
Abstract
Advancement of long femorally inserted central catheters (FICCs), particularly 4–5 Fr, 55 cm devices introduced via the superficial femoral vein at mid-thigh, may be limited by the presence of venous valves, bifurcations, or inadvertent diversion into collateral pathways such as the ascending lumbar vein. Smaller-caliber, more flexible catheters appear especially prone to primary maldirection along the iliac–caval axis. We describe a simple technical modification aimed at facilitating catheter progression toward the inferior vena cava and potentially reducing the risk of primary malposition. In this approach, the original internal stylet of a 4–5 Fr single-lumen, 55 cm catheter is replaced with a 0.035″ × 70 cm J-tip metallic guidewire. During the initial phase of insertion, the guidewire is kept entirely within the catheter lumen, thereby increasing the overall longitudinal stiffness of the system and improving pushability. After ~20–25 cm of advancement—corresponding to the expected position within the common femoral or iliac vein—the guidewire is advanced slightly, allowing the J-tip to protrude about 2 cm beyond the catheter tip. This configuration enables the guidewire to lead navigation toward the inferior vena cava. The increased shaft rigidity reduces the tendency to buckle and limits tip deflection during progression through the iliac segment. Furthermore, the minimally protruding, atraumatic J-tip, characterized by a wide curvature, appears less likely to engage narrow or posterior collateral pathways, such as the ascending lumbar vein, thereby favoring alignment with the larger-caliber inferior vena cava and promoting smoother advancement along the main venous axis. This guidewire-assisted maneuver is simple, reproducible, and compatible with ultrasound-based tip location protocols. Further prospective studies are warranted to assess its impact on technical success rates and on the reduction of catheter malposition.
Keywords
Introduction
Femorally inserted central catheters (FICCs), placed through ultrasound-guided puncture of the superficial vein, are increasingly adopted in patients in whom upper-body venous access is contraindicated or technically unfeasible. Clinical scenarios such as superior vena cava syndrome, thrombosis of the jugular or subclavian veins, chest wall infections, or extensive upper limb immobility often make the femoral route a safe and effective alternative.1–4
When long femoral catheters are inserted according to structured bundles such as the SIF protocol 2 and when tip location is confirmed intraprocedurally by ultrasound (ECHOTIP protocol), 5 complication rates are acceptable and comparable to other central venous access strategies. Nevertheless, primary malposition remains a recognized issue.
Among the possible maldirections, inadvertent cannulation of the ascending lumbar vein (ALV) represents a rare but potentially severe complication. As documented in multiple reports,6–18 ALV malposition may be asymptomatic or may present with infusion-related lumbar pain, neurological symptoms, retroperitoneal hemorrhage, or even hypovolemic shock.
In our clinical practice, we have observed that advancement of small-caliber (4–5 Fr), long (~55 cm) catheters inserted at mid-thigh via the superficial femoral vein may occasionally be difficult. The catheter may encounter resistance at venous valves, may abut bifurcations, or may deviate posteriorly toward lumbar collateral pathways. This appears to be more frequent when using highly flexible devices.
We describe here a simple technical modification aimed at improving catheter progression along the iliac–caval axis by temporarily increasing shaft rigidity and using a J-tip guidewire as a mandrel to guide navigation at the iliocaval confluence.
Material and methods
The technique is applied to long 4 or 5 Fr, single lumen 55 cm peripherally inserted central catheters (PICCs) placed through the superficial femoral vein at mid-thigh with the intention of reaching the inferior vena cava. The materials required are routinely available in vascular access practice and include a standard microintroducer set, the 4–5 Fr, 55 cm single lumen PICC, and a 0.035″ metallic guidewire 70 cm in length with an atraumatic J-tip.
Venous access is obtained by ultrasound-guided puncture of the superficial femoral vein according to established recommendations.2,3 Real-time ultrasound guidance allows accurate identification of the vessel, optimal puncture at mid-thigh, and avoidance of arterial injury. After successful cannulation, a microintroducer is positioned using the modified Seldinger technique, following standard procedural steps for FICC placement. The catheter has to be flushed with saline prior to guidewire insertion in order to lubricate the lumen and facilitate smooth extraction.
Before catheter advancement, the original internal stylet supplied with the device is removed and replaced with a 0.035″ × 70 cm J-tip metallic guidewire inserted into the catheter lumen. Initially, the guidewire is positioned so that its J-tip remains entirely within the distal portion of the catheter, with no protrusion beyond the catheter tip (Figure 1). In this configuration, the guidewire functions solely as an internal stiffening element.
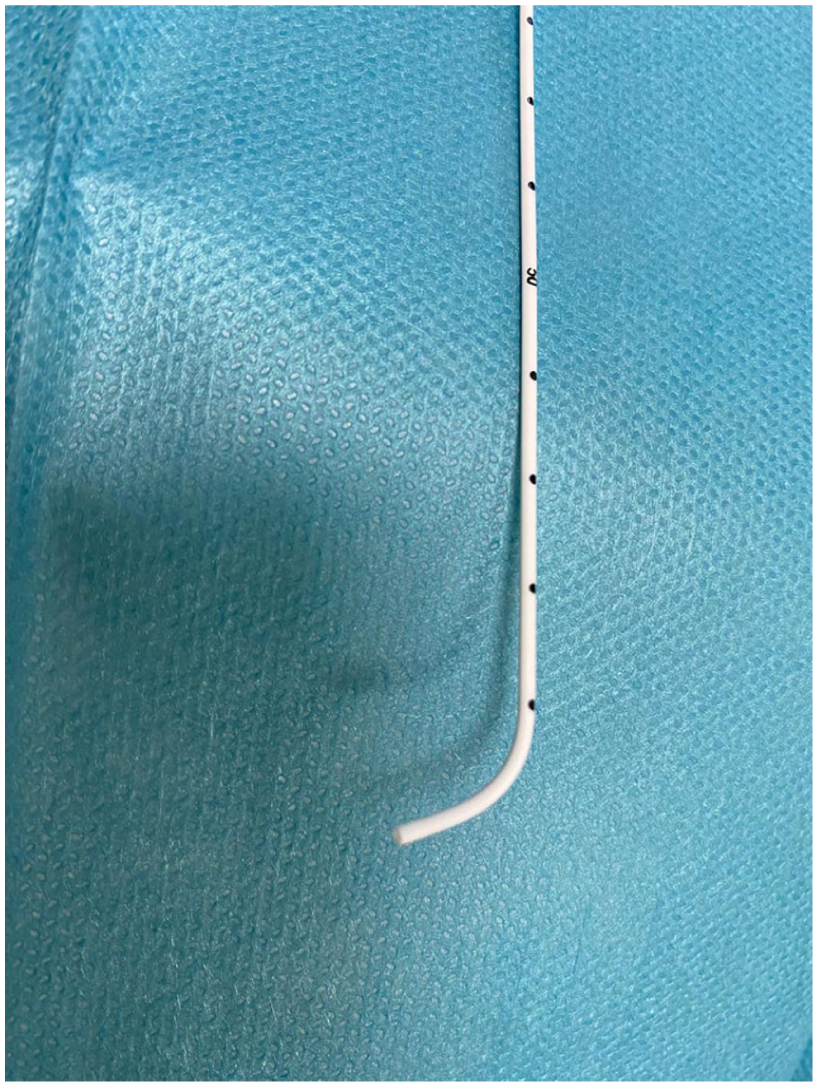
Preparation of the guidewire-assisted femoral PICC insertion technique. The original internal stylet of the 4–5 Fr, 55 cm PICC is removed and replaced with a 0.035″ × 70 cm J-tip metallic guidewire. At this stage, the J-tip is kept entirely within the distal lumen of the catheter, without protruding beyond the tip.
The catheter–guidewire assembly is then advanced through the microintroducer. During the first ~15–20 cm of progression—corresponding anatomically to advancement from the superficial femoral vein toward the common femoral and iliac veins—the guidewire remains completely contained within the catheter lumen. In this phase, the presence of the 0.035″ metallic core increases longitudinal rigidity, reduces the tendency to buckle or undergo accordion-like shortening, and improves transmission of forward force across venous valves and venous curvatures. Advancement is performed gently and without force while maintaining awareness of insertion depth.
Once ~15–20 cm have been inserted and the catheter tip is presumed to lie within the common iliac vein, the guidewire is gently advanced ~2 cm beyond the distal tip of the catheter (Figure 2). The J-tip now protrudes minimally and becomes the leading element of the system. Further progression toward the inferior vena cava is carried out slowly and without force. The curved J-tip reduces the likelihood of inadvertent engagement into narrow collateral branches because its rounded configuration makes entry into small-caliber vessels mechanically less favorable. At the level of the iliocaval confluence, its curvature may promote deflection away from posteriorly oriented tributaries, particularly the ascending lumbar vein. At the same time, its atraumatic profile and wider radius tend to favor continuation along the main venous axis, facilitating alignment with the larger-caliber inferior vena cava rather than diversion into smaller collateral pathways.
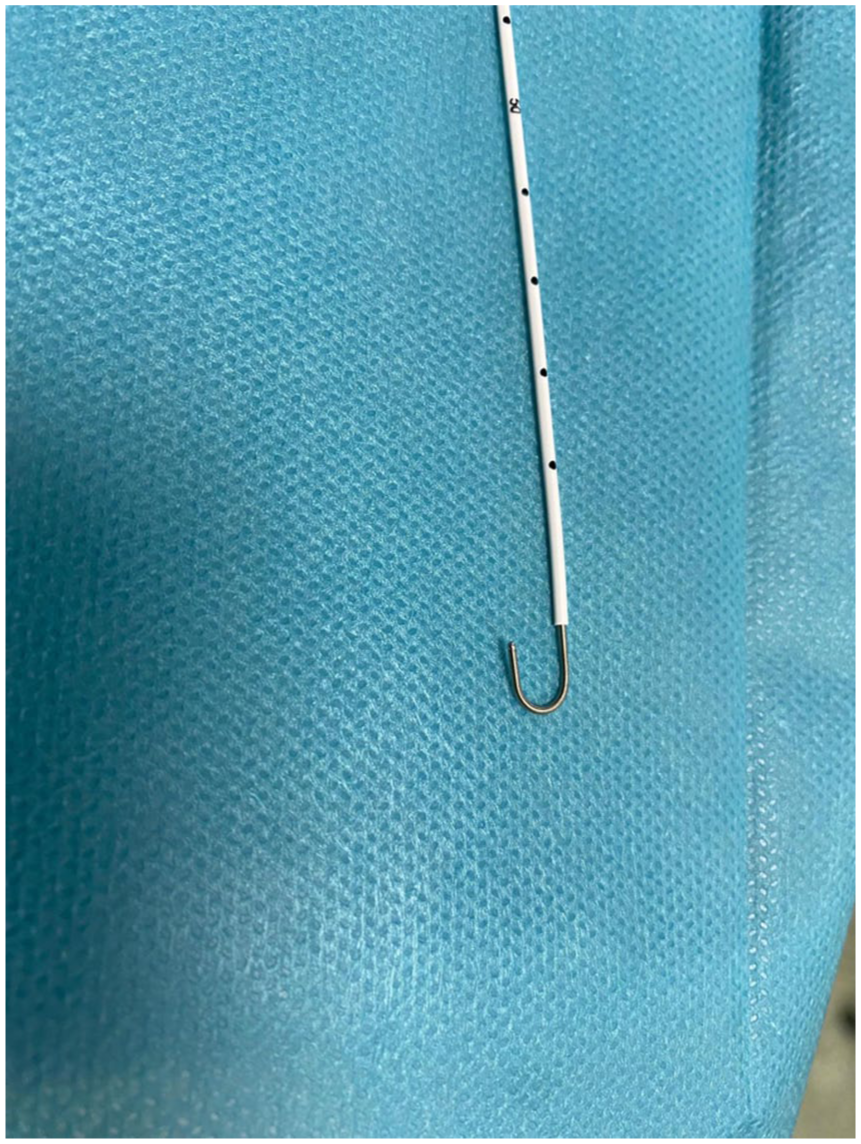
J-tip-led iliocaval navigation. After ~15–20 cm of catheter advancement—corresponding to presumed positioning within the common iliac vein—the guidewire is gently advanced about 2 cm beyond the catheter tip. The minimally protruding J-tip becomes the leading element of the system, facilitating alignment with the inferior vena cava.
Particular attention must be paid to the length of the external catheter segment. When using 55 cm PICCs with an external extension of ~15 cm, it may not be possible to advance the 70 cm guidewire sufficiently to allow the J-tip to protrude beyond the catheter tip, since the wire length is essentially equal to that of the catheter. Therefore, it is preferable to use PICCs with a shorter external segment (typically around 11 cm) or to shorten the distal portion of the catheter by ~3 cm. Care must also be taken to avoid inserting the entire guidewire into the external extension segment, as this may make retrieval difficult without removing the catheter.
This issue does not arise when using trimable catheters, as the extension tubing is connected only after catheter insertion. The same applies to FICC-ports, which are cut to size after placement. However, in such cases, the total catheter length must be carefully considered, since these devices are typically 70 cm long and may fully accommodate the guidewire. As a precaution, shortening the distal portion of the catheter by ~5 cm ensures that the guidewire remains longer than the catheter.
After satisfactory advancement has been achieved, the guidewire is withdrawn and final tip position is confirmed intraprocedurally using ultrasound-based techniques. Transhepatic visualization of the subdiaphragmatic inferior vena cava, with or without bubble test, is recommended in accordance with current consensus statements.5,6,19 The maneuver described here is intended exclusively to facilitate catheter navigation and does not replace ultrasound-based tip location, which remains mandatory before clinical use of the device.
Results
This maneuver has been progressively adopted in our unit in situations where advancement of long 4–5 Fr femoral catheters proved technically challenging, as well as in patients with a history of previous femoral insertions complicated by maldirection.
From a procedural perspective, several consistent observations emerged. First, the catheter–guidewire assembly demonstrated improved pushability, with greater axial stability during advancement and more effective transmission of forward force. Second, kinking phenomena were not observed: the typical accordion-like shortening or buckling that may occur during iliac progression with highly flexible catheters appeared to be minimized. Third, the transition at the iliocaval confluence seemed smoother; when the J-tip was allowed to protrude minimally beyond the catheter tip, progression toward the inferior vena cava appeared more linear and required fewer corrective manipulations.
Finally, although this assessment is necessarily subjective, resistance suggestive of posterior deviation into collateral pathways was encountered less frequently, suggesting a reduced tendency toward lumbar maldirection.
No insertion-related vascular injury attributable to the maneuver was observed. In all cases, final catheter position was confirmed by ultrasound-based tip location before clinical use.
Discussion
Although femoral catheterization is generally regarded as a technically straightforward procedure, the advancement of long, small-caliber catheters along the iliac–caval axis is not invariably simple. The anatomical relationship between the common iliac vein and the ascending lumbar vein creates a potential route for maldirection, particularly when highly flexible devices are used. At the level of the iliocaval confluence, subtle variations in angulation and vessel geometry may favor posterior deviation rather than direct progression into the inferior vena cava.
The ascending lumbar vein originates from the common iliac vein at a relatively small angle and courses posteriorly, running parallel to the inferior vena cava. In this anatomical context, a soft catheter tip may be deflected posteriorly, especially when forward force is applied without sufficient axial support. This mechanical vulnerability likely contributes to the observation that small-bore and highly flexible catheters are disproportionately represented among reported cases of ALV malposition.6–18
The technique described in this report seeks to address this issue through two complementary mechanical effects. First, the temporary introduction of a 0.035″ guidewire within the catheter lumen increases longitudinal stiffness. Compared with standard internal stylets supplied with 4–5 Fr devices, the larger metallic core of the 0.035″ guidewire enhances bending resistance and improves transmission of forward force, thereby reducing the likelihood of tip deflection at bifurcations or angulated segments.
Second, when the guidewire is advanced 2–3 cm beyond the catheter tip, the curved J-tip acts as a navigation element. Its rounded configuration distributes contact pressure over a broader surface and makes entry into narrow or acutely angled collateral veins mechanically less favorable. At the same time, its curvature tends to favor alignment with the larger-caliber inferior vena cava, rather than continuation into posterior tributaries such as the ascending lumbar vein.
Importantly, this maneuver does not eliminate the need for proper tip location. As documented in several reports,5–18 adequate aspiration and infusion through the catheter do not exclude ALV malposition. Only ultrasound-based confirmation—preferably visualization of the catheter in the subdiaphragmatic IVC and/or synchronous appearance of microbubbles during bubble test—can reliably confirm correct positioning.5,19
The present report should be interpreted as a technical description supported by mechanical rationale and clinical experience rather than by formal outcome data. Prospective studies would be necessary to quantify reduction in ALV malposition rates, assess procedural time, evaluate safety in larger populations and compare this approach with standard advancement techniques.
Nevertheless, the maneuver is simple, reproducible, does not require additional dedicated devices beyond a standard 0.035″ guidewire, and integrates seamlessly with current ultrasound-based protocols.
Although one might expect that a J-tip could complicate guidewire removal, we have not encountered significant difficulties in practice. In our experience, removal of the J-tip has never resulted in catheter tip displacement or retraction. It is, however, essential to flush the catheter with saline prior to guidewire removal in order to lubricate the lumen and facilitate smooth extraction.
An effective solution to avoid the guidewire length being similar to or equal to that of the catheter, taking into account the external extension segment, would be to use a guidewire of at least 80 cm in length.
Conclusions
Advancement of 4–5 Fr, 55 cm femorally inserted central catheters may occasionally be hindered by venous valves, bifurcations, or posterior deviation into the ascending lumbar veins.
Replacing the original catheter stylet with a 0.035″ × 70 cm J-tip guidewire during insertion temporarily increases shaft rigidity and allows controlled J-tip-led navigation at the iliocaval confluence.
The deliberate choice of a J-tip guidewire is based not only on the increased stiffness provided by a larger-caliber metallic core, but also on the wider tip profile once it protrudes beyond the catheter. This configuration makes inadvertent entry into collateral veins less likely.
In our opinion, the wide curvature of the J-tip reduces the probability of entering small- to medium-caliber collateral vessels, such as lumbar veins.
This modification appears to facilitate linear progression toward the inferior vena cava and may reduce the likelihood of lumbar vein malposition.
Future efforts will focus on identifying longer guidewires. Ideally, this technique should be performed using guidewires longer than 80 cm to avoid the described constraints.
Ultrasound-based tip confirmation remains mandatory.
There are some limitations that may restrict the applicability of this technique. A 0.035″ guidewire cannot be used with 5 Fr double-lumen PICCs, as the internal lumen is insufficient to accommodate the wire. This limits the use of the technique in clinical situations where a double-lumen device is required. An alternative could be the use of 0.018″ nitinol micro-guidewires, available in lengths of 70–80 cm. These wires offer excellent flexibility, shape memory, and atraumatic tips, which could potentially allow even smoother and more controlled catheter advancement along the venous axis. However, in the authors’ opinion—yet to be confirmed by further study—such smaller wires may not provide the same protective effect against inadvertent entry into small collateral veins as the J-tip configuration.
This aspect requires further investigation and validation in a larger clinical series.
Further prospective evaluation is warranted to validate the clinical impact of this technique.
Footnotes
Author contributions
Benv.S conceived the technique and was the first to apply it in clinical practice. PC, ZF, SB, PE, CL, and Bor.A repeatedly applied the technique, contributing to the evaluation of its benefits and potential risks. Benv.A drafted the manuscript in English. BD prepared the photographic material and figure captions. FC coordinated all research activities. All authors contributed, according to their respective roles, to the drafting of the scientific manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Consent from the patients was obtained; the study does not require specific ethical approval, as it involves a minor modification of a technique, that is, already well described and established in the existing literature.