
Abstract
Background:
Midline catheters have been considered a preferred alternative to peripheral intravenous catheters and central venous catheters. However, little is known about the safety of infusing irritants through midline catheters. We aimed to evaluate safety outcomes after the administration of irritants through midline catheters.
Methods:
This was a retrospective observational cohort study that included 1613 patients who had a midline catheter from April 2020 to December 2023. We used descriptive statistics and inferential statistics to characterize and compare the groups and conducted multivariable regression analysis adjusted for potential confounders. Subgroup analyses (with tests for interaction) were used. A 1:1 propensity score matching analysis was performed to repeat the analysis that achieved stringent control for confounders. Sensitivity analysis was conducted to test the stability of the results.
Results:
1184 patients received irritants through midline catheters and 429 patients did not receive irritants. There were no significant differences in catheter-related complications between the groups (before matching: 9.9% vs 6.8%, p = 0.062; after matching: 9.9% vs 6.6%, p = 0.105). The multivariate analysis revealed that the platelet count, the catheter duration, and the vein selection were significant independent risk factors associated with catheter-related complications. Subgroup analyses indicated that there were no significant interactions. The results of the sensitivity analysis were robust.
Conclusions:
We found no significant association between the administration of irritants through midline catheters and catheter-related complications. However, the drug indications for midline catheters need to be further confirmed by well-conducted randomized clinical trials with large cohorts of patients.
Introduction
Intravenous access is essential for the management of any inpatients. 1 According to the report, an estimated 150 million peripheral intravenous catheters and 5 million central venous catheters are placed annually. 2 It is essential to choose a vascular access device that prioritizes blood vessel health and preservation.3,4
The NAVIGATE (NomenclAture Via Integrated Global Advancements in Terminology Efficiencies) consensus defines that a midline catheter (MC) is longer than 15 cm and inserted into deep veins of the upper arm, and the catheter tip is located in the axillary vein or subclavian vein. 5 Because the tip of the MC is located in a vein with a larger diameter, it has a faster blood flow rate and better drug dilution capacity; the success rate of catheter insertion is higher, and the indwelling time is longer, which compensates for the deficiency of short peripheral intravenous catheters.6–8
However, there are discrepancies in the medication indications for MC (>15 cm) usage among various medical institutions and professional organizations. Irritant is defined as an agent capable of producing discomfort (e.g. burning or stinging) or pain as a result of irritation in the internal lumen of the vein with or without immediate external signs of vein inflammation. 9 There are consensuses recommend that known irritants should be infused through central vascular access devices rather than MCs.10,11 However, the level of evidence for the consensus is not strong (rating of IV), the sample sizes of the involved studies are limited, 9 and whether such practice is prevalent or harmful remains unknown. Based on the previous findings and our multi-center randomized controlled study on the ideal tip position of the MC, 12 we aimed to retrospectively collect real-word clinical data to evaluate the association of irritant administration through MCs (>15 cm) with tips that were located in the subclavian vein or axillary vein of the chest wall with catheter complications and to identify the factors that influence complications.
Methods
Study design and setting
This study was conducted at a comprehensive university hospital, with 129 nursing units and over 6500 beds, located in China. The hospital information system was used for the study. Our study was approved by the Institutional Review Board of the hospital and registered at ClinicalTrials.gov (NCT05710835). This study adhered to the Strengthening Reporting of Observational Studies in Epidemiology reporting guidelines. 13
Participants
For this study, we included adult (aged 18+ years) inpatients who underwent the same single-lumen, valved MC (25 cm, 4 French, Specath®) placement through the upper arm with tip positioned at the subclavian vein or axillary vein of the chest wall and did not receive other venous catheters while using the MC and who signed informed consent forms from April 2020 to December 2023. Patients were excluded if they were admitted to a non-medicine service, or if they regularly used anticoagulant medications, or if the drugs infused through the MC included chemotherapeutic agents or could not be identified as irritants.
Catheter placement and evaluation of tip position
MC were inserted according to manufacturers’ directions for use. The methods of catheter insertion included: preprocedural ultrasound assessment; appropriate skin antiseptic using 2% chlorhexidine and maximum sterile barrier protection; choice of appropriate vein, adoption of the Zone Insertion Method™; ultrasound-guided puncture; ultrasound-guided tip navigation; correct securement of the catheter, and appropriate protection of the exit site. An intravenous therapy specialist nurse confirmed catheter tip positioning by ultrasound during catheterization, and the position of the catheter tip was adjusted according to ultrasound imaging. X-ray imaging was performed after catheterization to confirm the position of the catheter tip.
Data collection
The study data were obtained through various types of electronic health records (EHRs) of the participants and recorded on structured templates. Demographic information, including the age, sex, body mass index, alcoholic consumption history, and smoking history. Disease-related information, including the diagnosis, history of malignant tumors, history of thrombosis, hypertension, and diabetes, was collected. The white blood cell count, and platelet count were recorded according to the last result before catheterization. The line-specific information included the choice of vein, the number of puncture needles, the duration of MC, and the catheter-related complications. Drug information, including the drug name, drug dose, infusion mode, infusion frequency, and infusion days, was collected. We standardized the collected data, such as drug names and diagnoses.
Variables
In our study, drugs with high osmolarity (>600 mOsm/L) or low (<5) or high (>9) pH, and other solutions with potential irritant effects on the vein wall were classified as irritants according to the scope of drug application via MCs in the guidelines. 10 We judged drugs on the basis of drug instructions, pharmacopoeia information, guidelines, etc.14 –16
The primary outcomes included phlebitis, catheter-related thrombosis, catheter occlusion, infiltration, and extravasation. The judgment criteria for each complication were as follows: (1) phlebitis: inflammation of a vein; may be accompanied by pain/tenderness, erythema, edema, purulence, and/ or palpable venous cord; rated by a phlebitis scale (see Table S1) 9 ; (2) catheter-associated thrombosis: the formation of 1 or more symptomatic (i.e. pain or swelling) blood clots in a vein verified by ultrasonography or a computed tomography scan 17 ; (3) catheter occlusion: obstruction of a vascular access device lumen, preventing or limiting the ability to flush and/or administer solutions through a lumen or withdraw blood 9 ; (4) infiltration: inadvertent administration of a nonvesicant solution or a medication into surrounding tissue; rated by an infiltration scale (see Table S2) 9 ; (5) extravasation: inadvertent infiltration of vesicant solution or medication into surrounding tissue; rated by a standard tool or definition (see Table S3). 9
Secondary outcomes were catheter dislodgement, bleeding, catheter-related bloodstream infection, and exudate. The judgment criteria for each complication were as follows: (1) catheter dislodgement included dislodgement of more than 3 cm 18 ; (2) bleeding: the blood exudation at the puncture site 48 h after catheterization 19 ; (3) catheter-related bloodstream infection: It is diagnosed if the same organism is isolated from a blood culture and the tip culture and the quantity of the organisms isolated from the tip is greater than 15 colony forming units. Alternatively, differential time to positivity requires the same organism to be isolated from a peripheral vein and a catheter lumen blood culture, with growth detected 2 h earlier (i.e. a 2-h shorter incubation time) in the sample drawn from the catheter 9 ; (4) exudate was noted when the puncture site had liquid exudation.
Statistical analysis
Categorical variables were presented as frequencies with percentages (%), and continuous variables were presented as the means with standard deviations or medians with interquartile ranges. The differences between the groups were compared with t-tests or Mann-Whitney U test for continuous variables and Fisher-exact test or Pearson’s chi-squared test for categorical variables. Multivariable logistic regression was used to examine the association between exposure groups and catheter-related complications, adjusting for potential confounders. All confounders, including the age, body mass index, smoking status, diabetes status, hypertension status, alcohol consumption status, cancer history, thrombus history, white blood cell count, platelet count, number of puncture needles, vein, catheter duration, and catheterization history, were selected a priori on the basis of biological plausibility.
Subgroup analyses
Subgroup analyses were conducted according to age (<65 or ⩾65 years), body mass index (<18.5, 18.5–24, or >24 kg/m2), hypertension (no/yes), diabetes (no/yes), vein (basilic, brachial, or cephalic), duration (⩽6 or >6 days), and catheterization history (0 or >0). The possibility of effect modification of the exposure-outcome association was assessed by introducing interactive terms to the regression model.
Propensity score matching
In order to achieve stringent control for confounders, planned primary analyses also included examining the associations between the exposure groups and catheter-related complications via propensity score matching. Propensity score matching was performed using a 1:1 matching ratio and sampling without replacement with a caliper of 0.02. Descriptive statistics and inferential statistics were conducted to characterize and compare the two groups.
Sensitivity analyses
A sensitivity analysis was performed in orthopedic patients that with the same type of disease using a multivariable logistic regression model that adjusted for all covariates was used to evaluate the robustness of the findings.
All analyses were performed with a two-tailed text, and a p value <0.05 was considered statistically significant. Statistical analyses were carried out using the SPSS software (Version 26.0) and R software (Version 4.3.3).
Results
General characteristics
Figure 1 showed a flowchart of the study cohort. A total of 1670 patients in hospitals between 1st April 2020 and 31st December 2023 were enrolled. After excluding 57 patients who met the exclusion criteria, a total of 1613 patients were included in the final analysis. There were 1184 (73.4%) patients who received irritants via MCs and 429 (26.6%) patients who did not receive irritants during the specified time period. The patients who did not receive irritants through MCs were significantly older (median 65.0 [IQR 51.0–75.0] vs 61.00 [40.0–72.0] years, p < 0.001). There were more diabetic patients who received irritants via MCs (274 [23.1%] vs 132 [30.8%], p < 0.002). Compared with patients who did not receive irritants through MCs, patients who received irritants through MCs had higher white blood cell counts (median 7.6 [IQR 5.6–9.7] vs 7.00 [5.10–9.60] × 109/L, p = 0.036) and longer catheter duration (median 10.0 [IQR 6.0–16.0] vs 6.00 [4.0–11.0] days, p < 0.001). The baseline characteristics are shown in Table 1. In the included patients, we identified a total of 24 infused irritants, including 8 anti-infective drugs, 2 digestive-related drugs, 6 vasoactive drugs, 3 sedatives and analgesics, and 5 other drugs. The list of irritants used is shown in Table S4.
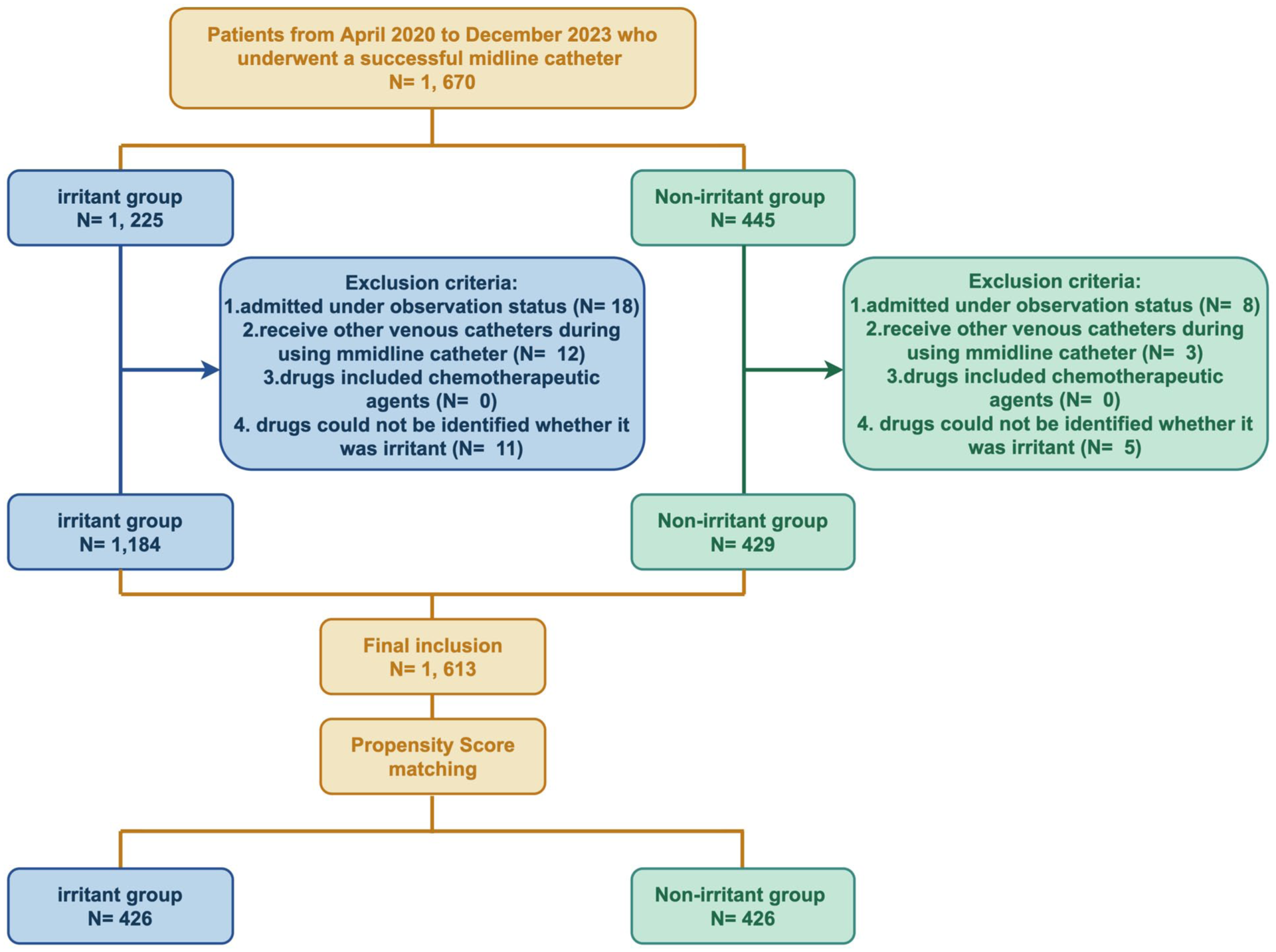
Flowchart of the study population.
Baseline characteristics of study population.
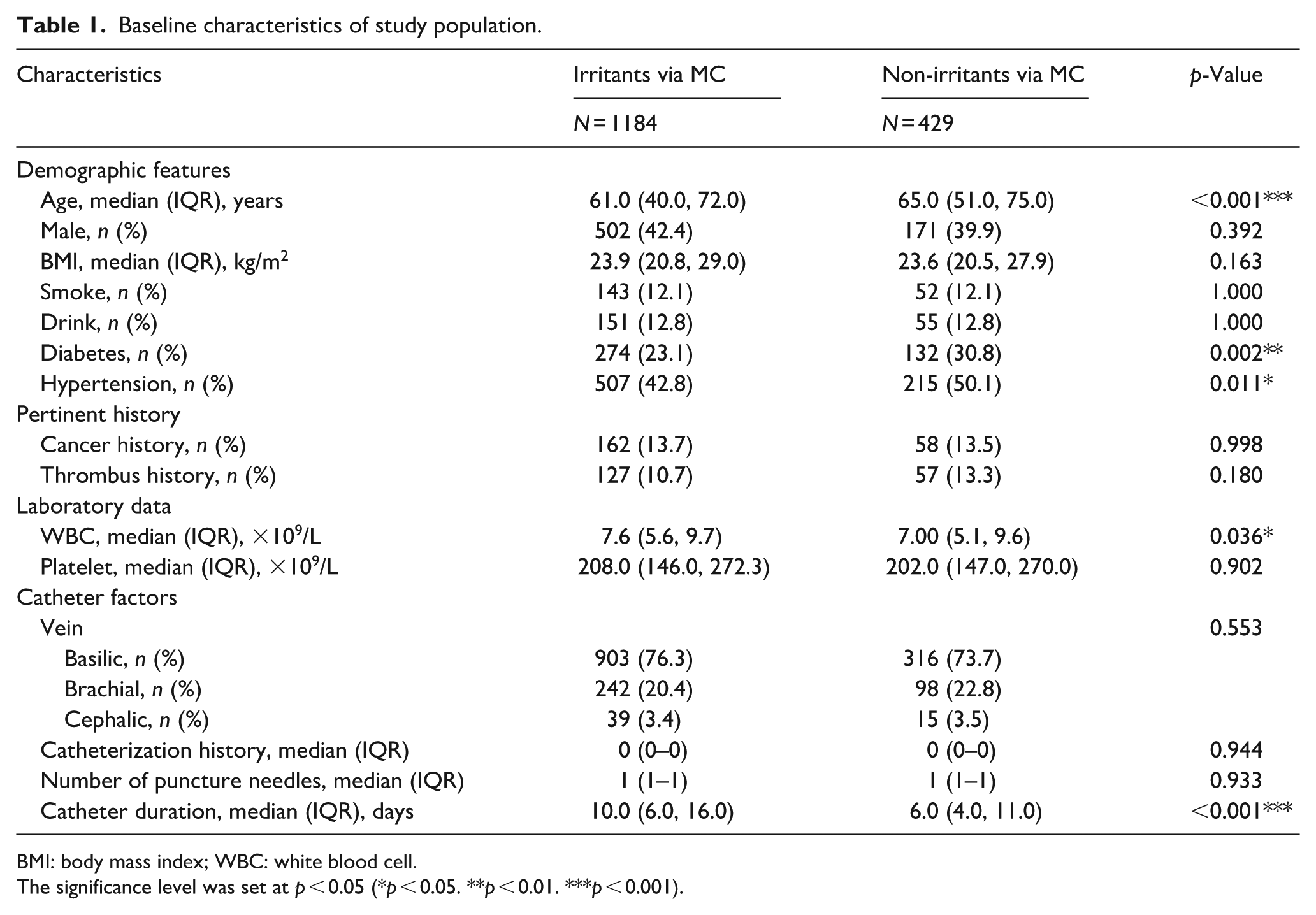
BMI: body mass index; WBC: white blood cell.
The significance level was set at p < 0.05 (*p < 0.05. **p < 0.01. ***p < 0.001).
Comparison of the catheter-related complications
A total of 117 (9.9%) patients who received irritants through MCs and 29 (6.8%) patients who did not receive irritants developed catheter-related complications during the catheter indwelling period (p > 0.05). None of the 1613 patients included in the two groups had complications including phlebitis, catheter-related infection, infiltration, and extravasation. There were no significant differences in the incidences of exudate, bleeding, catheter dislodgement, catheter occlusion, or catheter-related thrombosis between the two groups (p > 0.05; Table 2).
Comparison of the incidence of catheter-related complications between the two groups.
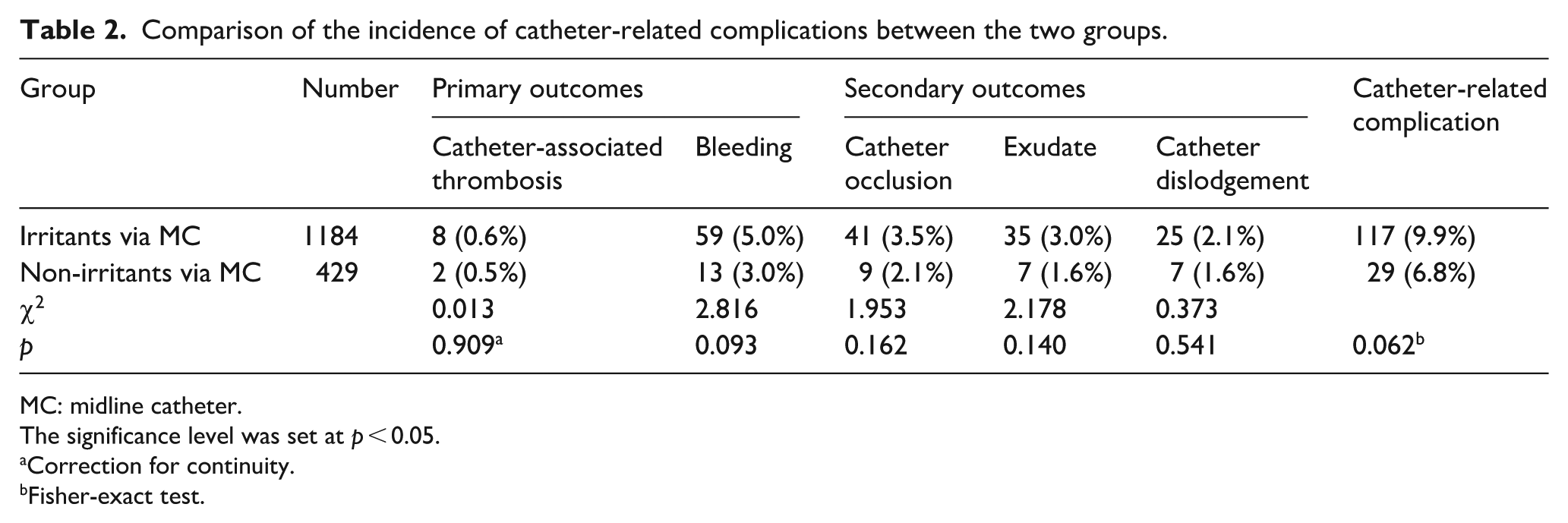
MC: midline catheter.
The significance level was set at p < 0.05.
Correction for continuity.
Fisher-exact test.
Multivariate logistic regression analysis
Multivariate logistic regression analysis revealed that the platelet count (p = 0.008, adjusted OR = 0.997, 95% CI = 0.995–0.999), the catheter duration (p < 0.001, adjusted OR = 1.036, 95% CI = 1.020–1.051), and the choice of vein, for example, brachial (vs basilica; p = 0.002, adjusted OR = 2.369, 95% CI = 1.385–4.052), were significant independent risk factors associated with catheter-related complications. The results are shown in Table 3.
Multivariable logistic regression analyses of factors associated with catheter-related complication.
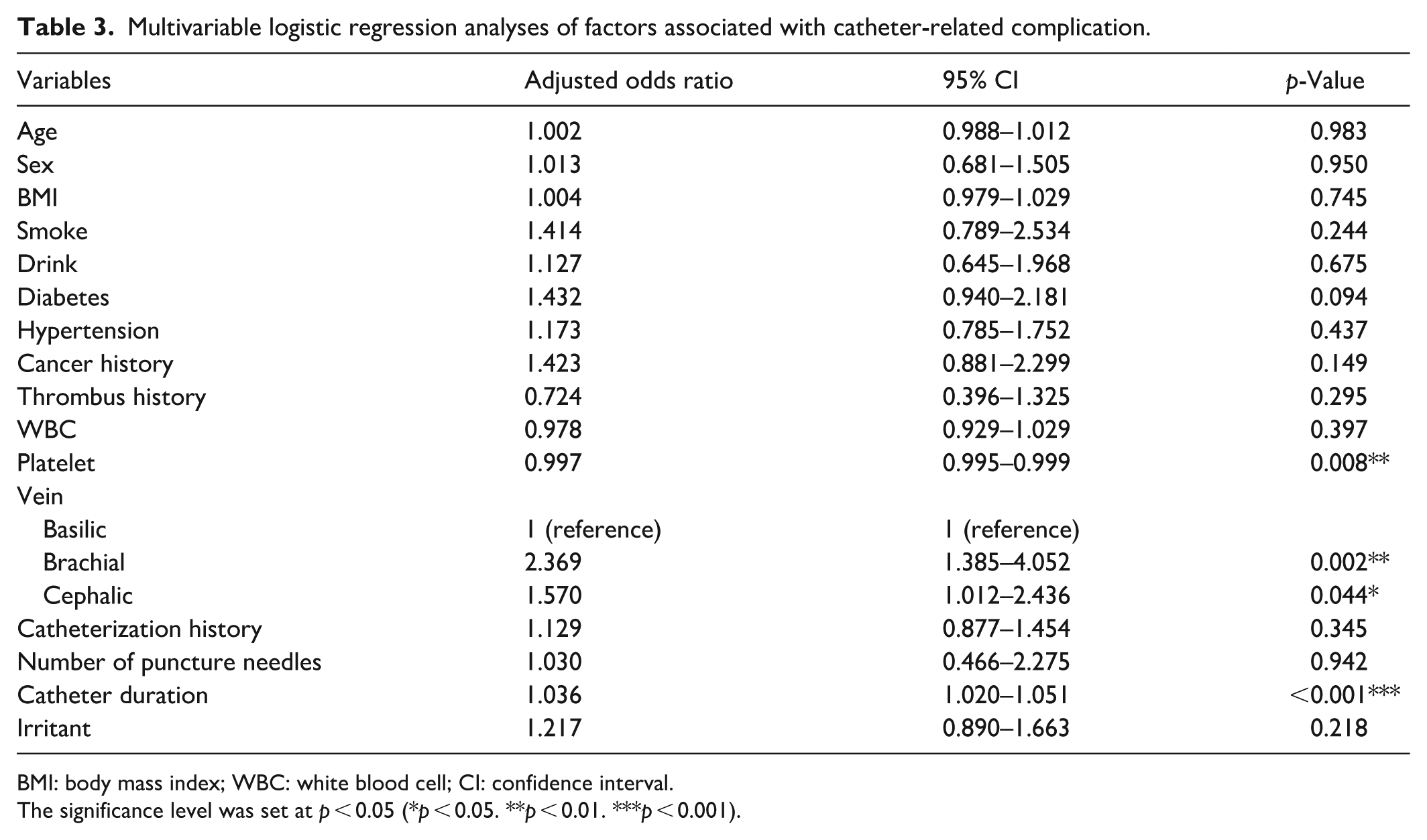
BMI: body mass index; WBC: white blood cell; CI: confidence interval.
The significance level was set at p < 0.05 (*p < 0.05. **p < 0.01. ***p < 0.001).
Subgroup analyses
There were no significant associations between irritant administration through MCs and catheter-related complications in the subgroups of age, body mass index, hypertension, diabetes, vein, catheter duration, and catheterization history subgroups (p > 0.05). All the interaction tests were non-significant (p > 0.05). Details of the subgroup analysis are presented in Figure 2.
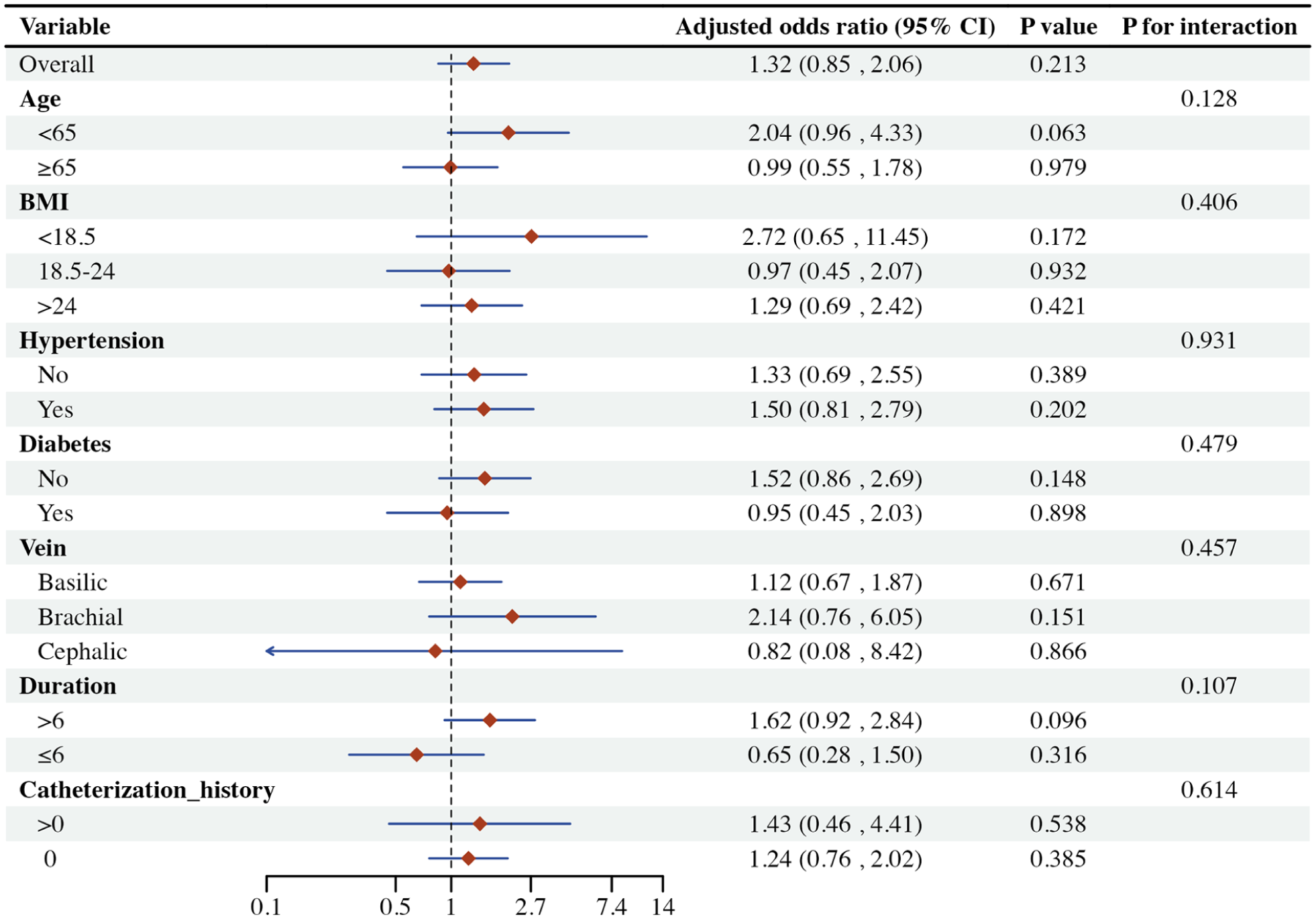
Forest plot of subgroup analyses.
Comparison of the catheter-related complications after propensity score matching
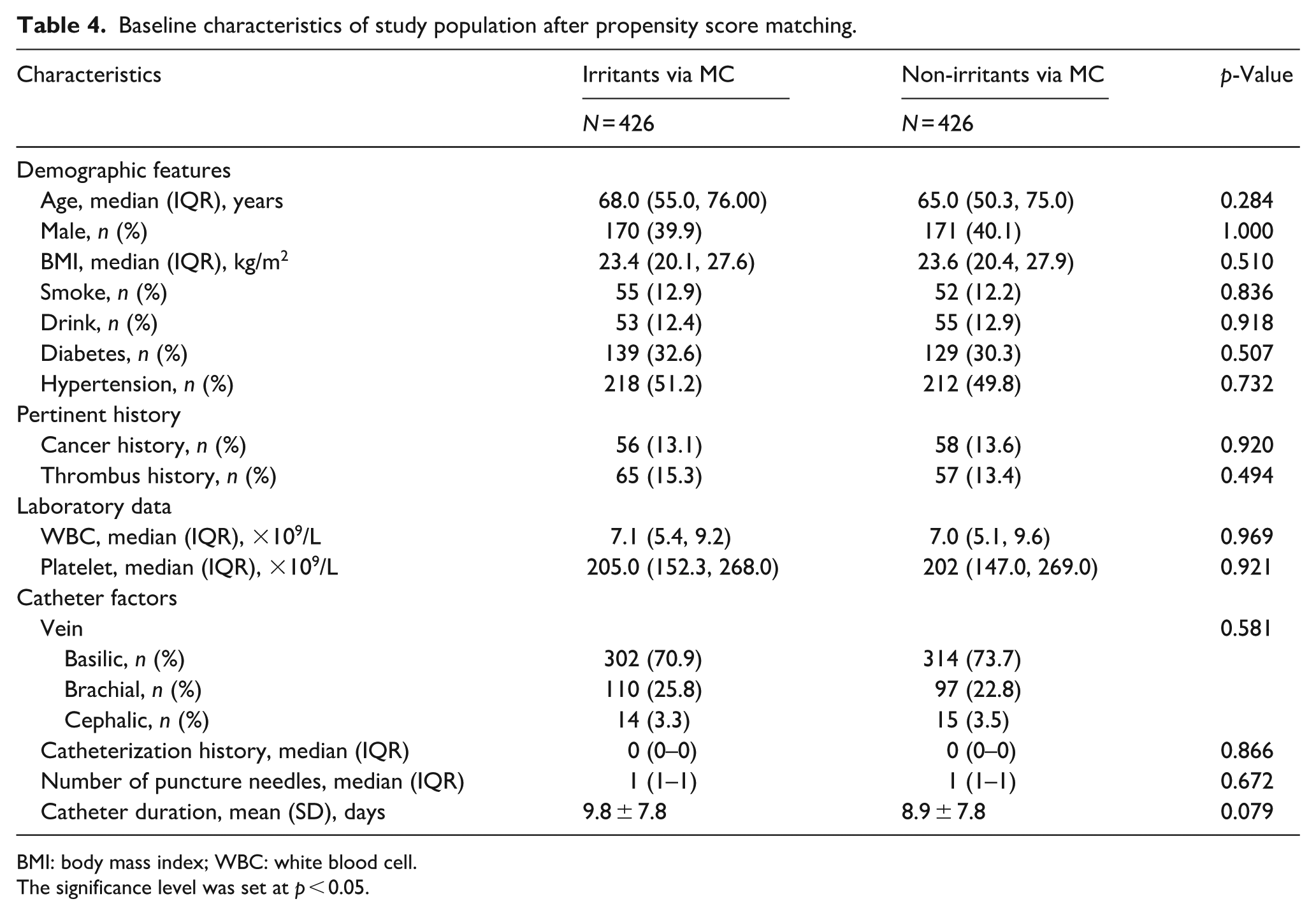
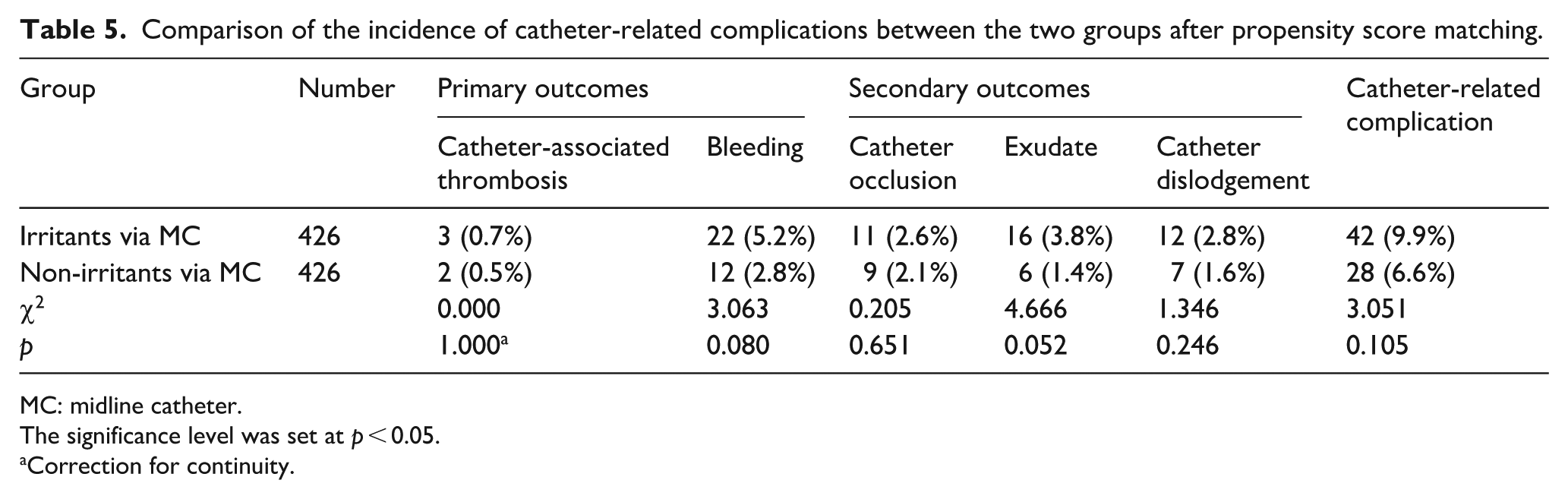
The matching ratio was set to 1:1 and the caliper width was set to 0.2. Finally, 426 patients in each group were selected for the analysis. After propensity score matching, the baseline characteristics were well balanced between the groups. Comparisons of patient characteristics and other variables between the two groups are shown in Table 4. None of the 852 patients included in the two groups experienced phlebitis, catheter-related infection, infiltration, and extravasation. There were no significant differences in the incidences of exudate, bleeding, catheter dislodgement, catheter occlusion, or catheter-related thrombosis between the two groups (p > 0.05; Table 5). The results of multivariate logistic regression analysis after propensity score matching are shown in Table S5.
Baseline characteristics of study population after propensity score matching.
BMI: body mass index; WBC: white blood cell.
The significance level was set at p < 0.05.
Comparison of the incidence of catheter-related complications between the two groups after propensity score matching.
MC: midline catheter.
The significance level was set at p < 0.05.
Correction for continuity.
Sensitivity analyses
A total of 405 orthopedic patients were analyzed and the results of the sensitivity analysis were robust (p = 0.136, adjusted OR = 3.281, 95% CI = 0.688–15.646) in Table S6.
Discussion
Principal findings
To our knowledge, this was the first study to analyze the clinical records of patients with MCs and to explore the effects of irritants on catheter-related complications. The first finding of importance was that the number of catheter-related complications associated with the administration of irritants through MCs was not high, and there were no significant differences in catheter-related complications before and after propensity score matching compared with patients who did not receive irritants. This may be related to the position of the catheter tip. The tip of the MC were located in the subclavian vein or axillary vein of the chest wall where the blood flow rate was as high as 300–1000 mL/min. 20 Because of the high speed of the blood flow, irritants were easily diluted, reducing blood coagulation and the irritation to the endothelium of the blood vessel, thereby not significantly increasing the risk of catheter-related complications.12,20,21 However, it is also possible that, as with any comparative effectiveness study, we failed to adjust for unobserved confounders, which may have underpowered our study to detect a true difference in the odds of developing a catheter-related complication. Second, we identified the platelet count, the vein (brachial and cephalic), and the catheter duration were as significant risk factors for catheter-related complications. When a MC catheter as a foreign body is inserted into a blood vessel, platelets accumulate around the catheter, easily forming a thrombus, which can lead to exudation and catheter blockage. 22 Because the cephalic vein was more superficial and has more branches and valves than the basilic vein, this can slow blood flow or damage the valves, increasing the risk of catheter-related complications. 23 Therefore, the basilic vein is the first choice for catheterization.9,24 These findings were further confirmed by subgroup analysis, propensity score matching, and sensitivity analysis. In total, our findings should provide confidence that the use of MCs for irritants was likely safe from the standpoint of catheter-related complications.
Comparison with other studies
As the use of MCs has gradually increased, the safety of drug infusion through this type of catheter has attracted increasing attention. To our knowledge, three articles have investigated the safety of the infusion of two kinds of irritants (but also vesicants) through MCs. Caparas and Hu 25 conducted a prospective, controlled, randomized clinical trial on 54 patients to determine whether intravenous vancomycin could be safely administered through a MC (not mentioned the tip position) and reported that the two groups did not differ significantly with respect to total complications (17.9% with peripherally inserted central catheters vs 19.9% with the midline). However, the sample size of this study was small and the research time was short. A recent multi-center prospective cohort study of MC catheter tip in the subclavian vein and a retrospective study performed on 248 patients reported that there was no significant association of vasopressor administration with catheter-related complications.26,27 However, different from our results, in the subgroup analysis of the catheter duration, there was an association between drug administration through the midline and catheter-related complications. In our study, we have expanded the research scope of drug infusion in order to explore the drug indications for MCs.
Other studies have compared the safety of catheters. Swaminathan et al. 4 compared the outcomes of peripherally inserted central catheters with those of MCs used in patients for whom there was an indication of difficult vascular access or antibiotic therapy for 30 or fewer days in 48 hospitals, and reported that, compared with peripherally inserted central catheters, MCs were associated with fewer bloodstream infections and catheter occlusions but with similar thrombosis events. However, this study did not account for differences in manufacturers, coatings, or device-specific features that are peculiar to catheters. Marsh et al. 8 conducted a parallel-group, pilot randomized controlled trial of 143 participants and reported that peripheral intravenous catheters had shorter functional dwell time and a greater incidence of post-insertion failure compared to MCs. One systematic review revealed that MCs had lower infection rates and higher rates of mechanical complications than the reported rates of central venous catheters. 2 Another meta-analysis also showed that the incidence of catheter-related bloodstream infection for MCs was lower than that for peripherally inserted central catheters during intravenous infusion therapy. In view of these results, MCs have advantages and are worthy of further exploration and clinical promotion.
Limitations and strengths of the study
Importantly, several limitations to the study should be noted when interpreting and making use of the results. First, as this was a retrospective study, unmeasured confounding factors may have affected the conclusions. However, we used the propensity score matching method to minimize bias between the two groups. Second, because we did not find the relevant information for a few drugs, we could not judge whether they were irritants according to the judgment criteria used for irritants in this study. We excluded these patients, which may have affected the results. And MCs were not suitable for all patients, so we were unable to collect all irritants. Third, although the variables included in the models were clinically chosen and based on plausible pathways, our models do not imply causation and only show associations between exposure and outcomes.
However, the strengths of our study stemmed from its novelty in comparing the safety of irritants delivered through MCs that were located in the subclavian vein or axillary vein of the chest wall, which clarified the indications for the catheters and could help inform healthcare professionals about catheter selection in clinical practice. Our results were internally consistent when robust statistical techniques, multivariate analysis, subgroup analysis, propensity score matching analysis, and sensitivity analysis were used.
Conclusions
It is crucial to choose the appropriate catheter for patients in clinical nursing. MCs can serve as a bridge between peripheral intravenous catheters and central venous catheters. In this study, we found no significant association between the administration of irritants through MCs with catheter-related complications. As the use of midlines for irritant delivery becomes more common, randomized clinical trials are needed to help ensure patient safety.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298251387289 – Supplemental material for The association of irritant administration via midline catheters with catheter-related complications: A longitudinal cohort study
Supplemental material, sj-pdf-1-jva-10.1177_11297298251387289 for The association of irritant administration via midline catheters with catheter-related complications: A longitudinal cohort study by Yi Zhang, Chang Liu, Jie Wang, Xiuzhu Cao, Yilin Chen, Yiyu Zhuang and Linfang Zhao in The Journal of Vascular Access
Supplemental Material
sj-pdf-2-jva-10.1177_11297298251387289 – Supplemental material for The association of irritant administration via midline catheters with catheter-related complications: A longitudinal cohort study
Supplemental material, sj-pdf-2-jva-10.1177_11297298251387289 for The association of irritant administration via midline catheters with catheter-related complications: A longitudinal cohort study by Yi Zhang, Chang Liu, Jie Wang, Xiuzhu Cao, Yilin Chen, Yiyu Zhuang and Linfang Zhao in The Journal of Vascular Access
Footnotes
Acknowledgements
Author contributions
Linfang Zhao and Yi Zhang: Conceptualization, Methodology, Visualization, Formal analysis, Investigation, Data curation, Writing—original draft, Writing—review & editing. Yiyu Zhuang: Conceptualization, Methodology, Formal analysis, Investigation, Data curation, Project administration, Funding acquisition. Chang Liu: Methodology, Formal analysis, Investigation, Data curation, Supervision, Funding acquisition. Jie Wang: Methodology, Formal analysis, Data curation, Funding acquisition, Writing—review & editing. Xiuzhu Cao: Methodology, Formal analysis, Data curation, Writing—review & editing. Yilin Chen: Methodology, Formal analysis, Data curation, Visualization.
Availability of data and material
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Nursing Clinical Research Project of Shaoyifu Hospital Affiliated to Zhejiang University School of Medicine (grant numbers 2024HLKY06) and Zhejiang Medical and Health Science and Technology Project (grant numbers 2021KY740).
Ethical approval
Permission was obtained from the Clinical Research Ethics Committee and the institution where the research was conducted.
Consent for publication
All authors consent for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.