
Abstract
Background:
Peripherally inserted central catheter ports (PICC-ports) combine peripheral insertion with implantable reservoirs, offering reduced invasiveness compared to chest ports. Evidence from Latin America remains limited.
Objective:
To evaluate the safety, efficacy, and device survival of PICC-ports in oncology patients at a Colombian tertiary care center.
Methods:
Retrospective cohort study of 50 consecutive adult cancer patients receiving PICC-ports (January 2023-December 2024). All procedures were performed using ultrasound guidance and intracavitary electrocardiographic navigation under local anesthesia.
Results:
Technical success: 100% (95% CI: 92.9%–100%). No early complications occurred. Late complications occurred in 4% of patients: one case of catheter-related thrombosis and one case of catheter dislodgement. Overall complication rate: 3.1 per 10,000 catheter-days (95% CI: 0.35–2.07). Median dwell time: 117 days. Catheter retention: 94.0% at 30 days, 89.2% at 90–180 days.
Conclusions:
PICC-port implementation achieved excellent safety outcomes comparable to international benchmarks, supporting its use as an alternative to chest ports in resource-constrained settings.
Keywords
Introduction
Permanent central venous access is essential for administering prolonged intravenous therapies in oncology patients.1,2 Traditional totally implantable venous access devices have been placed in the chest wall, requiring a surgical or central venous approach with associated procedural complications.3–5 Peripheral arm ports emerged as an alternative; however, they are placed without a standardized protocol, typically accessing arm veins without ultrasound guidance and without optimizing the catheter-to-vein ratio, 6 resulting in significant complication rates, including upper-extremity deep vein thrombosis in 9.5% of patients (nearly five times higher than the 2.0% observed with chest ports), overall adverse events in up to 19.2%, infections of 0.17 per 1000 catheter-days. 7
To reduce these complications, the PICC-port technique was developed as a technically distinct approach. Using ultrasound-guided micro-Seldinger access at the proximal upper arm (basilic or brachial vein), the catheter is tunneled to a subcutaneous mid-arm pocket where the port is implanted. By targeting larger-caliber proximal veins, this approach optimizes the catheter-to-vein ratio. 5 In a European multicenter study, device removal due to serious adverse events occurred in only 1.2% of cases, with catheter-related bloodstream infection in 0.42% and symptomatic thrombosis in 2.1%. 8
While European studies have characterized PICC-port outcomes, Latin American data remain scarce. We aimed to describe our institutional experience in a Colombian tertiary care center, evaluating technical efficacy, complications, device dwell time, and clinical outcomes in oncologic patients requiring long-term treatment and prolonged vascular access.
Methods
Study design and setting
This retrospective observational cohort study evaluated PICC-port outcomes in consecutive patients treated at Fundación Valle del Lili, a tertiary center in Cali, Colombia, from January 2024 through August 2025. The study design adheres to the PROGRESS (Preferred Reporting of Observational Studies in Endovascular Strategies) framework for prognostic research, 9 specifically addressing fundamental prognostic questions by examining the natural history and determinants of vascular access-related outcomes in contemporary clinical practice. Study conduct and reporting follow STROBE guidelines for observational cohort studies. 10
Study population
We enrolled consecutive, selected and eligible patients meeting predefined inclusion and exclusion criteria during the study period, employing a non-probability consecutive sampling strategy (Figure 1). Eligible patients were adults (⩾18 years) with histologically or cytologically confirmed malignancies requiring prolonged central venous access (anticipated duration >4 weeks) who underwent PICC-port placement during the study period and required intermittent intravenous chemotherapy administration as determined by their treating oncologist. Patients were excluded if they presented with uncorrectable severe coagulopathy (international normalized ratio >2.0 or platelets <50,000/μL), active or prior ipsilateral upper extremity deep vein thrombosis, absolute contraindications for PICC-port placement (bilateral radical mastectomy with complete axillary lymphadenectomy, superior vena cava syndrome), advanced chronic kidney disease (estimated glomerular filtration rate <30 mL/min/1.73 m2) requiring ipsilateral arteriovenous fistula preservation, or anatomical constraints precluding safe catheter placement as determined by ultrasound evaluation.
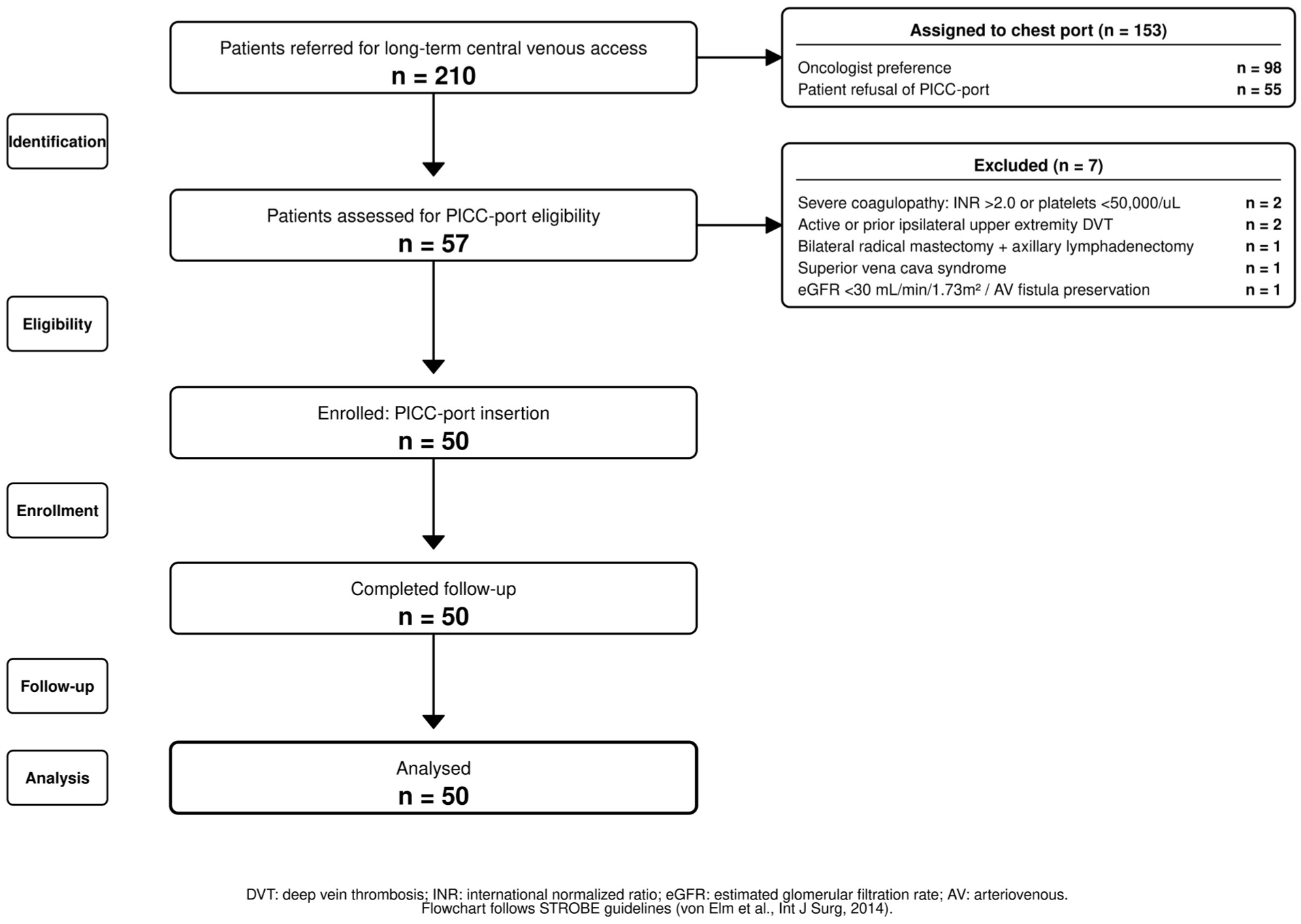
STROBE flow chart of patient selection.
Device and procedures
All devices were implanted by the institutional vascular access team, composed of board-certified physicians and certified clinical nurses with formal training in ultrasound-guided techniques and intracavitary electrocardiographic navigation. The vascular device used in all patients was the 5-French Polysite™ 2000 Series Micro Port (Vygon, Écouen, France). Intracavitary navigation was performed using the Arrow VPS Rhythm system (Teleflex, Wayne, PA, USA).
Procedures were performed under maximal aseptic conditions in non-operative procedure rooms. The basilic or brachial vein was identified bilaterally using real-time ultrasound, selecting the vessel with the largest diameter and minimal depth while maintaining the recommended 33% catheter-to-vein ratio. Patients were positioned supine with the selected upper limb abducted and fully exposed from the shoulder to the pectoral region, and the head turned contralaterally. The intracavitary navigation system was prepared by connecting electrodes, calibrating the navigator, and verifying the electrocardiographic signal. Wide-field antisepsis with chlorhexidine was performed, and sterile drapes were placed, including sterile covers for the ultrasound transducer and navigation system.
Local anesthesia was administered by infiltrating skin and subcutaneous tissue with 2% lidocaine without epinephrine at the puncture site. Ultrasound-guided venipuncture was performed with confirmation of venous blood return, followed by guidewire advancement. Proper intravascular guidewire position was verified ultrasonographically. A 3-mm skin incision was made, and a peel-away introducer was inserted; the dilator was removed while maintaining the sheath within the vessel. The 5-French catheter was then advanced under electrocardiographic navigation until maximal P-wave amplitude was achieved, confirming correct tip placement at the cavoatrial junction.
For subcutaneous pocket creation, the Zone Insertion Method (ZIM) was employed. The skin and tunneling tract were infiltrated with 2% lidocaine with epinephrine, and an approximately 2-cm skin incision was made, followed by blunt dissection to create a pocket approximately 1.5 cm in diameter. The catheter was tunneled from the pocket to the venous entry site and connected to the port reservoir, ensuring stability of the anchoring system. The chamber was flushed with saline to confirm appropriate flow and blood return. Finally, the pocket was closed in layers using absorbable sutures, medical-grade topical cyanoacrylate adhesive (Dermabond; Ethicon, Somerville, NJ, USA) was applied to the skin incision, and a sterile dressing was placed.
Variables and outcomes
Primary outcome measures
The primary outcome was device-related complications stratified by temporal occurrence. Early complications were defined a priori as adverse events occurring within 30 days of device insertion, including: procedure-site hematoma requiring intervention, local soft tissue infection, catheter malposition necessitating repositioning, and superficial or deep vein thrombosis. Late complications were defined as adverse events occurring ⩾30 days following insertion, including: catheter-related bloodstream infection (CRBSI) diagnosed per Infectious Diseases Society of America criterio, 11 symptomatic deep vein thrombosis confirmed by compression duplex ultrasonography, and mechanical device dysfunction requiring salvage intervention or removal.
Secondary outcome measures
Secondary outcomes included device survival time, defined as the interval from insertion to removal for any indication. Reasons for device removal were categorized as: (1) planned removal following treatment completion, (2) device-related complication, (3) patient death, or (4) device malfunction. All-cause mortality was ascertained through medical record review and institutional registries.
Data collection and management
Data were abstracted from electronic health records using standardized case report forms. Procedural details were obtained from vascular access team procedure logs. Follow-up data were obtained from outpatient oncology visits, infusion center encounters, emergency department presentations, and hospital readmissions. Data quality was ensured through logic checks and source verification, and analyses were performed using de-identified datasets.
Statistical analysis
We performed descriptive statistical analysis using Stata version 17.0 (StataCorp LLC, College Station, Texas, USA). Continuous variables were assessed for normality using the Shapiro-Wilk test and visual inspection of Q-Q plots. Variables demonstrating normal distribution were summarized as mean ± standard deviation (SD), whereas non-normally distributed variables were reported as median with interquartile range (IQR, 25th–75th percentile). Categorical variables were expressed as frequencies with proportions (percentages) and exact 95% confidence intervals (CI) calculated using the Wilson score method without continuity correction.
Person-time and incidence rate calculations
Total person-time at risk was calculated as the sum of individual catheter-days from device insertion to the first occurrence of device removal, patient death, or administrative censoring at study conclusion. Mean follow-up time was computed as total person-time divided by the number of patients. The cumulative incidence rate was expressed as events per 10,000 person-days with 95% confidence intervals calculated assuming a Poisson distribution. Complication-specific incidence rates were similarly calculated per 10,000 catheter-days at risk for early complications (<30 days), late complications (⩾30 days), catheter-related bloodstream infections, and thrombotic events.
Survival analysis
Device survival was analyzed using Kaplan-Meier methodology with catheter retention (freedom from device removal for any cause) as the primary time-to-event outcome. The survival function was estimated non-parametrically, with time zero defined as the date of device insertion. Events were defined as device removal for any indication including: complication-related removal, planned removal after treatment completion, device dysfunction, or patient death. Right-censoring was applied to devices remaining functional and in situ at administrative study closure.
Catheter retention probabilities were estimated at predefined clinically relevant time points: 30, 90, and 180 days post-insertion. Point estimates with 95% confidence intervals were calculated using the Greenwood variance formula. Median survival time (time to 50th percentile retention) was reported with 95% CI when estimable; if >50% of devices remained functional at study conclusion, median survival was reported as “not reached” with the corresponding retention probability and confidence interval at the longest follow-up time.
Sample size and missing data
Given the exploratory nature of this single-center study, no formal sample size calculation was performed. Analyses were primarily descriptive. Missing data were reported for each variable, and a complete-case analysis approach was used without imputation. For bivariate comparisons, a two-sided alpha of 0.05 was considered statistically significant without adjustment for multiple comparisons.
Results
Patient and procedural characteristics
A total of 50 oncology patients underwent PICC-port placement for chemotherapy delivery. The median age was 63 years (IQR 54–71), and 64% were female. The median body mass index was 26.0 kg/m2 (IQR 22.0–31.0). The most common comorbidities were hypertension (24%) and diabetes mellitus (14%). Twenty-two percent of patients had hematologic malignancies, while 78% had solid tumors. The basilic vein served as the access site in 96% of cases, with device placement in the left upper extremity in 72% of patients. The median venous diameter was 5.4 mm (IQR 4.9–6.6; Table 1).
Patient and procedural characteristics.
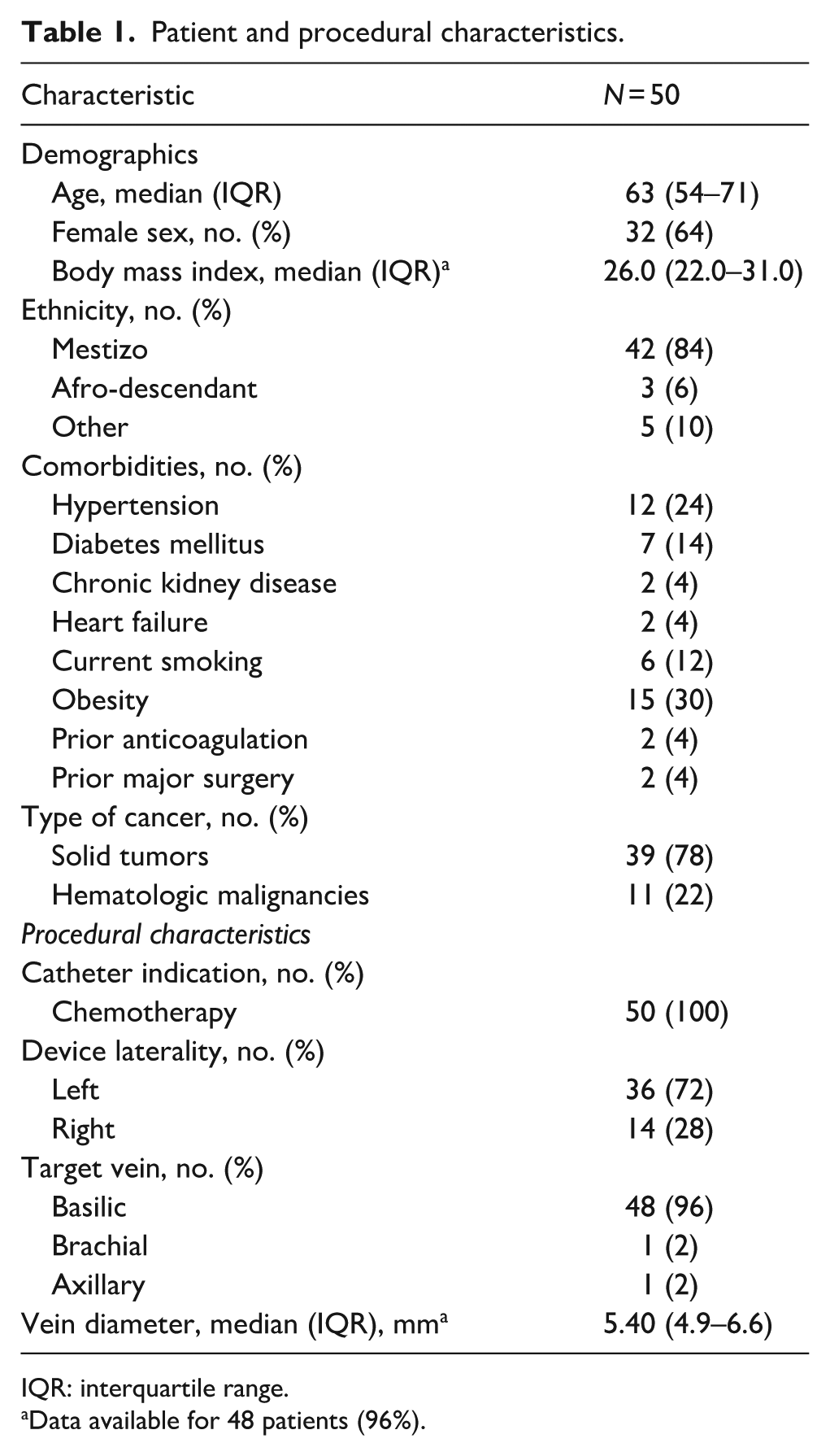
IQR: interquartile range.
Data available for 48 patients (96%).
Outcomes and complications
Technical success was achieved in all procedures (100%). No early complications occurred within 30 days (0%, 95% CI: 0%–7.1%). Temporary postoperative ecchymosis lasting 3–7 days was observed in three patients (6%). Late complications developed in two patients (4%): one case of catheter-associated deep vein thrombosis confirmed by ultrasound and managed with anticoagulation without device removal, and one catheter-related bloodstream infection treated conservatively. The overall complication rate was 3.1 per 10,000 catheter-days (Table 2).
PICC-Port complications and clinical outcomes.
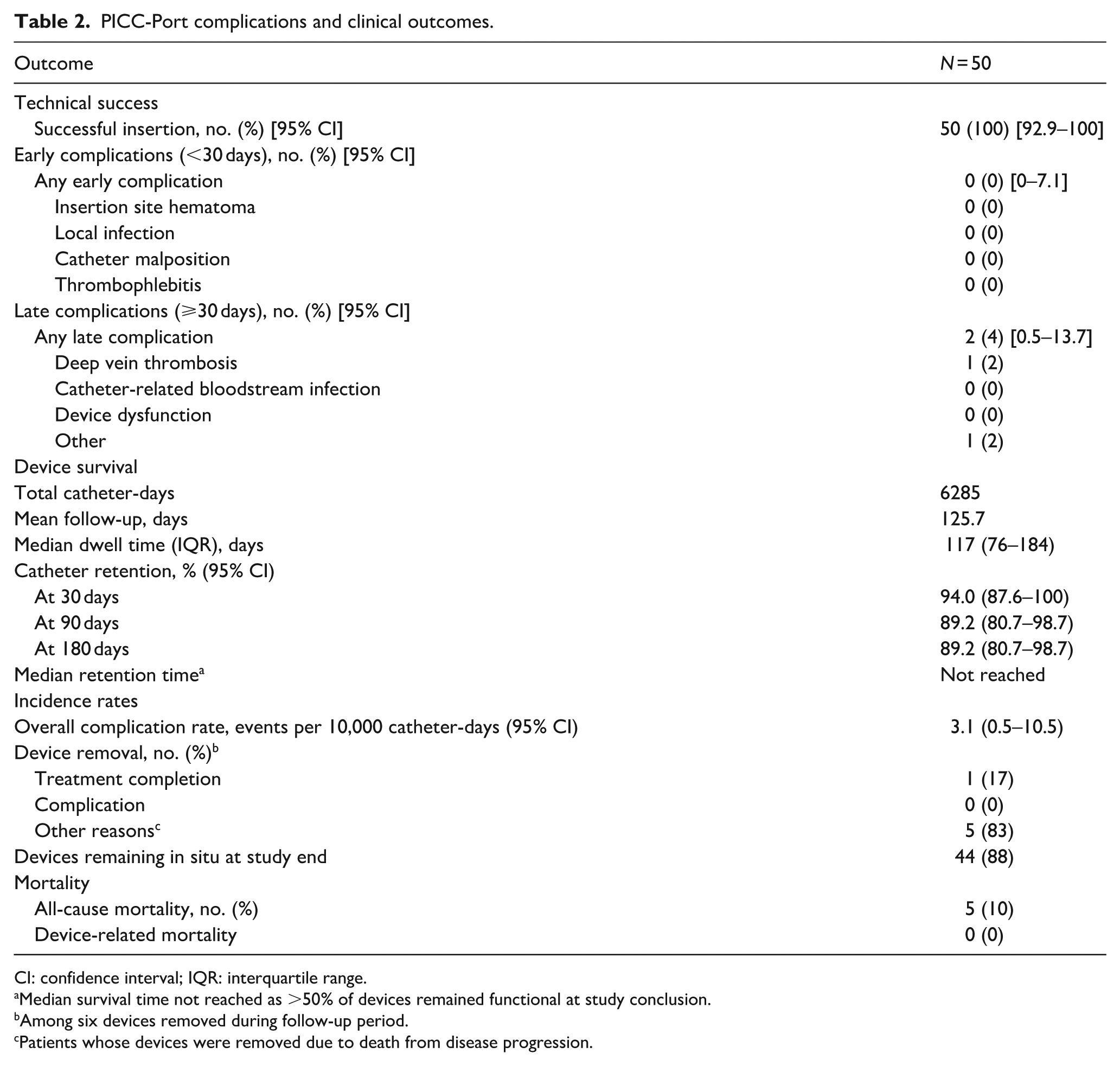
CI: confidence interval; IQR: interquartile range.
Median survival time not reached as >50% of devices remained functional at study conclusion.
Among six devices removed during follow-up period.
Patients whose devices were removed due to death from disease progression.
Kaplan-Meier analysis demonstrated catheter survival of 94.0% at 30 days and 89.2% at both 90 and 180 days (Figure 2). The median device dwell time was 117 days (IQR 76–184), with median survival time not reached. Five patients died from disease progression; no device-related deaths occurred.
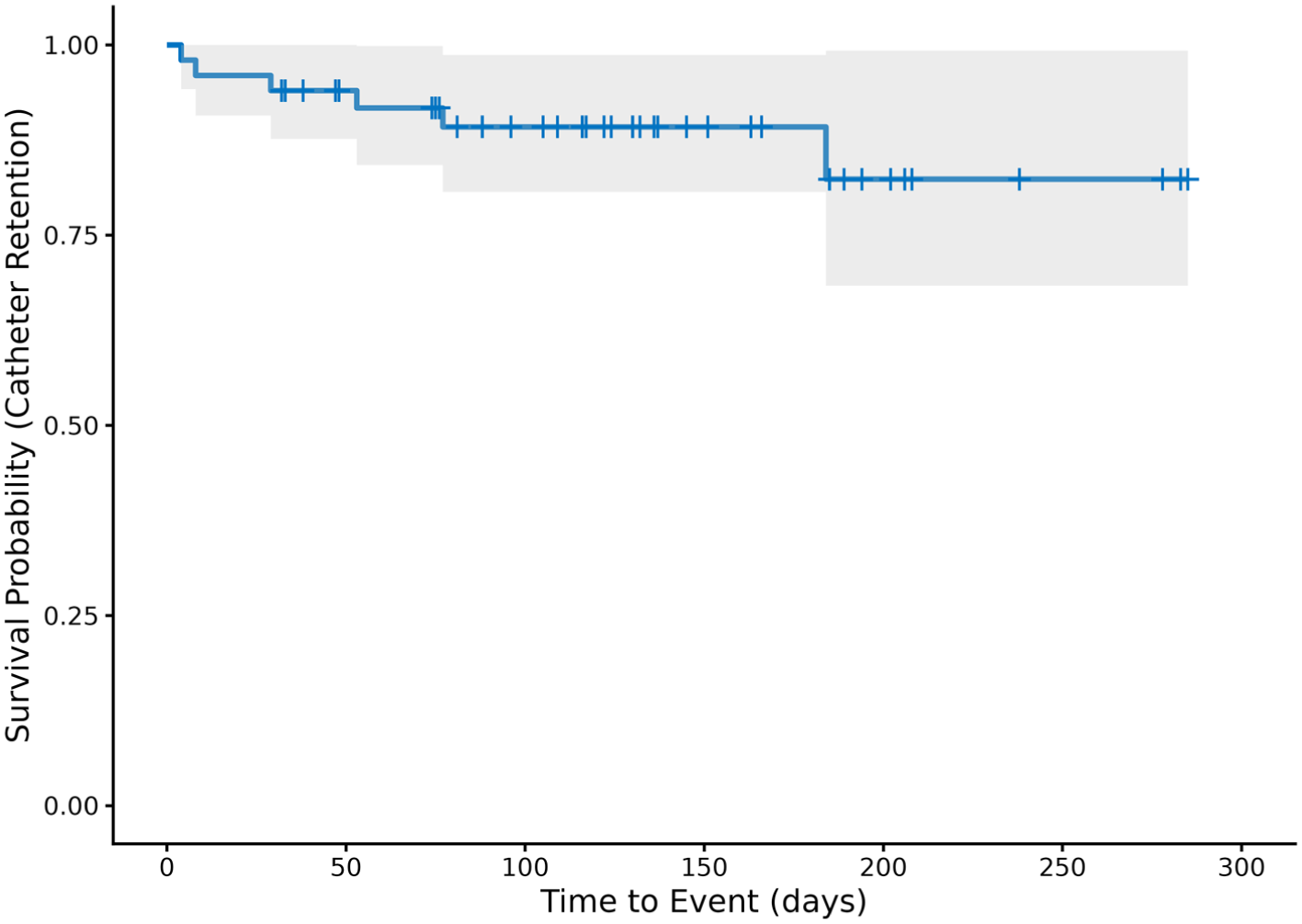
Kaplan-Meier catheter retention.
Discussion
This prospective observational study evaluated the safety and efficacy of PICC-port devices in oncology patients at a Colombian tertiary referral center. We achieved 100% technical success with no early complications and only 4% late adverse events. These outcomes compare favorably with published European series, demonstrating that PICC-port technology can be safely implemented in Latin American settings with appropriate training and protocols.
The absence of early complications is consistent with European reports, which show rates below 3% when procedures are performed by specialized teams using ultrasound guidance and intracavitary electrocardiographic navigation.8,12 In the GAVeCeLT multicenter study (n = 4480), device removal occurred in 1.2% of cases, with bloodstream infection in 0.42% and symptomatic thrombosis in 2.1%. 5 Our late complication rate (4%) and overall incidence (3.1 per 10,000 catheter-days) were within or below these benchmarks. Minor postoperative findings were less frequently documented (6% vs 18% transient ecchymosis reported in GAVeCeLT), likely because such self-limited events may not have been reported due to the retrospective data collection.
Traditional chest ports typically demonstrate complication rates of 5%–15%.1,3 Our results suggest that PICC-ports, when placed using appropriate insertion techniques, achieve safety profiles equivalent to chest ports while offering advantages in procedural invasiveness.
The median device dwell time of 117 days reflects typical chemotherapy treatment durations for solid tumors. While patients with hematological malignancies may require longer access periods, our findings demonstrate adequate device longevity for the predominant solid tumor population. The Kaplan-Meier analysis showing 89.2% catheter retention at 90 days provides reassuring evidence of device durability through multiple chemotherapy cycles.
Several procedural factors likely contributed to our favorable outcomes. All insertions were performed by a dedicated vascular access team with standardized training, emphasizing ultrasound-guided venipuncture, optimal catheter-to-vein ratio (⩽0.33), and electrocardiographic tip confirmation.13,14 This systematic approach minimizes mechanical complications, including catheter malposition, venous trauma, and arterial puncture.
The peripheral insertion site and mid-upper arm reservoir placement confer potential advantages over chest ports. The arm location avoids risks associated with central venipuncture such as pneumothorax, hemothorax, and injury to central vessels or thoracic duct. 15
Procedural efficiency merits emphasis. PICC-port insertions were completed in non-operative procedure rooms under local anesthesia without fluoroscopy or sedation, contrasting with chest port placement which typically requires operating room resources, fluoroscopy, and anesthesia. This facilitates broader access to totally implantable devices in resource-constrained settings.
Clinical implications for Latin American settings
Our findings suggest that PICC-port programs are technically feasible in Latin American settings without requiring dedicated interventional radiology suites or fluoroscopy. The absence of early complications in our cohort indicates that the learning curve may be overcome with structured training, particularly in teams experienced in standard PICC insertion.
From a health economics perspective, formal cost-effectiveness analysis was beyond our study scope. Although PICC-port device costs are comparable to chest ports, overall economic impact may vary by institution. Placement in procedure rooms and the low complication rates may reduce facility and complication-related costs. However, feasibility depends on local resources and device availability. Further cost-effectiveness studies are needed in Latin American settings, considering infrastructure, procedural efficiency, complication management, and indirect patient costs.
Study limitations
Several limitations warrant acknowledgment. The single-center design and small sample size limit generalizability, as our experience may not reflect outcomes at centers with less vascular access expertise. The observational, non-randomized design precludes definitive conclusions about PICC port superiority.
The limited follow-up duration may underestimate late complications that occur beyond 6 months. Our cohort consisted predominantly of patients with solid tumors; generalizability to hematological malignancies requiring longer access or non-oncological indications remains uncertain.
The retrospective design could introduce ascertainment bias. Despite using multiple data sources, mild outpatient complications may have been underreported. Finally, we did not assess patient-reported outcomes, such as quality of life or satisfaction, 16 which European studies suggest favor PICC-ports but require validation in Latin American populations.
Future research directions
Several research priorities emerge from our findings. Multicenter prospective registries across Latin America would establish regional benchmarks, identify risk factors, and inform implementation strategies. Randomized controlled trials comparing PICC-ports to chest ports and external PICCs are needed, incorporating patient-centered outcomes including quality of life, procedural pain, and patient preferences.
Cost-effectiveness analyses tailored to Latin American healthcare contexts would inform resource allocation and reimbursement policies, considering both healthcare system costs and patient-related burdens, including transportation costs, caregiver time, and productivity losses. Research examining optimal patient selection criteria would guide clinical decision-making based on treatment duration, chemotherapy regimen characteristics, patient anatomy, comorbidities, and patient preferences.
Conclusions
Our experience with PICC-ports in oncology patients demonstrated an excellent safety profile with low complication rates. These findings support PICC-ports as a viable and less invasive alternative to chest ports when performed by trained teams using ultrasound guidance and electrocardiographic navigation.
PICC-ports offer advantages: efficient placement outside operating rooms without fluoroscopy or sedation, lower infection risk, and minimal maintenance requirements. In resource-constrained Latin American settings, these features reduce both healthcare costs and patient burden while enabling high-volume oncologic centers to manage increased demand. With appropriate training and standardized protocols, vascular access teams in middle-income countries can achieve safety outcomes comparable to high-income settings. Validation through larger multicenter studies is warranted.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The Biomedical Research Ethics Committee of Fundación Valle del Lili approved the study (Protocol No. 351) on June 17, 2025, and classified it as risk-free under Colombian regulations (Resolution 8430 of 1993).
Informed consent
The requirement for informed consent was waived due to the retrospective analysis of de-identified medical records without direct participant contact.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions but are available from the corresponding author on reasonable request.*