
Abstract
Arterio-arterial grafts (AAG) represent a specialized type of vascular access. However, AAG is associated with a high incidence of thrombotic occlusion, which prompted us to improve this surgical approach. The improved technique involves creating a low-flow autologous arteriovenous fistula (AVF) at the distal end of the AAG, termed improved AAG (IAAG). We report a case of a 65-year-old female patient with recurrent thrombosis of her AAG, who underwent creation of a low-flow autologous arteriovenous fistula (AVF) at the distal end of the AAG. The patient was followed up for 15 months postoperatively, and the intervention frequency was significantly lower than that before the operation. This case demonstrates that the IAAG surgical technique can prolong the patency of AAG.
Keywords
Introduction
Currently, there are three main types of vascular access for hemodialysis patients: autologous arteriovenous fistula (AVF), arteriovenous graft (AVG), and central venous catheter (CVC). With the increasing number of hemodialysis patients and the prolongation of dialysis vintage, many patients face exhausted peripheral venous resources, central venous occlusion, and other conditions that prevent the creation of AVF or AVG, and even CVC placement. In such cases, an arterio-arterial graft (AAG) can be established to provide vascular access for hemodialysis.1–4 However, AAG is associated with a high incidence of thrombosis and occlusion, and once this occurs, patients are left in the predicament of being unable to undergo dialysis. Thrombosis may be related to slow blood flow velocity within the AAG graft and repeated puncture injuries. To address the high thrombotic risk associated with AAG, we attempted to increase the blood flow velocity in the graft for patients with AAG. The surgical technique involves creating a low-flow AVF at the distal end of the AAG. We refer to the procedure combining AAG with the creation of a low-flow AVF at its distal end as the improved AAG (IAAG). We report a case of recurrent thrombosis after AAG surgery, in which IAAG was established.
Case report
The patient was a 65-year-old Asian female on chonic hemodialysis for 4 years. She had a 20-year history of hypertension and a 20-year history of type 2 diabetes mellitus. The patient initiated hemodialysis in 2021. Due to the slender veins in both upper extremities, multiple attempts to create an AVF were unsuccessful. The patient had no history of hematological diseases or hyperlipidemia. Coagulation tests and platelet counts were within normal limits. Therefore, non-vascular causes for repeated AVF failure were excluded. Hemodialysis was done via a right internal jugular vein tunneled central venous catheter (TCC). She underwent thrombolytic therapy and catheter replacement multiple times for TCC dysfunction, with catheter replacement occurring on average every 6 months; however, recurrent TCC dysfunction persisted.
In January 2024, the patient was admitted to our hospital again due to catheter dysfunction. Central venous CTA revealed a right internal jugular vein TCC is appropriately positioned with the catheter tip located in the right atrium, and severe stenosis of the superior vena cava. As conventional vascular access could not be established, we created a left upper arm brachial artery-brachial artery AAG (type α) for the patient. Surgical procedure: (1) Routine preoperative preparation, regional nerve block anesthesia; (2) Longitudinal skin incisions were made near the axilla and above the elbow, the proximal and distal brachial arteries were dissected respectively, and an “α-shaped” subcutaneous tunnel was created; (3) A 6 mm diameter prosthetic vascular graft was placed into the tunnel, blood flow of the brachial artery was occluded, and the prosthetic graft was anastomosed end-to-side to the distal end and proximal end of the brachial artery respectively; (4) After completion of the anastomoses, the brachial artery proximal to the distal anastomosis was ligated with a 1 cm segment of prosthetic vascular graft, and the vascular clamps were released; (5) The subcutaneous tissue and skin were closed layer by layer (See Figure 1). Hemodialysis via the AAG as the vascular access was initiated 2 weeks postoperatively.
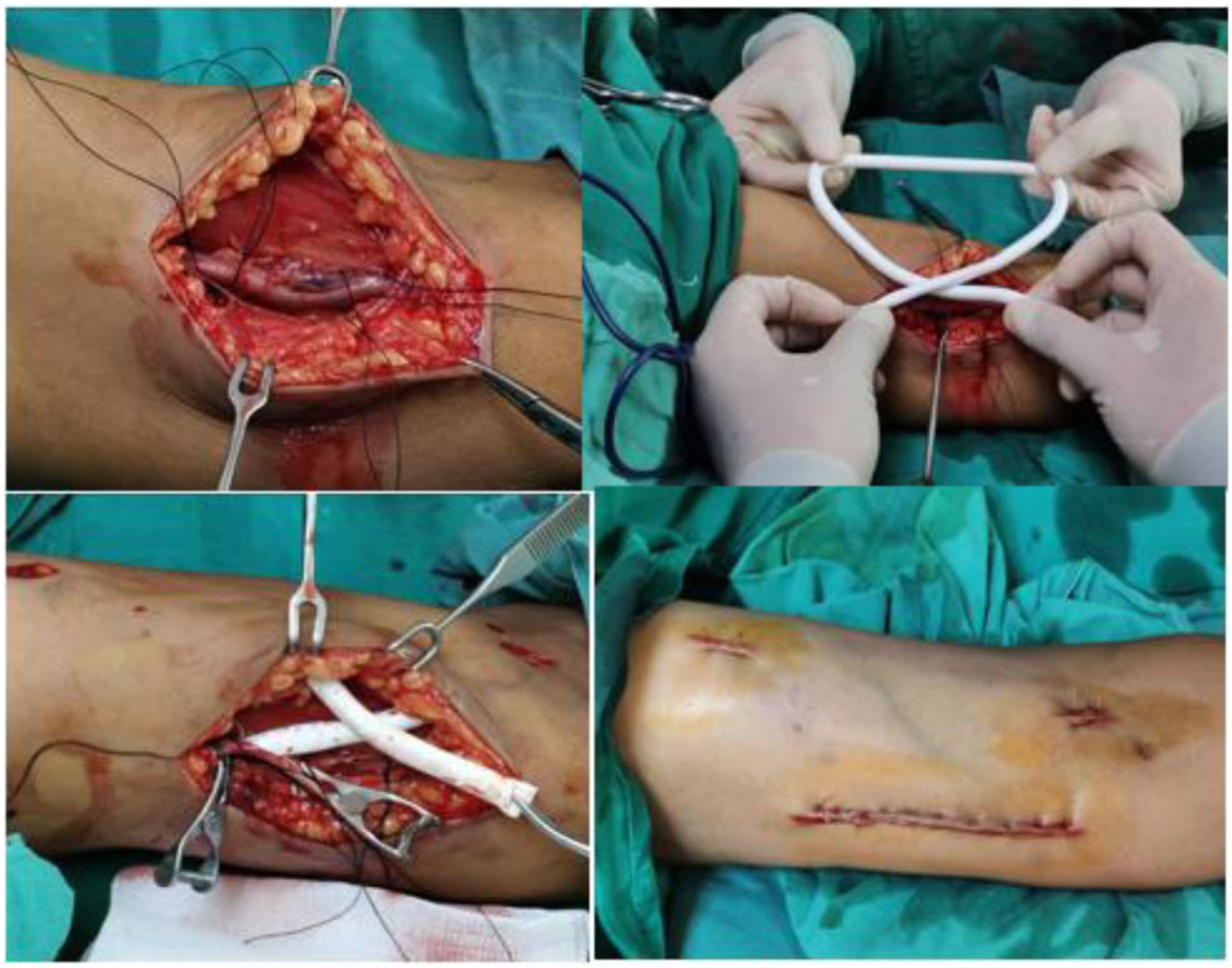
Intraoperative photographs
In April 2024, the patient experienced poor flow during puncture of the AAG while undergoing routine dialysis at a local hospital. Ultrasonography revealed intimal hyperplasia of the AAG with mural thrombosis. She was admitted to our hospital and underwent thrombectomy via left AAG incision combined with percutaneous transluminal angioplasty (PTA). The AAG remained patent postoperatively and continued to be used for dialysis.
In June 2024, the patient developed difficult hemostasis of the left upper extremity AAG after dialysis, and diminished pulsation was noted following compressive hemostasis. Local ultrasonography indicated AAG thrombosis with luminal stenosis, and the patient presented to our hospital again. Vascular access ultrasound revealed a blood flow velocity of 102.67 cm/s in the brachial artery proximal to the AAG, and 45.72 cm/s within the AAG itself. Mural thrombosis was observed in the AAG puncture zone, with a residual lumen of less than 30% (see Figure 2).
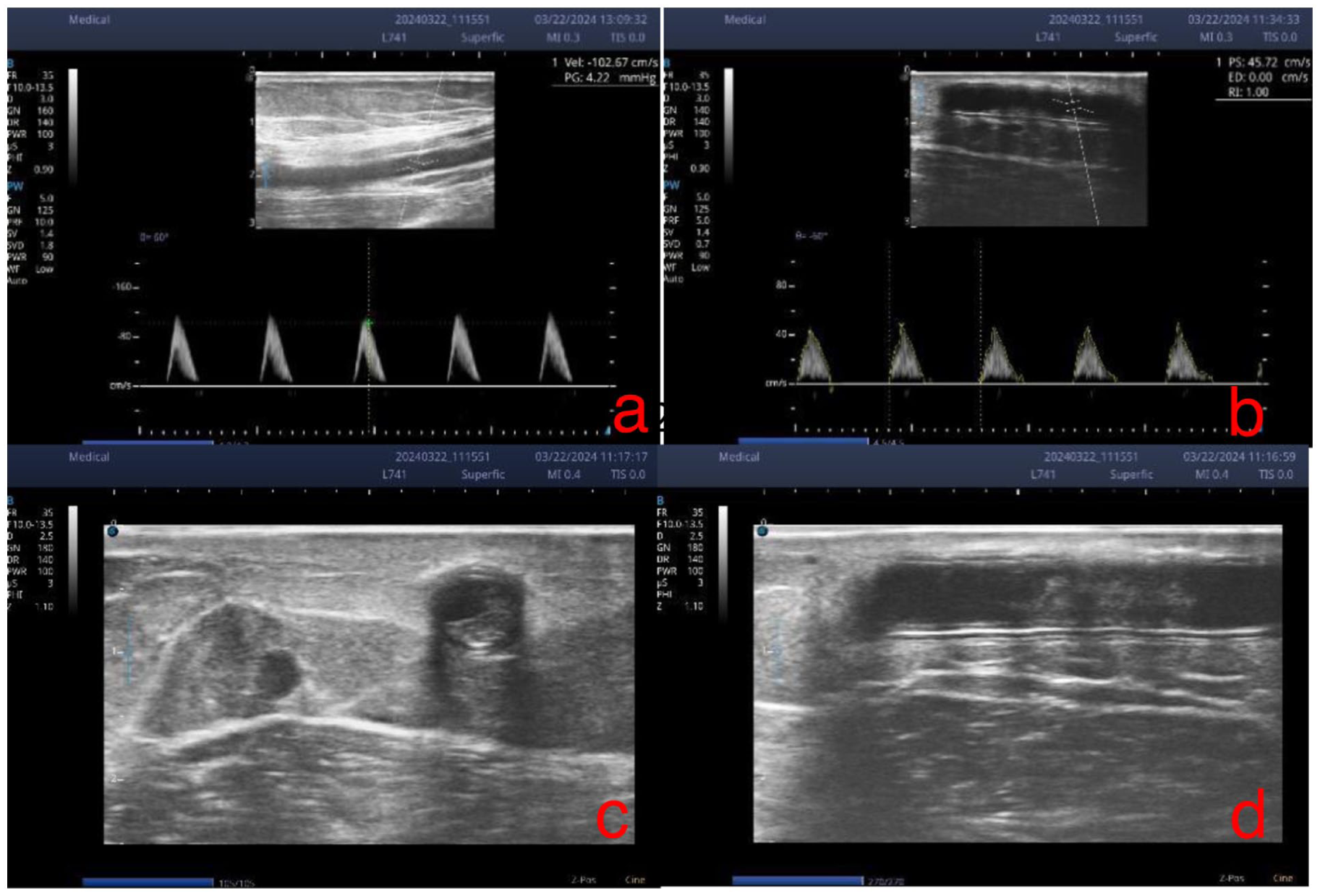
Ultrasonography: (a) blood flow velocity in the brachial artery proximal to the AAG was 102.67 cm/s, (b) blood flow velocity within the AAG was 45.72 cm/s, and (c) short-axis ultrasound showing mural thrombosis in the lumen of the AAG puncture zone, with residual lumen < 30%.
The patient had experienced two episodes of intraluminal graft thrombosis within 5 months; to reduce the thrombotic rate, we planned to establish an IAAG for the patient, the schematic diagram is presented in Figure 3. Evaluation of the left upper extremity vessels showed that the internal diameter of the brachial artery distal to the AAG was 3.0 mm, and the internal diameter of the basilic branch of the median cubital vein was 1.5 mm after tourniquet inflation. A low-flow brachial artery-basilic branch of the median cubital vein AVF could be created at the distal end of the AAG. The strategy for managing AAG thrombosis was consistent with previous management, namely open thrombectomy combined with PTA. The planned treatment regimen was AAG open thrombectomy combined with PTA, concurrent with creation of a brachial artery-basilic branch of the median cubital vein AVF at the distal end of the AAG. Surgical steps were as follows: (1) Following regional nerve block anesthesia, a transverse skin incision was made at the elbow, and approximately 1.5 cm of the graft was dissected. The anterior wall of the graft was incised after vascular clamping. A guidewire assisted by a 5.5F thrombectomy catheter was introduced into the AAG via the incision to retrieve thrombus from both the downstream and upstream segments of the incision, removing thrombus and hyperplastic tissue. (2) A guidewire and balloon were passed across the stenotic lesion, and percutaneous transluminal angioplasty was performed using 6 mm and 7 mm high-pressure balloons respectively. Post-procedure imaging demonstrated that the stenosis within the graft was largely corrected and the thrombus had resolved. (3) A longitudinal incision of the skin and subcutaneous tissue was made 1.5 cm below the elbow crease at the distal end of the AAG. The basilic branch of the median cubital vein (3 cm) and the brachial artery (3 cm) were dissected. A 4 mm arteriotomy was created on the brachial artery, and an end-to-side anastomosis between the basilic branch of the median cubital vein and the brachial artery was performed using 7-0 vascular sutures. After completion of the anastomosis, venous and arterial clamps were released sequentially; patent flow in the fistula was confirmed, and a palpable thrill was detected locally. After adequate hemostasis, the prosthetic graft was closed, and the skin was sutured layer by layer.
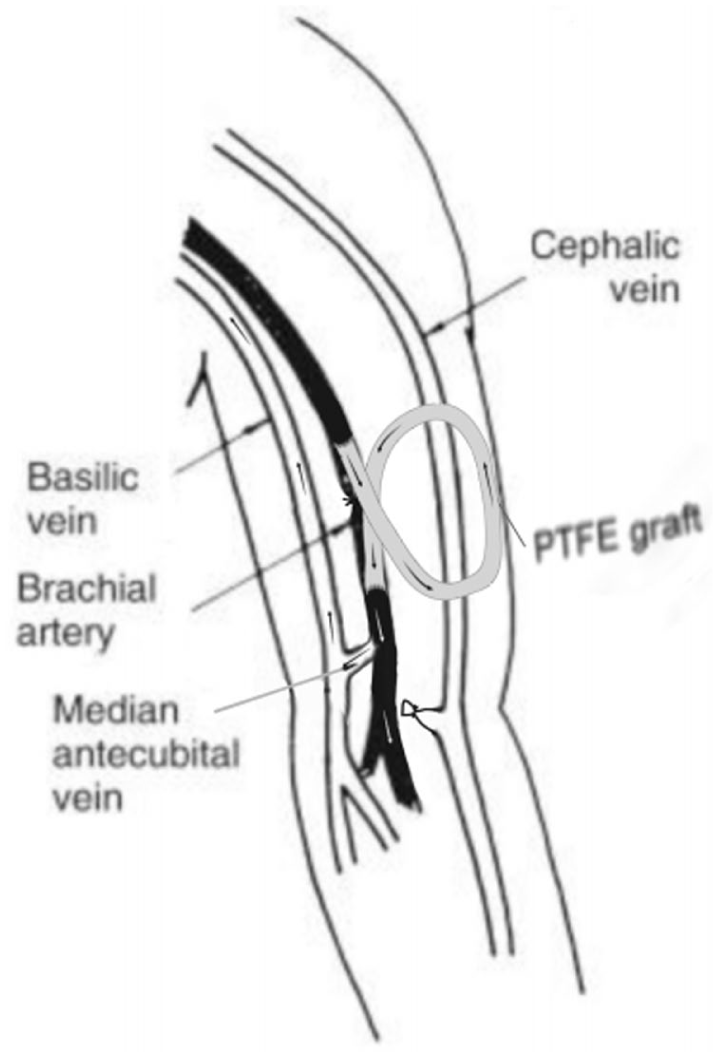
Schematic diagram of the improved arterio-arterial graft (IAAG).
Postoperative follow-up: On postoperative day 2, the patient began hemodialysis via puncture of the AAG, and the procedure was uneventful. Telephone follow-ups were conducted at 3 and 6 months postoperatively, during which the patient reported no swelling of the head, neck, or access-side extremity, adequate dialysis blood flow, normal venous pressure, and uneventful use of the vascular access. At 9 months postoperatively, the patient attended our clinic for follow-up. Physical examination of the access showed no swelling of the head, neck, or access-side extremity; palpable pulsation of the graft, with strength equal to that of the contralateral brachial artery; no thrill was palpable over the AAG anastomotic site, but a bruit was audible.(see Figure 4). Ultrasonographic examination revealed patent lumens of the brachial artery proximal to the AAG, the proximal anastomosis, the distal anastomosis, and the brachial artery distal to the AAG. There was anterior wall damage of the graft in most of the AAG puncture zones, mild intimal hyperplasia in one puncture zone with a small amount of mural thrombosis, and a residual lumen > 70%. The vessel diameter in non-puncture zones was normal, and the blood flow of the brachial artery was 244.9 ml/min (see Figure 5).

No swelling of the head and neck, and no swelling of the access-side extremity.
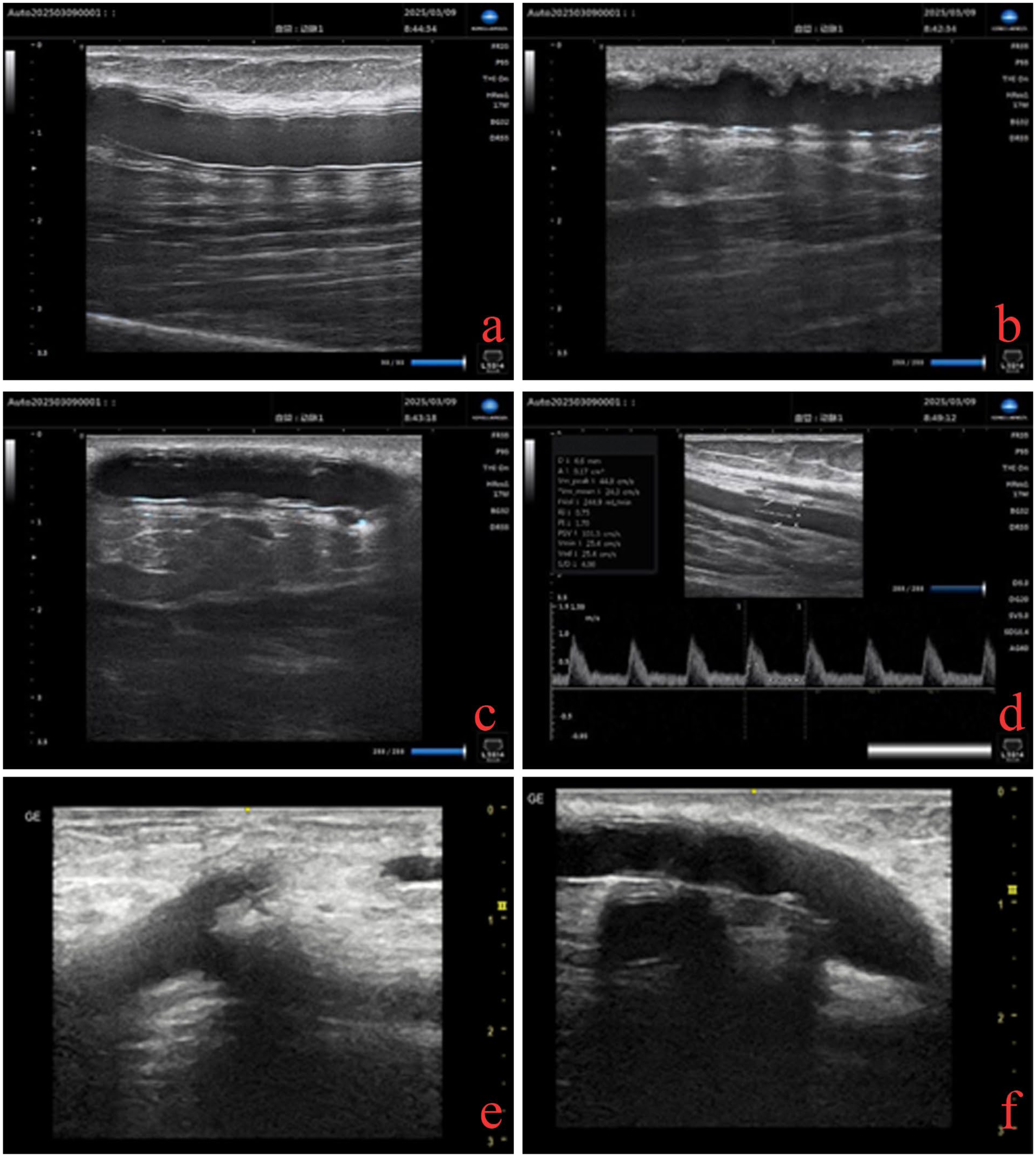
(a) Patent lumen in the non-puncture zone of the AAG, (b) anterior wall damage of the graft in the AAG puncture zone, with patent lumen, (c) a small amount of mural thrombosis in the AAG puncture zone, residual lumen > 70%, (d) brachial artery blood flow was 244.9 ml/min, (e) AVF anastomosis, and (f) AVG distal anastomosis.
At the 12-month routine follow-up in the vascular access monitoring clinic, the patient was found to have hyperplasia and stenosis in the AAG puncture zone, combined with stenosis of the draining vein of the distal brachial artery AVF, as well as a small amount of mural thrombosis within the graft. Percutaneous transluminal angioplasty was performed on both the AVF and AAG, after which the stenotic lesions were corrected. The blood flow in the brachial artery proximal to the AAG was measured at 432.66 ml/min. At the 15-month telephone follow-up, the patient continued hemodialysis using the IAAG with uneventful procedures. The pump-controlled blood flow rate was set at 230 ml/min, the measured venous pressure was 170–210 mmHg, and the online Kt/V was 1.35. And the hemostasis time after dialysis was approximately 30 min. No swelling of the patient’s head, face, or extremities was noted. The patient remains under ongoing follow-up.
Discussion
As a vascular access for hemodialysis, AAG is indicated for dialysis patients in whom AVF or AVG cannot be created due to conditions such as central venous occlusion, severe heart failure, exhausted peripheral veins, and distal limb ischemia associated with arteriovenous fistulas. According to the literature, its 6- and 12-month patency rates are not inferior to those of AVG.5–7 Among 13 AAG cases at our center, mural thrombosis in AAG was frequently observed; in particular, thrombosis and intimal hyperplasia in the puncture zone represent the major complication and the primary cause of AAG dysfunction. 1 Analysis suggests that this is related to slow blood flow velocity within the AAG graft, combined with repetitive dialysis puncture injuries.
The literature reports that the criterion for AAG creation is a brachial artery blood flow velocity ⩾ 50 cm/s, and AAG should be established with caution in patients with low brachial artery blood flow velocity. 5 This is because slow brachial artery blood flow may compromise dialysis adequacy and increase thrombotic risk. The frequent thrombotic episodes in this patient after AAG creation were considered to be attributable to the slow blood flow velocity within the AAG. Studies have shown that brachial artery diameter and blood flow increase over time following AVF creation.8,9 Therefore, we hypothesized that creating a low-flow AVF distal to the AAG could increase blood flow velocity within the AAG and reduce thrombotic risk, and we refer to this surgical technique as IAAG (as shown in Figure 3).
Establishment of a low-flow AVF at the distal end of the AAG can significantly accelerate blood flow within the graft and promote physiological dilation of the feeding artery. This mechanism is well supported by hemodynamic and biological principles. The newly constructed venous outflow tract remarkably reduces the overall circulatory resistance. The decreased resistance leads to increases in blood flow volume and velocity, which accelerates and stabilizes blood perfusion in the AAG, alleviates blood stasis, and reduces the risk of thrombosis. Meanwhile, elevated blood flow velocity increases vascular wall shear stress and activates the mechanotransduction pathway in vascular endothelial cells, thereby inducing vascular smooth muscle relaxation, extracellular matrix remodeling, and adaptive arterial dilation. 10 This serves as the biophysical basis for the improved patency rate of the IAAG technique. Studies have verified that AVF creation establishes a low-resistance venous outflow tract, rapidly increasing brachial arterial blood flow from a preoperative baseline of 65 ± 42 to 448 ± 213 ml/min in radial-cephalic AVFs. 10 For brachial-basilic AVFs, the brachial arterial blood flow reaches 1450 ± 221 ml/min at 3 months after surgery. 8 Following AVF creation, brachial arterial blood flow velocity is markedly elevated. It is hoped that this approach can address the problem of recurrent thrombosis in AAG.
At our center, brachial artery transposition has been performed in several cases. However, this surgical procedure has specific requirements for the internal diameter of the brachial artery. Most studies recommend that the brachial artery diameter should be greater than 4 mm, with a minimum cutoff of 3.0 mm. 11 The patient had a brachial artery diameter of only 3.0 mm, complicated by vascular calcification and poor vessel wall elasticity. Based on our clinical experience, such an artery is difficult to puncture even after transposition. Furthermore, repeated puncture may damage the arterial structure and cause complications including aneurysm and arterial rupture. In addition, the short length of the transposed artery limits the puncture interval, increases the access recirculation rate, and consequently leads to inadequate dialysis. We have also added to the Discussion section the rationale for choosing the IAAG technique rather than brachial artery superficialization.
This patient was unable to create an AVF due to slender peripheral veins, and suffered from recurrent dysfunction of the right internal jugular TCC accompanied by severe superior vena cava stenosis. For these reasons, a left upper arm AAG was constructed. Because the patient experienced two episodes of intraluminal graft stenosis with mural thrombosis within 5 months after AAG placement, an IAAG was subsequently created. The blood flow of the AVF does not need to meet the guideline-recommended standard; a flow rate of approximately 200–500 ml/min is sufficient to increase blood flow velocity within the AAG and prolong its patency. Meanwhile, the patient had severe superior vena cava stenosis. Therefore, attention should be paid to swelling of the head, neck, and upper extremity caused by impaired venous return, and excessively high fistula flow should be avoided.
No swelling was noted in the access-side limb of patients after IAAG surgery; the AAG had good pulsation, a bruit was auscultated over the AVF, and the brachial artery blood flow measured by ultrasound was 244.9 ml/min. Although this was far below the criterion of >500 ml/min for a mature AVF, 12 it represented a significant increase compared with the preoperative brachial artery blood flow. The first episode of AAG luminal stenosis with mural thrombosis occurred at 12 months after IAAG creation, indicating a marked improvement in the primary patency rate of the IAAG. Following PTA, blood flow within the AVF increased, and the blood flow in the brachial artery proximal to the AAG was measured at 432.66 ml/min post-procedure. A small-diameter balloon (4 mm) was selected for PTA to avoid excessive blood flow and prevent swelling of the patient’s head, neck, and access-side extremity. At 15 months postoperatively, telephone follow-up confirmed that the patient had no swelling of the head, neck, or access-side extremity, and the vascular access functioned well. However, if excessive blood flow of the AVF subsequently causes swelling of the head, neck or upper extremity in the future, a flow-limiting procedure should be performed on this low-flow fistula.
Conclusions
AAG provides a new vascular access option for dialysis patients in whom conventional vascular access cannot be established. Based on its characteristics, our team has improved the AAG procedure. The improved technique involves creating a low-flow AVF distal to the AAG. This surgical method was designated as IAAG by our team.
The low-flow AVF does not need to achieve the blood flow rate required for a puncturable dialysis AVF; it is intended solely to increase blood flow velocity within the AAG and improve its long-term patency. Since the blood flow through the AVF is relatively low, it has minimal impact on cardiac function and does not increase the venous drainage burden of the extremity in patients with central venous occlusion. Although the present patient had severe superior vena cava stenosis, no limb swelling occurred after creation of the low-flow AVF. Therefore, the IAAG technique is compatible with the indications for AAG and can be attempted in patients who require AAG for maintenance hemodialysis, with the aim of improving the patency rate of AAG.
We will continue to perform the IAAG procedure in eligible patients, or create a low-flow AVF at the distal end of the AAG in a single stage, to observe the long-term patency rate of IAAG.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.