
Abstract
Background:
Catheterization of the vein is frequently a painful procedure. Assessing venous cannulation induced pain (VCP) before surgery have been used to predict the intensity of postoperative pain and postoperative opioid consumption. The aim of this study was to investigate the intra-individual variation in venous cannulation induced pain at three consecutive time points and factors influencing levels of reported pain.
Methods:
Participants (n = 101) were included at the blood-donor-center of a regional hospital in Sweden. All completed the Hospital Anxiety and Depression Scale and Pain Catastrophizing Scale and reported previous pain condition or ongoing use of analgesics upon inclusion. During three consecutive visits, venous cannulation was performed in a standardized manner, during which pain intensity was reported using the Visual Analogue Scale (VAS).
Results:
The intra-individual variation in VCP, measured using the mean coefficient of variation, was 1.2. This means that the mean intra-individual difference in pain upon VCP between the three time points was 20%. A tendency toward higher intra-individual variation with higher pain intensities was found. Mean intra-individual range in VCP was 1.9 (SD 1.8) VAS-units. No correlation was found between anxiety- or depression nor pain catastrophizing and pain associated with venous cannulation. Subjects with preexisting pain conditions did not experience more pain in this situation.
Conclusions:
Venous cannulation pain intensities show low intra-individual variations. Subjects with higher pain intensity during venous cannulation are prone to greater intra-individual variations. If low pain perceived this is likely to repeat. To our knowledge this has never been investigated before and has implications for using pain evaluations as proxy for sensitivity measurements but also for how we handle patients with previous pain on venous cannulation.
Keywords
Introduction
Obtaining vascular access can be a painful event. Successful venous cannulation is associated with pain intensities corresponding to 1.0–5.0 Visual Analogue Scale (VAS)- or Numeric Rating Scale (NRS)-units.1–5 Previous work has shown that venous cannulation pain (VCP), measured with the VAS, is influenced by an array of different variables. Multiple attempts have been shown to induce more pain, 2 larger cannula means more discomfort 5 and the antecubital fossa is associated with less pain compared to the back of the hand. 6 One can of-course use local anesthesia to lower the pain experienced, especially when using larger cannulas, like lidocaine or vapocoolant spray, although in clinical practice many times deprioritized.5,7 Various types of distractions have been shown to lower the levels of pain perceived during venous cannulation, such as an unannounced flash of light or simply talking about mundane events during the procedure.8,9 Operator gender and the assumed operator experience when performing a supposedly painful procedure also affect perceived procedure related pain as lower pain levels have been found when pain is evaluated by a woman.10,11
Since most in-patient procedures require venous access, inquiring about pain sensitivity and taking measures to minimize any unnecessary discomfort could be advantageous. The individual perception of pain in general varies and has been shown to depend on gender,12–14 age, 15 previous social experiences, 16 socioeconomical state, 17 and psychometric factors such as anxiety and pain catastrophizing.18,19 Experimentally and for study-purposes, pain can be induced in standardized ways using different techniques such as temperature,1,20 electricity, 14 and pressure 21 in an effort to measure pain perception and sensitivity. There is a significant number of studies indicating that pain thresholds and tolerance assessed using the above techniques can be correlated with post-operative pain and postoperative opioid consumption enabling a more individualized care.4,21–23 VCP levels, as it induces pain on individual levels, has also been linked to levels of postoperative pain and opioid consumption.4,24,25 If the perceived pain intensity during venous cannulation is related to individual pain sensitivity this would have implications for patients coming back for repeated cannulations but also when using VCP as a prediction method in the surgical setting.
What has yet to be studied, is the level of intra-individual variability concerning the pain perceived during venous cannulation. Few studies concern the subject of intra-individual variations in pain perception. Does venous cannulation, as a source of pain, produce the same levels of pain for the same individual on different occasions? The aim of this study was to assess if the individual self-reported pain intensity upon venous cannulation vary from one time to another if the trigger of pain is similar.
Primary outcome was the intra-individual variation in VCP reported during three consecutive and independent time points. We hypothesize that the VCP for the three visits will vary less than 20% within each individual. Secondary aim was to investigate the influence of anxiety, depression, or pain catastrophizing at baseline on the pain perceived.
Methods
Study design
We carried out a prospective observational cohort study at the blood-donor-center at Hallands Hospital in Halmstad, Sweden. Volunteers received written and oral information and were consecutively included by the nursing staff when informed and written consent was obtained. Each participant was given a unique inclusion number to ensure patient confidentiality and blinding of results. These blood-donors were all attending the blood-center on a regular basis; women three times yearly and men four times yearly. Each participant was included for pain-assessment during three consecutive visits. Nursing-staff at the blood-center were responsible for filing data-forms and one of the authors collected and digitalized the study-forms on a regular basis. The patients were given an inclusion number to link the different measurements but no code was kept and therefor the data was anonymized. Inclusion criteria were ability to understand Swedish and the written information given and age 18–80. Exclusion criteria was less than three visits to blood-center during 1 year.
The regional Ethical Review Board at Lund University, Lund, Sweden, approved the study on October 11th 2016 (Dnr: 2016/671). No interventions or harmful procedures were added to the care or treatment of participants. No compensation, financial, or otherwise, was given to participants. The study protocol complies to the declaration of Helsinki and reporting is done in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Outcome
Primary outcome was the intra-individual variation in VCP reported during three consecutive and independent time points.
Hypothesis: Measuring VCP at three different time points, the VAS score will vary less than 20% for each individual.
Secondary outcome was possible associations between anxiety, depression, pain catastrophizing, gender, and previous pain condition and VCP.
Psychometric evaluation and pain history
Participants completed the Hospital Anxiety and Depression Scale (HADS) and the Pain Catastrophizing Scale (PCS) upon inclusion only. The HADS is a 14-item scale designed to evaluate self-reported anxiety and depression in somatic healthcare. 26 The HADS has been used in research on pain prediction, 27 and has been translated and validated into Swedish. 26 The PCS is a questionnaire showing promising results regarding predictability of acute postoperative pain. 28 It comprises 13 questions measuring the negative orientation around the thought of having pain and has been frequently used in pain research. 29 PCS scores have been found to have weak association with VCP. 19
Information regarding previous pain history, chronic pain, and ongoing treatment with analgesics was collected during the first visit.
Venous cannulation and pain measurements
Once included, participating blood-donors were asked to report VCP on a horizontal VAS ruler immediately after the procedure. Data on VCP were collected on three consecutive visits, generating three data point measures per participant. To minimize influence of previous results, individual VCP were not presented to the participant. Each VCP-score was registered separately from each cannulation time point, so that the participant and investigator would be blinded to previous results. All were cannulated with the same size needle (1.5 mm) at the same location (anterior cubic fossae). The disinfectant used was chlorhexidine cutanic solution (Fresenius Kabi®) 5 mg/mL, applied and then left for a few seconds to dry. Nursing staff with at least 3 years working experience at the blood center carried out all the venous cannulations.
Statistics
Sample size was based on an expected deviation of 20% on the VAS scale (unpublished pilot study). For a hypothetical expected difference of approximately 10%, (beta error = 0.20; Power = 0.80) and a level of significance at 0.05, this would require at least a sample size of the 86 participants. To ensure that these participants were included during 1 year we opted to include 160 individuals.
We consider VAS to be an ordinal scale since for example VAS 4.0 does not necessarily mean twice as much pain as VAS 2.0 and clinically significant changes in pain intensity are different along the length of the VAS-scale. 30 Subsequently, results are reported as median with interquartile range (IQR) on group level. The VCP-levels (3 visits) are calculated as mean levels within each individual. The Mann-Whitney U-test was used to compare gender differences regarding age, VCP, HADS- and PCS-scores. To test the correlation of HADS- and PCS-scores with pain intensity, a Spearman’s correlation test was used. Friedmans test was used to investigate the effect of time on the median VCP-levels. Bland-Altman plots were set up to describe the pain variability within subjects. Levels of probability (p) below 0.05 were considered to indicate statistical significance.
Results
Participants were prospectively included in the study from 12th December 2016 to 25th January 2017 and were then followed during repeated visits until December 2017. During this time 837 blood donors visited the lab and at times when the logistical demands allowed 170 of these donors were asked to participate. There was no participation refusal in this cohort. Of 170 initial inclusions, 101 completed three consecutive VAS-measurements during three visits and of these, 69 were excluded due to not returning for three visits within the pre-defined time frame (Figure 1). Population characteristics can be seen in Table 1.
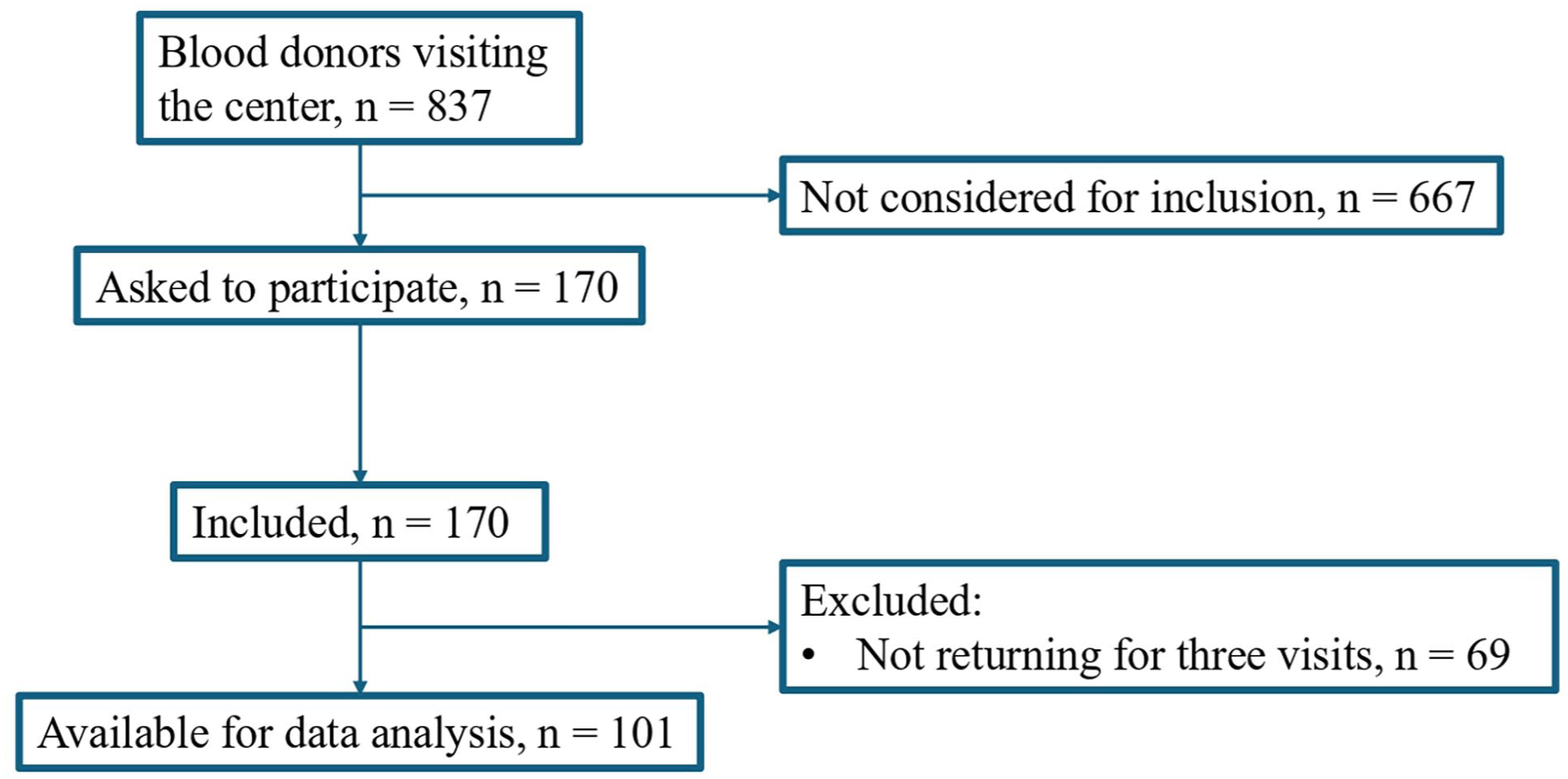
Inclusion flowchart.
Participants characteristics for the cohort and for men and women respectively.
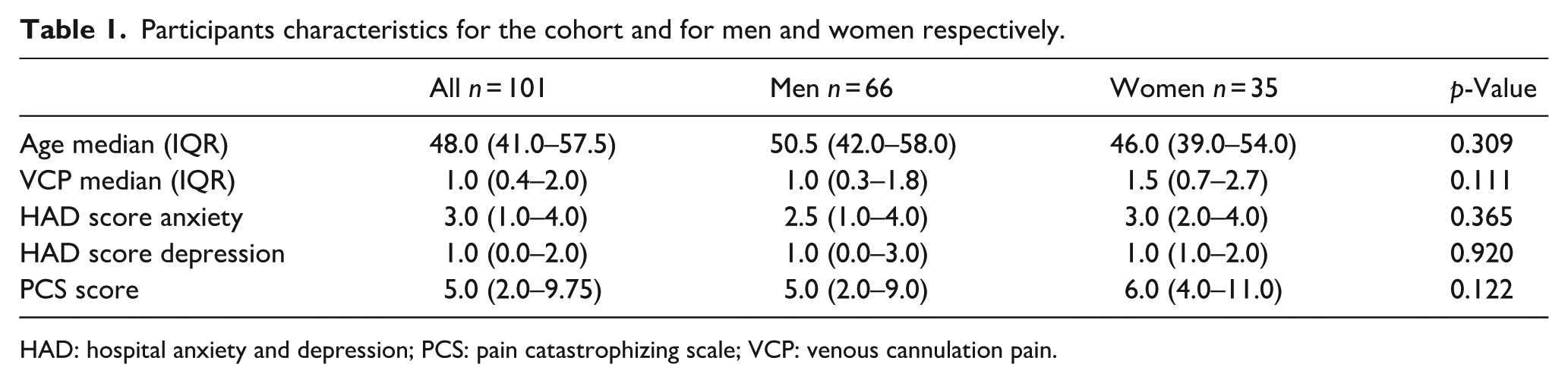
HAD: hospital anxiety and depression; PCS: pain catastrophizing scale; VCP: venous cannulation pain.
Primary outcome: Repeated pain measurements
The mean coefficient of variation was 1.2 (intra-individual variation) meaning that the mean difference in VAS between the three different visits was 20% (Figures 2–4). Individual levels of pain (VAS) are shown in Figure 1 (Figure 2). The mean range (difference between lowest and highest VAS in each subject) was 1.9 (SD 1.8) VAS units. A positive relationship was seen between the individual standard deviation and VCP (rs = 0.864, p < 0.001) meaning that donors rating higher VAS upon venous cannulation had higher variation in pain intensity at the three visits. Donors experiencing low pain also showed low variations at the three visits (Figure 2). There was no statistical difference in median VCP at the different time points on group level (Table 2).
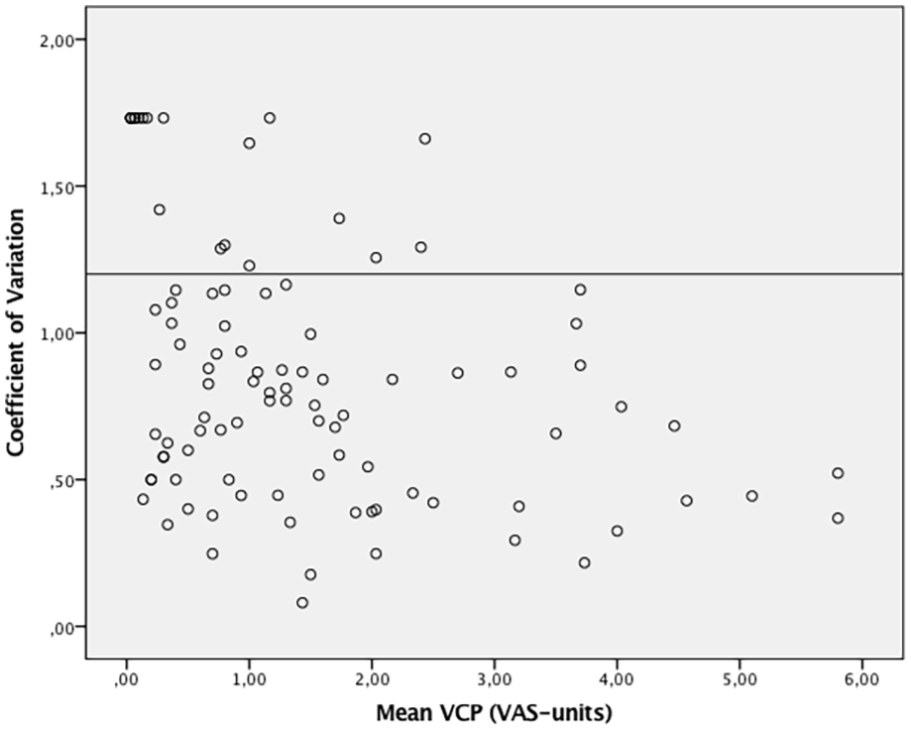
Bland Altman Plot describing the intra-individual variations in pain by coefficient of variance against mean venous cannulation pain. The horizontal line describes the pre-defined cut-off value of 20% intraindividual variance.
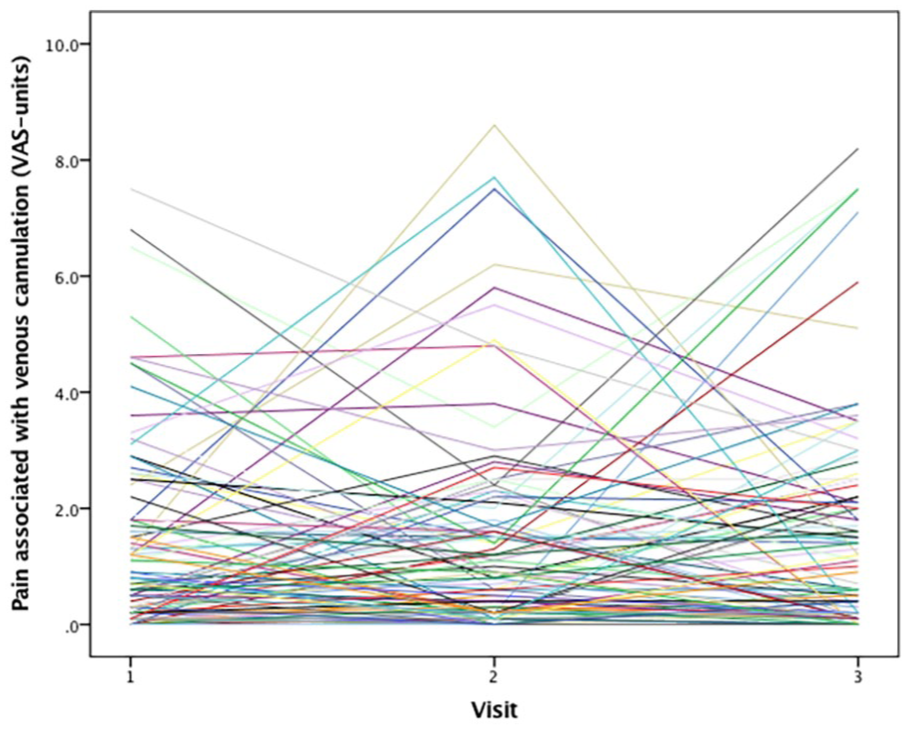
Spaghetti-plot illustrating the distribution of pain scores within participants over the three consecutive cannulations. Each line represent one individual.
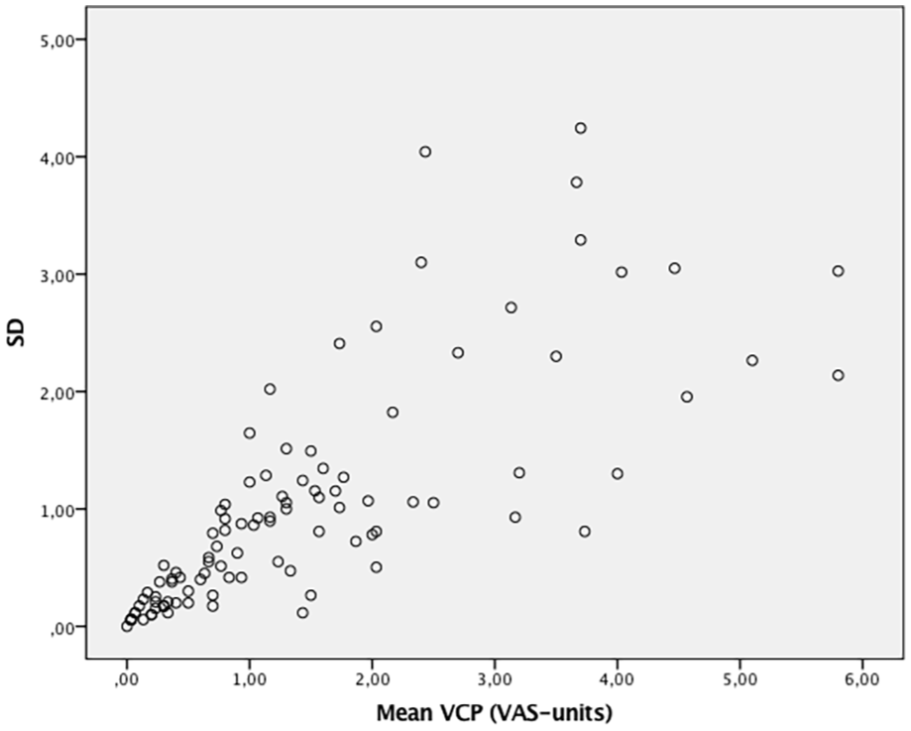
Bland Altman Plot describing the intraindividual variations in pain by plotting standard deviation against mean venous cannulation pain.
There was no overall effect of time on the median pain associated with venous cannulation.

Secondary outcomes: Factors influencing VCP
There was a positive correlation between PCS and HADS for anxiety (rs = 0.28, p = 0.004) as well as HADS for depression (rs = 0.46, p < 0.001). There was no correlation between HADS and VCP nor the PCS and VCP. No gender difference was found in VCP, PCS, or HADS.
No significant differences in median VCP were found between participants with (VCP 1.0, IQR 0.3–1.9) or without (VCP 1.6, IQR 0.8–3.9) previous pain condition (p = 0.081).
Discussion
This study shows that intra-individual variation in pain (measured using VAS) on venous cannulation is small at low pain levels. A tendency toward greater intra-individual variations was seen at greater pain levels. Intra-individual variations were tested using venous cannulation under standardized conditions, separated by a fair amount of time. To compare intra-individual variations within our group we used the coefficient of variation (CV) for each individual. The CV is a useful measurement because it illustrates variation regardless of absolute values. The mean CV for the group of 1.2, that is the variation in pain was 20% at consecutive visits, means that the absolute variations in pain levels are higher at higher VAS-levels. Further validating this, when comparing each participant’s standard deviation from the three visits, with the participants reported mean VCP, we saw a tendency toward greater intra-individual variations for participants who reported higher VAS-scores. Even though the levels vary greatly if on the higher end of the scale the clinical implication would be that if you have experienced a cannulation painful the risk of the next procedure to also be painful is higher. The importance of this finding is that VCP as a method for pain sensitivity is reliable over time. A patient who do not find venous cannulation painful is less likely to find it painful the next time and thus the implication of using anesthesia for this procedure is lower. As doctors tend to find anesthesia redundant 7 they should perhaps focus first on patients who tend to find the procedure painful upon previous exposure. This could also be of importance when applying this method in the clinical surgical setting as a prediction method. We thus believe this finding validates the method of using VCP as a repeatable measurement of pain sensitivity.
We need to consider multiple factors that might influence VCP, such as size of needle, 5 number of attempts, 2 cannulation site, 6 and operator experience. 10 To minimize the impact of these factors we chose to recruit participants from the blood-center, where these circumstances are all pre-determined and the routine surrounding the cannulation is very similar.
There are some limitations to consider when reading this article. The benefits of using blood-donors are apparent (ease of inclusion, homogenic population, and already planned for venous cannulation regularly) but there are also limitations. One can argue that the selection of participants limits the external validity of our study. Blood-donors are a healthy group being exposed to a stimulus that is well known to them, in a comfortable environment without stressing factors as indicated by the low pain levels in this study compared to other studies.5,7 Also, we did only evaluate anxiety, depression, pain catastrophizing, and preoperative pain once, before the first visit. It is possible that this fact changed over the year of returning visits for some patients. This could possibly have influenced the results regarding these factors and association with VCP. However, the importance for VCP-levels per se seems low since there was no difference in median levels between the three visits.
In conclusion we found the variation in VAS-scores to be 20% during repeated cannulations. There is a tendency toward greater intra-individual variation in pain if participants find the procedure more painful. Pain associated with venous cannulation does not seem to be associated with depression, anxiety, pain catastrophizing, or gender. To our knowledge this has never been investigated before and has implications for using pain evaluations as proxy for sensitivity measurements but also for how we handle patients with previous painful experiences during venous cannulation. In the future it would be interesting to individualize anesthesia during venous cannulation focusing on the patients with higher sensitivity.
Footnotes
Acknowledgements
We would like to thank the administration at the blood-donor-central at Hallands Hospital Halmstad for helping with data collection. For help with statistical analyses we would like to thank the department for research and development at Hallands Hospital Halmstad.
Author contributions
Conceptualization: MJ/AP. Methodology: AP/KM. Formal analysis: MJ/AP/KM. Investigation: MJ/AP. Writing: MJ/AP. Reviewing and Editing: MJ/KM/AP.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Financial support from Region Halland was provided for the research, authorship, and/or publication of this article.
Data availability statement
Anonymized data will be shared upon reasonable request to the author.
Ethical approval
The regional Ethical Review Board at Lund University, Lund, Sweden, approved the study on October 11th 2016 (Dnr: 2016/671). All participants provided written and oral informed consent prior to enrollment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Informed consent
All participants provided written and oral informed consent prior to enrollment in the study.