
Abstract
Background:
Radiocephalic arteriovenous fistulas (RCAVFs) are the preferred initial haemodialysis access but are limited by high non-maturation rates, particularly in populations with smaller vessels and high diabetic burden. Preoperative duplex ultrasound (DUS) guides vessel selection but inconsistently predicts postoperative haemodynamic adaptation. We evaluated whether a standardised 2-week postoperative DUS checkpoint could function as a clinical workflow tool for early risk stratification and long-term patency prediction.
Methods:
In this prospective single-centre study, 57 patients undergoing primary RCAVF creation were followed for up to 10 years. Two-week postoperative DUS assessed vein diameter (VD), brachial artery flow (BAF) and resistive index (RI). Receiver operating characteristic analysis identified thresholds predicting 6-week Kidney-Disease-Outcomes-Quality-Initiative-defined maturation. Kaplan–Meier and Cox regression analyses evaluated long-term primary (PP) and secondary patency (SP).
Results:
Six-week maturation occurred in 56%, and functional maturation in 61% of patients initiated on dialysis. Two-week VD demonstrated the strongest discrimination for maturation (AUC 0.81, 95% CI 0.50–0.84, p = 0.01), followed by BAF (AUC 0.72, 95% CI 0.65–0.90, p = 0.02). RI showed weaker performance (AUC 0.67, 95% CI 0.50–0.83, p = 0.05). A VD <5 mm independently predicted long-term PP loss up to 10 years (HR 2.43, 95% CI 1.21–4.86, p = 0.01). BAF predicted early maturation but not long-term PP and SP. Early vein and flow expansion kinetics were not independently associated with long-term outcomes.
Conclusions:
A 2-week postoperative DUS checkpoint provides actionable early structural risk stratification after RCAVF creation. Early structural calibre reflects adaptive remodelling and independently predicts long-term PP, supporting integration of this checkpoint into routine practice.
Keywords
Introduction
Arteriovenous fistulas (AVFs) remain the preferred vascular access for patients requiring long-term haemodialysis because of superior longevity and lower infection and thrombosis rates compared with arteriovenous grafts (AVGs) and catheters.1,2 Radiocephalic AVFs (RCAVFs) are prioritised over brachiocephalic (BAVFs) and brachiobasilic (BBAVFs) AVFs by contemporary guidelines as their distal location preserves proximal venous capital and reduces ischaemic complications.2–5 However, RCAVFs are associated with higher non-maturation and reintervention rates, frequently due to juxta-anastomotic stenosis (JAS) and limited venous remodelling capacity.3,6,7
These challenges are particularly relevant in Asian populations, where smaller baseline vessel calibre and high diabetic burden are prevalent. 8 Preoperative duplex ultrasound (DUS) mapping is guideline-recommended to ensure anatomical suitability.2,5 Nevertheless, adequate preoperative vessel diameter does not reliably predict early postoperative adaptation, as successful maturation depends on dynamic haemodynamic and structural remodelling after arterialisation.9,10
This creates a surveillance gap in the immediate postoperative period, when remodelling trajectories are established but clinical failure is not yet apparent. Early postoperative DUS may therefore provide incremental prognostic value beyond anatomical selection by capturing functional adaptation of the newly created AVF. Previous studies have suggested potential predictive value of early postoperative flow measurements.11,12 However, their generalisability was constrained by short-term follow-up and non-standardised outcome definitions.
We therefore evaluated whether a standardised 2-week postoperative DUS checkpoint could serve as a clinically actionable workflow tool by determining whether early structural and haemodynamic parameters in the form of vein diameter (VD), brachial artery flow (BAF) and resistive index (RI) predict 6-week Kidney Disease Outcomes Quality Initiative (KDOQI)-defined maturation and stratify long-term primary patency (PP) and secondary patency (SP) up to 10 years in a multi-ethnic Asian RCAVF cohort.
Methods
Study design and patient population
This prospective single-centre study included consecutive patients undergoing primary RCAVF creation by a single vascular surgeon (CRL) under brachial plexus block between October 2013 and October 2014. Both pre-dialysis and maintenance haemodialysis patients were eligible. Inclusion required primary RCAVF creation with longitudinal follow-up extending up to 10 years.
Patients younger than 21 or older than 80 years, those undergoing BCAVF, BBAVF, AVG or secondary VA creation or VA creation performed under general or local anaesthesia were excluded. All patients underwent preoperative duplex vessel mapping. Radial arteries were selected only if internal diameter measured ≥2 mm without significant calcification. The protocols and procedures with regards to AVF creation and postoperative surveillance have been described in our previous work. 13
The study was approved by the Institutional Review Board of the National Healthcare Group. Written informed consent was obtained from all participants.
DUS measurements
DUS assessment was performed at 2 weeks postoperatively using a 10-MHz linear probe (GE Logic R7, GE Medical Systems). All measurements were obtained by a single experienced operator (CJR) to minimise interobserver variability.
VD was measured 5 cm downstream from the wrist joint within the forearm cannulation segment. BAF was measured at the mid-upper arm level with the patient sitting in an upright position, with arm horizontal and abducted at 45°. Resistive index (RI) was automatically calculated by the ultrasound scanner using the standard equation: RI = ([peak systolic velocity-end diastolic velocity]/peak systolic velocity). VD and BAF absolute (static) expansion and daily expansion rate at 2-week postoperative cut-off were also calculated relative to preoperative baseline measurements. Each measurement was repeated three times and averaged for analysis.
Outcomes
The primary outcome was 6-week AVF maturation defined according to KDOQI ‘rule of 6’ criteria: BAF ≥600 mL/min, VD ≥6 mm and vein depth <6 mm at 6 weeks postoperatively. 2 AVFs were considered mature if they met these haemodynamic criteria irrespective of cannulation attempts, given inclusion of pre-dialysis patients.
Functional maturation was defined as successful two-needle AVF cannulation within 3 months of access creation among patients initiated on haemodialysis.
Secondary outcomes included PP and SP at 2, 5 and 10 years, intervention rate per access-year calculated from time of creation, early stenotic lesion characteristics within 3 months of AVF creation based on DUS surveillance findings, and causes of access abandonment.
PP was defined as the interval from access creation to first intervention to maintain or restore patency, access thrombosis or access abandonment. SP was defined as the interval from access creation to final access abandonment, including reinterventions performed after thrombosis.
Key VA terms, including maturation, PP and SP, lesion classification and intervention metrics, were defined using standardised terminology adapted from established definitions and are shown in Supplemental Table 1.4,14 These definitions are consistent with current clinical practice recommendations.2,5
Statistical analysis
All statistical analyses were performed using SPSS version 29 (IBM Corp., Chicago, IL). Continuous variables are presented as median with interquartile range (IQR) and categorical variables as frequencies and percentages.
Receiver operating characteristic (ROC) curves were constructed to evaluate the predictive performance of 2-week VD, BAF and RI on 6-week KDOQI maturation. Optimal cut-off values were determined using Youden’s index. Area under the curve (AUC), sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and overall accuracy were calculated for those three parameters. An AUC >0.7 was considered clinically meaningful in accordance with established diagnostic performance methodology. 15 Static expansion and rate-of-expansion variables were analysed similarly.
Long-term PP and SP were estimated using Kaplan–Meier survival analysis, stratified by optimal 2-week VD and BAF cut-offs identified from ROC analysis. Survival analysis was not performed for RI as prior work has suggested that its prognostic value is primarily confined to immediate postoperative period during which vasospasm is more likely to influence short-term outcomes, with limited evidence supporting long-term prognostic relevance. 16 Number-at-risk tables were displayed beneath each curve.
Univariate Cox proportional hazards regression was performed to identify predictors of PP loss. Variables assessed included age, DM, smoking status, PAD, 2-week VD, RI, and VD and BAF static and rate of expansion. Variables with p < 0.10 on univariate analysis were entered into multivariable Cox regression to determine independent predictors of PP loss.
SP was not modelled as a dependent variable, as it incorporates post-baseline reinterventions and may thus introduce treatment-related confounding.
Intervention rates were calculated as the total number of access-related endovascular or surgical procedures divided by cumulative access-years of follow-up, expressed as interventions per access-year (Supplemental Table 1). Follow-up time was defined from access creation to thrombosis, abandonment, death, transplantation, conversion to peritoneal dialysis or study end.
Results
Fifty-seven patients underwent primary RCAVF creation. Demographic and baseline clinical characteristics are summarised in Table 1. The median age was 58 years (IQR 52–65), 68% were male, and 74% had DM. PAD was present in 11%. Sixteen patients (28%) were pre-dialysis at the time of access creation.
Patients’ baseline characteristics.
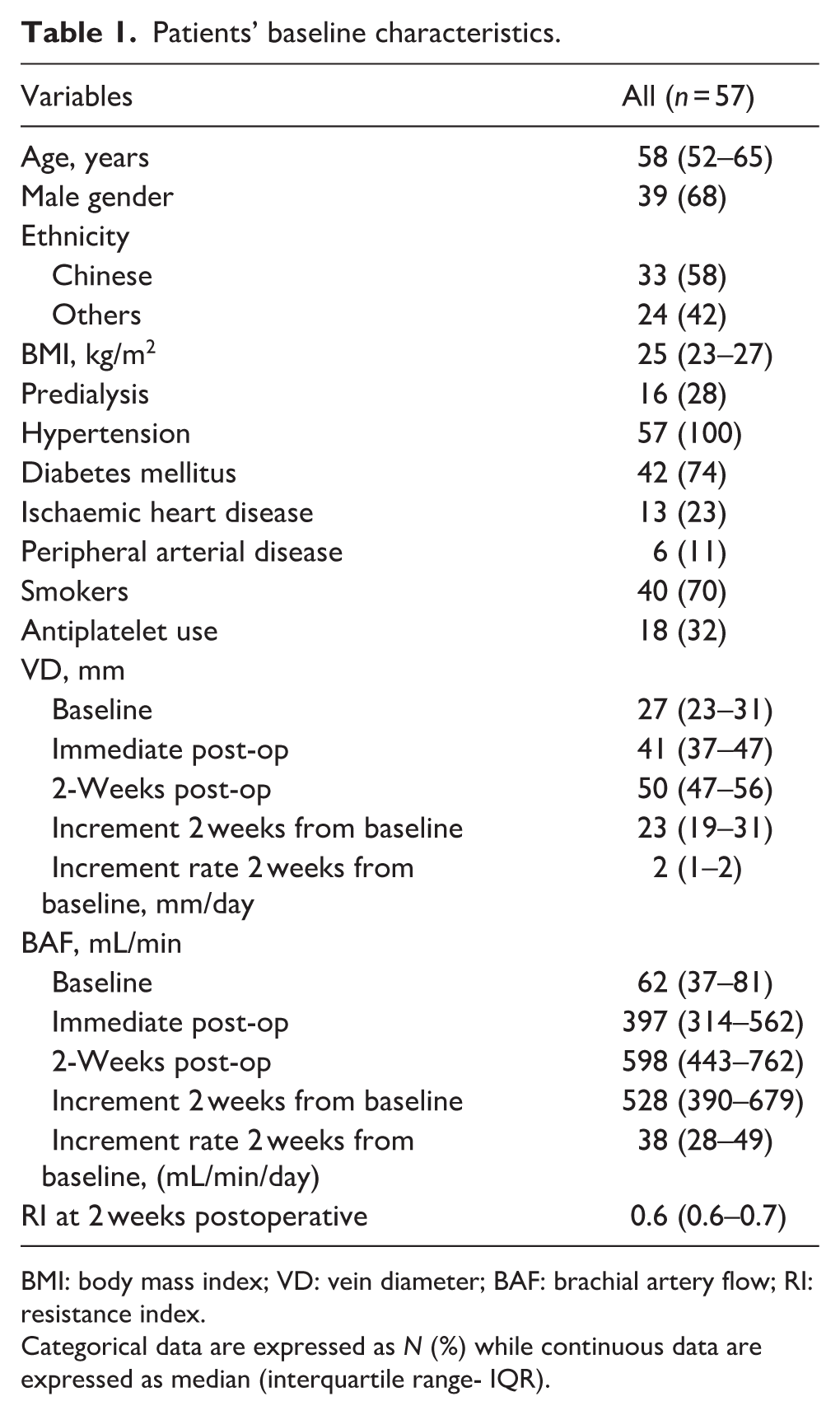
BMI: body mass index; VD: vein diameter; BAF: brachial artery flow; RI: resistance index.
Categorical data are expressed as N (%) while continuous data are expressed as median (interquartile range- IQR).
At 2 weeks postoperatively, median VD was 5.0 mm (IQR 4.7–5.6), BAF 598 mL/min (IQR 443–762) and RI 0.6 (IQR 0.6–0.7). The median VD expansion was 2.3 mm (IQR 1.9–3.1), corresponding to a median expansion rate of 0.2 mm/day (IQR 0.1–0.2). Median BAF expansion was 528 mL/min (IQR 390–679), with a median expansion rate of 38 mL/min/day (IQR 28–49).
Six-week maturation based on KDOQI criteria occurred in 56% of AVFs. Among the 72% of patients who commenced haemodialysis, functional maturation was achieved in 61%.
Superimposed ROC curves for VD, BAF and RI are shown in Figure 1. Two-week VD demonstrated the strongest discrimination for 6-week maturation (AUC 0.81, 95% confidence interval (CI) 0.50–0.84, p = 0.01). Best VD cut-off was found to be ≥5 mm, giving a sensitivity of 82%, specificity 50%, PPV 65%, NPV 72% and overall accuracy 68%. BAF showed acceptable predictive performance (AUC 0.72, 95% CI 0.65–0.90, p = 0.02). At ≥500 mL/min best threshold, sensitivity was 85%, specificity 68%, PPV 77%, NPV 78% and accuracy 77%. RI demonstrated limited standalone predictive utility (AUC 0.67, 95% CI 0.50–0.83, p = 0.05), with lower overall performance compared with VD and BAF. Predictability data for expansion parameters are summarised in Supplemental Table 2. Their AUC all fall <0.7, suggesting that they are insufficient for clinical decision making on their own.
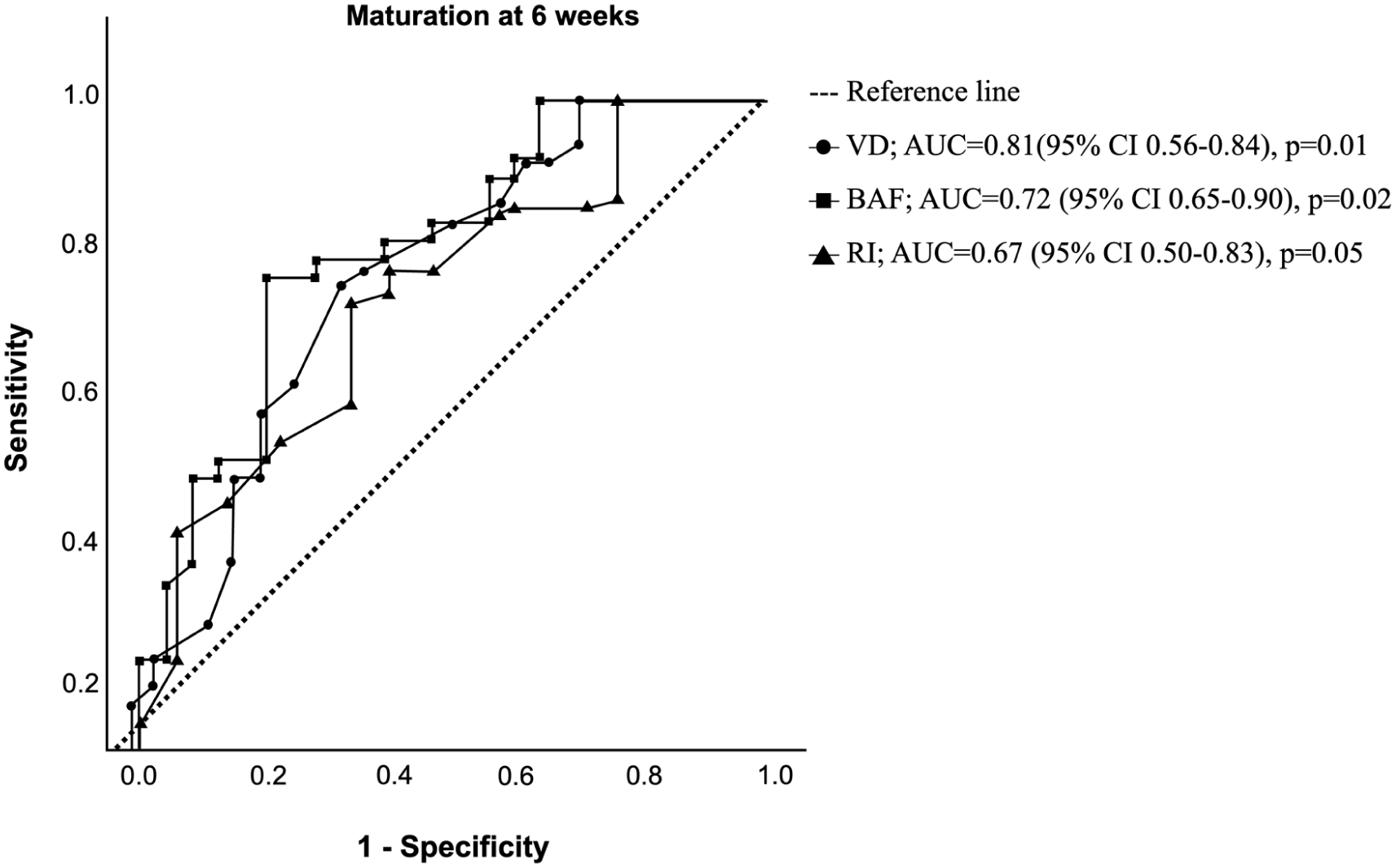
Receiver operating characteristic curves for prediction of arteriovenous fistula maturation at 6 weeks based on vein diameter (VD), brachial artery flow (BAF) and resistive index (RI) measured at 2 weeks.
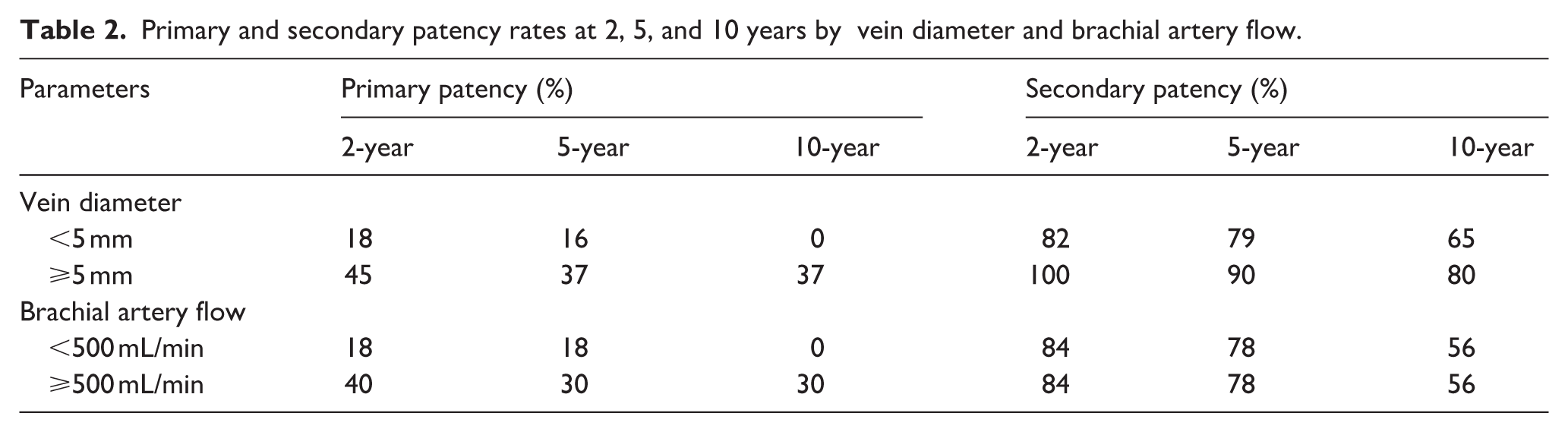
Over a median follow-up of 5.04 years, Kaplan–Meier analysis demonstrated significantly superior PP in RCAVFs with VD ≥5 mm compared with <5 mm (log-rank p = 0.001; Figure 2; Table 2). Two-, five- and ten-year PP rates were 45%, 37% and 37% for VD ≥5 mm versus 18%, 16% and 0% for VD <5 mm, respectively. However, SP did not differ significantly between VD strata. Similarly, BAF ≥500 mL/min did not significantly impact on long-term PP or SP (Figure 3; Table 2). It should be cautioned, nonetheless that survival estimates at later time points should be interpreted with caution given diminishing numbers at risk and increasing standard error.
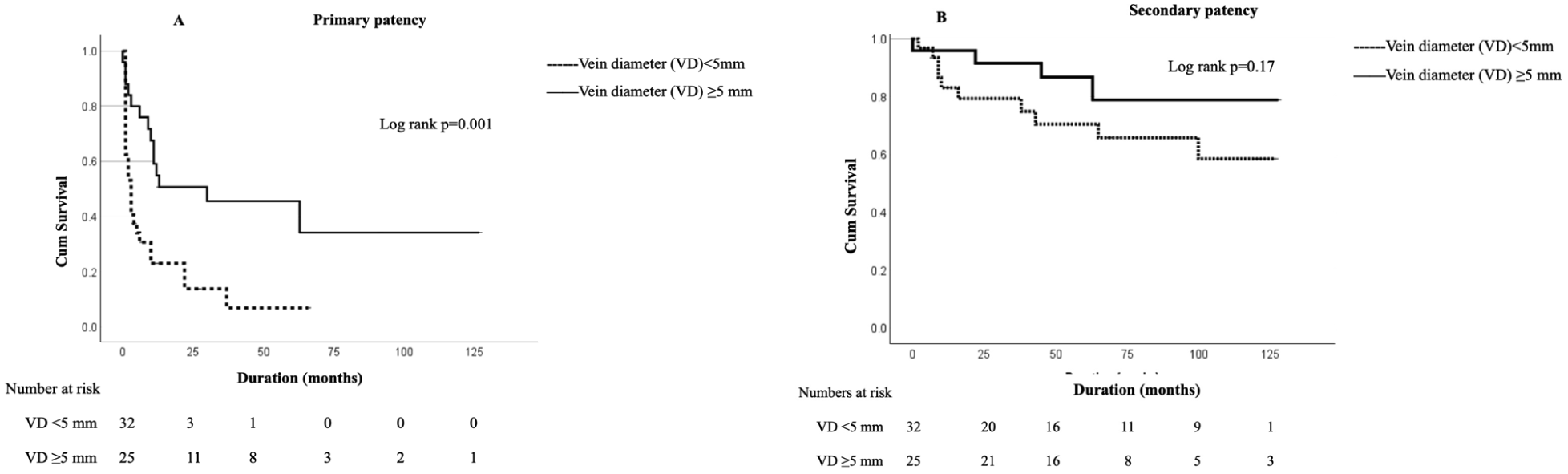
Kaplan–Meier survival curves comparing radiocephalic arteriovenous fistula primary patency (a) and secondary patency (b) stratified by vein diameter ≤5 mm versus >5 mm.
Primary and secondary patency rates at 2, 5, and 10 years by vein diameter and brachial artery flow.
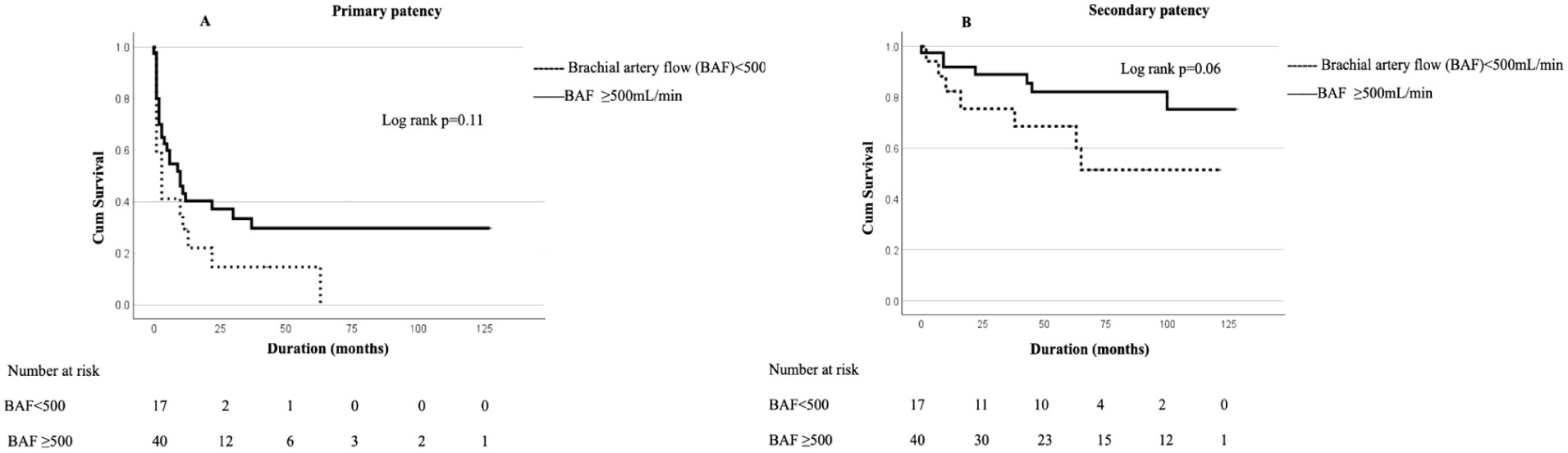
Kaplan–Meier survival curves showing primary patency (a) and secondary patency (b) of radiocephalic arteriovenous fistulas stratified by brachial artery flow.
On univariate Cox regression, PAD (HR 4.93, 95% CI 1.82–13.33, p < 0.01) and 2-week VD <5 mm (HR 2.73, 95% CI 1.39–5.31, p < 0.01) were associated with loss of PP (Table 3). Both remained independently predictive on multivariable analysis (PAD HR 3.52, 95% CI 1.28–9.69, p = 0.02; VD <5 mm HR 2.43, 95% CI 1.21–4.86, p = 0.01). However, RI and BAF static and rate of expansion, were not independently associated with PP loss after adjustment (Table 3).
Unadjusted (univariate) and adjusted (multivariate) Cox regression analysis showing variables affecting the loss of primary patency.
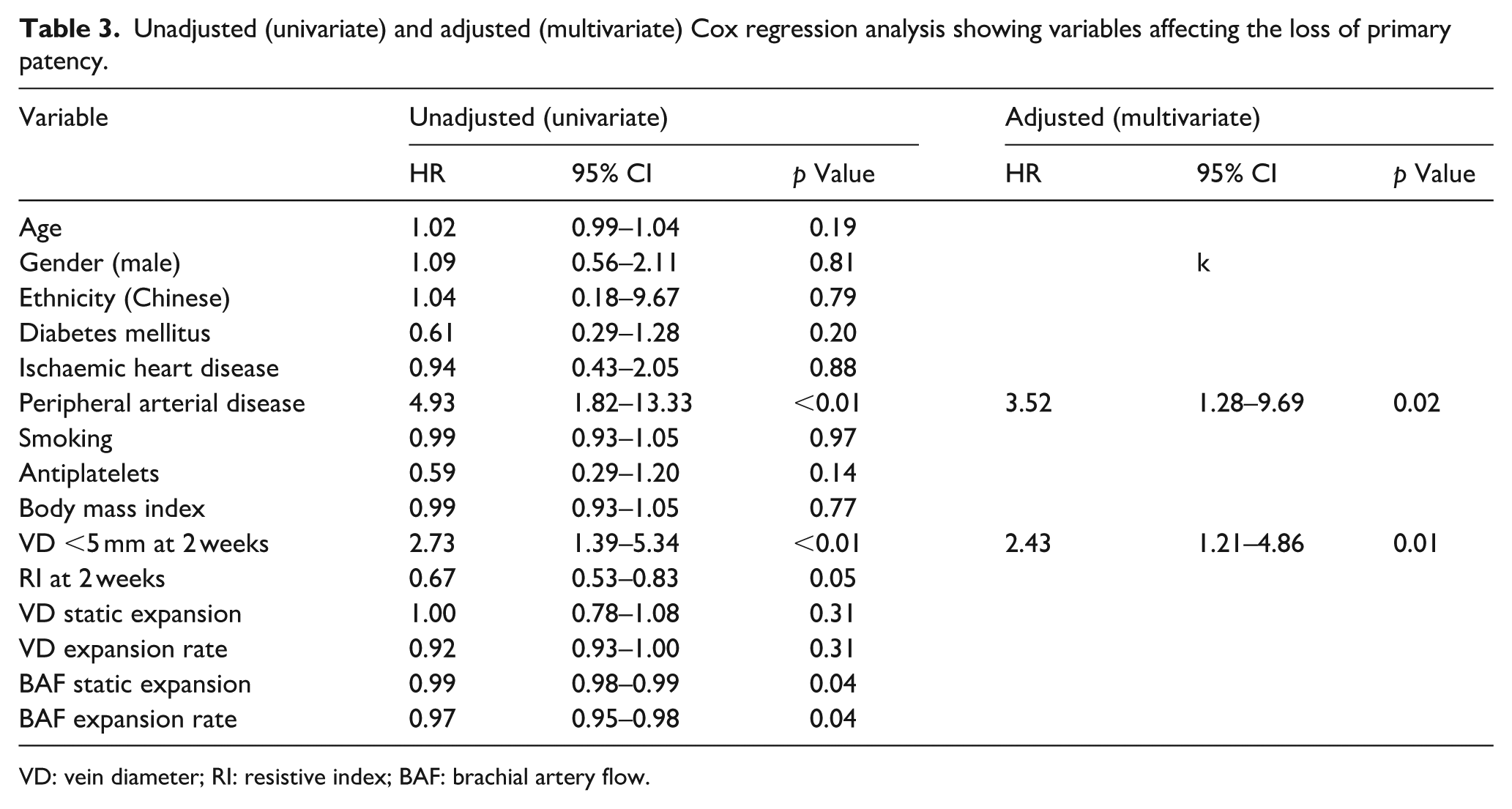
VD: vein diameter; RI: resistive index; BAF: brachial artery flow.
Intervention burden was greater in RCAVFs with VD <5 mm (Supplemental Table 3). Intervention rate per access-year was 0.82 in VD <5 mm compared with 0.34 in VD ≥5 mm (p = 0.01). Balloon-assisted maturation (BAM) was performed in 44% versus 19%, respectively. Thrombectomy occurred in 40% versus 9%. Collateral or accessory vein coiling was rare, being performed in only one case with VD ≥5 mm.
Stenotic lesion distribution within 3 months is summarised in Supplemental Table 4. Inflow and juxta-anastomotic stenoses were more frequent in the VD <5 mm group (56% vs 25%), whereas outflow stenosis rates were comparable.
The most common cause of RCAVF abandonment was death with a functioning AVF, occurring in 44% of VD <5 mm and 47% of VD ≥5 mm cases, with no significant difference between strata (Supplemental Table 5). No patient was lost to follow-up.
Discussion
In this prospective study of primary RCAVFs, 2-week postoperative VD emerged as a durable structural marker of access trajectory. While BAF predicted 6-week maturation, only VD ≥5 mm independently predicted long-term PP up to 10 years. RI and early expansion kinetics were not independently associated with durable outcomes. These findings reinforce the concept that early structural consolidation rather than isolated haemodynamic signals determines long-term RCAVF behaviour.
The early postoperative period represents a critical biological window characterised by endothelial recovery, inflammatory modulation and outward venous remodelling in response to increased shear stress. Experimental and translational data demonstrate that sustained luminal expansion reflects adaptive remodelling, whereas failure of outward remodelling predisposes to neointimal hyperplasia (NIH) and JAS.10,17–21 Our findings extend this paradigm by showing that absolute structural calibre at 2 weeks rather than expansion rate most reliably reflects whether adaptive remodelling has stabilised or diverged towards maladaptive change.
The prognostic relevance of early postoperative calibre assessment has also been observed in Asian cohorts, where smaller baseline vessels and higher diabetic burden are prevalent.22,23 Collectively, these data suggest that remodelling capacity, rather than baseline anatomy alone, governs long-term patency in such populations.
From a temporal perspective, early flow-based studies likely reflect transient hyperaemic responses immediately following anastomosis rather than stabilised structural remodelling. Indeed, Ladenheim et al. demonstrated that first-week flow strongly predicts early PP, while Inagaki et al. showed that early postoperative RI identifies short-term failure risk.12,16 In contrast, Hou et al. reported that 2-week duplex parameters predicted maturation in a Chinese RCAVF cohort, suggesting that this time point captures a more consolidated phase of venous remodelling. 11 Our findings thus extend this temporal framework by demonstrating that AVF trajectory reflects the interaction between baseline anatomical suitability and the capacity for adaptive haemodynamic and structural remodelling following arterialisation, a concept supported by several clinical and translational studies.9,22-25.
Importantly, our findings complement rather than replace evidence-based preoperative DUS mapping recommendations.2,5 More so, the fact that 2-week VD predicted PP but not SP is consistent with remodelling biology, as SP reflects post-baseline reinterventions rather than intrinsic structural durability, as previously described by Pirozzi et al. 26
From a clinical perspective, a routine 2-week DUS checkpoint allows early identification of suboptimal venous remodelling during a potentially modifiable window. A VD <5 mm signalled increased susceptibility to JAS, higher intervention burden and greater reliance on BAM. The higher frequency of BAM in this group suggests that early structural limitation, rather than accessory vein diversion, was the dominant mechanism of failure, consistent with existing literature on the roles of BAM and accessory veins in AVF maturation.27,28
Finally, 2-week structural calibre offers a practical and reproducible metric for integration into predictive models. Incorporating early postoperative DUS data into machine-learning frameworks, an approach piloted by Fitzgibbon et al. may enable more personalised and strategically timed vascular access care. 29
Our study, however, has several limitations. The modest sample size limits statistical power and precision of survival estimates at extended follow-up. In later phases of the Kaplan–Meier analyses, the number at risk fell below 10 in some strata and the standard error of the survival estimate exceeded 10% at selected time points. As noted by Pocock et al., survival curves with diminishing risk sets may appear visually separated despite increasing statistical imprecision. 30 Therefore, late follow-up estimates were interpreted cautiously. These features reduce precision but do not invalidate consistent early and mid-term trends.
As an observational study, causal inference cannot be established. Assisted primary patency (APP) was not formally analysed; while its inclusion may have provided additional insight into pre-emptively treated AVFs, the absence of significant differences in SP suggests this omission is unlikely to have materially altered conclusions regarding intrinsic durability.
In addition, although some contemporary literature has advocated a more permissive ‘rule of 5’ threshold, we retained the KDOQI rule-of-6 criteria to preserve methodological consistency and comparability with established maturation studies. The use of stricter haemodynamic thresholds may therefore have overestimated non-maturation relative to functional cannulation success, which likely explains the discrepancy between the two in our cohort. Nonetheless, adherence to KDOQI definitions strengthens interpretability across studies.
Finally, the impact of early interventions triggered by duplex findings was not formally evaluated, and advanced mechanistic imaging of NIH or direct shear stress quantification was not performed.
Conclusion
Two-week postoperative DUS functions as a practical clinical workflow tool following RCAVF creation. A VD ≥5 mm at 2 weeks independently predicted durable PP up to 10 years, underscoring early structural consolidation as the principal determinant of long-term access trajectory. Incorporating a standardised 2-week surveillance checkpoint into routine practice provides a clear and actionable opportunity during the critical remodelling phase.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261443162 – Supplemental material for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas
Supplemental material, sj-docx-1-jva-10.1177_11297298261443162 for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas by Claude Jeffrey Renaud, Allen Yan Lun Liu, Clarice Chua Kah Hwei, Tan Khin Swee Elisabeth, Abdul Haque bin Abdul Jabbar, Lee Wei Han and Chuo Ren Leong in The Journal of Vascular Access
Supplemental Material
sj-docx-2-jva-10.1177_11297298261443162 – Supplemental material for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas
Supplemental material, sj-docx-2-jva-10.1177_11297298261443162 for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas by Claude Jeffrey Renaud, Allen Yan Lun Liu, Clarice Chua Kah Hwei, Tan Khin Swee Elisabeth, Abdul Haque bin Abdul Jabbar, Lee Wei Han and Chuo Ren Leong in The Journal of Vascular Access
Supplemental Material
sj-docx-3-jva-10.1177_11297298261443162 – Supplemental material for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas
Supplemental material, sj-docx-3-jva-10.1177_11297298261443162 for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas by Claude Jeffrey Renaud, Allen Yan Lun Liu, Clarice Chua Kah Hwei, Tan Khin Swee Elisabeth, Abdul Haque bin Abdul Jabbar, Lee Wei Han and Chuo Ren Leong in The Journal of Vascular Access
Supplemental Material
sj-docx-4-jva-10.1177_11297298261443162 – Supplemental material for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas
Supplemental material, sj-docx-4-jva-10.1177_11297298261443162 for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas by Claude Jeffrey Renaud, Allen Yan Lun Liu, Clarice Chua Kah Hwei, Tan Khin Swee Elisabeth, Abdul Haque bin Abdul Jabbar, Lee Wei Han and Chuo Ren Leong in The Journal of Vascular Access
Supplemental Material
sj-docx-5-jva-10.1177_11297298261443162 – Supplemental material for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas
Supplemental material, sj-docx-5-jva-10.1177_11297298261443162 for Two-week postoperative duplex ultrasound as a clinical workflow tool for risk stratification of radiocephalic arteriovenous fistulas by Claude Jeffrey Renaud, Allen Yan Lun Liu, Clarice Chua Kah Hwei, Tan Khin Swee Elisabeth, Abdul Haque bin Abdul Jabbar, Lee Wei Han and Chuo Ren Leong in The Journal of Vascular Access
Footnotes
Author contributions
Conception and design – CJR, CRL. Analysis and interpretation – AL, CJR. Data collection – CJR, CRL. Critical revision – CC, AB, WHL, TKSE. Approval of manuscript – CJR, CRL, CC, AB, WHL, TKSE. Agreement to be accountable – all authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Institutional Review Board of the National Healthcare Group.
Informed consent
Written informed consent was obtained from all participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.