormant in the depths of memory until it surfaces at critical moments in the operating room. This report presents one such encounter, where a routine plan for arterial cannulation took an unexpected turn, reminding clinicians how important it is to stay alert to anatomical differences even in the most familiar procedures.
A 67-year-old female with a history of chronic hypertension was scheduled for radical cholecystectomy under general anesthesia. Given her age, comorbid status, and the anticipated hemodynamic fluctuations during a major abdominal procedure, continuous invasive arterial blood pressure monitoring was planned. Following induction and endotracheal intubation, attempts were made to palpate the right radial pulse only to find that it was conspicuously absent at the expected wrist location. However, the patient was hemodynamically stable. Further examination revealed a superficial pulsation on the dorso-lateral aspect of the forearm running over the anatomical snuff box (Figure 1(a)). Using an L-shaped hockey stick probe (HSP), ultrasound confirmed an artery of good caliber running superficially along this aberrant track (Figure 1(b)). A 20G cannula was placed under ultrasound guidance and transduced, showing a well-formed waveform on the monitor (Figure 1(c)).
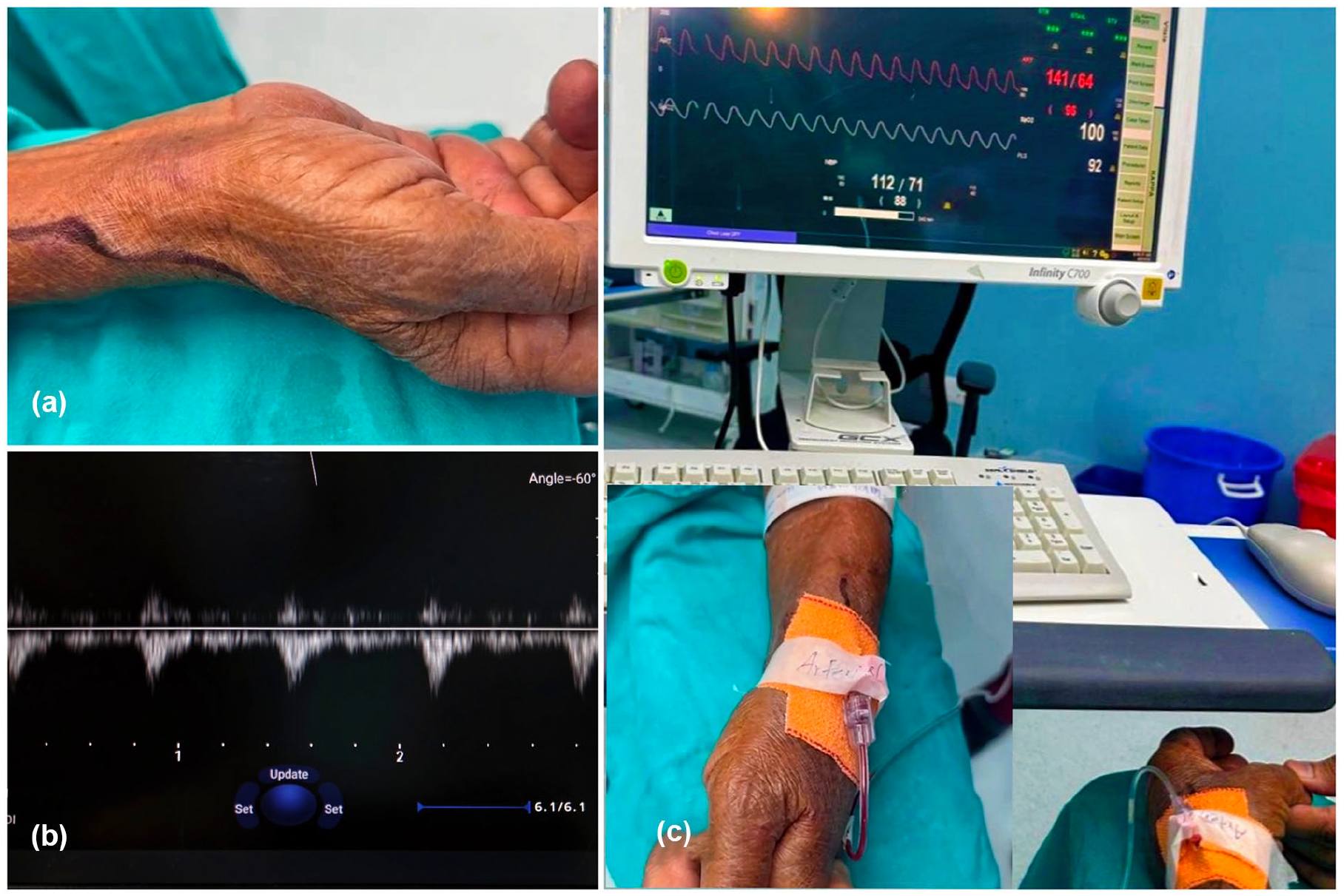
Identification and cannulation of an aberrant high-origin radial artery: (a) aberrant arterial pulsation seen on the dorsolateral forearm over the anatomical snuffbox, with its course marked using a skin marker, (b) point-of-care ultrasound image showing an arterial pulse wave doppler waveform confirming flow along the aberrant track, and (c) successfully cannulated radial artery with a 20G cannula in place and arterial waveform on monitor.
The radial artery is classically described as a branch of the brachial artery arising in the cubital fossa, coursing down the lateral forearm. However, variations in its origin and trajectory are not only possible but also documented. A high-origin radial artery, also known as brachioradial artery, can arise from the axillary or proximal brachial artery and travel along an altered superficial course. Clinically, this variation can lead to challenges such as misidentification as a vein, failed or difficult cannulation, increased risk of accidental injury, or being mistakenly interpreted as hypotension or pulselessness.
Recent cadaveric and imaging-based studies emphasize that radial artery variations are more common than previously thought. Shilpa et al. identified a 6.7% prevalence of high-origin radial arteries arising from the axillary artery in South Indian cadavers. 1 Haładaj et al. found brachioradial arteries in 9.2% of dissected limbs, many of which had a tortuous course and atypical branching patterns that could impact both surgical and endovascular procedures. 2
Mohanty et al. documented a duplication of the radial artery posing diagnostic and procedural challenges. 3 Yang et al. succinctly connected anatomical variation with clinical implications, warning of the potential for failed cannulation, arterial injury, or misinterpretation during angiography. 4
In this case, point-of-care ultrasonography was invaluable for identifying, confirming, and safely accessing the aberrant artery. Moreover, the implementation of standardized ultrasound-guided protocols such as the Safe Insertion of Arterial catheters (SIA) approach can enhance detection of aberrant vascular anatomy and minimize complications during arterial cannulation. 5 The pivotal lesson lies beyond the probe: when anatomical expectations fail, clinicians must think anatomically before they think pathologically. In the absence of a palpable pulse at the conventional site, particularly in elderly or vasculopathic patients, anatomical variation should be a top differential—not hypoperfusion alone.
In modern medicine, especially in operating rooms and intensive care units, peripheral vascular access is frequently used for arterial blood gas analysis, continuous blood pressure monitoring, cardiac output monitoring, and other hemodynamic assessments, with the radial artery being the most commonly accessed site. Therefore, awareness of radial artery anatomical variants must be integrated into both preoperative evaluation and procedural training. While this case supports the routine use of ultrasound for vascular access, it more importantly highlights the enduring need for anatomical literacy in clinical decision-making.
Footnotes
Author contributions
Shikha Jain: Conceptualization, Writing—original draft, Writing—review & editing, Final approval. L Pfokreni: Conceptualization, Writing—original draft, Writing—review & editing. Vaishali Waindeskar: Writing—original draft, Writing—review & editing. Abhinav Vijay: Writing—original draft, Writing—review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was taken from the patient.