
Abstract
The basilic vein is one of the two primary veins used for creating an autogenous arteriovenous fistula in the upper extremity. In the creation of an arteriovenous fistula with basilic vein transposition in the forearm, an incision along the forearm is typically required to prepare the basilic vein. This extensive surgical incision can lead to wound healing issues. In this case, we reported that the basilic vein in the forearm could be prepared endoscopically. This method allowed for avoiding the surgical incision along the vein to be transposed. Endoscopic vein preparation allows for less surgical dissection in basilic vein transposition, and thus may be beneficial in avoiding postoperative wound complications.
Keywords
Introduction
Arteriovenous fistula (AVF) is the prioritized vascular access method for hemodialysis in end-stage renal failure. In creating an AVF, it is advised that it be autogenous and constructed in the forearm. A transposition using the basilic vein located in the forearm is a preferable AVF. Nevertheless, the long surgical incision causes reluctance among surgeons.
With advancements in devices and techniques used for graft harvesting in coronary bypass surgery, the practice and prevalence of vascular endoscopic approaches are increasing. 1 The extensive surgical exploration involved in basilic vein transposition is driving the search for less invasive interventions. 2
The reason for choosing this technique is to avoid wound site complications by reducing skin incision and surgical dissection. Transposition was preferred to facilitate needle cannulation and to improve patient comfort during dialysis. In this case report, the aim is to demonstrate the benefit of the endoscopic approach for vein harvesting and preparation in forearm basilic vein transposition. The patient consented to the publication of the case details and images.
Case report
A 68-year-old female patient with a history of known hypertension, hypercholesterolemia, hyperparathyroidism, glaucoma, polycystic kidney disease, nephrolithiasis, and right upper extremity deep vein thrombosis presented to our clinic for the need of an arteriovenous fistula.
The patient had been undergoing hemodialysis for 45 months with a left distal radiocephalic arteriovenous fistula. Thrombosis occurred in the cephalic vein of the forearm AVF due to thrombophlebitis. The patient continued the hemodialysis program with a right jugular permanent tunneled hemodialysis catheter. During follow-up, the patient developed right upper extremity deep vein thrombosis. Physical examination revealed that the left cephalic vein was thrombosed in a long segment after the arteriovenous anastomosis, and partial flow was observed in the side branches after the anastomosis. The cephalic vein in the arm was found to be less than 2 mm in diameter. However, the basilic vein in the arm showed good development. The basilic vein calibration in the forearm was sufficient for AVF. Since the patient’s radial artery had developed due to the long-term radiocephalic AVF, it was decided to transpose the appropriately sized basilic vein in accordance with the principle of starting distally for AVF creation.
Under regional anesthesia and sedation, the ineffective radiocephalic AVF was first closed. The basilic vein was located through a 2.5 cm transverse incision in the distal forearm and was freed endoscopically up to the proximal side of the medial epicondyle (Figures 1 and 2). A more extensive basilic vein dissection and liberal mobilization were performed, reaching beyond the proximal medial epicondyle. The segment of the basilic vein under the medial epicondyle, previously used as the venous puncture site for the former AVF, was found to be significantly dilated and adhered to the skin. Since the vein was tightly adhered to the skin at the puncture site, it was not suitable for endoscopic dissection. Therefore, a 1 cm skin incision was made, and the vein was dissected from the skin. The basilic vein was transected from the distal forearm and brought out through the area above the medial epicondyle. Its branches were ligated, it was inflated and prepared, and markings were made on the vein to ensure proper alignment and prevent twisting. A tunnel extending to the site of the anastomosis with the radial artery was created using the dissector of an endoscopic vein harvesting device. The basilic vein was then transferred to the pre-prepared radial artery anastomosis site, where it was anastomosed to the radial artery, creating an AVF (Figure 3). A thrill was present. On postoperative day 36, Doppler ultrasonography showed a basilic vein diameter of 5 mm. The patient was subsequently able to undergo effective dialysis through the fistula.

Endoscopic preparation of the basilic vein.
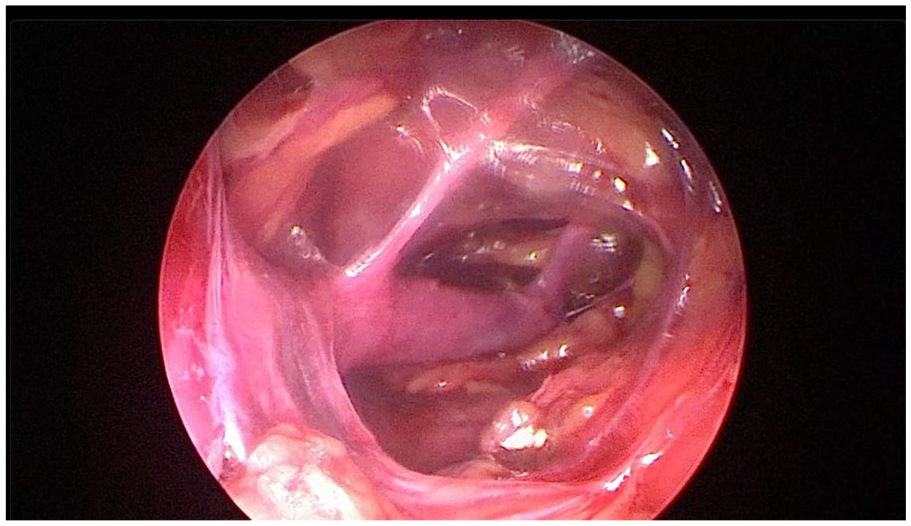
Endoscopic image of basilic vein.
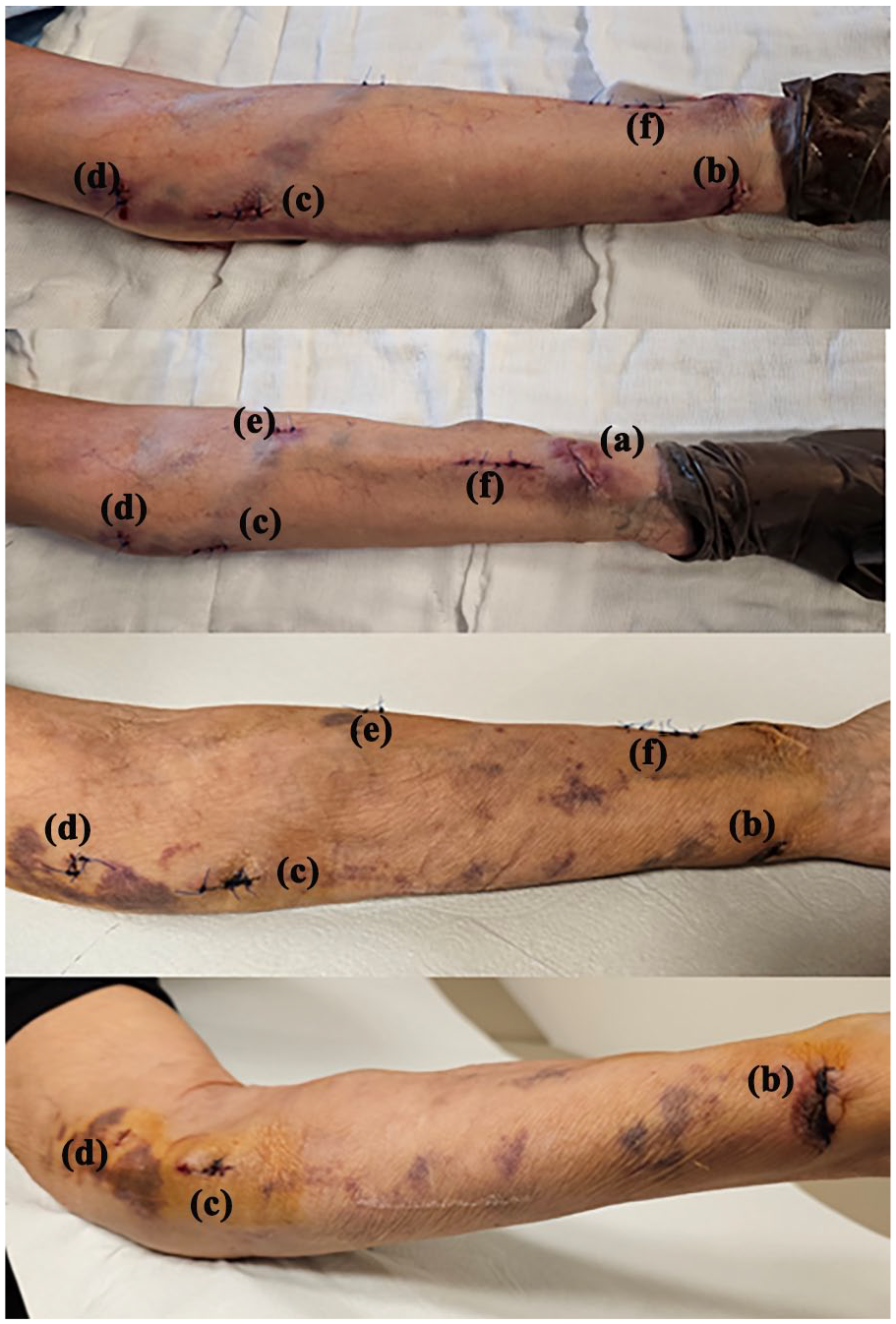
Incisions during AVF closure and endoscopic forearm radiobasilic AVF creation: (a) incision site where the old ineffective AVF was closed, (b) entry point for basilic vein harvesting, (c) incision site made due to adhesions, (d) incision site for exteriorizing and preparing the basilic vein, (e) incision site for exteriorizing through the tunnel and twist control, and (f) incision for anastomosis.
Discussion
The basilic vein lies deep in the arm, and when an AVF is created using the basilic vein, superficialization or transposition is necessary for hemodialysis to be performed. Extensive surgical dissection has led surgeons to adopt minimally invasive approaches. In a brachiobasilic AVF created using a minimally invasive approach with a laryngoscope, efforts were made to limit the incision area with two incisions: one at the anastomosis site and another just before the axilla. 3 In forearm AVF creation, vascular access was established by endoscopically harvesting the saphenous vein. 4
A limited number of studies on brachiobasilic vein transposition have been published with the use of endoscopic vascular harvesting devices. One study conducted with the same device we used in our surgery includes 11 patients who underwent endoscopic basilic vein transposition. In that study, two preventable complications occurred: bleeding due to an unligated side branch and thrombosis resulting from vascular geometry distortion due to insufficient vessel mobilization. The fistula maturation rate was 100%. 5 In the AVFs created with the basilic vein in the forearm included in our study, superficialization was not required, but transposition was necessary. There are two stages to forearm basilic vein transposition. The first involves freeing and preparing the basilic vein, and the second involves creating a tunnel extending to the lateral side of the volar surface of the forearm and passing the vein through this tunnel. 6 An incision is made along the forearm to free and prepare the basilic vein. With endoscopic preparation of the basilic vein, a long forearm incision is not required. Fewer incisions may help reduce postoperative complications such as infection and wound healing disorders. This benefit may become more pronounced in obese patients requiring more extensive dissection and in diabetic patients with impaired wound healing.
In the literature, a limited number of studies on endoscopic basilic vein transposition have reported the creation of brachiobasilic AVF in the arm. In this case, however, the endoscopic basilic vein transposition was performed in the forearm, and a radiobasilic AVF was created. We aimed to demonstrate that endoscopic AVF can be used not only for the creation of brachiobasilic AVF in the arm but also for the creation of forearm radiobasilic AVF.
In this case, we opted to create an AVF using the forearm basilic vein and radial artery. The patient’s history of a radiocephalic AVF contributed to the presence of a radial artery with well-developed flow. Transposing the forearm basilic vein to the radial artery helps avoid an anastomosis with the ulnar artery, the dominant artery of the hand, and may also reduce the risk of potential distal ischemia.
Additionally, ulnar artery–basilic (UB) vein AVF can be performed on the medial volar surface of the forearm with a limited incision, and it shows secondary patency comparable to that of radiocephalic AVF. 7 The forearm basilic vein can be prepared endoscopically and an AVF can be created with the ulnar artery. In endoscopic forearm basilic vein transposition, the port entry aligns with the surgical incision of the ulnar-basilic AVF. Unlike in our case, this allows AVF creation at the endoscopic port site without the need for a secondary radial incision.
Endoscopic preparation of the basilic vein requires specific training for the surgeon. The endoscopic method can be applied in native tissue. If there is a surgical history in the area where the basilic vein is to be prepared, endoscopic preparation of the vein is not possible.
Conclusion
The preparation of the basilic vein for AVF creation via forearm basilic vein transposition can be effectively performed using an endoscopic method. This approach, requiring less surgical dissection, may help prevent postoperative wound complications.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.