
Abstract
Superior vena cava (SVC) occlusion is a major complication in hemodialysis patients, impairing access function and requiring timely intervention. A 69-year-old man undergoing maintenance hemodialysis for 8 years presented with a 1-month history of inadequate flow in a left upper-arm arteriovenous graft (AVG). Physical examination revealed prominent chest and abdominal wall veins with a caput-medusae pattern. DSA showed multiple venous stenoses, and complete SVC and right subclavian vein occlusion. Using coronary guidewires and microcatheters, the occluded segments were successfully recanalized, followed by SVC angioplasty and the placement of a covered stent. Postoperatively, venous dilation and facial edema resolved, and AVG function improved. This case illustrates the feasibility of adapting coronary guidewire and microcatheter techniques as an alternative approach for recanalization of complex central venous occlusion in selected hemodialysis patients.
Keywords
Introduction
Hemodialysis is the primary renal replacement therapy for patients with end-stage renal disease, and its effectiveness is closely dependent on the patency of the vascular access. During long-term hemodialysis, vascular-related complications not only interfere with adequate dialysis delivery but may also pose significant risks to patient survival. 1 Central venous stenosis or occlusion (CVS/CVO) is a serious complication in this patient population. Typical manifestations include dilated chest and abdominal wall veins, ipsilateral upper-limb swelling or venous congestion, elevated venous pressure, and reduced dialysis access function. 2 When the superior vena cava (SVC) is severely involved, the condition may progress to superior vena cava syndrome (SVCS), which commonly presents with facial, neck, and upper-limb swelling, dyspnea, headache, and even cognitive or sensory disturbances. In the general population, malignancy is the leading cause of SVCS, accounting for approximately 70% of all cases. 3 However, with the increasing number of patients undergoing long-term hemodialysis and repeated central venous catheterization, benign causes of SVCS related to dialysis access have become increasingly prevalent. In this setting, SVC occlusion not only threatens the long-term patency of the dialysis access but may also progress to a life-threatening emergency. 4 Management of chronic SVC occlusion in hemodialysis patients remains technically challenging. Endovascular recanalization is generally preferred, but procedural success may be limited in long-standing occlusions, particularly when conventional venous techniques are unsuccessful or unavailable. Although sharp and radiofrequency-assisted recanalization methods have been described, these approaches may be associated with higher procedural risk or require specialized equipment and expertise. In this context, we report a case of chronic SVC occlusion in a maintenance hemodialysis patient successfully treated using coronary guidewire and microcatheter–based techniques. This case illustrates the feasibility of adapting technical principles and equipment commonly used in coronary interventions as an alternative strategy for traversing complex central venous occlusions in selected patients.
Case report
A 69-year-old man was admitted for insufficient blood flow in a left upper-arm arteriovenous graft (AVG) for 1 month. He was diagnosed with end-stage renal disease in 2017 and subsequently initiated hemodialysis. During the course of treatment, a semi-permanent catheter was placed in the right internal jugular vein, and a native arteriovenous fistula (AVF) was created in the left forearm. After 6–8 weeks of maturation, the fistula became suitable for dialysis use, and the right internal jugular catheter was removed, using AVF for hemodialysis. In 2020, the patient developed reduced flow in the left forearm AVF and subsequently underwent creation of a left upper-arm arteriovenous graft (AVG) to maintain dialysis access. This graft functioned adequately until 1 month before admission, when decreased blood flow recurred. Admission physical examination: Vital signs were stable. The patient had a medium build, clear consciousness, fluent speech, facial edema, and no obvious congestion, rashes, erythema, infections, ulcers, or wounds on the skin. The veins of the chest and abdomen were significantly dilated and extended to the neck. There were no obvious abnormalities in muscle strength and tone of the limbs, and there was no significant pitting edema in both lower extremities (Figure 1(a)). Important auxiliary examination showed mild reductions in blood cell counts on complete blood count, while other parameters were largely within normal limits. Liver function tests were normal. Abdominal ultrasound revealed no evidence of cirrhosis, splenomegaly, or portal vein thrombosis. Chest CT-Scan demonstrated multiple small pulmonary nodules, as well as multiple enlarged lymph nodes in the mediastinum and axillary regions. Digital subtraction angiography (DSA) showed mild-to-moderate stenosis at the anastomosis between the left AVG and axillary vein, moderate stenosis in the proximal segment of the left subclavian vein, occlusion of the right subclavian vein, and occlusion of the superior vena cava (Figure 2(a) and (b)).
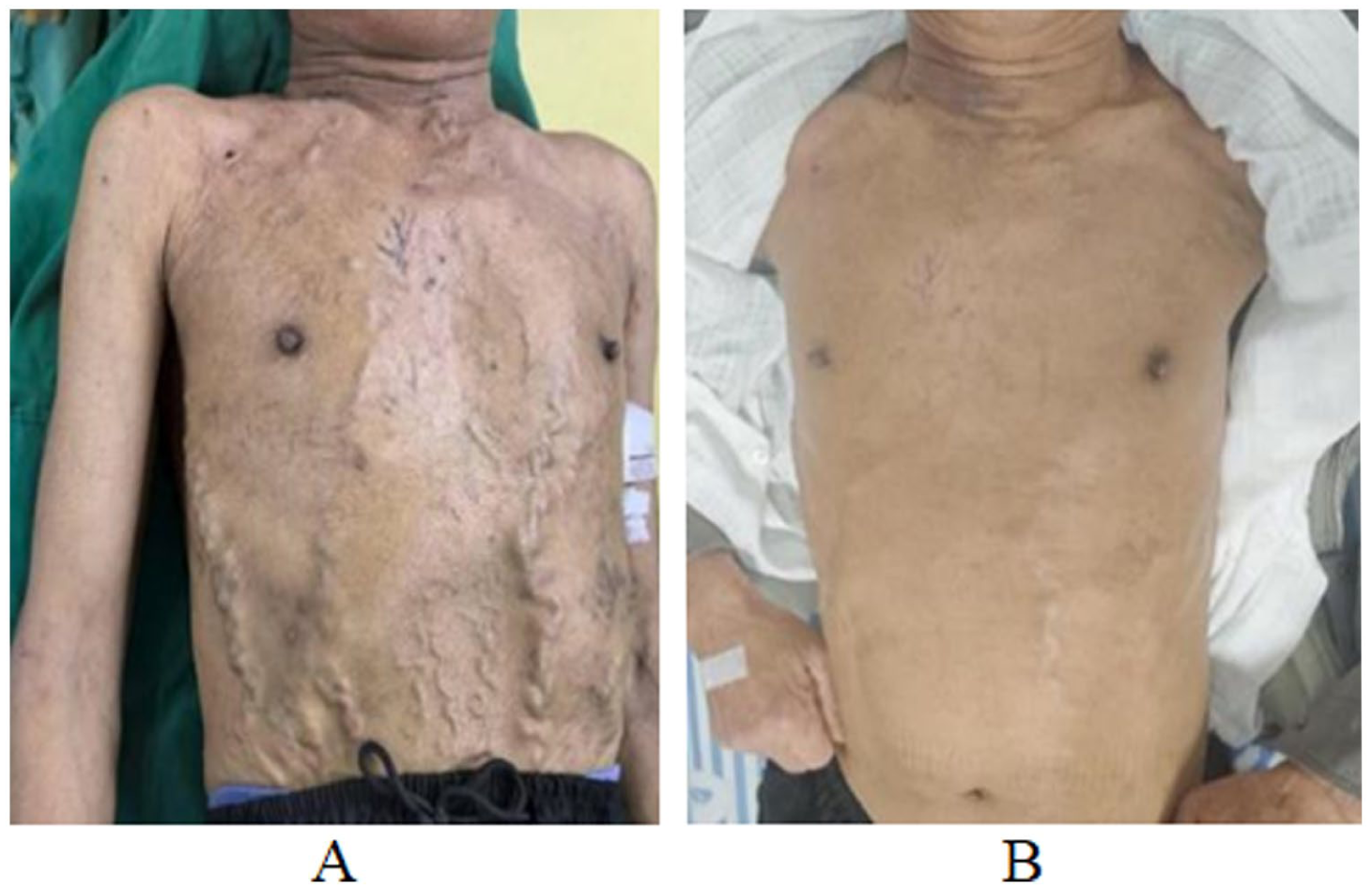
(a) Marked dilation of the chest and abdominal wall veins at admission and (b) significant improvement in venous dilation following angioplasty and placement of a superior vena cava stent.
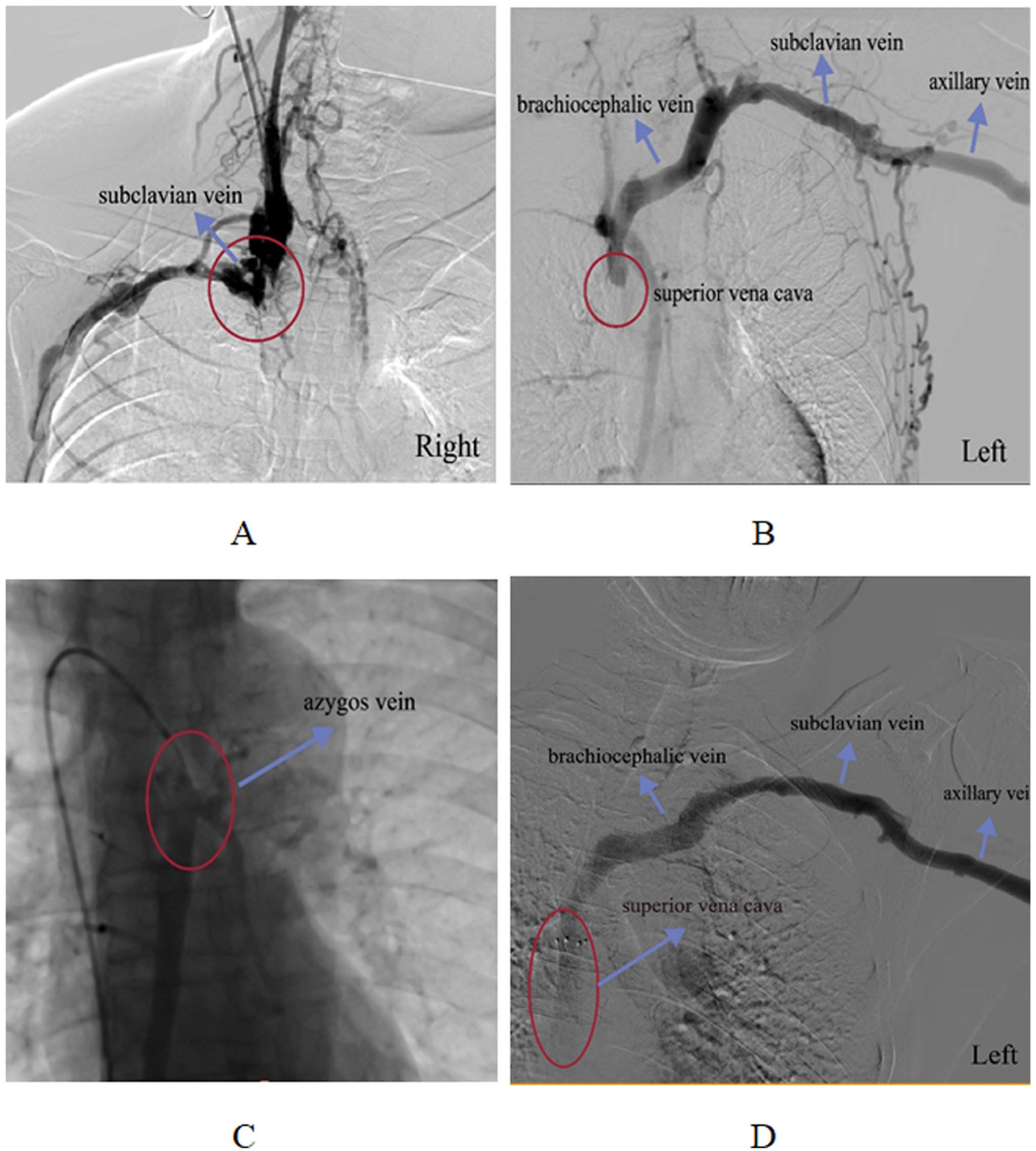
(a) Occlusion at the proximal segment of the right subclavian vein, (b) venography demonstrating complete occlusion of the superior vena cava, (c) advancement of the guidewire and microcatheter through the occluded superior vena cava into the azygos vein, and (d) venography following PTAS shows restored venous return and resolution of the previously observed retrograde collateral circulation.
The patient presented with complete occlusion of the superior vena cava. After consultation with the department of cardiology team, interventional recanalization was planned. During the procedure, via a right femoral vein puncture approach, the initial attempt to advance a 0.035-inch Loach guidewire across the occluded segment was unsuccessful. A 6F JR3.5 guiding catheter was subsequently introduced. With assistance from an Instantpass 2.6F-130 cm microcatheter, a 0.014-inch Sion coronary guidewire was advanced. After multiple attempts, it successfully crossed the occlusion, entered the azygos vein, and was retained (Figure 2(c)). Stepwise dilatation of the superior vena cava was then performed using coronary balloon catheters (1 mm × 6 mm, 2 mm × 20 mm, 3 mm × 15 mm), and an Ultratimes coronary balloon catheter (4 mm × 30 mm). The 5F single-curve catheter was exchanged for a 2.6 m Loach guidewire, which was positioned in the azygos vein, and a 7F sheath was advanced. Peripheral balloon catheters (D Konquer 6 mm × 40 mm, 8 mm × 40 mm, 10 mm × 40 mm) were then used for sequential dilatation of the superior vena cava. Post-dilatation angiography revealed residual stenosis of >70%. A balloon (Bard 12 mm × 60 mm) was subsequently used to dilate the proximal left innominate vein and superior vena cava; however, angiography still demonstrated elastic recoil with greater than 50% stenosis. Ultimately, a fluency stent (Bard 14 mm × 60 mm) was deployed across the stenotic segment of the superior vena cava. The stent was precisely positioned without obstructing the ostia of the azygos vein or the left innominate vein (Figure 2(d)). Post-stent angiography confirmed restored patency of the superior vena cava. Following the intervention, the patient’s thoracoabdominal varices showed marked improvement, and the artificial arteriovenous fistula regained patency. The patient was discharged in stable condition after a 2-week postoperative hospitalization (Figure 1(b)).
It should be noted that central venous recanalization, particularly for chronic occlusions, carries a risk of thrombus dislodgement leading to pulmonary embolism. Previous reports have documented fatal pulmonary embolism following endovascular interventions in hemodialysis patients. 5 In this case, thrombus burden was carefully evaluated preoperatively, gentle endovascular techniques were applied, and close postoperative monitoring was performed; no embolic complications occurred. Clinicians are advised to remain vigilant about this risk in clinical practice and to prepare appropriate contingency plans.
Discussion
Central venous stenosis or occlusion is a common clinical problem for patients undergoing maintenance hemodialysis. Its occurrence is mainly related to the previous history of central venous catheter insertion, the long-term use of tunnel-type dialysis catheters, or pacemaker electrode wires, among other factors. 6 Repeated central venous catheterization and the formation of blood turbulence after the establishment of arteriovenous fistulas (AVF) or grafts (AVG) can cause damage to the venous intima, thereby triggering thrombosis and fibrotic repair reactions, ultimately leading to vascular lumen stenosis or even complete occlusion. 6 Such lesions are commonly seen in hemodialysis patients who establish upper limb vascular access, often involving the jugular vein, subclavian vein, brachiocephalic vein, and superior vena cava, etc. 7 When the superior vena cava becomes occluded, due to the obstruction of the main venous return blood flow, the systemic circulation can establish compensatory return pathways through collateral circulation, such as thoracic wall veins, intercostal veins, and superficial abdominal veins. Clinically, the visible dilation of the thoracic and abdominal wall veins may indicate that there is upper vena cava or central venous obstruction in the hemodialysis patient. 2
Imaging assessment of central venous stenosis or occlusion (CVS/CVO) is essential for establishing a definitive diagnosis and guiding subsequent treatment planning. Doppler ultrasound, as the preferred noninvasive screening modality, can evaluate hemodynamic changes in peripheral veins as well as segments of the proximal central venous system. However, because the subclavian vein, azygos vein, and superior vena cava are deeply located and partially obscured by thoracic bony structures, ultrasound often provides limited visualization of these regions. Digital subtraction angiography (DSA) remains the gold standard for diagnosing CVS/CVO. This technique provides real-time imaging with high spatial resolution, enabling precise evaluation of stenosis severity, occlusion length, and collateral circulation development. It also allows simultaneous interventional procedures, including percutaneous transluminal angioplasty or stent placement, to be performed during the same session. For patients who are not suitable candidates for DSA, computed tomography venography (CTV) and magnetic resonance venography (MRV) serve as important alternative imaging modalities. Both modalities clearly depict venous anatomy, define the extent of lesions, and assess collateral circulation, providing significant clinical value—particularly for evaluating recurrent or complex cases. 8
Endovascular intervention is currently the primary therapeutic strategy for central venous stenosis or occlusion (CVS/CVO), with percutaneous transluminal angioplasty (PTA) and percutaneous transluminal angioplasty and stent placement (PTAS) being the most widely adopted techniques. These interventions can rapidly re-establish venous patency and relieve clinical symptoms. Nevertheless, substantial heterogeneity persists across studies regarding technical success, complication rates, and long-term patency, and a unified treatment consensus has yet to be established. 9 Several retrospective and meta-analytic studies have attempted to clarify the comparative efficacy of PTA and PTAS. Cantador et al. 10 analyzed 25 cases of stenosis and 22 cases of occlusion, reporting that 64% of patients underwent combined PTA and stenting, while 36% received PTA alone. High rates of early clinical improvement were achieved within 30 days, and at 12 months, primary and assisted primary patency rates were 57% and 72%, respectively. Similarly, in a meta-analysis by Wu et al. 11 involving 281 patients treated with PTA and 192 patients treated with PTAS, primary patency did not differ significantly between the two modalities at 3, 6, 12, or 24 months. Notably, however, PTA demonstrated consistently higher assisted primary patency. Further evidence from Tao et al. 12 compared PTA alone with sequential PTAS in 26 patients. Primary patency rates at 3, 6, 9, and 12 months were comparable between the two strategies, with only modest differences. Based on these findings, the authors recommend PTA alone for lesions exhibiting <50% central venous elastic retraction, whereas sequential PTAS is favored when central venous elastic retraction is ⩾50%. Both approaches were deemed safe and effective, underscoring the importance of individualized decision-making. Collectively, current evidence underscores that treatment selection for CVS/CVO in maintenance hemodialysis patients should be based on lesion characteristics, degree of central venous elastic retraction, and patient-specific factors. Equally important, rigorous postoperative surveillance and timely reintervention are crucial for optimizing long-term patency and clinical outcomes.
Traditional percutaneous venous recanalization techniques, including balloon angioplasty and stent placement, are effective for short-segment or partial central venous stenosis. However, in chronic total occlusions or long-segment fibrotic lesions, procedural failure commonly occurs because standard guidewires cannot traverse the occluded segment. To improve recanalization success in these complex lesions, advanced approaches such as sharp recanalization and radiofrequency (RF) guidewire-assisted recanalization have been increasingly implemented. 13 Sharp recanalization has shown feasibility in selected refractory cases. Wei et al. 14 reported successful recanalization of a 6.9-cm superior vena cava occlusion in a hemodialysis patient using the RUPS-100 puncture system under bidirectional fluoroscopic guidance, with preserved access function at 30 months. However, risks such as vessel perforation and pericardial hematoma must be considered. RF guidewire-assisted recanalization offers another option for lesions resistant to conventional techniques. In a retrospective series by Moawad et al. 15 the PowerWire RF guidewire achieved an 81% technical success rate with a 14% major complication rate. Primary patency at 1 and 2 years reached 94% and 85%, respectively, accompanied by significant symptom improvement. Compared with sharp recanalization, RF guidewire-assisted recanalization may provide higher efficacy and potentially better safety in managing chronic central venous occlusions. Despite encouraging outcomes, both sharp and RF-assisted techniques carry risks of major complications, including hemothorax and cardiac tamponade due to vascular perforation. Careful patient selection, strict adherence to procedural indications, and meticulous intraoperative imaging guidance are essential to ensure safe and effective use in clinical practice.
Conclusion
Based on the present case and available literature, dilation of the chest and abdominal wall veins in hemodialysis patients with superior vena cava (SVC) occlusion represents a compensatory manifestation of collateral venous circulation. Definitive diagnosis requires imaging studies to identify the location and etiology of the occlusion, and treatment should be individualized according to the patient’s specific condition. Endovascular intervention is a safe and effective therapeutic option; however, regular postoperative follow-up and, when necessary, repeat interventions are required to maintain long-term patency. In cases of complete venous occlusion in which conventional venous guidewires are unable to cross the lesion, this case indicates that the use of smaller-caliber coronary guidewires with superior penetration capability and torque control, in conjunction with microcatheter support and subsequent stepwise balloon dilation, may enable controlled recanalization of fibrotic venous segments. Notably, under the collaboration of a multidisciplinary team, this strategy does not represent a direct application of coronary chronic total occlusion techniques, but rather an adaptation of selected guidewire-handling principles and device properties to address a technically challenging venous anatomy. Such a strategy may be considered as an alternative option in selected patients.
Footnotes
Author contributions
Conceptualization, Data curation, Writing—original draft, Writing—review & editing: Longzhu Li. Data curation, Formal Analysis, Investigation, Methodology, Writing—review & editing: Juan Du and Jingchun Yao. Methodology, Resources, Visualization, Writing—review & editing: Qing Xia and Xinhu Tang. Funding acquisition, Resources, Supervision, Validation, Writing—original draft, Writing—review & editing: Meijun Wu.
Data availability
The data of this study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Jiangxi Provincial Department of Education Scientific Research Project (Grant No. GJJ190936).
Ethical approval
This study was performed in accordance with the Declaration of Helsinki. This human study was approved by the Ethics Committee of Affiliated Hospital of Jiujiang University (Jiangxi Province, China)—approval: jjumer-b-2025-11002.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report; all information has been de-identified.