
Abstract
Background:
Percutaneous transluminal angioplasty (PTA) for dysfunctional radial cephalic arteriovenous fistulas (RC-AVF) is associated with severe pain. This study evaluates the effectiveness of ultrasound-guided selective cutaneous nerve block (SCNB) in reducing procedural pain.
Methods:
A total of 292 dialysis patients with RC-AVFs undergoing 292 PTA procedures were retrospectively reviewed. Patients were categorized into three groups based on the anesthesia method: infiltration anesthesia (IA, n = 50), ultrasound-guided infiltration anesthesia (USIA, n = 74), and USIA combined with SCNB (USIA + SCNB, n = 168). SCNB targeted the lateral antebrachial cutaneous nerve (LACN) in all cases, with additional superficial radial nerve (SRN) blocks performed in 106 cases at the operator’s discretion. Ultrasound imaging with an 18 MHz linear probe was used to visualize nerves and veins, and 1% lidocaine was administered using a 25G 25 mm needle. Pain was assessed using the Numerical Rating Scale (NRS).
Results:
No significant differences in baseline characteristics were observed among the IA, USIA, and USIA + SCNB groups. The mean NRS pain scores during balloon inflation were significantly lower in the USIA + SCNB group (2.33 ± 2.08) compared to the IA group (5.24 ± 2.34, p < 0.001) and the USIA group (4.14 ± 2.70, p < 0.001). Among 38 cases with isolated forearm lesions, there was no significant difference between LACN-only and LACN + SRN blocks (2.42 ± 2.04 vs 2.63 ± 1.92, p = n.s.). However, in 75 cases with isolated peri-anastomotic lesions, the addition of an SRN block significantly reduced pain compared to LACN block alone (1.77 ± 1.82 vs 3.00 ± 1.78, p < 0.05).
Conclusion:
SCNB, particularly LACN block for forearm stenosis and combined LACN + SRN block for peri-anastomotic lesions, effectively reduces pain during PTA of RC-AVFs. When combined with USIA, SCNB further enhances analgesic effectiveness during PTA, and the two methods demonstrate a synergistic effect. This method provides safe, motor-sparing anesthesia, improving patient comfort in endovascular procedures.
Keywords
Introduction
Arteriovenous fistulas (AVFs) are essential for performing hemodialysis but can become dysfunctional due to various factors such as venous intimal hyperplasia, stenosis with a shrinking pattern, calcification, and thrombotic occlusion. Maintaining the patency of these AVFs is critically important. Percutaneous transluminal angioplasty (PTA) is widely used as the first-line treatment for dysfunctional dialysis AVFs because it is less invasive than surgical options and can be performed on an outpatient basis. 1
Various methods are available for pain management during PTA, including infiltration anesthesia (IA), nerve blocks, and intravenous anesthesia. However, the KDOQI guidelines do not specify a standardized approach for pain relief management during PTA.1–4 Hemodialysis patients often have multiple underlying diseases and comorbidities and exhibit a high rate of restenosis, with approximately 70% requiring reintervention within 12 months. 5 Consequently, IA, which has fewer complications, is commonly chosen. Nevertheless, IA often fails to provide adequate pain relief. Recently, more precise methods like ultrasound-guided infiltration anesthesia (USIA) have been developed to specifically target the posterior wall of the vein and its surroundings at the stenosis site. 6
Brachial plexus blocks and intravenous anesthesia can provide effective pain relief but are associated with side effects such as motor paralysis and tongue depression, requiring postoperative monitoring and hospitalization, making them unsuitable for outpatient-oriented care.3,4
The introduction of drug-coated balloons (DCBs) has significantly extended the patency periods of dialysis AVFs, 7 yet the intolerable pain experienced by patients during balloon dilation remains a drawback of PTA for dialysis AVF dysfunction, presenting a significant challenge for adequate pain relief.2–4,6,8
Recent advancements in ultrasonographic anatomy have enabled the precise identification of cutaneous nerves, which are sensory nerves that do not include motor fibers. 9 Matsuda et al. have demonstrated the effectiveness of pain relief during vascular dilation at the stenosis site by primarily blocking the musculocutaneous nerve (MCN), crucial for the sensation of the anterolateral forearm, thus minimizing motor paralysis. 10 This report included cases where lateral antebrachial cutaneous nerve (LACN), a terminal sensory branch of the MCN, was blocked.
Consequently, cutaneous nerve blocks can effectively block sensory nerves without causing motor paralysis. To enhance the efficacy of traditional IA and USIA, we initiated ultrasound-guided selective blockade of the LACN and superficial radial nerve (SRN) in the forearm, targeting areas corresponding to the sensory distribution of the stenotic lesions.
This study aims to retrospectively assess and compare the pain levels during PTA with traditional IA alone versus those with the addition of selective cutaneous nerve blocks (SCNB), in order to evaluate the optimal choice of nerve block based on the lesion location.
Methods
Registration of patients and PTA sessions: This retrospective, single-center study adhered to the principles of the Declaration of Helsinki and received approval from the Certified Review Board of the Saitama Medical Center, Saitama Medical University (Approval Number: 2024-113). A total of 372 adult patients undergoing hemodialysis were registered, and between January and December 2023 (Figure 1).
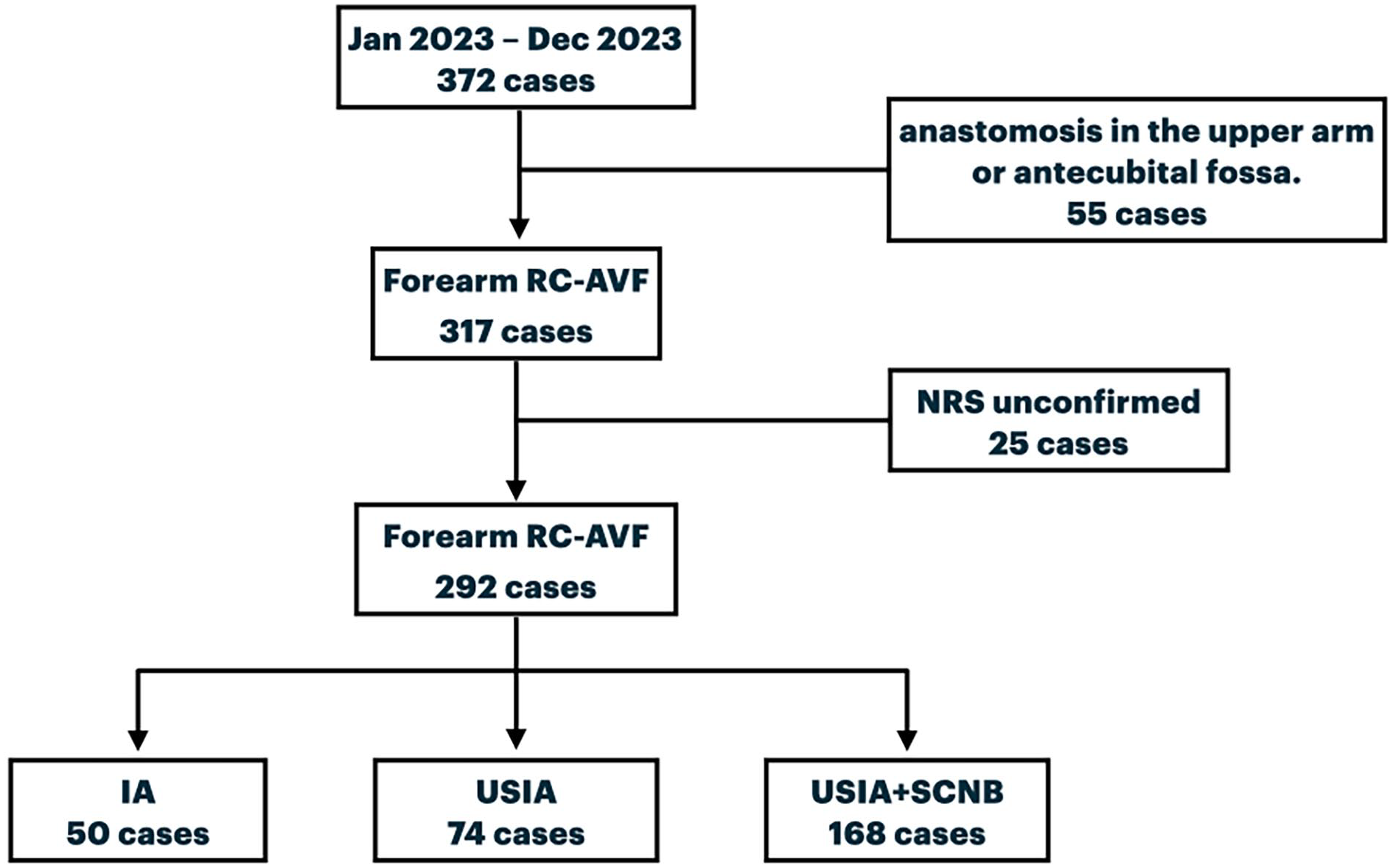
Flow chart.
Inclusion criteria
Patients with radiocephalic arteriovenous fistulas (RC-AVFs) with anastomoses near the wrist.
Patients with at least one stenosis along the cephalic vein, extending from the anastomosis to the antecubital fossa.
PTA was indicated for patients who met at least one of the following conditions: 3-1. A mean brachial artery blood flow (Vascular Access flow) of less than 350 mL/min and a RI greater than 0.65, confirmed by preoperative ultrasound. 3-2. Access troubles such as blood removal failure or difficulty in hemostasis during dialysis sessions and a mean brachial artery blood flow (Vascular Access flow) less than 500 mL/min.
Exclusion criteria
Patients with AVFs that did not have anastomoses near the wrist.
Patients for whom Numeric Rating Scale (NRS) scores during balloon dilation could not be obtained.
Patients who declined participation through informed consent documents.
Pregnant women or those with potential pregnancy.
Patients diagnosed with cancer.
Any other cases deemed unsuitable by the principal investigator.
During PTA, one of the following anesthesia methods was performed: IA, USIA, or USIA combined with SCNB of either the LACN or both the LACN and the SRN. The choice of anesthesia method was determined by the operator, with ultrasound-guided cutaneous nerve blocks actively performed for patients who had previously experienced severe pain during PTA. The technique for ultrasound-guided block used in this study was new to our department, and some results reflect the initial phase of our “learning curve.” Ultimately, NRS scores during balloon dilation were evaluated for 292 patients with RC-AVFs having anastomoses near the wrist: 50 cases with IA, 74 cases with USIA, and 168 cases with USIA + SCNB (Figure 1).
Infiltration anesthesia and ultrasound-guided infiltration anesthesia: IA involves the direct injection of 1% lidocaine (5–10 mL) into subcutaneous tissue or tissue surrounding a specific small area, targeted based on palpation and angiographic findings, performed immediately before balloon dilation during the PTA session. In contrast, USIA involves injecting 1% lidocaine in a cradle-like pattern to the lateral and inferior aspects of the stenosis, identified using ultrasound during the final examination before the start of the PTA session.
Selection of the cutaneous nerve for blockade: LACN, which sensorily innervates the anterolateral region of the forearm where the cephalic vein from the AVF is located, was anesthetized under ultrasound guidance before all PTA sessions. SRN, providing sensory innervation to the dorsolateral area of the palm, was added based on the operator’s judgment, due to the SRN’s sensory innervation not always corresponding to the area of stenosis and the effectiveness being unclear during the initial phase of our “learning curve.”
Methods and effectiveness assessment of ultrasound-guided cutaneous nerve block: The ultrasound-guided cutaneous nerve block was performed with the patient in the supine position and the upper limb abducted, while the operator sat caudally. A 5–18 MHz linear probe was used to visualize the nerves on a monitor of the ultrasound device (SONIMAGE HS2; KONICA MINOLTA, JAPAN), and a 25G 25 mm needle (TERUMO needle; TERUMO, JAPAN) was guided accordingly. A short-acting 1.0% lidocaine (4.0 mL per nerve) was administered around each nerve in real-time under ultrasound guidance. The LACN is located near the boundary between the biceps brachii tendon and the brachialis muscle, close to the elbow joint.
In the antecubital fossa, the LACN pathway from the posterior side of the biceps brachii tendon laterally (Radial side) upwards, and after elevating, it distributes medially around the median cephalic vein. With the elbow extended, the nerve was identified using the echo probe in a short-axis view near the skin layer within the honeycomb-like structures at the elbow, where the medication was administered (Figure 2(a)).
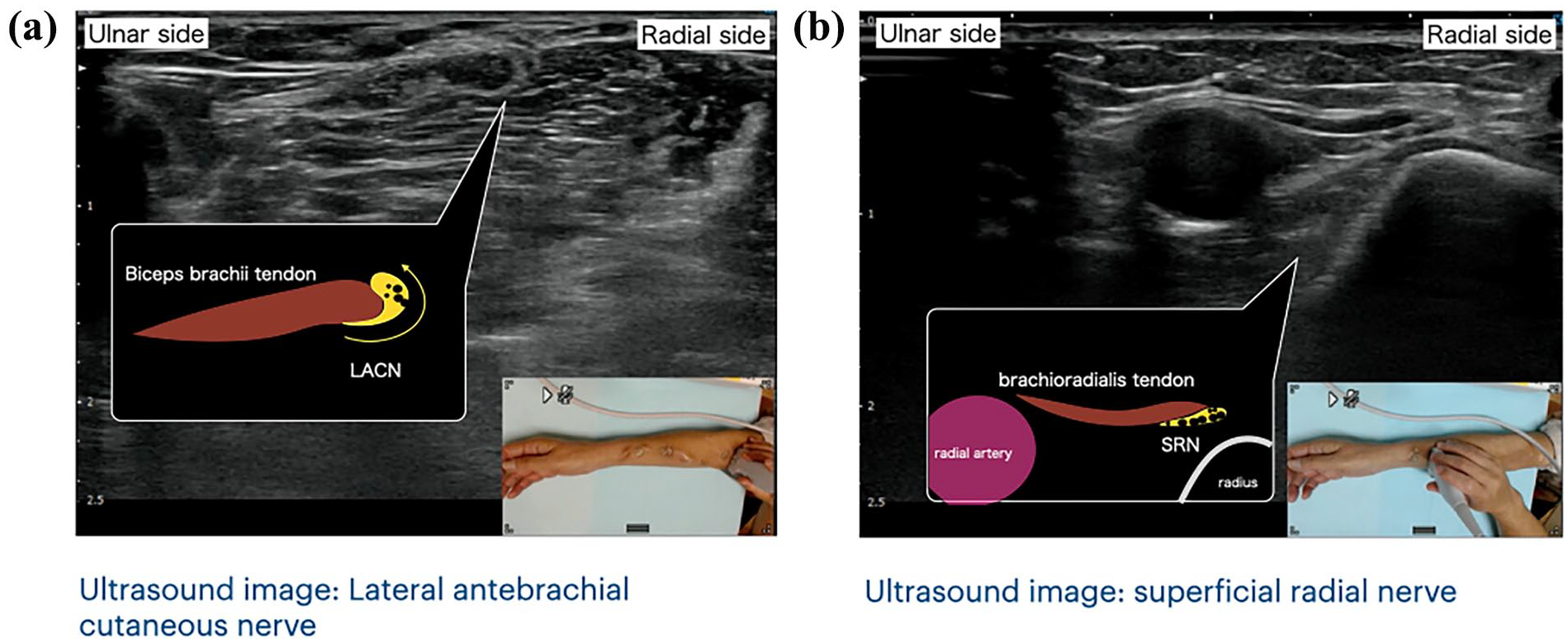
Localization of the cutaneous nerves LACN and SRN: (a) a landmark for the LACN is the biceps brachii tendon in the antecubital fossa, where the nerve pathway from the posterior side of the tendon laterally (radial side) and upwards and (b) a landmark for the SRN is the brachioradialis tendon near the wrist, where it lies between the radial artery and the radius and is located posterior side to the brachioradialis tendon. More distally (toward the wrist), the SRN is located on the radial side and extends upwards from the brachioradialis tendon.
SRN pathway from beneath the brachioradialis tendon and between the radial artery and the radius. Near the radial styloid process, it courses from the dorsal side of the brachioradialis tendon to the radial side and becomes superficial. With the elbow extended and externally rotated, the nerve was visualized using the echo probe in a short-axis view near the radial styloid process, and medication was administered at the site located dorsally to the brachioradialis tendon (Figure 2(b)).
The effectiveness of the pure sensory nerve blocks of the LACN and SRN was confirmed by evaluating sensory hypoesthesia in the innervated areas using an alcohol swab rubbing technique, performed at least 5 min after the nerve block, and based on classical dermatomal maps. Hypoesthesia in the lateral forearm indicated successful LACN blockade, while hypoesthesia over the dorsolateral aspect of the hand confirmed SRN blockade. When the anastomotic site was considered close to the SRN’s sensory territory, an SRN block was additionally performed at the operator’s discretion. However, the location of the anastomosis did not always correspond precisely with classical dermatomal maps, and the decision to perform SRN blockade was made selectively based on the operator’s judgment.
Ultrasound-guided cutaneous nerve blocks were performed in the order of the LACN followed by the SRN. This sequence, starting from the more proximal site, was intended to achieve effective pain relief in the distal regions. Similarly, USIA was performed after the nerve blocks for the same purpose of enhancing distal analgesia. In all cases where ultrasound-guided nerve blocks were performed, 1% lidocaine was additionally administered in a cradle-like pattern around the lesion using USIA. This approach aimed to enhance pain management by combining traditional IA and USIA with ultrasound-guided nerve blocks. Furthermore, USIA was performed after the nerve block to reduce the pain associated with the USIA procedure itself.
Assessment of pain intensity during balloon inflation in PTA: The level of pain was assessed using the NRS, which allows for rapid verbal responses and has a high correlation with the Visual Analog Scale (VAS). 11 During maximum pressure inflation at the primary stenosis site, pain was self-reported by patients on a scale from 0 (no pain), 2 (mild pain), 4 (slightly more pain), 6 (more pain), 8 (substantial pain), to 10 (worst possible pain). In cases where multiple lesions were present, the primary lesion causing access failure was evaluated.
Definition of lesion sites in arteriovenous fistulas: Peri-anastomotic lesions were defined as those extending from the radial artery inflow to the anastomosis and continuing to the site where the dorsal vein merges into the cephalic vein. Forearm lesions were defined as those extending proximally along the forearm cephalic vein from the junction where the dorsal vein merges into the cephalic vein, up to the level where major venous branches—including communicating veins, the median basilic vein (ulnar side), and the median cephalic vein (radial side)—diverge. Antecubital fossa lesions were defined as lesions involving the communicating veins, the median basilic vein (ulnar side), and the median cephalic vein (radial side).
Evaluation criteria
NRS scores during balloon inflation for each anesthesia method.
To evaluate the effectiveness of the SRN block, sessions involving only forearm lesions (excluding peri-anastomotic lesions) were analyzed to compare NRS results between LACN block alone and both LACN and SRN blocks.
Additionally, sessions involving only peri-anastomotic lesions (excluding forearm lesions) were analyzed to compare NRS results between LACN block alone and both LACN and SRN blocks.
Factors influencing moderate to severe pain, defined as NRS scores of 5 or higher, were analyzed based on lesion site, lesion characteristics, treatment factors, and complications.
PTA procedure: USIA and SCNB were performed approximately 5 min before the start of the procedure, followed by basic disinfection 10 min after the anesthesia, and then the procedure was started. Prior to sheath insertion, local infiltration anesthesia was administered at the puncture site. A 4, 5, or 6 Fr sheath was inserted over the cephalic vein, most often via retrograde insertion. Venography was performed to confirm the target stenosis site. After passing a 0.035-inch guidewire through the lesion, balloon catheters using either super non-compliant or semi-compliant balloons were selected, with diameters of 4, 5, or 6 mm appropriate to the proximal and distal sizes of the vessels. If IA was chosen, 1% lidocaine was administered around the stenosis area before balloon dilation. Balloon dilation was carried out until full expansion or until reaching the balloon’s rated burst pressure, maintaining pressure for at least 30 s and up to 1 min. The NRS score was assessed at the time of maximum inflation pressure. If patients experienced severe pain or if unexpected dilation of an unplanned area was required, additional infiltration anesthesia was administered. Finally, venography confirmed the resolution of stenosis, the sheath was removed, hemostasis was achieved through suturing, and the procedure was concluded.
Post-procedural management: After the PTA session, patients underwent an ultrasound examination to assess functionality and confirm hemostasis before discharge. The use of cutaneous nerve blocks, which do not cause motor paralysis, allowed patients to be discharged without waiting for the resolution of sensory anesthesia. The effects of the short-acting lidocaine used for the blocks dissipated approximately 1.5–2.0 h after completion.
Statistical analysis: The 292 cases with RC-AVFs were divided into groups receiving IA, USIA, and SCNB. The significance of differences between each pair of the three groups was determined using analysis of variance (ANOVA) followed by Bonferroni-corrected two-sided multiple t-tests (three comparisons across three groups). Subsequently, to verify the most effective cutaneous nerve block technique by lesion site, parametric tests such as t-tests and non-parametric tests such as U-tests were conducted, and chi-squared test was used to compare categorical data. To identify factors contributing to pain, lesion factors, treatment factors, and complications were used as explanatory variables in logistic regression analysis. This analysis was performed using the SPSS microcomputer assistance program (Version 20.0; IBM Corp., Armonk, NY) running on Windows. A p-value of <0.05 was considered statistically significant.
Results
Demographics and clinical characteristics were shown in Table 1. In this study, 292 patients were registered, of whom 107 (36.6%) were female. The average age at the time of PTA session was 73.5 ± 12.4 years. Among these patients, diagnoses included diabetic nephropathy (n = 95, 32.5%), chronic glomerulonephritis or nephrotic syndrome (n = 62, 14.0%), renal sclerosis (n = 42, 9.5%), hereditary kidney diseases such as autosomal dominant polycystic kidney disease (n = 6, 1.4%), and undiagnosed conditions (n = 87, 19.6%). The mean duration of dialysis was 8.7 ± 14.5 years, and on average, 8.9 ± 20.0 years had elapsed since the creation of their AVFs. Pre-PTA Vascular Access (VA) flow was 381.3 ± 246.8 mL/min, and the Resistive Index (RI) was 0.70 ± 0.17, indicating impaired VA function. De novo lesions were observed in 72 cases (24.7%), and recurrent lesions in 220 cases (75.3%). The balloons used for dilation included Super Non-Compliant Balloons (SNCB) in 174 cases (59.6%) and Semi-Compliant Balloons (SCB) in 118 cases (40.4%). The balloon size was 5.5 ± 0.7 mm, and the balloon length was 55.5 ± 25.1 mm. The maximum inflation pressure was 24.9 ± 7.6 atm. Post-PTA VA flow was 621.8 ± 275.8 mL/min, and RI was 0.58 ± 0.11. The 3-month TLPP rate was 86.3% (252/292).
Baseline demographics and clinical characteristics.
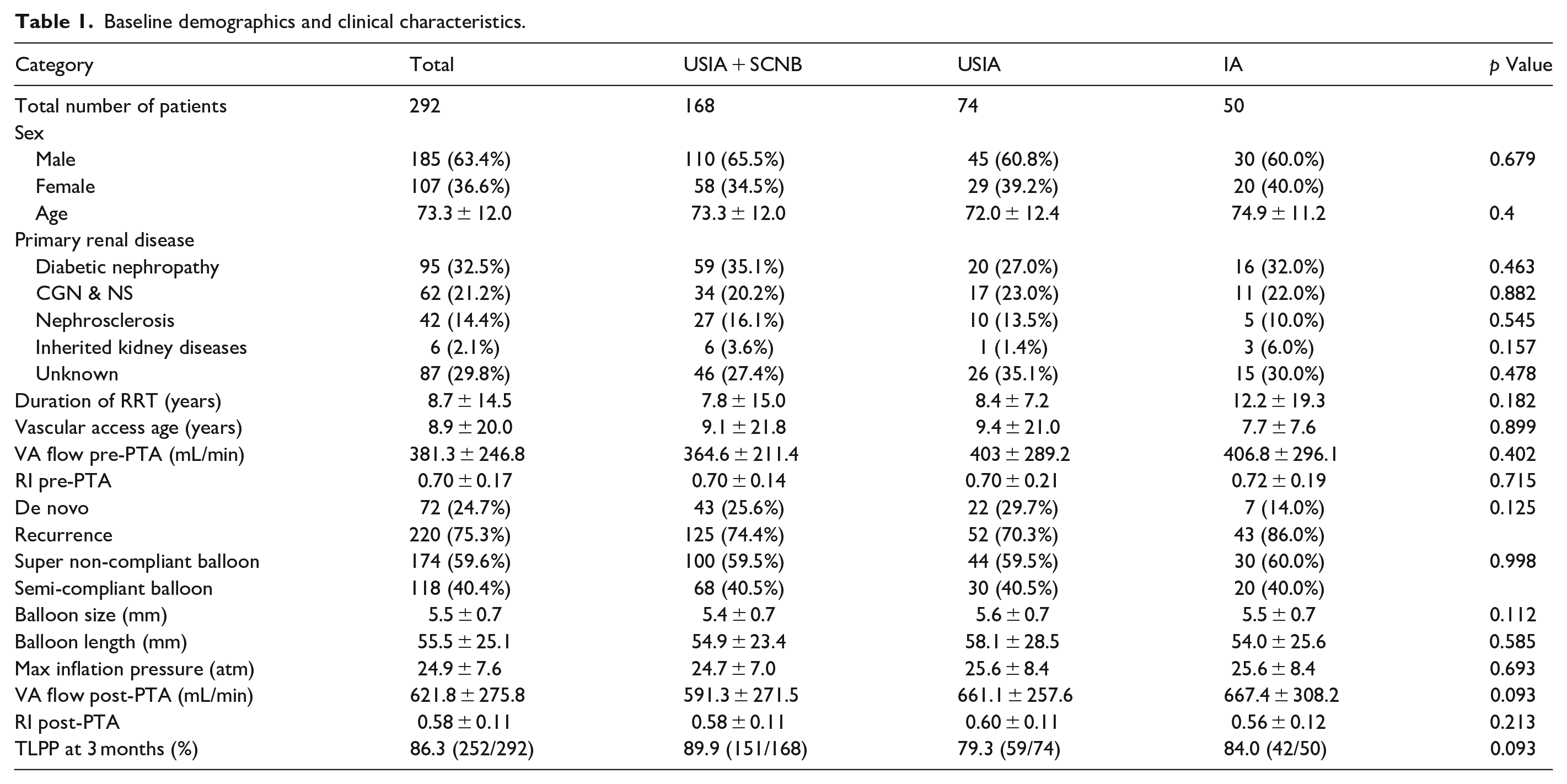
IA was administered in 50 cases, USIA in 74 case, and USIA combined with SCNB in 168 cases. The demographics and clinical characteristics of the IA, USIA, and USIA + SCNB groups are presented in Table 1. No statistically significant differences were observed in demographic and clinical characteristics among the IA, USIA, and USIA + SCNB groups. Every nerve block was successful, with all cases involving a block of the LACN. Specifically, LACN alone was blocked in 62 cases, and an additional block including the SRN was executed in 106 cases. Additionally, all nerve block procedures were followed by USIA at the stenosis site. No anesthesia-related complications such as hematoma formation, nerve damage, or lidocaine toxicity were observed. The mean NRS scores were as follows: 5.24 ± 2.34 in the 50 IA cases, 4.14 ± 2.70 in the 72 USIA cases, and significantly lower at 2.33 ± 2.08 in the 168 USIA + SCNB cases, demonstrating effective pain reduction during venous stenosis dilation (Figure 3).
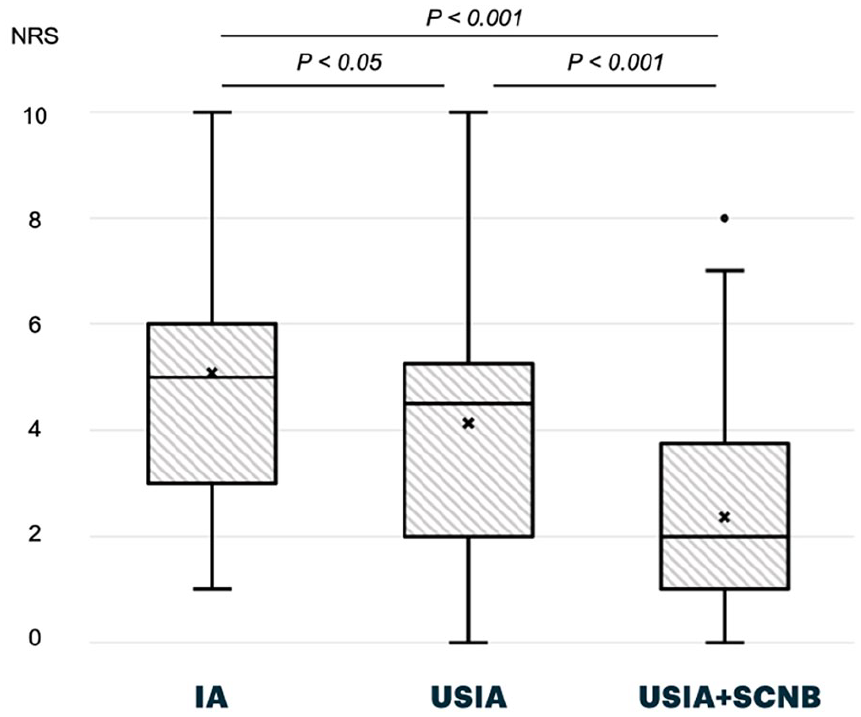
NRS by anesthesia type.
Among the 168 patients who underwent USIA + SCNB, lesion distribution was as follows: isolated peri-anastomotic lesions were observed in 75 cases (18 in the LACN group and 57 in the SRN + LACN group), isolated forearm lesions in 38 cases (19 in each group), and isolated antecubital lesions in 8 cases (6 in the LACN group and 2 in the SRN + LACN group). In addition, combined peri-anastomotic and forearm lesions were found in 37 cases (16 in the LACN group and 21 in the SRN + LACN group), while forearm and antecubital lesions coexisted in 4 cases (2 in each group). Only a small number of patients (6 cases) presented with extensive lesions involving all three regions—peri-anastomotic, forearm, and antecubital—with 1 in the LACN group and 5 in the SRN + LACN group. No cases exhibited a combination of peri-anastomotic and antecubital lesions without forearm involvement. To eliminate the potential influence of multiple balloon inflations on NRS scores, we evaluated the effect of selective cutaneous nerve blocks using only cases with a single primary lesion: 75 cases with isolated peri-anastomotic lesions and 38 cases with isolated forearm lesions.
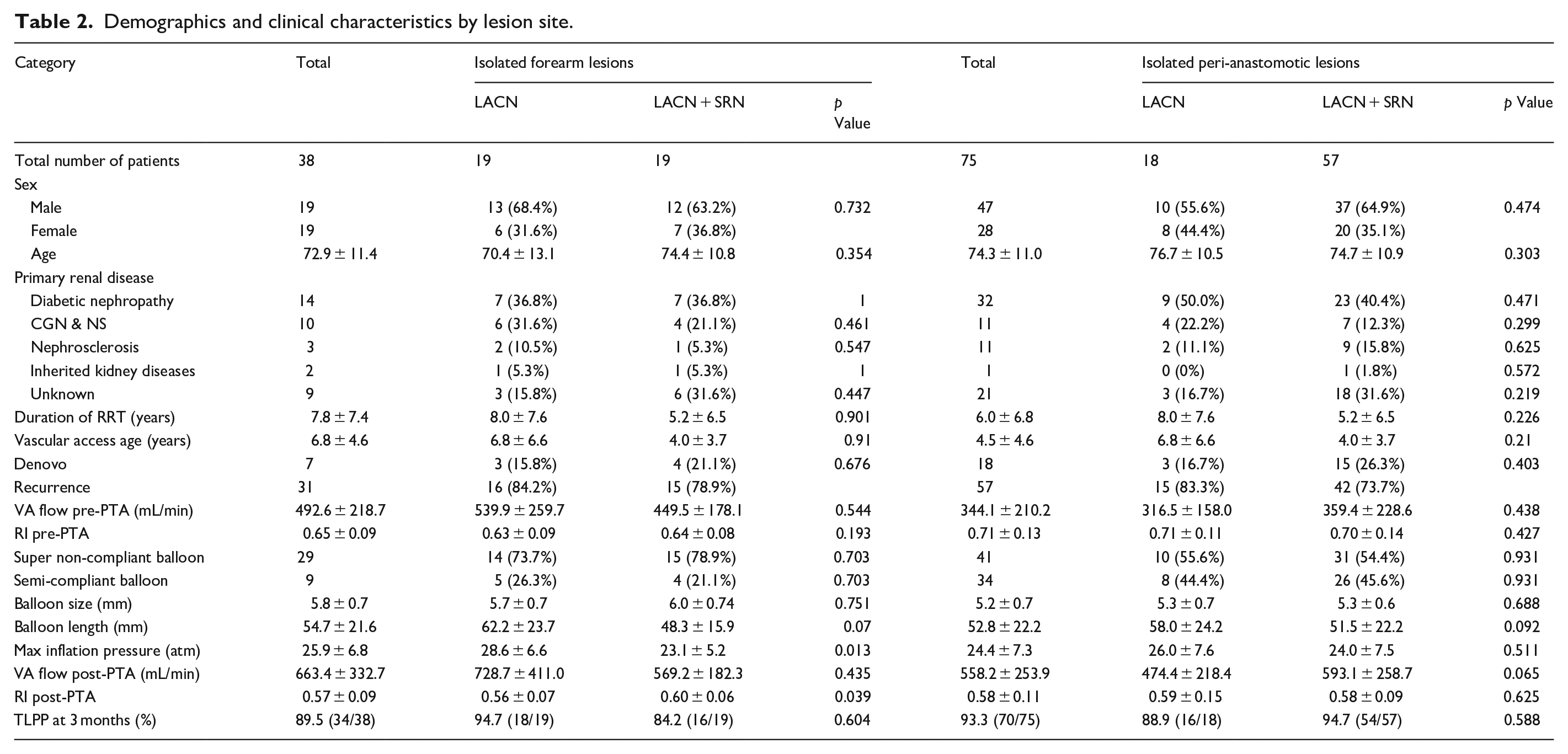
In the sessions treating isolated forearm lesions, 19 were treated with LACN block alone and 19 with both LACN and SRN blocks. The demographics and clinical characteristics of these two groups are presented in Table 2. There were no statistically significant differences between the groups in age, sex, duration of renal replacement therapy (RRT), or VA age. Regarding clinical features, the maximum inflation pressure was significantly higher in the LACN group (28.6 ± 6.6 atm) compared to the LACN + SRN group (23.1 ± 5.2 atm), and the post-PTA RI was significantly lower in the LACN group (0.56 ± 0.07) than in the LACN + SRN group (0.60 ± 0.06). However, the 3-month target lesion primary patency (TLPP) rate was 94.7% (18/19) in the LACN group and 84.2% (16/19) in the LACN + SRN group, with no statistically significant difference.
Demographics and clinical characteristics by lesion site.
The mean NRS score during balloon inflation was 2.42 ± 2.04 in the LACN group and 2.63 ± 1.92 in the LACN + SRN group, showing no statistically significant difference (Figure 4(a)).
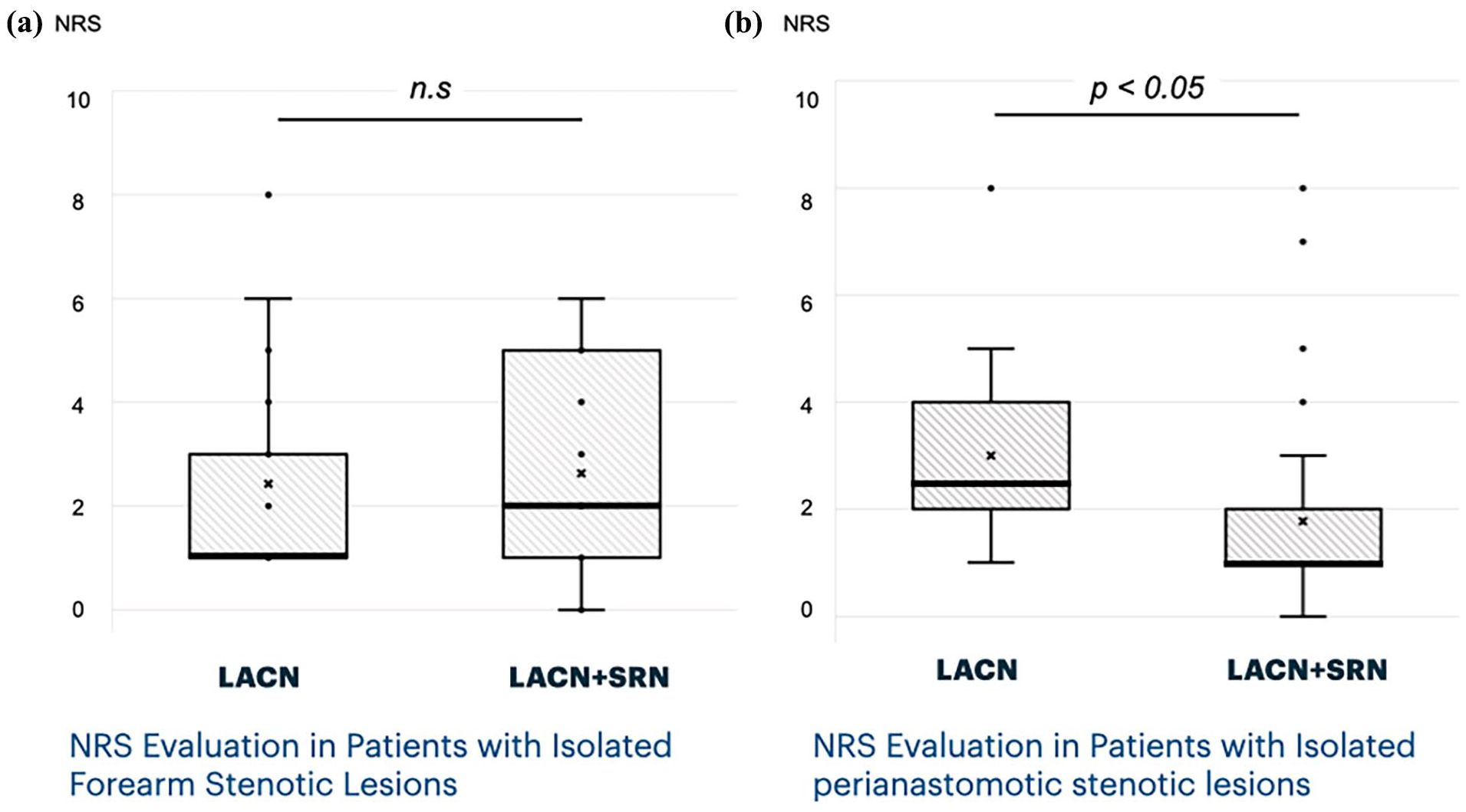
Effect of nerve blocks in forearm and anastomotic lesions: (a) the effect of SRN block is minimal in isolated forearm cephalic vein stenosis and (b) the effect of SRN block is significant in isolated peri-anastomotic stenosis.
In the sessions treating isolated perianastomotic stenotic lesions, 18 involved only an LACN block and 57 both LACN and SRN blocks out of 168 USIA + SCNB cases. The demographics and clinical characteristics of the LACN and LACN + SRN groups with isolated peri-anastomotic lesions are presented in Table 2. No statistically significant differences were observed in demographic and clinical characteristics between the LACN and LACN + SRN groups with isolated peri-anastomotic lesions. Here, the NRS for LACN-only block sessions was 3.00 ± 1.78, and significantly decreased to 1.77 ± 1.82 when an SRN block was added, indicating substantial pain reduction (Figure 4(b)).
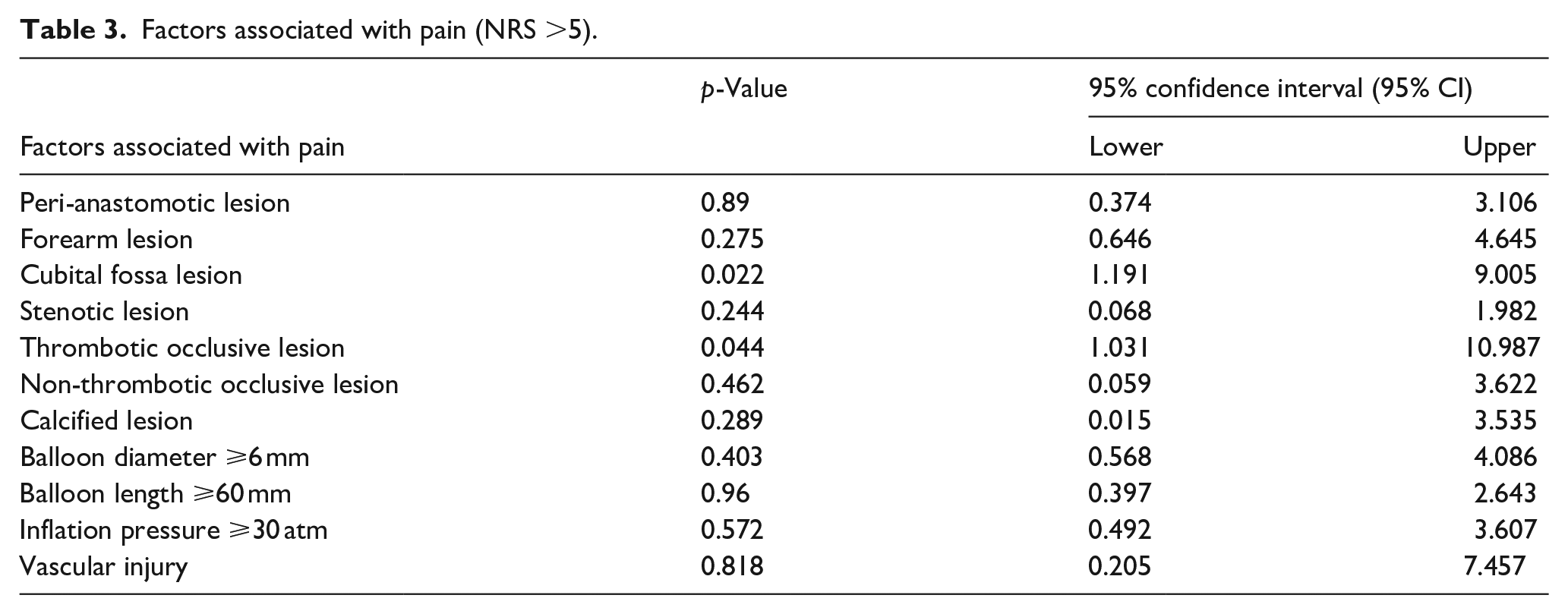
Among the 168 patients who underwent USIA + SCNB, moderate to severe pain, defined as an NRS of 5 or higher, was associated with lesions located in the antecubital area. In addition, thrombotic occlusive lesions were significantly associated with higher NRS scores. No significant correlation was observed between NRS scores of 5 or higher and other lesion characteristics, including stenotic morphology, balloon length, diameter, or inflation pressure (Table 3).
Factors associated with pain (NRS >5).
Discussion
This study demonstrated that the combination of USIA and SCNB significantly reduced procedural pain compared to IA or USIA alone. Furthermore, a notable feature of this study is that in all cases where SCNB was applied, an LACN block was performed, and its efficacy as an anesthetic technique was confirmed—achieving significant pain relief without causing motor paralysis.
Previous research has documented the pain reduction benefits of supraclavicular and axillary brachial plexus blocks during PTA for dialysis arteriovenous fistulas dysfunction.12–15 These blocks, often used in orthopedic surgeries of the upper limb distal to the shoulder, can lead to “dead arm,” a condition of complete motor paralysis, while providing substantial analgesia. This study proposes reducing the need for such potent anesthesia by selectively blocking only peripheral sensory nerves under ultrasound guidance.
Matsuda et al. highlighted the MCN for its critical role in the sensation of the anterolateral forearm. They demonstrated effective pain relief by blocking the MCN, particularly in cases of long or multiple lesions at the wrist or anatomical snuffbox, limiting motor paralysis to the upper arm flexors. 10 Our findings extend this approach, showing that blocking the LACN—a peripheral branch of the MCN without motor fibers—can effectively reduce sensation in the anterolateral forearm without inducing motor paralysis.
Traditionally, the superficial branch of the radial nerve (SRN) is described as primarily innervating the dorsolateral aspect of the hand.16,17 However, Hasenkam et al. demonstrated that ultrasound-guided blockade of the SRN from a mid-forearm approach resulted in a broader sensory distribution than classical dermatomal maps suggest, including not only the dorsolateral hand but also the radial side of the mid-forearm. 18 In our study, the addition of an SRN block significantly improved pain relief during balloon dilation for peri-anastomotic lesions. This finding may be explained by the alignment between the sensory territory described by Hasenkam et al. and the anatomical location of peri-anastomotic lesions in our study. Previous anatomical studies have reported frequent neural connections and variant sensory distributions between the SRN and LACN. In a large-scale anatomical study by Khadanovich A et al. major communicating branches between the LACN and SRN were found in 73.5% of 102 cadaveric forearms, and minor secondary connections were observed in an additional 10.8%. 19 Similarly, Davidovich ER and Nascimento OJ reported the presence of clear anastomosis in 41.2% of cases based on electrophysiological analysis. 20 In addition to discrete communicating branches, the SRN and LACN frequently exhibit overlapping sensory territories or variant innervation patterns. Davidovich and Nascimento demonstrated through nerve conduction studies that in approximately 8%–11% of 200 upper limbs, the LACN partially or entirely supplanted the SRN by innervating the radial dorsum of the hand and the thumb. 21 Therefore, it is conceivable that effective analgesia for peri-anastomotic lesions during balloon angioplasty was achieved not solely through SRN blockade, but also through the concomitant LACN block, reflecting the contribution of both nerves to the regional sensory network. The SRN block was performed via an ulnar (caudal) approach from the mid-forearm. A 25G needle was used to hydrodissect the space between the brachioradialis muscle and the radial artery, allowing access to the SRN within the flexor compartment. The injected anesthetic solution spread longitudinally within the flexor compartment adjacent to the radial artery. Although the primary neural supply to the radial artery is provided by the median nerve, 22 and the direct effect of the SRN block itself may be limited, it is conceivable that the infiltration anesthesia around the radial artery contributed to pain relief during procedures involving peri-anastomotic lesions.
In the wrist region near the anastomosis, in addition to the LACN and SRN, the posterior antebrachial cutaneous nerve (PACN), as reported by Finneran and Sandhu, may also contribute to the sensory innervation. 23 In the present study, PACN blockade was not performed, and it is possible that USIA provided supplementary analgesia in its place. However, due to variability in the effectiveness of USIA among cases, this remains a potential limitation of the study.
In Japan, where 95% of dialysis patients have forearm arteriovenous fistulas, there is a substantial requirement to suppress sensation in the anterolateral forearm. 24 Vascular interventions for dialysis shunts are typically performed outpatient, not necessitating hospital stays. By administering a small amount of short-acting lidocaine around the nerve under ultrasound guidance, both the onset and cessation of its effects are expedited, thus facilitating outpatient-oriented nerve blocks.
Identifiable factors linked with moderate to severe pain included lesions in the antecubital area, where the LACN becomes superficial, and thrombotic occlusive lesions (Table 3). Pain in this region, particularly in the proximal area near the median basilic vein, is likely attributable to the sensory innervation of the medial antecubital fossa by the medial antebrachial cutaneous nerve, which was not targeted in this study. Thrombotic occlusive lesions often induce localized inflammatory phlebitis, accompanied by erythema and tenderness, 25 and the thrombectomy procedure for AVFs is generally recommended to be performed under sedation using agents such as fentanyl and midazolam. 26 These findings suggest that such lesions are associated with a level of pain that requires deep sedation for adequate control. While the location of the lesion and the presence of thrombotic occlusion prominently influenced pain intensity, other factors such as calcification, balloon diameter, length, inflation pressure, and vascular damage had minimal impact. Based on these findings, although clinical characteristics observed in the analysis of isolated forearm lesions showed that the maximum inflation pressure was significantly higher in the LACN group and the post-PTA RI was significantly lower in the LACN group, the influence of these variables on pain was considered to be limited.
Limitations
This study has several limitations. First, it was a retrospective analysis conducted during the early phase of SCNB implementation, and SCNB was introduced as an additional intervention alongside conventional IA and USIA. Due to ethical considerations, it was not feasible to evaluate the analgesic efficacy of SCNB alone without concurrent IA or USIA; thus, SCNB was always performed in combination with USIA. Therefore, this study does not directly demonstrate the independent effectiveness of SCNB. Second, since the decision to perform SCNB was based on operator discretion and the patient’s prior experience of severe pain during previous PTA sessions, the possibility of selection bias due to the non-randomized design cannot be excluded. Third, all nerve block procedures were performed during the initial phase of the learning curve in our department, and variability in technical proficiency may have influenced the consistency and effectiveness of the nerve blocks. Fourth, pain intensity was assessed using patient-reported NRS scores, which may have been influenced by subjective factors such as operator presence and treatment expectations, introducing the potential for observer bias. Lastly, anatomical variations in the course and sensory distribution of the LACN and SRN may have contributed to inconsistencies in block effectiveness across patients and represent an inherent limitation in the generalizability of the findings.
Conclusion
SCNB based on the sensory distribution corresponding to the lesion and dilation sites is effective for pain management during PTA in RC-AVFs. This study demonstrated that an LACN block is useful for cephalic vein stenosis in the forearm, and that adding an SRN block contributes to pain relief in cases involving peri-anastomotic lesions. Ultrasound-guided selective cutaneous nerve block combined with ultrasound-guided infiltration anesthesia, effectively reduces pain during PTA of RC-AVFs, and the two methods have a synergistic effect.
Footnotes
Acknowledgements
We extend our gratitude to the staff of the Blood Purification Center and the Department of Radiology at Saitama Medical University General Medical Center, who were involved in the treatment. We also thank Takayanagi Kaori for her assistance with the statistical analysis of this paper.
Author contributions
Conceptualization: Taisuke Shimizu. Data Curation: Tatsuro Sano, Toru Hida, Akihiko Seo, Nozomi Abe, Takayuki Tohara. Investigation: Kouki Ogawa, Takayuki Hamada, Maki Okamoto. Methodology: Taisuke Shimizu. Supervision: Shunsuke Takahashi, Tomonari Ogawa, Akito Maeshima, Hajime Hasegawa. Writing—original draft: Taisuke Shimizu. Writing—review & editing: Tomonari Ogawa.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Animal studies: no animal studies were carried out by the authors for this article. The study was conducted with the approval of the Institutional Ethics Committee (approval number: 2024-113).
Informed consent
Opt-out. This study aims to contribute to public health improvement. Considering the time constraints and costs associated with obtaining informed consent, the potential disruption to the study’s execution by seeking individual consent is deemed significant. Therefore, information about this study will be made publicly available, providing participants with the opportunity to opt out. If any participant declines to participate, they will not be included in the study, except in cases where the results have already been published. A public disclosure document in the common format of the university will be posted on the Research Ethics Committee website of the Comprehensive Medical Center, ensuring that participants can easily access the information.