
Abstract
Background:
Radial artery catheterization (RAC) remains challenging, with a high failure rate. This study investigated whether ultrasound-measured radial artery (RA) diameter could predict RAC failure in patients undergoing major cardiac or vascular surgery.
Methods:
Consecutive patients scheduled for major cardiac or vascular surgery were prospectively included. Ultrasound images of the left RA were acquired by one operator, while a second operator, blinded to these images, performed RAC using the palpation method. RAC failure was defined as three or more attempts, a change in operator, or cannulation site. All ultrasound images were subsequently analyzed by an expert vascular physician, also blinded. RA internal diameter and depth were measured. Intra- and inter-observer reproducibility were assessed.
Results:
Of 247 patients, 58 (23%) experienced RAC failure. Absent or weak radial pulse (OR 6.36, 95% CI 2.59–15.65; p < 0.001), female sex (OR 2.55, 95% CI 1.36–4.77; p = 0.003), and wrist circumference <18 cm (OR 1.96, 95% CI 1.08–3.54; p = 0.03) each significantly increased RAC failure risk. The RA internal diameter was significantly smaller in the failure group (1.9 ± 0.4 vs 2.1 ± 0.4 mm, p < 0.01). RA was also deeper in the failure group (3.4 ± 1.6 vs 2.9 ± 1.1 mm, p = 0.05). The area under the curve for RA internal diameter to predict RAC failure was 0.62 (95% CI 0.53–0.70, p = 0.007), with an optimal threshold of 1.8 mm. RAC failure prolonged anesthesia induction and doubled the risk of hematoma (p < 0.001). Intra- and inter-observer agreement for RA internal diameter were excellent (ICC 0.86, 95% CI 0.78–0.92 and 0.94, 95% CI 0.91–0.97, respectively).
Conclusion:
A small RA internal diameter significantly increases RAC failure risk. These findings should inform cannulation site selection, technique, and operator choice to improve procedural success and patient safety.
Keywords
Introduction
Radial arterial catheterization (RAC) is a standard monitoring tool used to measure invasive blood pressure continuously in patients undergoing cardiac or major vascular surgery, both in the operating room and the intensive care unit (ICU). 1 The radial artery (RA) is the most commonly used site due to its superficial location, ease of access, and relatively low risk of complications. 2
RAC is a common yet technically challenging procedure, routinely performed by nurse anesthetists (NAs). 3 Literature reports a first-attempt failure rate ranging from 10% to 40%. 4 While ultrasound guidance has been shown to improve RAC success rates, 4 the blind palpation method remains widely used in clinical practice, primarily due to its simplicity and speed.
Previous studies on coronary catheterization procedures have shown that a smaller wrist circumference, lower body weight, and shorter height are associated with a reduced RA diameter and an increased risk of vascular complications.5,6 However, in perioperative settings, the RA diameter is not routinely measured to predict RAC failure. We hypothesized that a smaller RA diameter increases the risk of RAC failure.
This study aimed to determine the predictive value of RA diameter, as measured by ultrasonography, in predicting RAC failure when using digital palpation. Secondary objectives included identifying other risk factors for RAC failure, evaluating the impact of RAC failure, and assessing intra- and interobserver agreement for ultrasound measurements.
Methods
Study design
This prospective, monocentric, observational study was conducted in consecutive patients undergoing cardiac or aortic surgery at Montpellier University Hospital (France) between April 2021 and April 2022. The study was designed and conducted in accordance with the STROBE guidelines. 7 The institutional review board approved the research protocol and waived the requirement for written informed consent.
Study population
Patients were screened the day before surgery. Eligible patients were those over 18 years of age, scheduled for cardiac or aortic surgery, and able to provide informed consent. Exclusion criteria included pregnancy, emergency surgery, the presence of an arterial catheter, local contraindications for RAC, refusal to participate, and cases where the catheter was primarily placed using ultrasound guidance.
Validation of the nurse anesthetist team
Before the study commenced, twenty experienced NAs with comparable training were validated as investigators. This validation followed specific theoretical and practical training in peripheral ultrasound imaging, provided by our vascular physician.
Procedure of RAC
In the operating room, ultrasound images of the left RA were recorded by the first operator (NA1), who was strictly assigned to ultrasound imaging. The same ultrasound machine (Mindray® TE7™, Shenzhen, China), linear probe (L14-6Ns™), and transmission gel were used for all patients. Ultrasound settings (depth, gain, and focus) were kept identical for all examinations. The imaging site for all patients was the same as the RA puncture site, located 2 cm from the wrist joint (Figure 1).
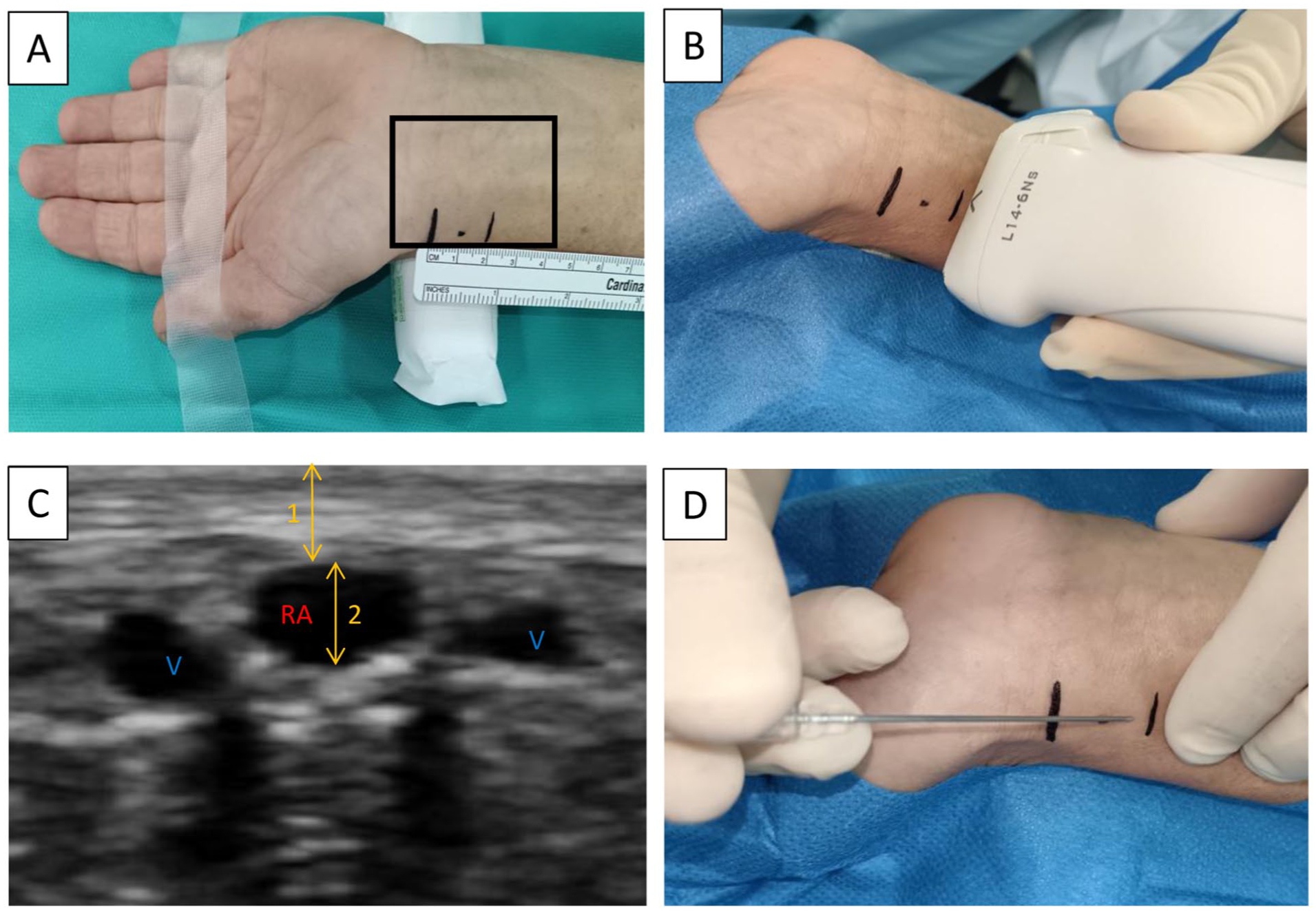
Ultrasound-guided measurement technique and RA catheterization procedure: (a) anatomical landmarks for the puncture site, located 2 cm proximal to the wrist joint, (b) positioning of the ultrasound probe for imaging, (c) ultrasound image of the RA, and (d) RA cannulation site, located 2 cm proximal to the wrist joint.
The second operator (NA2) performed RAC on the left side using the palpation method alone (Figure 1). The radial pulse was classified as follows: 0 for absent, 1 for weak, and 2 for strong. The catheters used were Vygon®, 6 cm in length, 20 gauge (Vygon®; Ecouen, France, reference 6115.096).
Definition of RAC failure
RAC failure was defined as requiring three or more punctures, a change of operator, or a change in the catheterization site during the initial cannulation attempt. Shifting from blind cannulation to ultrasound guidance was not allowed for the first two attempts. The duration of the catheterization procedure, the number of punctures, and the reasons for failure were recorded.
Clinical risk factors
Data collected included gender, age, weight, height, American Society of Anesthesiologists (ASA) score, and tobacco consumption. Vascular risk factors such as diabetes, dyslipidemia, arterial hypertension, and chronic kidney failure were also documented.
Ultrasound measurements
All ultrasound imaging was analyzed by an expert vascular physician, who was blinded to the RAC success or failure status. The expert measured the internal diameter of the RA, and its depth (Figure 1). In the first 50 patients included, RA measurements were repeated by both the expert and NA1 to assess inter- and intra-observer reproducibility.
Statistical methods
Considering a small diameter as the positive test and failure as the event to predict, we aimed to analyze 300 patients to maximize the positive predictive value and specificity. Baseline data were compared between failure and success groups using standard statistical tests, and the correlation between ultrasound measures was assessed using Pearson’s correlation coefficient and its 95% confidence interval (CI).
Predictive values
The predictive value of each measure was assessed using the area under the receiver operating characteristic curve (AUC of the ROC) and its 95% CI. As no threshold of the internal diameter could efficiently satisfy our objectives on specificity, we used the Youden’s index to derive the most discriminative threshold and calculated the sensitivity, specificity, and predictive values of this threshold.
Intra- and interobserver agreement
Intra- and interobserver agreements were assessed using the intraclass correlation coefficient (ICC) and its 95% CI. Discordance was further explored using Bland–Altman plots.
Consequences of RAC failure
The arterial catheters were used throughout the perioperative period. Clinical complications, such as wrist hematoma, ischemia, or severe pain at the left wrist, were assessed the day after surgery in the intensive care unit (ICU). The duration of anesthesia and in-hospital length of stay were also recorded.
Results
Study population
Between April 2021 and April 2022, 600 patients were eligible, and 329 were included. Eighty-two patients were excluded due to non-analyzable ultrasound images, and data from 247 patients were analyzed (Figure 2). Baseline characteristics are presented in Table 1.
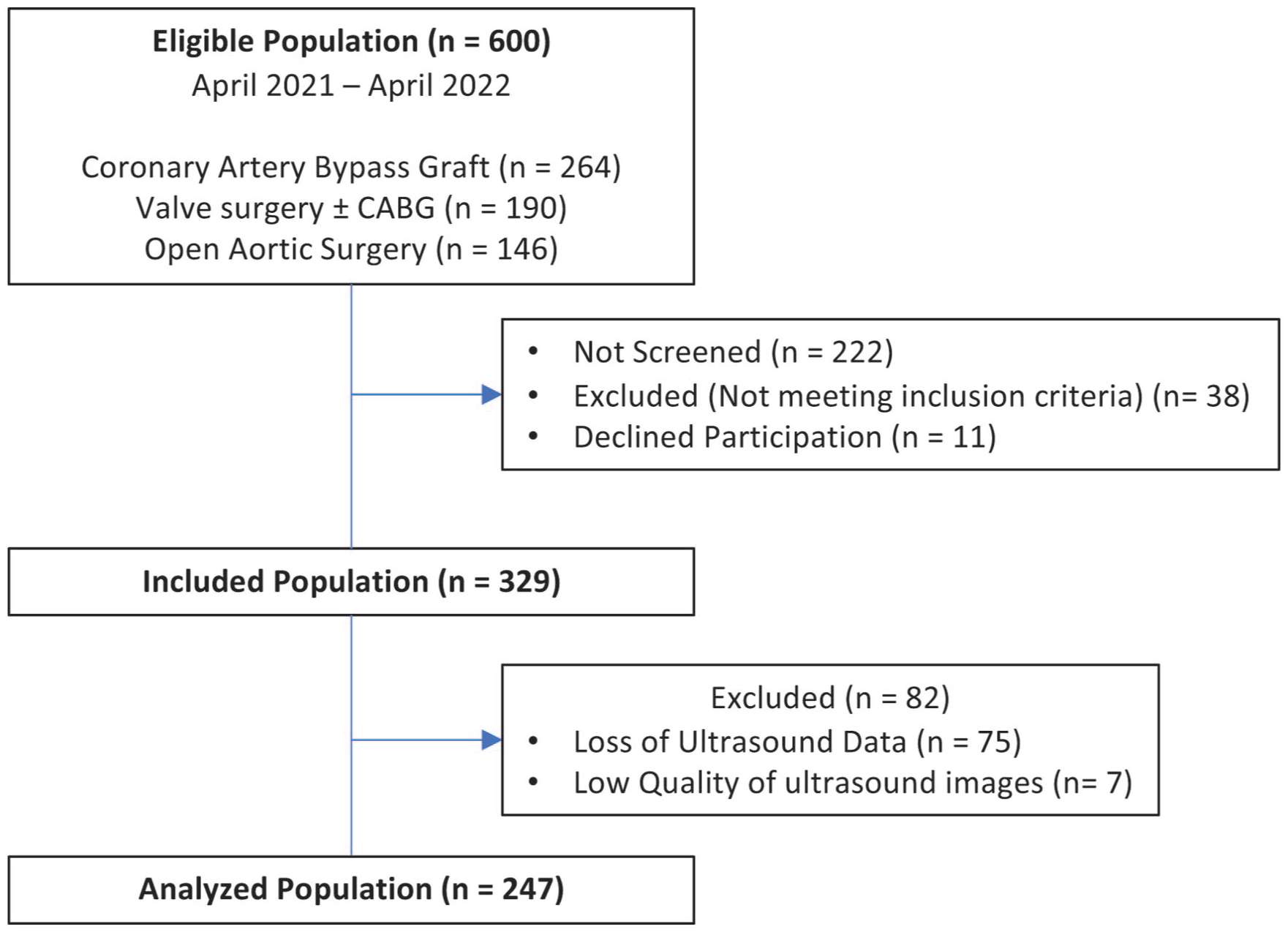
Flow chart of the study.
Study population. Demographic data and proportion of risk factors and cardiovascular diseases in the RAC success and failure groups.
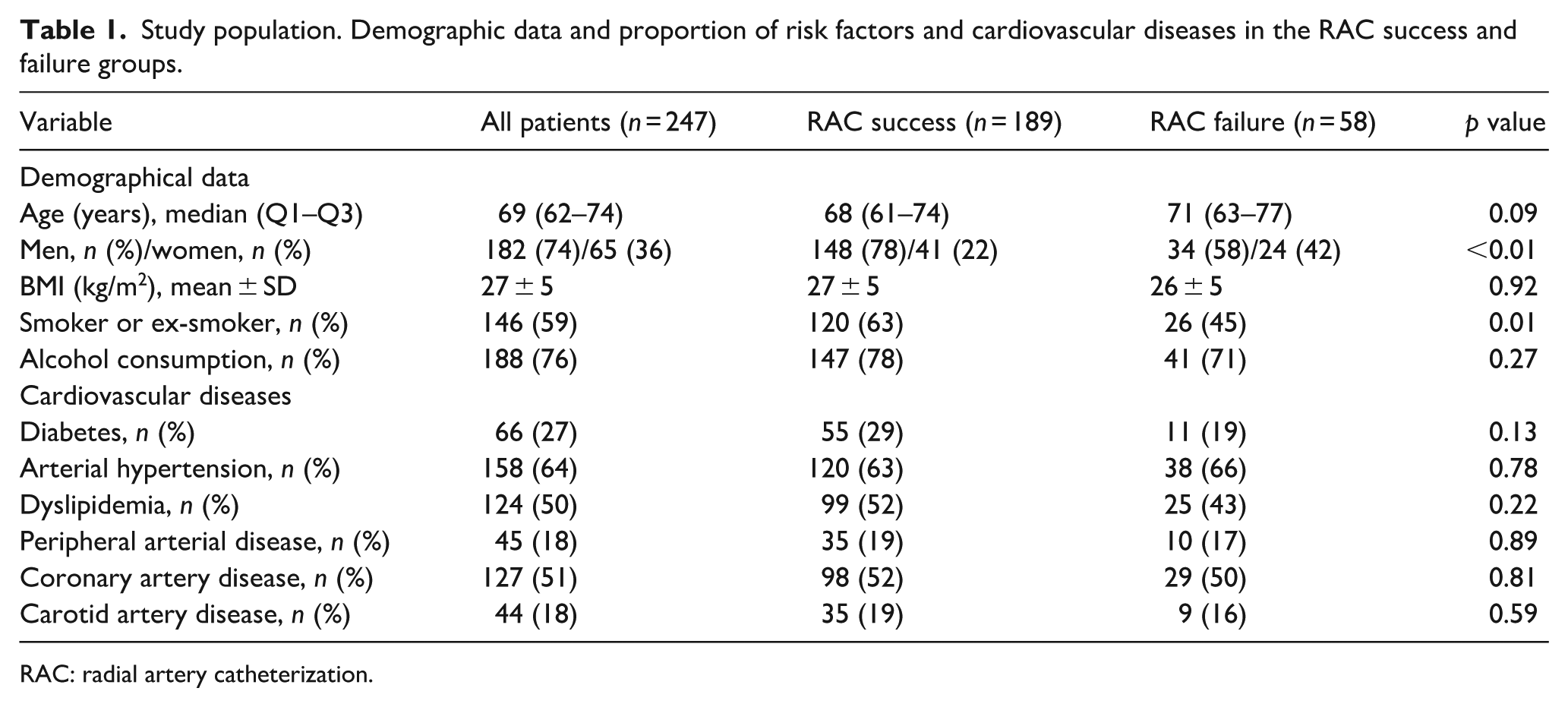
RAC: radial artery catheterization.
Proportion of RAC failure
Of the 247 patients, 58 (23%) were in the RAC failure group, and 189 (77%) in the success group. RAC succeeded after the first puncture in 144 patients (58%) and after the second in 45 patients (18%). Three or more punctures were attempted in 56 patients, with operator or cannulation site changes in two cases. RAC failed in 33 patients (13%) after the third puncture, and 15 patients (6%) had four or more punctures, with a maximum of 10 attempts. The main failure causes were absence of arterial blood flow and guidewire insertion failure.
Clinical risk factors for RAC failure
The presence of an absent or weak radial pulse was associated with a sixfold increase in the risk of failure (OR = 6.36, 95% CI 2.59–15.65, p < 0.001). The risk of RAC failure was approximately doubled in women (OR = 2.55, 95% CI 1.36–4.77, p = 0.003) and in patients with a wrist circumference <18 cm (OR = 1.96, 95% CI 1.08–3.54, p = 0.03). Mean age and cardiovascular risk factors were comparable between groups (Table 1). In the failure group, mean arterial pressure (MAP) was lower (79 ± 12 vs 84 ± 15 mmHg, p = 0.02), and reperfusion time after the Allen test was longer (6 ± 2 vs 5 ± 3 s, p = 0.04; Table 2). A wrist circumference <18 cm doubled the risk.
Clinical parameters and ultrasound measurements in the RAC success and failure groups.
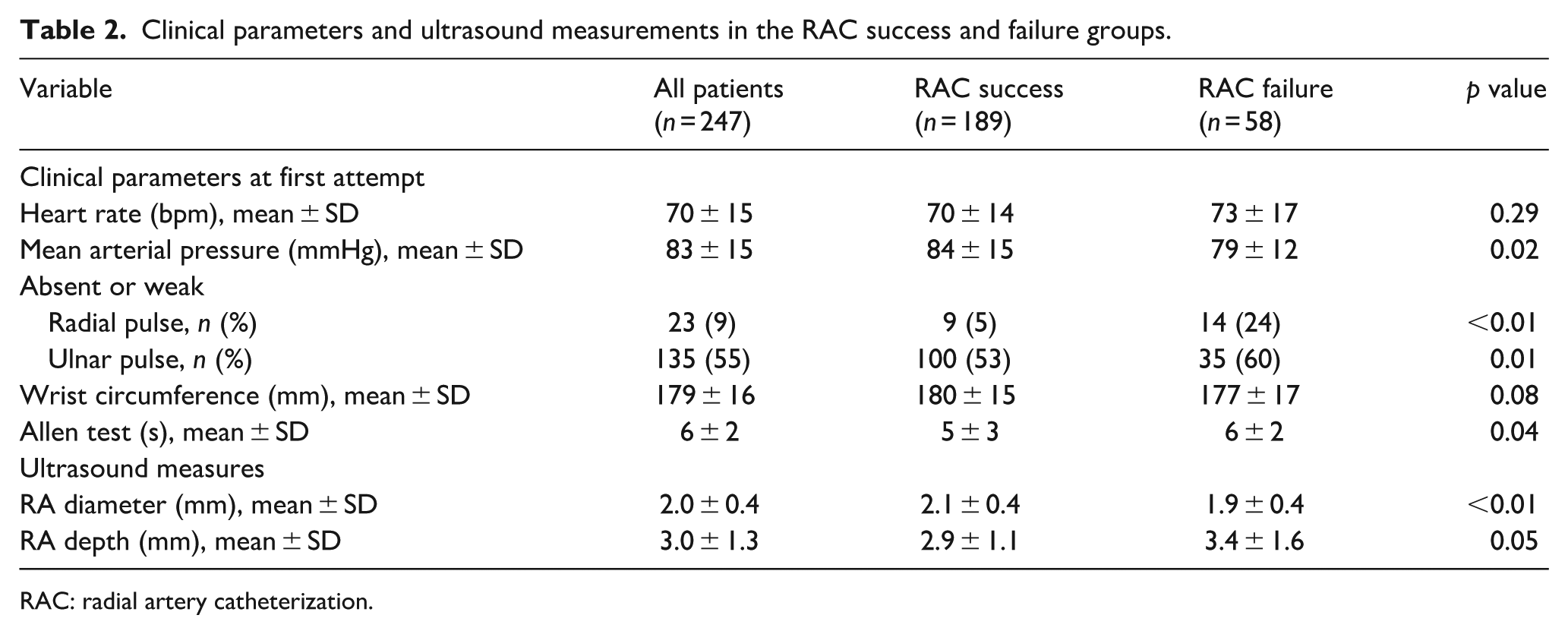
RAC: radial artery catheterization.
Ultrasound measurements
RA internal diameter was smaller in the failure group (1.9 ± 0.4 vs 2.1 ± 0.4 mm, p < 0.01). The RA was also deeper in the failure group (3.4 ± 1.6 vs 2.9 ± 1.1 mm, p = 0.05; Table 2).
Predictive values of the RA internal diameter
The RA internal diameter’s ability to predict RAC failure was modest but significant (AUC = 0.62, 95% CI 0.53–0.70, p = 0.007; Figure 3(a)). The optimal RA internal diameter threshold was 1.8 mm (Figure 3(b)), with a sensitivity of 52% (95% CI 38–65) and specificity of 66% (95% CI 59–73). Positive predictive value was 32% (95% CI 23–42). Below 1.4 mm, the positive predictive value exceeded 40%. Combining an RA internal diameter <1.8 mm with an absent or weak pulse increased specificity to 97% (95% CI 94–99) and positive predictive value to 64%.
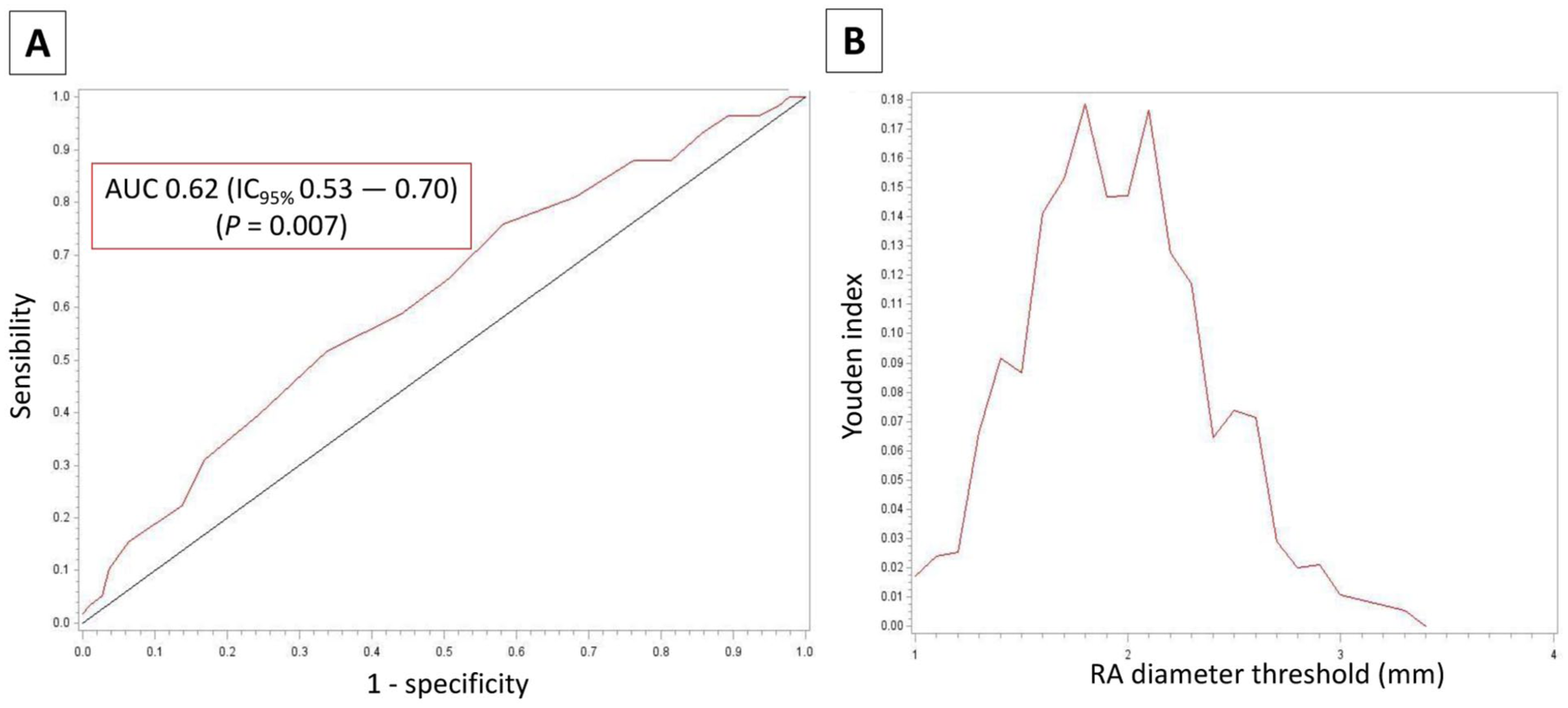
Ability of the RA internal diameter to predict RAC failure: (a) ROC curve showing the diagnostic performance of RA diameter for predicting RAC failure and (b) Youden index curve illustrating the optimal cutoff value of RA diameter that maximizes the sum of sensitivity and specificity for RAC failure prediction.
Intra- and interobserver agreement
ICC values indicated excellent reproducibility for RA internal diameter: intra-observer (0.86, 95% CI 0.78–0.92) and inter-observer (0.94, 95% CI 0.91–0.97).
Consequences of RAC failure
Hematoma was the only complication observed, occurring more than twice as often in the failure group (72% vs 32%, RR = 2.29, 95% CI 1.75–2.97, p < 0.001). RAC duration was significantly longer in the failure group (28 ± 17 vs 9 ± 9 min, p < 0.001), with a maximum of 93 min. Anesthetic time prior to incision increased by 10 min (57 ± 19 vs 46 ± 17 min, p < 0.01). Hospital length of stay was similar between groups (14 ± 11 vs 13 ± 11 days, p = 0.17).
Discussion
RAC remains a cornerstone of hemodynamic monitoring in cardiac and major vascular surgeries. 1 Despite its widespread use, RAC failure continues to pose a significant challenge, 4 with failure rates defined by three or more attempts reaching up to 23% in our study, with 42% of patients requiring more than one puncture. These results underscore the limitations of the traditional palpation technique, which is associated with a high likelihood of failure.4,8 This highlights the urgent need to reconsider the reliance on blind puncture and supports the transition towards ultrasound-guided techniques. 2
For the first time, our study evaluated the predictive value of RA diameter, measured by ultrasound, to predict RAC failure in a large cohort of 247 patients. A key contribution of our study is the identification of critical factors associated with RAC failure, including reduced RA diameter and increased RA depth. Ultrasound assessment allowed us to pinpoint these variables, which are crucial for recognizing patients at higher risk of difficult or failed cannulation. This aligns with the recommendations from the European Society of Anesthesiology, which advocates for the use of ultrasound in hypotensive, hypovolemic, and hemodynamically unstable patients, as well as those with vascular diseases and weak pulses. 9
Clinical risk factors
Our study identified several clinical risk factors for RAC failure, foremost an absent or weak radial pulse, which was associated with a sixfold increase in failure risk. Female sex and a small wrist circumference were also significant predictors, each approximately doubling the risk of failure. These findings are clinically relevant and consistent with previous studies5,10,11 that have reported associations between failure and factors such as low weight, small wrist circumference, and Asian race. Each of these factors is likely related to a smaller arterial diameter. Other anatomical or physiological factors—such as hypotension—may play a critical role. This is supported by our finding that MAP was significantly lower in the failure group, further indicating that hemodynamic status may impact RAC success. 9
Sonographic predictors of RAC failure
Our results demonstrate that a small RA diameter is significantly associated with a higher failure rate. An RA internal diameter below 1.8 mm had a positive predictive value of 32% for RAC failure, which increased to 64% when combined with an absent or weak radial pulse. This suggests that while RA diameter is a valuable decision-making tool, it should not be used in isolation. Our study is the first to reported excellent intra- and interobserver agreement for ultrasound measurements of the RA, thereby reinforcing the reliability of these assessments.
Consequences of RAC failure
Difficult radial arterial catheterization (RAC) not only significantly prolongs procedural time but also disrupts workflow efficiency, leading to notable delays. 12 In our cohort, RAC duration was substantially longer in the failure group (28 ± 17 vs 9 ± 9 min, p < 0.001), with one case reaching 93 min. RAC failure also extended anesthetic management by an average of 10 min. Additionally, the rate of hematoma at the puncture site was more than doubled in the failure group. Previous research identified RA diameter as an independent determinant of vascular complications post-procedure. These findings reinforce the clinical advantages of ultrasound guidance, which effectively reduces hematoma rates and arterial catheter cessation of function by minimizing both the number of attempts and the mean time to cannulation. 13
Study limitations
First, our definition of RAC failure—three or more punctures or a change of operator/site—may be debated, as we consider a “failed puncture” to have clinical significance. Literature definitions vary (one to five attempts),6,14 and cannulation duration may be as important as the number of attempts. A consensus from the Society for Cardiovascular Angiography and Intervention recommends changing the cannulation site if transradial access is not achieved within 3 min after the first attempt. 15
Second, our study focused on the blind palpation technique, and further research is needed to evaluate the impact of a small RA diameter on ultrasound-guided RAC failure rates. In children, authors have already reported that a reduced RA diameter is an independent predictor of RAC failure, even when ultrasound is used. 16
Third, the operator effect was not analyzed, although we mitigated this risk by providing standardized training to the 20 nurse anesthetists involved and enrolling consecutive patients.
To standardize our local practices, we focused exclusively on the left radial artery, 2 cm from the wrist joint. However, some studies suggest that a more proximal cannulation site, 17 at least 4 cm from the wrist joint, may offer advantages due to the linear tract of the artery and reduced wrist motion. Further research is needed to explore the benefits of proximal sites (Supplementary Results).
Perspectives
Our findings strongly support abandoning the blind technique in favor of routine ultrasound assessment of risk and guidance, in line with recent international guidelines. 2 A deeper understanding of the risk factors influencing RAC failure could help anesthesiologists make informed decisions about changing the cannulation site, device size, or referring the procedure to a more experienced operator. 17 Future studies could explore the use of risk scores 11 to predict difficult RAC and guide the selection of the most appropriate technique, site, or operator, or even consider performing a median nerve block prior to cannulation. Finally, in nurse anesthetist training programs, mastery of ultrasound-guided catheterization techniques should be complemented by comprehensive training in ultrasound measurement and interpretation. This integrated approach will ensure both procedural proficiency and accurate assessment of vascular structures.
Conclusion
In this prospective study of 247 patients, a smaller radial artery diameter was significantly associated with a higher failure rate of palpation-guided RAC. Our results emphasize the importance of considering RA diameter prior to cannulation and support the adoption of ultrasound guidance to improve success rates and reduce complications.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261455502 – Supplemental material for Ultrasound to predict radial artery catheterization failure in patients undergoing major cardiovascular surgery (UPRAC)
Supplemental material, sj-docx-1-jva-10.1177_11297298261455502 for Ultrasound to predict radial artery catheterization failure in patients undergoing major cardiovascular surgery (UPRAC) by Jerome Paniego, Gudrun Boge, Marc Mourad, Claire Duflos, Matheus Van Rens, Remy Ruiz, Emmanuel Lorne and Pierre Sentenac in The Journal of Vascular Access
Footnotes
Acknowledgements
We are grateful to the nurse anesthetist research team of the Arnaud de Villeneuve Montpellier University Hospital, to Valerie Macioce, medical writer, and Fanchon Herman, methodologist.
Author contributions
JP: conceptualization, methodology, investigation, writing—original draft, funding acquisition, supervision, project administration, response to reviewers. MM, MVR, and EL: resources, review, and editing, validation, response to reviewers. CD: conceptualization, methodology, formal analysis. GB and RR: supervision, validation, investigation. PS: conceptualization, methodology, formal analysis, writing—original draft, review, funding acquisition, project administration, response to reviewers.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the institution and received a grant in 2019 from a research program PHRIP (hospital program for nurses research) and the DGOS (French General Directorate of Health Care Provision).
Ethical approval
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki. The institutional review board approved the research protocol and waived the need for written informed consent (ID-RCB: 2020-A01661-38). The study was prospectively registered at ClinicalTrials.gov, NCT04730479, before the inclusion of the first patient.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.