
Abstract
Background:
Noise in pediatric emergency departments can impair procedural performance. We evaluated the effect of active noise-canceling (ANC) earphones on the outcomes of pediatric peripheral intravenous catheter (PIVC) insertion.
Methods:
This randomized controlled trial included 202 children (<8 years) requiring PIVC insertion. Participants were randomly assigned to operators wearing ANC earphones or a control group without earphones. The primary outcome was the first-attempt success rate, and secondary outcomes included procedure time.
Results:
First-attempt success rates were similar between the ANC and control groups (89.5% vs 89.7%; p > 0.99). The overall time reduction was not statistically significant (p = 0.089; Cohen’s d = −0.17). However, effect size estimates suggested relatively larger differences in challenging scenarios, including patients with difficult venous access (Cohen’s d = −0.39) and those requiring multiple attempts (Cohen’s d = −0.66).
Conclusions:
Among skilled operators, ANC earphones were not associated with an improved first-attempt success rate. Exploratory analyses suggested a potential signal of reduced cannulation time in more complex situations; however, these findings were hypothesis-generating and require confirmation in larger, multicenter studies.
Introduction
Peripheral intravenous catheter (PIVC) insertion is one of the most frequently performed invasive procedures in pediatric care, both in emergency departments and on general wards. 1 However, securing PIVC access in children is technically more challenging than in adults, and a substantial proportion of pediatric patients are classified as having difficult intravenous access (DIVA). 2 This difficulty is also reflected in DIVA prediction tools, which consider factors such as younger age and reduced vein visibility or palpability.3,4
In response, clinical practice has adopted various strategies, including early identification of high-risk DIVA patients for ultrasound-guided insertion and the implementation of PIVC insertion algorithms and specialized vascular access teams. These approaches mainly focus on optimizing patient, vessel, and technique-related factors to improve success rates and reduce complications.5–7
By contrast, the influence of the operator’s cognitive and emotional environment—particularly factors such as noise and stress—on PIVC success has received relatively little attention. The detrimental effects of noise on procedural performance are well documented in operating rooms and intensive care units. Prior studies have shown that average noise levels in healthcare settings frequently exceed World Health Organization (WHO) recommendations and are associated with impaired team communication, increased error rates, procedural delays, and heightened mental workload.8,9 Simulator-based studies further suggest that background noise worsens error rates and task completion times in arthroscopic and laparoscopic procedures, or at least significantly increases mental workload.10,11
However, these findings are largely restricted to adult operating rooms and simulated settings. There is a paucity of research on how noise exposure affects the operator’s psychological state and procedural success in real-world clinical situations that require short bursts of intense concentration, such as pediatric PIVC insertion. This represents an important gap in the literature, given that pediatric PIVC insertion depends not only on technical and anatomical difficulty but also on the operator’s psychological state and working environment.
Active noise canceling (ANC) technology may offer a practical way to mitigate these environmental constraints. Environmental noise can increase mental workload and degrade performance on attention-demanding tasks, particularly in safety-critical work settings. 12 A recent neurophysiological study using functional near-infrared spectroscopy demonstrated that wearing ANC devices significantly modulates prefrontal cortex responses in noisy environments, thereby preserving cognitive resources and maintaining concentration. 13 These findings suggest that ANC may reduce auditory distraction and support concentration during procedures demanding high levels of attention.
In this study, we aimed to evaluate the effect of ANC on clinical performance by randomizing the use of active noise-canceling earphones among operators during pediatric PIVC insertion. We compared the primary outcome of first-attempt success rate and secondary outcomes, including procedure time and number of attempts.
Methods
Study design and setting
This was a single-center, parallel-group, randomized controlled trial conducted in the pediatric emergency department of a tertiary children’s hospital in South Korea. Patient recruitment and data collection were conducted between June 2022 and January 2023. The trial aimed to compare the outcomes of PIVC insertion performed by operators wearing ANC earphones versus those performing the procedure under standard environmental conditions without earphones. This study was reported in accordance with the CONSORT statement and was registered at cris.nih.go.kr (KCT0008116).
Participants
Eligible participants were children younger than 8 years of age who presented to the pediatric emergency department and required PIVC insertion during the study period.
We excluded children classified as level 1 on the Korean Triage and Acuity Scale (KTAS), a widely used 5-level emergency department triage system in Korea. KTAS level 1 denotes the highest acuity requiring immediate resuscitation, such as cardiopulmonary resuscitation or impending airway compromise. We also excluded children requiring immediate central venous or intraosseous access and those for whom peripheral access was not attempted due to clinical reasons.
Consecutive eligible patients were screened, and those fulfilling all inclusion and exclusion criteria were enrolled after informed consent had been obtained from their legal guardians.
All PIVC procedures were performed by members of a dedicated vascular access team (hereafter referred to as operators). This team consisted of clinicians whose primary responsibility is peripheral blood sampling and catheter placement in both adult and pediatric sections of the emergency department. Team members rotate between the adult and pediatric areas on a monthly schedule and perform the majority of vascular access procedures in the pediatric emergency department. All operators participating in the trial provided written informed consent.
Interventions
Participants assigned to the active noise-canceling intervention (ANC group) underwent PIVC insertion performed by an operator wearing active noise-canceling earphones throughout the procedure. The devices were set to “Noise Cancellation” mode to minimize ambient noise, without playing any music or additional audio content. We used AirPods Pro (1st generation; Apple Inc., Cupertino, CA, USA) for this study.
In the control group, PIVC insertion was performed according to standard care, without the use of earphones. Apart from the use of ANC, all other aspects of the procedure—including vein selection, catheter gauge, and assistance from nurses or caregivers—followed local standard protocols and were left to the discretion of the treating team. No cases in either group involved procedural sedation/analgesia, topical or local anesthetics, or ultrasound-assisted/ultrasound-guided insertion during the study period.
Outcomes
The primary outcome was first-attempt PIVC success, defined as successful cannulation with blood return and flushing on the first needle insertion attempt.
Secondary outcomes included the cannulation time for the final attempt by the initial operator, the number of needle insertion attempts performed by the initial operator, and initial operator failure. For each index PIVC attempt, cannulation time was recorded in seconds. Time zero was defined as tourniquet application, chosen as the point at which the procedure begins to directly affect the child. Timing was measured by a trained research assistant (a former paramedic) using a stopwatch at the bedside. The end point was the moment successful peripheral IV patency was confirmed, defined as either (i) visible blood return (when blood sampling was required) or (ii) successful catheter flushing followed by immediate connection of IV fluids (when no blood sampling was performed).
Safety and adverse events
Given the minimal-risk classification, adverse events were prospectively defined as minor procedural outcomes (including puncture failure) and systematically assessed during and immediately after each attempt. A trained research assistant directly observed all procedures and monitored for any communication-related issues. Before the intervention, we confirmed that the ANC setting did not interfere with routine clinical communication, and operators were able to communicate with staff and caregivers as needed while wearing the earphones.
Sample size calculation
We determined the sample size based on the hypothesis that the use of ANC would improve the first-attempt success rate compared with the control group. Because first-attempt PIVC success rates in children vary across clinical settings and operator expertise, and a pediatric emergency department validation study of the DIVA prediction rule reported a first-attempt failure rate of approximately 22%, we conservatively assumed a baseline first-attempt success rate of 75% in the control group. 14 In addition, first-time PIVC insertion success rates approaching 90% have been reported in settings with greater procedural experience, supporting the plausibility of targeting an absolute 15-percentage-point improvement. 15 Assuming a two-sided α of 0.05 and 80% power, we estimated that approximately 100 participants were required per group to detect a clinically meaningful absolute increase of 15 percentage points in the first-attempt success rate, from 75% in the control group to 90% in the ANC group. Accordingly, we planned to enroll at least 200 participants in total. In the final analysis, 202 participants were included (ANC group, n = 95; control group, n = 107).
Randomization and allocation concealment
Participants were randomly assigned in a 1:1 ratio to either the ANC group or the control group. Before the trial commenced, the principal investigator generated the randomization sequence using computer-generated permuted blocks with a fixed block size of 4. The allocation sequence was concealed in sequentially numbered, opaque, sealed envelopes, which were maintained by a research assistant who was not involved in the clinical assessment. Once an eligible child was identified and informed consent was obtained, the child was enrolled. Immediately prior to the PIVC procedure, the research assistant opened the corresponding envelope in numerical order to reveal the group assignment. Treating physicians were not involved in generating the random sequence. Due to the visible nature of the intervention, blinding of the operators and participants was not feasible.
Statistical analysis
Baseline characteristics and unadjusted outcomes were compared using the Mann–Whitney U test for continuous variables and the chi-square or Fisher’s exact test for categorical variables. Procedure time was analyzed only for cases where the initial operator achieved successful cannulation. Effect sizes for continuous outcomes were quantified using Cohen’s d.
To adjust for potential confounders, we fitted a multivariable linear regression model for procedure time (log-transformed due to skewness) and a multivariable logistic regression model for prolonged procedure (>75th percentile). Both models were adjusted for multiple attempts, age, triage level, vein palpability, vein visibility, and operator pediatric experience.
Exploratory analyses included attempt-stratified comparisons and subgroup analyses based on the pediatric DIVA score and operator pediatric experience tertiles (low, middle, and high), categorized from the cohort distribution of experience in months (⩽7, 8–11, and ≥12 months in this dataset). 4
Potential effect modification was assessed in separate regression models by including interaction terms between ANC use and the DIVA score, and between ANC use and operator experience. All tests were two-sided with a significance level of p < 0.05, without adjustment for multiple comparisons.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. 2203-161-1310; approval date: May 25, 2022). Written informed consent was obtained from the legal guardians of all participating patients, as well as from the participating operators.
Results
A total of 202 children were randomized, with 95 assigned to the ANC group and 107 to the control group (Figure 1). No participants were lost to follow-up or excluded after randomization. Baseline demographic and clinical characteristics were well balanced between groups (Table 1). Median age was 35.0 months (IQR 18.5–60.0) in the ANC group and 33.0 months (IQR 17.5–48.0) in the control group. The proportion of females (37.9% vs 41.1%), triage level 3–5 (90.5% vs 85.0%), visible veins (84.0% vs 86.0%), palpable veins (72.3% vs 64.5%), and operator pediatric experience (median 10.0 vs 7.0 months) did not differ significantly between groups.
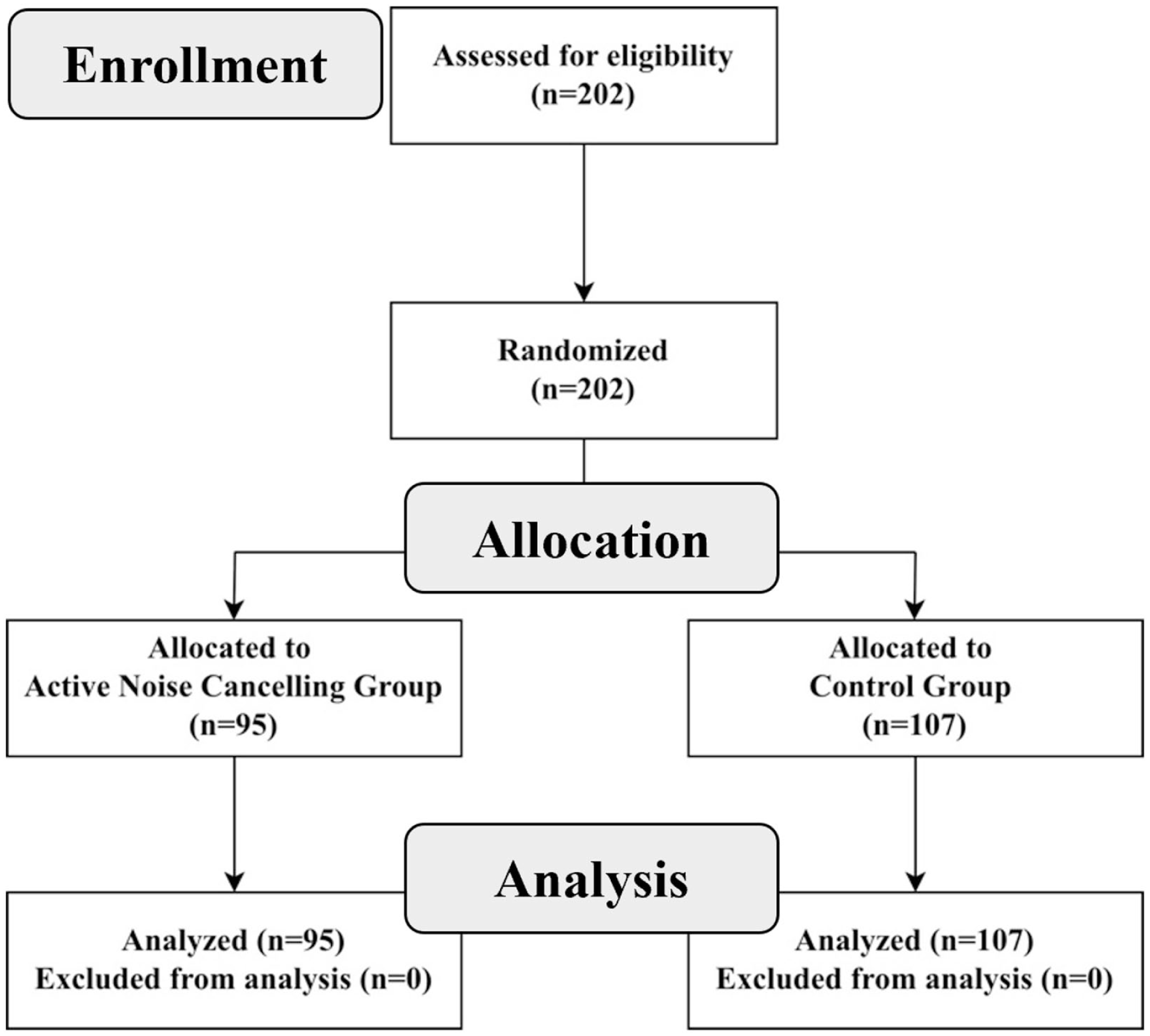
Flow diagram of the study participants.
Baseline demographic and clinical characteristics of the study participants.
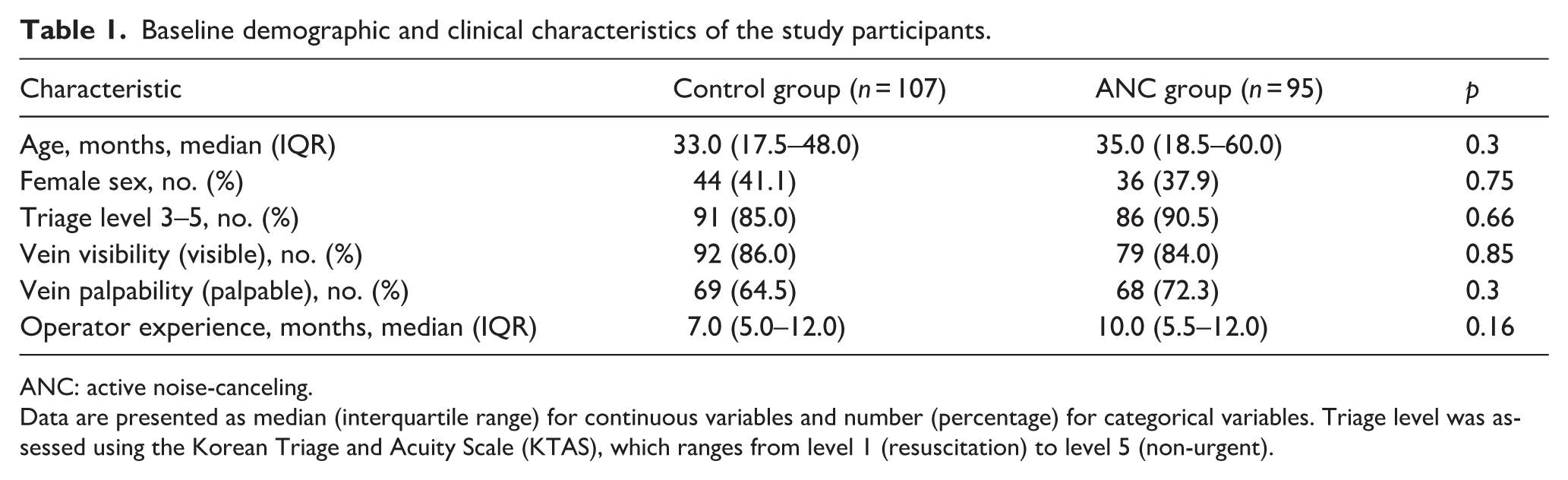
ANC: active noise-canceling.
Data are presented as median (interquartile range) for continuous variables and number (percentage) for categorical variables. Triage level was assessed using the Korean Triage and Acuity Scale (KTAS), which ranges from level 1 (resuscitation) to level 5 (non-urgent).
The primary outcome, first-attempt success, was high and similar in both groups: 85/95 (89.5%) in the ANC group and 96/107 (89.7%) in the control group (p = 1.000; Table 2).
Comparison of procedural outcomes between groups.
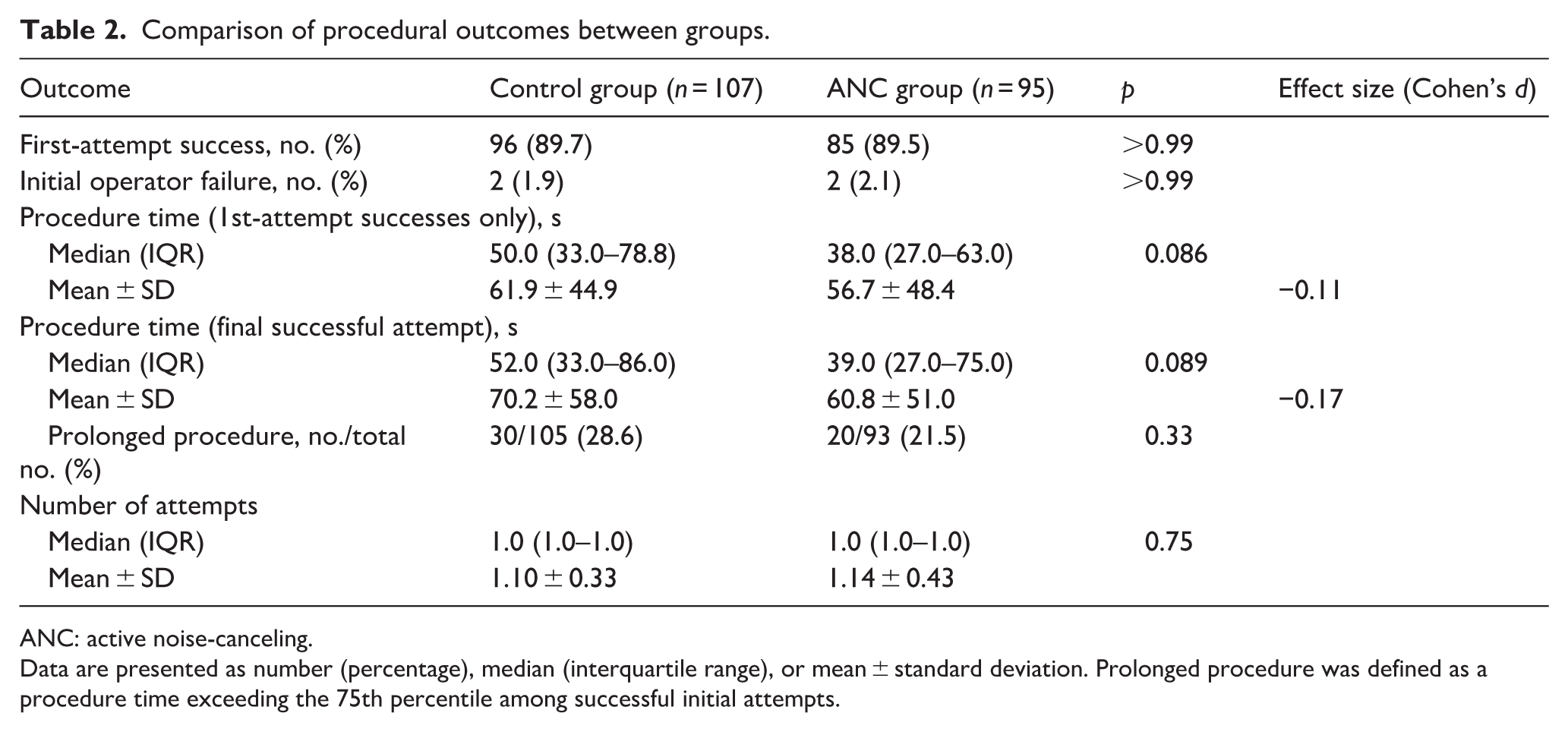
ANC: active noise-canceling.
Data are presented as number (percentage), median (interquartile range), or mean ± standard deviation. Prolonged procedure was defined as a procedure time exceeding the 75th percentile among successful initial attempts.
Regarding secondary outcomes, the median procedure time for the final cannulation attempt among cases with successful cannulation by the initial operator was numerically shorter in the ANC group (39.0 s, IQR 27.0–75.0) than in the control group (52.0 s, IQR 33.0–86.0). The corresponding means were 60.8 ± 51.0 versus 70.2 ± 58.0 s, with a Mann–Whitney U test p value of 0.089 and a small effect size (Cohen’s d = −0.17). In an analysis restricted to first-attempt successes, procedure times again tended to be shorter in the ANC group (median 38.0 vs 50.0 s; mean 56.7 ± 48.4 vs 61.9 ± 44.9 s), although the difference did not reach statistical significance (Mann–Whitney U test p = 0.086; Cohen’s d = −0.11).
The proportion of prolonged procedures, defined as procedure time above the 75th percentile among successful initial attempts, was 21.5% (20/93) in the ANC group and 28.6% (30/105) in the control group (p = 0.328).
Multivariable linear regression for log-transformed procedure time showed that ANC use was not independently associated with shorter cannulation time (β = −0.07; 95% CI −0.23 to 0.09; p = 0.39), whereas older age, lower acuity (i.e. a higher KTAS level), visible veins, fewer attempts, and greater pediatric experience of the operator were significantly associated with shorter procedure time (Table 3). In the corresponding logistic regression model, ANC use was not significantly associated with prolonged procedure (OR 0.80; 95% CI 0.36–1.76; p = 0.58), whereas multiple attempts (OR 4.19; 95% CI 1.18–14.85; p = 0.027) were associated with a higher odds of prolonged cannulation, and visible veins and greater operator pediatric experience were associated with a lower odds of prolonged cannulation.
Multivariable analysis of factors associated with procedure time and prolonged procedures.
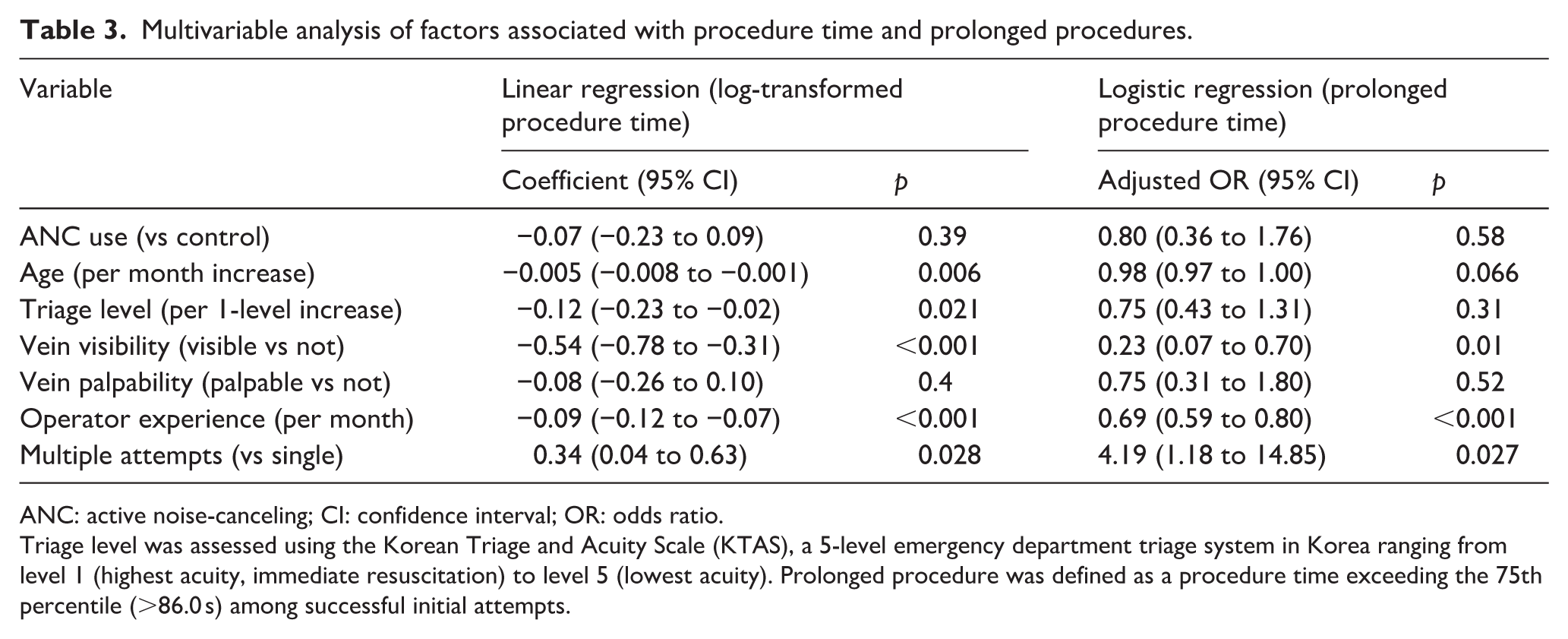
ANC: active noise-canceling; CI: confidence interval; OR: odds ratio.
Triage level was assessed using the Korean Triage and Acuity Scale (KTAS), a 5-level emergency department triage system in Korea ranging from level 1 (highest acuity, immediate resuscitation) to level 5 (lowest acuity). Prolonged procedure was defined as a procedure time exceeding the 75th percentile (>86.0 s) among successful initial attempts.
Additional exploratory analyses did not demonstrate a clear interaction between ANC use and difficult IV status, operator experience, or number of attempts (Table 4). Among children with difficult veins, ANC use was associated with a numerically shorter mean procedure time (90.9 ± 81.5 vs 124.0 ± 89.9 s; Cohen’s d = −0.39), but this difference was not statistically significant (p = 0.109). Similarly, tertile-stratified analyses by operator pediatric experience and attempt-stratified analyses (first vs multiple attempts) showed no statistically significant ANC effect, although effect sizes suggested a potentially larger time reduction in the small subgroup requiring multiple attempts (Cohen’s d = −0.66, n = 17). This exploratory subgroup finding should be interpreted cautiously given the small sample size.
Subgroup analysis of procedure time according to clinical difficulty and operator experience.
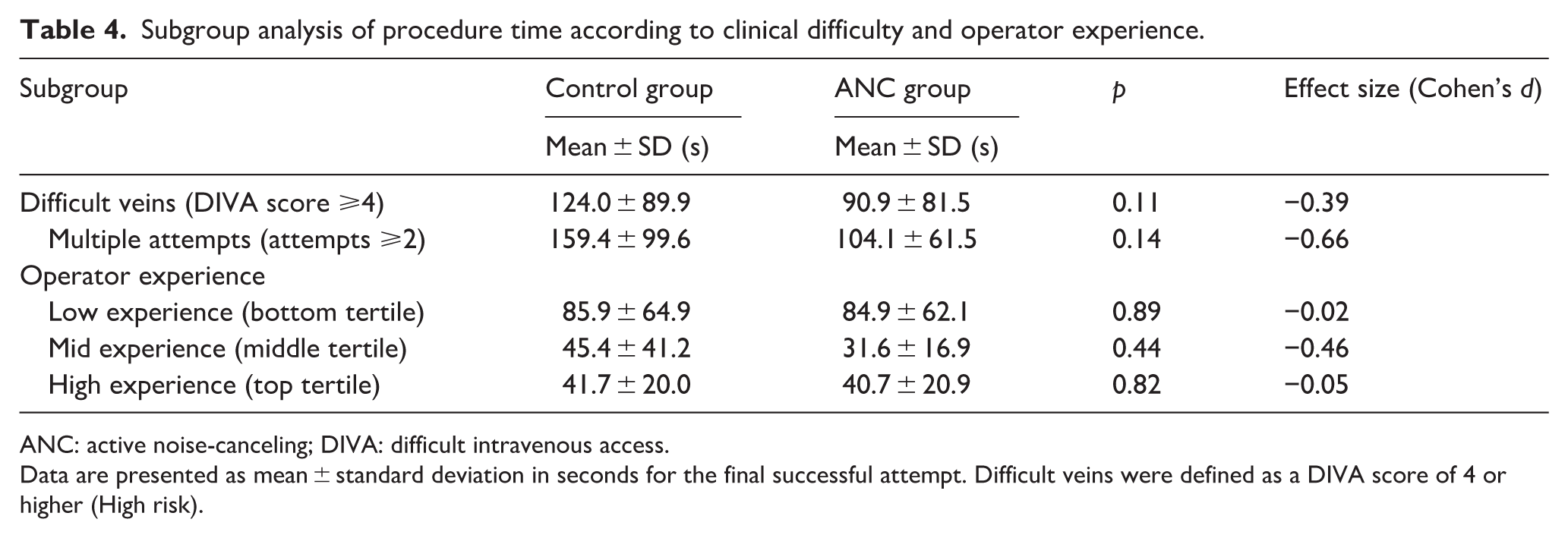
ANC: active noise-canceling; DIVA: difficult intravenous access.
Data are presented as mean ± standard deviation in seconds for the final successful attempt. Difficult veins were defined as a DIVA score of 4 or higher (High risk).
Discussion
In this randomized controlled trial conducted in a pediatric emergency department, we evaluated the effect of ANC earphones on operator performance. While the primary outcome of first-attempt success rate was comparable between groups (89.5% vs 89.7%), procedure time was shorter in the ANC group (median 39.0 vs 52.0 s). However, this between-group difference did not reach statistical significance (p = 0.089) and should be interpreted cautiously. Taken together, our findings suggest a possible signal of reduced procedure time with ANC in this setting, which warrants confirmation in adequately powered studies.
The lack of a statistically significant difference in the primary outcome might be interpreted through two potential factors. First, a strong ceiling effect likely limited detection of an intervention effect, as baseline first-attempt success at our institution was already exceptionally high, approaching 90% and exceeding rates commonly reported in pediatric studies.1,16–19 When baseline performance is already near-optimal, it is plausible that environmental interventions may have a limited margin to demonstrate further incremental gains in binary outcomes. Second, the characteristics of the acoustic environment in our study setting may differ from those in previous research.9,11,20 Unlike prior studies that primarily established the detrimental impact of continuous background noise in operating rooms, the auditory distractions in a pediatric emergency department are likely more intermittent and unpredictable. It is possible that this distinct noise profile may have attenuated the potential benefits of noise cancellation on routine procedural success.
Despite the absence of a difference in success rates, the observed trend toward reduced procedure time prompted a multivariable analysis to identify independent determinants of efficiency. Our regression models revealed that vein visibility, operator experience, and the number of attempts were significantly associated with procedure time. These findings align well with established predictors of difficult intravenous access.2–4,21,22 Specifically, the identification of non-visible veins as a delay factor is consistent with the variables emphasized in the modified DIVA score—such as the Spanish validation model excluding prematurity 4 —which prioritizes vein visibility and palpability. Similarly, the association between greater operator experience and shorter procedure time corroborates prior pediatric literature showing that outcomes improve with greater procedural expertise, including reports from vascular access specialist teams and studies of ultrasound-guided PIVC insertion, particularly in children with difficult access.23–25 Given that the effects of environmental noise on performance vary by task demands and cognitive workload, it is plausible that ANC could have a greater impact among less experienced operators who may have less automaticity and reserve capacity during demanding procedures. However, this hypothesis was not directly tested in our study and should be evaluated in adequately powered future work. In addition, multiple attempts were strongly associated with prolonged procedure times, reflecting the inherent difficulty and complexity of cases requiring re-insertion.
To further investigate the potential utility of ANC, we conducted a stratified analysis based on difficulty factors. Although statistical significance was not reached for interaction terms, a distinct trend was observed in the subgroup requiring multiple attempts, where the ANC group showed a substantial reduction in procedure time (Cohen’s d = −0.66). While this observation warrants cautious interpretation due to the limited sample size, it aligns with the theoretical framework of cognitive resource management. Cognitive aids are posited to yield maximal benefit during deviations from expected clinical pathways rather than during routine procedures.26,27 For an experienced operator, the initial attempt represents a standard task; however, a subsequent failure shifts the clinical context into a high-acuity scenario. This phase is frequently compounded by escalating environmental stressors, such as the patient’s distress and parental anxiety. In this setting, ANC may serve to mitigate extraneous cognitive load, thereby assisting the operator in maintaining attentional focus and executing the subsequent procedure with greater efficiency.
These results highlight the potential of ANC as a practical and accessible adjunctive tool in the pediatric emergency setting. While established techniques such as ultrasound-guided insertion have demonstrated clear benefits in improving vascular access outcomes,7,28 their implementation requires substantial capital investment and specialized training. In contrast, ANC leverages widely available consumer-grade technology and may be readily deployed as a supportive measure, particularly in situations where environmental or psychological stressors challenge operator performance. The integration of ANC into clinical practice, however, requires careful consideration of patient safety. Future clinical protocols may incorporate ambient sound pass-through features inherent in modern devices or establish standardized visual communication signals, ensuring that patient safety is maintained while preserving the cognitive benefits of noise reduction.
This study has several methodological and clinical strengths. Primarily, to the best of our knowledge, it represents the first randomized controlled trial to investigate the impact of wearable noise control technology in a real-world pediatric emergency department, moving beyond the limitations of previous simulation-based research. Second, we emphasized objective quantitative outcomes—specifically precise procedural timing and technical success—rather than relying solely on subjective self-reports of stress or distraction. Finally, the internal validity of our analysis was bolstered by rigorous adjustment for critical confounders, including the modified DIVA profile (vein visibility and palpability) and operator experience. This comprehensive approach allows for a more nuanced interpretation of how environmental factors interact with clinical difficulty.
However, several limitations must be acknowledged. First, although our sample size was calculated a priori based on standard assumptions, the exceptionally high baseline proficiency of our specialized team resulted in a distinct ceiling effect. Detecting a statistically significant improvement beyond this already elevated threshold would require a prohibitively large sample size, presenting a practical constraint within a single-center context. Consequently, the study may have been underpowered to detect subtle differences in secondary outcomes or within specific subgroups. Second, the visible nature of the intervention precluded operator blinding, which may have introduced potential performance bias due to the operators’ awareness of the intervention. Third, ambient noise levels were not objectively quantified, nor were subjective measures of operator stress or cognitive load assessed, limiting our ability to directly examine the proposed psychological mechanisms underlying the intervention’s effects. Accordingly, future multicenter studies involving diverse clinical environments and operators with varying levels of experience are warranted to further evaluate the generalizability of these findings.
In conclusion, while the use of active noise-canceling earphones by highly skilled operators did not significantly elevate the already high first-attempt success rate, likely due to a ceiling effect, our findings suggest a possible signal of improved procedural efficiency. Although secondary time outcomes were not statistically significant, exploratory analyses suggested that any time-related effects may be more apparent in more complex scenarios necessitating multiple attempts, where maintaining focus is paramount; however, these observations should be interpreted cautiously given the small subgroup size and limited power. Collectively, these results indicate that active noise control may serve as a feasible and low-cost adjunct to support operator focus during demanding clinical workflows, warranting confirmation in adequately powered, multicenter studies. By introducing a novel environmental modification to the pediatric emergency setting, this study provides a foundation for future research targeting higher-risk populations or less experienced clinicians, where the potential benefits of auditory optimization merit further evaluation.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261429330 – Supplemental material for Effect of active noise cancellation on pediatric peripheral intravenous catheter insertion: A randomized controlled trial
Supplemental material, sj-docx-1-jva-10.1177_11297298261429330 for Effect of active noise cancellation on pediatric peripheral intravenous catheter insertion: A randomized controlled trial by Eui Jun Lee, Jin Hee Kim, Jae Yun Jung, Jiwon Seo, Young Ho Kwak, Do Kyun Kim and Joong Wan Park in The Journal of Vascular Access
Footnotes
Acknowledgements
We thank the members of the Vascular Access Team (Emergency Medical Technicians) for their willing participation as operators in this study and for their assistance with data collection.
Abbreviations
The following abbreviations are used in this manuscript:
ANC: Active Noise-Canceling
PIVC: Peripheral Intravenous Catheter
KTAS: Korean Triage and Acuity Scale
DIVA: Difficult Intravenous Access
Author contributions
Conceptualization, E.J.L., J.H.K., and J.Y.J.; methodology, E.J.L., J.H.K., and J.Y.J.; formal analysis, E.J.L. and J.H.K.; investigation, E.J.L., J.H.K., and J.S.; data curation, E.J.L. and J.H.K.; writing—original draft preparation, E.J.L. and J.H.K.; writing—review and editing, J.Y.J., Y.H.K., D.K.K., and J.W.P.; supervision, J.Y.J.; project administration, J.Y.J. All authors have read and agreed to the published version of the manuscript.
Data availability statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Seoul National University Hospital (grant no. 04-2021-0770). The sponsors were not involved in the study design; data collection, analysis, or interpretation; writing of the manuscript; or the decision to submit the manuscript for publication.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. 2203-161-1310; approval date: May 25, 2022).
Informed consent
Informed consent to participate was obtained from the legal guardians of all pediatric participants prior to enrollment. Participating operators also provided informed consent to take part in the study.
Additional identifying information
Trial registration: cris.nih.go.kr (KCT0008116). Reporting guideline: CONSORT statement.
Trial registration
This study was registered under the Clinical Trials protocol registration system (KCT0008116).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.