
Abstract
Surgical management of perianastomotic venous collaterals during the creation of vascular access remains a critical yet often overlooked step. Traditionally, these branches are ligated to optimize hemodynamics and direct the entire flow into the primary venous outflow tract. However, pathophysiological analysis suggests that this practice may limit the overall resilience of the access. Perianastomotic collaterals serve a functional role as essential compensatory outflow pathways; in the presence of stenosis or obstruction of the primary venous segment, their patency maintains blood flow, reduces resistance, and prevents stagnation. Systematically preserving these branches, rather than ligating them, can significantly delay the onset of thrombotic events and ensure the functional survival of the access even if the main outflow fails. This “conservative” hemodynamic approach proposes a paradigm shift in surgical strategy, prioritizing vascular redundancy to improve long-term patency and minimize the need for complex salvage interventions.
Keywords
Introduction
Vascular access dysfunction remains a major determinant of morbidity in patients undergoing hemodialysis. Native arteriovenous fistulae (AVFs) are considered the preferred option; however, arteriovenous grafts (AVGs) and complex accesses are frequently required due to unfavorable vascular anatomy or prior access failure. 1
The majority of research has focused on the identification and treatment of venous outflow stenosis, which represents the primary cause of access dysfunction and thrombosis. 2 In contrast, limited attention has been devoted to adaptive mechanisms that develop in response to these hemodynamic alterations.
We conducted a literature review on surgical techniques in the creation of hemodialysis prostheses.
A review analyzes the role of prostheses, highlighting the importance of the anastomosis technique, to reduce intimal hyperplasia and the options for thrombosis management. 3
We found a detailed analysis of the causes of failure, including the management of outflow venous stenosis through PTA and the role of surgery in cases where angioplasty fails. 4
We found recommendations on clinical practice (size of target vein, shape of anastomosis, angle of approach, distance from venous needling, trauma to the target vein). 5
We did not find relevant technical suggestions that evaluate the management of venous collaterals in venous anastomosis of grafts for hemodialysis.
Among these, perianastomotic venous collaterals are commonly observed during surgical creation of the graft–vein anastomosis, and these collateral veins are frequently ligated to facilitate anastomotic construction and to promote preferential drainage through the primary venous outflow. 6
However, in other vascular territories, collateral circulation is widely recognized as a compensatory and protective mechanism.7,8 A similar paradigm may apply to hemodialysis access, where high-flow conditions and progressive outflow obstruction create a unique hemodynamic environment.
This review aims to redefine the role of perianastomotic venous collaterals, highlighting their potential protective function and proposing a clinically oriented strategy focused on their preservation.
Pathophysiological basis
The development of venous collaterals in arteriovenous access is primarily driven by hemodynamic stress. Outflow stenosis leads to increased venous resistance, elevated intraluminal pressure, and redistribution of flow toward alternative pathways. 9
Under these conditions, pre-existing venous channels dilate and remodel, forming collateral pathways that bypass the stenotic segment. This process is mediated by endothelial activation, shear stress alterations, and vascular remodeling mechanisms similar to those observed in arterial collateralization.10,11
From a functional perspective, this phenomenon can be interpreted as a decompression mechanism, allowing pressure relief within the access circuit. By providing alternative drainage routes, collaterals may reduce venous hypertension and preserve effective blood flow (Figure 1).

Protective hemodynamic role of venous collaterals.
In the context of high-flow arteriovenous access, these adaptive responses are amplified, making collateral development a key component of the overall hemodynamic balance.
Hemodynamic role of perianastomotic collaterals
The functional impact of venous collaterals is not uniform and depends on their contribution to overall flow dynamics.
Beneficial collaterals
In many cases, collaterals act as compensatory pathways that:
Reduce venous pressure
Maintain adequate outflow
Preserve dialysis efficiency
Delay thrombosis
These vessels function as a “safety valve,” protecting the access from the hemodynamic consequences of progressive stenosis and thrombosis.
Detrimental collaterals
Conversely, some collaterals may:
Divert blood flow away from the main circuit
Reduce effective dialysis flow
Increase recirculation
Contribute to local symptoms such as edema
Dynamic balance
Importantly, collateral function is dynamic. The same vessel may initially be beneficial but become detrimental if it dominates flow distribution. This duality highlights the importance of individualized hemodynamic assessment.
Limitations of current practice
Current management strategies are predominantly lesion-driven, focusing on the detection and correction of stenosis. In this framework, collaterals are often considered secondary or even undesirable findings. 12
This approach may lead to:
Underestimation of their functional role
Suboptimal hemodynamic outcomes
Early thrombosis
Toward a hemodynamic approach
We propose a shift toward a functional and hemodynamic model, in which perianastomotic collateral veins are not ligated if possible, because their preservation is favored when collaterals contribute to effective drainage.
Our experience
In the absence of a clear indication from the literature, our protocol for the venous anastomosis preparation (in prosthetic vascular accesses) provides the sparing of the perianastomotic venous collaterals.
We analyzed 69 grafts from 2020 to 2025 in our center, in 13 cases, approximately 20% of cases, we witnessed a phenomenon of complete occlusion of the venous outflow, but with patency of the graft although with increased venous pressures and decreased flow rate, guaranteed by the hypertrophy of the perianastomotic draining collaterals. Our theory is that if we had tied the anastomotic collaterals the graft would have thrombosed.
Despite a theoretical risk of low-flow vascular access due to the presence of collaterals and not a single outflow, we did not have any cases in which it was necessary to tie off collaterals post-procedure to promote venous drainage.
In this representative clinical case we have a patient (M, 46 yo) with a prosthetic vascular access in the left upper limb, between the brachial artery and the axillary vein, who developed progressively increasing venous pressures. Clinically, a thrill was still appreciable, although reduced in intensity. Duplex ultrasound demonstrated graft patency, with evidence of venous outflow stenosis at the level of the axillary vein and an access flow of approximately 700 mL/min. A strategy of close surveillance was therefore adopted, deferring intervention for the identified stenosis.
During follow-up, after approximately 2 months, a marked increase in venous pressures was observed. The thrill remained clinically detectable, although diminished. Duplex ultrasound confirmed continued graft patency, with a reduced access flow of approximately 300 mL/min.
Subsequent phlebography revealed occlusion of the primary venous outflow at the level of the axillary vein. However, graft patency was preserved by perianastomotic collateral circulation, which provided sufficient venous outflow and prevented graft thrombosis.
The lesion was treated with predilation (7 × 80 mm, Dorado 6 × 20 mm) followed by percutaneous transluminal angioplasty using a high-pressure drug-coated balloon (Aperto7 × 40 mm), restoring primary venous outflow and ensuring optimal graft function.
In this illustrative case, perianastomotic collateral vessels, despite occlusion of the primary outflow, prevented graft thrombosis (Figures 2 and 3).
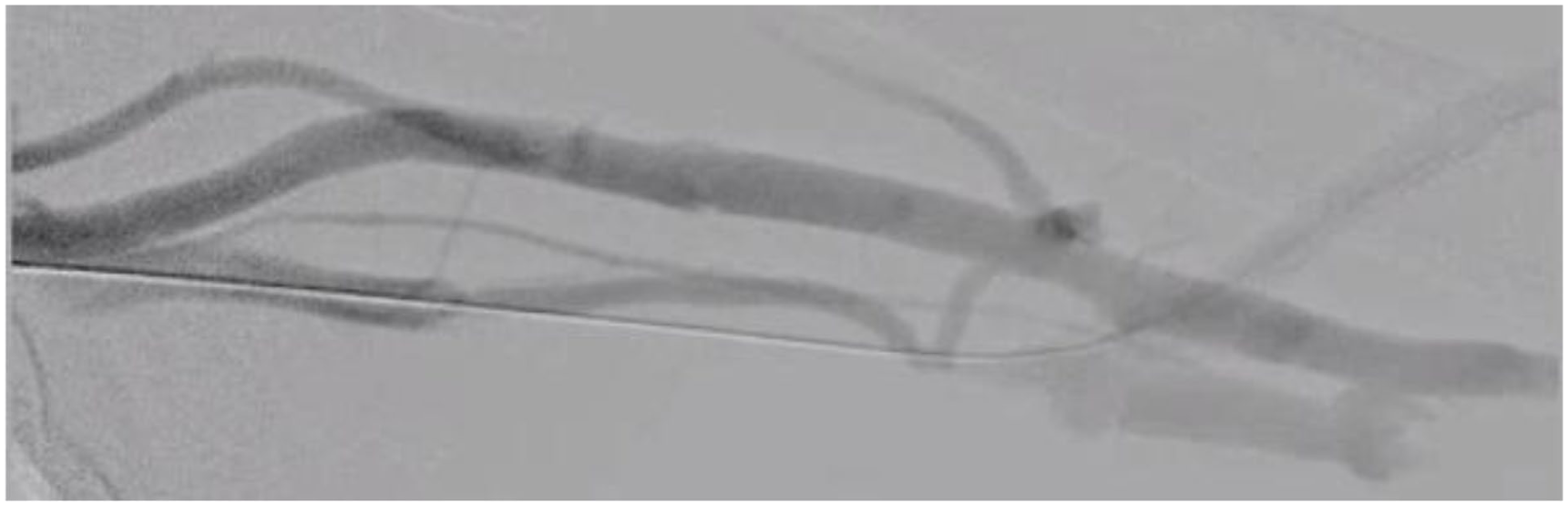
Pre-procedural phlebography.

Final phlebography.
Discussion
During the creation of prosthetic venous anastomoses, collateral veins of the primary venous outflow are frequently ligated to facilitate anastomotic construction and achieve hemostasis. However, the contribution of these vessels to long-term hemodialysis access patency is often underappreciated, unlike the creation of native vascular accesses, in which the perforating vein or collaterals are ligated to facilitate outflow into the superficial venous circulation and not into the deep one.
Preservation of perianastomotic venous collaterals may provide an alternative outflow pathway in the setting of primary outflow stenosis, thereby mitigating the risk of graft thrombosis and supporting sustained access patency. Even in cases of primary venous outflow occlusion, collateral pathways may provide sufficient drainage to prevent graft thrombosis. In fact in these cases, collaterals represent the dominant outflow pathway, and their absence may precipitate acute access failure.
In this setting, surveillance strategies—including intradialytic venous pressure monitoring, clinical assessment, duplex ultrasound evaluation of the graft, and access flow measurement—are essential to guide the timing of intervention for outflow stenosis.
Conclusions
Perianastomotic venous collaterals in AVGs represent critical components of the adaptive venous outflow system in hemodialysis access. Their preservation may maintain access function and delay thrombosis. A shift toward a hemodynamic, function-oriented approach may improve clinical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.