
Abstract
Aim:
Survival of patients with end-stage renal disease naturally depends on the preservation of functional vascular access. This study aims to compare 1-year patency rates, procedural success, and reintervention requirements of surgical revision with endovascular interventions in the treatment of arteriovenous fistula dysfunction.
Material and methods:
Data of 1008 patients who underwent intervention due to arteriovenous fistula dysfunction between 2015 and 2022 were analyzed retrospectively. Treatment allocation to the surgical group (n = 896) or endovascular group (n = 112) was strictly dictated by objective preoperative Doppler ultrasonography criteria, primarily absolute thrombus load. To accurately reflect the operative strategy and disease severity, the surgical cohort was categorized by primary clinical pathology: thrombosis, low flow (<600 mL/min), infection, cephalic arch stenosis, and aneurysm. Endovascular interventions primarily utilized paclitaxel-coated balloons and bare metal stents. The primary endpoint was the 1-year primary patency rate; the secondary endpoint was the need for reoperation.
Results:
The mean age was 59.2 ± 12.7 years, and males were the majority (61%). The 1-year primary patency rate was significantly higher in the surgical group (78.6%, n = 704) than in the endovascular group (24.0%, p < 0.001). Subgroup analysis of the surgical group revealed a patency rate of 81.0% (n = 552) for thrombectomy and 97.4% (n = 39) for cephalic arch stenosis. Although the low-flow group achieved a patency rate of 79.7%, it exhibited the highest reoperation rate at 21.7%. In the endovascular group, assisted primary patency reached 78.0% with secondary procedures, while the frequency of intervention was statistically significantly higher than in the surgical group.
Conclusion:
Surgical revision provides better patency and less re-intervention compared to endovascular methods for arteriovenous fistula dysfunction, especially in cases of high thrombus burden or cephalic arch stenosis. Single-stage open surgery guarantees long-term durability and immediate cannulation.
Keywords
Introduction
Chronic kidney disease (CKD) is a major public health problem, growing in parallel with the global increase in the prevalence of diabetes and hypertension. 1 Among renal replacement therapies, hemodialysis is the primary life-support treatment for more than 2.5 million patients worldwide.1,2 For these patients, the efficacy and quality of the dialysis process depend directly on the presence of a sustainable and uncomplicated vascular access route.
Autologous arteriovenous fistulas (AVFs), defined by Brescia and Cimino in 1966, are accepted as the “gold standard” vascular access route by KDOQI (Kidney Disease Outcomes Quality Initiative) and ESVS (European Society for Vascular Surgery) guidelines due to their lower infection rates, long-term patency durations, and cost-effectiveness compared to central venous catheters (CVC) and arteriovenous grafts (AVG).3,4
However, although the creation of an AVF is a surgical success, the process of “arterialization” triggered by the exposure of the physiologically low-pressure and low-flow venous system to high arterial flow and increased shear stress requires complex hemodynamic adaptations. 5 The transformation of laminar flow into turbulence and changes in wall tension (shear stress) trigger the neointimal hyperplasia cascade, predisposing to the development of stenosis and subsequent thrombosis. 6 Literature data indicate that 20%–50% of created fistulas become unusable due to maturation failure or late-term dysfunction. 7
Today, in the management of vascular access complications, the “Fistula First” approach has been replaced by the “ESKD Life-Plan” strategy, which centers on the patient’s life plan. 8 Although endovascular methods such as Percutaneous Transluminal Angioplasty (PTA) have gained popularity in the treatment algorithm due to their minimally invasive nature, the long-term durability of this strategy remains controversial. 9 Surgical revisions retain their “salvage” role, particularly in cephalic arch stenoses with high elastic recoil risk and total occlusions with a high organized thrombus burden. 10 Surgical intervention not only restores the lumen via techniques such as thrombectomy, aneurysmectomy, patchplasty, and bypass but also ensures the anatomical removal of the pathology.
The aim of this study is to compare the 1-year patency rates of surgical and endovascular methods in a large patient series (1008 cases) at our hospital, which serves as a tertiary center in our region. By employing strictly objective clinical criteria for treatment allocation, this study seeks to discuss the efficacy, patency rates, and complication profile of surgical revision in light of the current, high-level literature.
Materials and methods
This study is a single-center, retrospective cohort study conducted at the Cardiovascular Surgery Clinic of a Education and Research Hospital. The study period covers the years 2015–2022. The study protocol was prepared in accordance with the principles of the Declaration of Helsinki and was approved by the University Faculty of Medicine Ethics Committee (Date: January 14, 2026; Issue: 01–40). Patient confidentiality and data security were strictly maintained throughout the study.
In our region, which has a population of approximately 2 million, an average of 10,000 hemodialysis sessions are performed monthly in public and private institutions, supporting a permanent hemodialysis patient pool of 1000–1200 people. As the main reference center for vascular access, our clinic evaluated 4526 patients for the need for permanent vascular access between 2015 and 2022. Among them, 1305 patients diagnosed with arteriovenous fistula (AVF) dysfunction were screened.
To ensure a homogeneous study group, the following exclusion criteria were applied: pediatric patients (<18 years, n = 18), complications involving vascular grafts or central venous catheters (n = 45), isolated arterial access stenosis (n = 29), missing 12-month follow-up data (n = 89), and mortality during the follow-up period (n = 116). After these exclusions, 1008 patients were included in the final analysis. Patients were divided into two main groups: the Surgical Group (n = 896) and the Endovascular Group (n = 112).
Treatment allocation was strictly determined based on objective morphological criteria established by mandatory preoperative arterial and venous Doppler ultrasonography, alongside healthcare-economic realities. In cases of acute thrombosis, blood flow was naturally absent at presentation; thus, evaluation was limited to vessel diameters and thrombus characteristics. However, for functional but failing fistulas, Doppler flow volumes were routinely measured to guide proactive therapy. Patients presenting with an absolute high thrombus load were universally referred for open surgical revision. Given the lack of percutaneous mechanical aspiration systems at our center, surgical extraction was deemed the only definitive method to eliminate the dense clot and permit immediate postoperative hemodialysis, thereby successfully avoiding temporary central venous catheter (CVC) placement. Conversely, in our aging patient cohort with rapid vascular calcification, specific endovascular interventions (primarily utilizing paclitaxel-coated balloons and bare metal stents) were deliberately reserved for a “rescue” role, primarily serving patients with low thrombus burden but dense fibrotic strictures, or acting as bridging therapy.
To accurately mirror our surgical decision-making process and the true pathological burden, we classified our surgical cohort based on “Clinical Pathology and Primary Surgical Indication” rather than purely by precise anatomical location. From an open surgical standpoint, operative strategy is dictated by macroscopic pathology. Particularly in our largest subgroup—Primary Venous Thrombosis—the massive clot burden almost universally extended across multiple anatomical segments, making single-location assignment clinically unfeasible. The surgical group was further divided into five etiological subgroups: Primary Venous Thrombosis (n = 552; Figures 1–3): Mechanical thrombectomy using 3F–4F Fogarty (Figure 4) catheters or rotational devices via venous incision under local infiltration anesthesia for simple focal procedures, or ultrasound-guided axillary nerve block for complex interventions requiring extensive dissection, followed by patch angioplasty or anastomotic renewal.

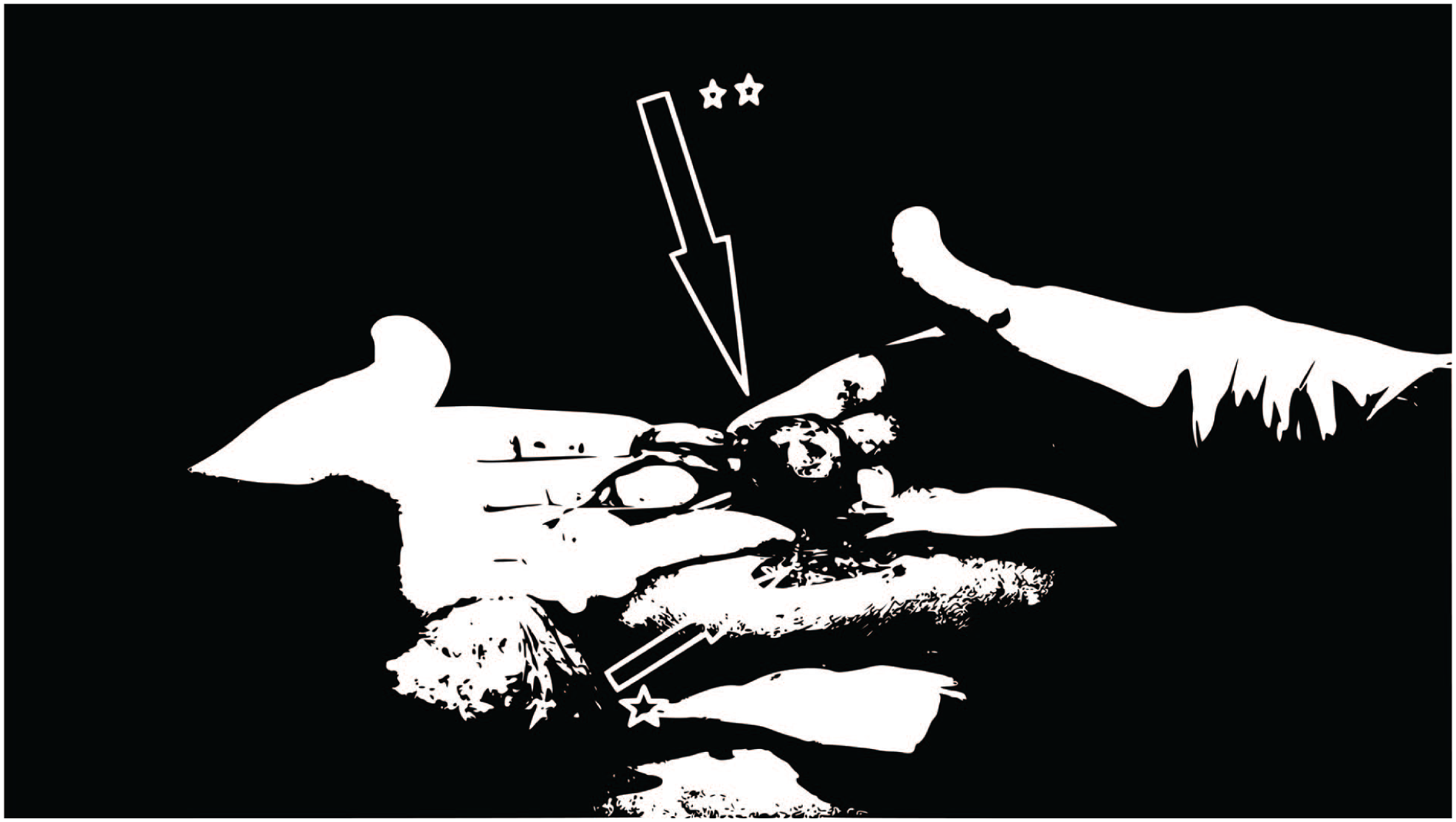
Surgical management of an aneurysmal arteriovenous fistula: (a) surgical dissection of the thrombosed aneurysm (*: exposed thrombosed aneurysm sac**), (b) resection of the aneurysmal segment (**: ligated vessel stump), (c) aneurysmorrhaphy (plication) of the vessel wall (***: plication suture line), and (d) macroscopic appearance of the excised aneurysmal sac (*: excised pathological tissue)**.
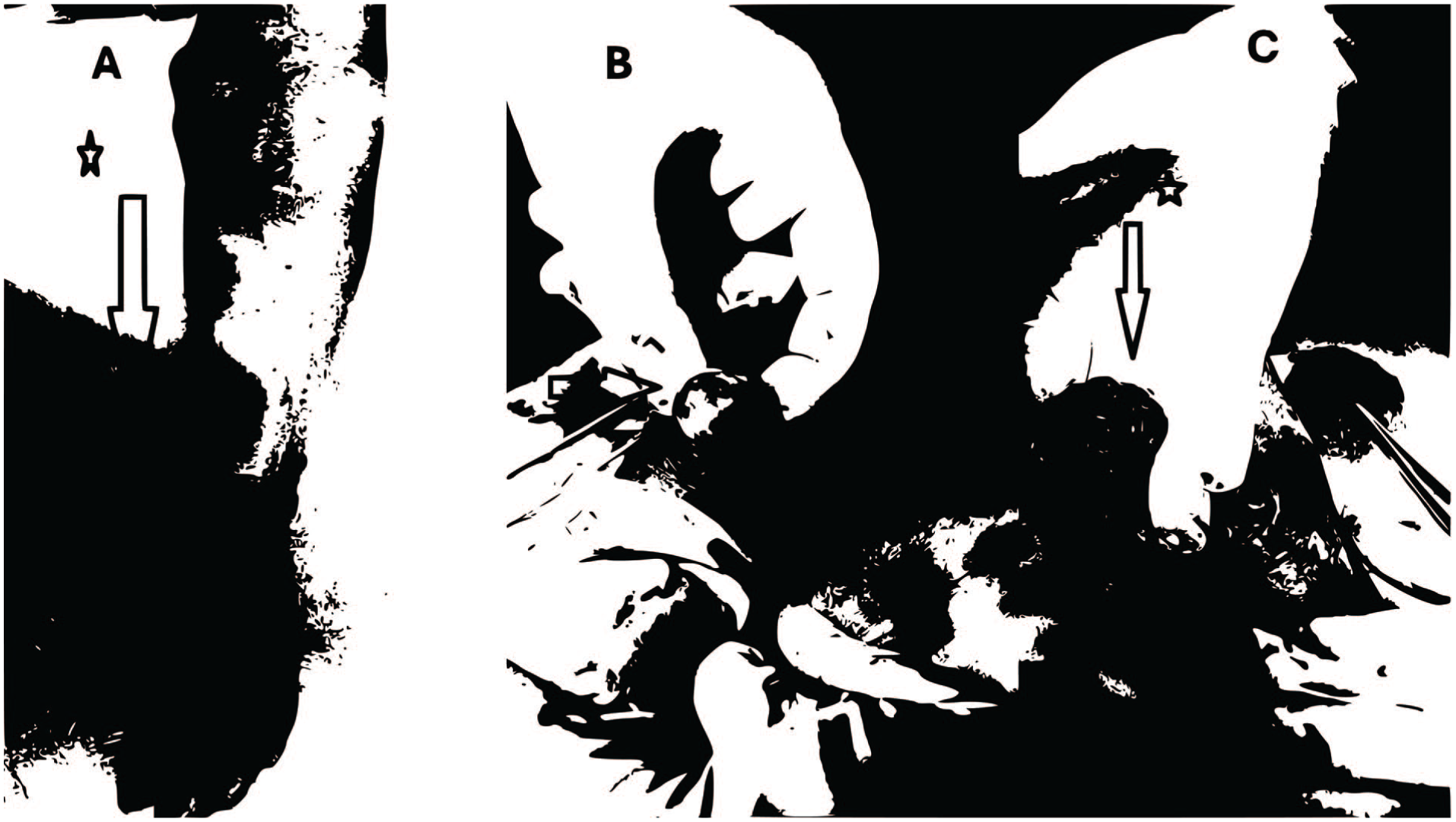
Radial artery aneurysm and intraluminal pathology: (a) preoperative clinical view of a radial artery aneurysm (*: aneurysmal dilatation**), (b) intraoperative dissection of the aneurysmal sac (*: exposed aneurysm), and (c) Organized thrombus removed from the aneurysm (**: massive organized thrombus burden)**.

Surgical exposure of a radial-cephalic arteriovenous aneurysm: (a) preoperative clinical view (*: massive arteriovenous aneurysm**), (b and c) intraoperative dissection and opening of the aneurysmal segment (**: opened aneurysmal sac), and (d) macroscopic view of the extracted pathological material (***: excised thrombus and sac wall)**.
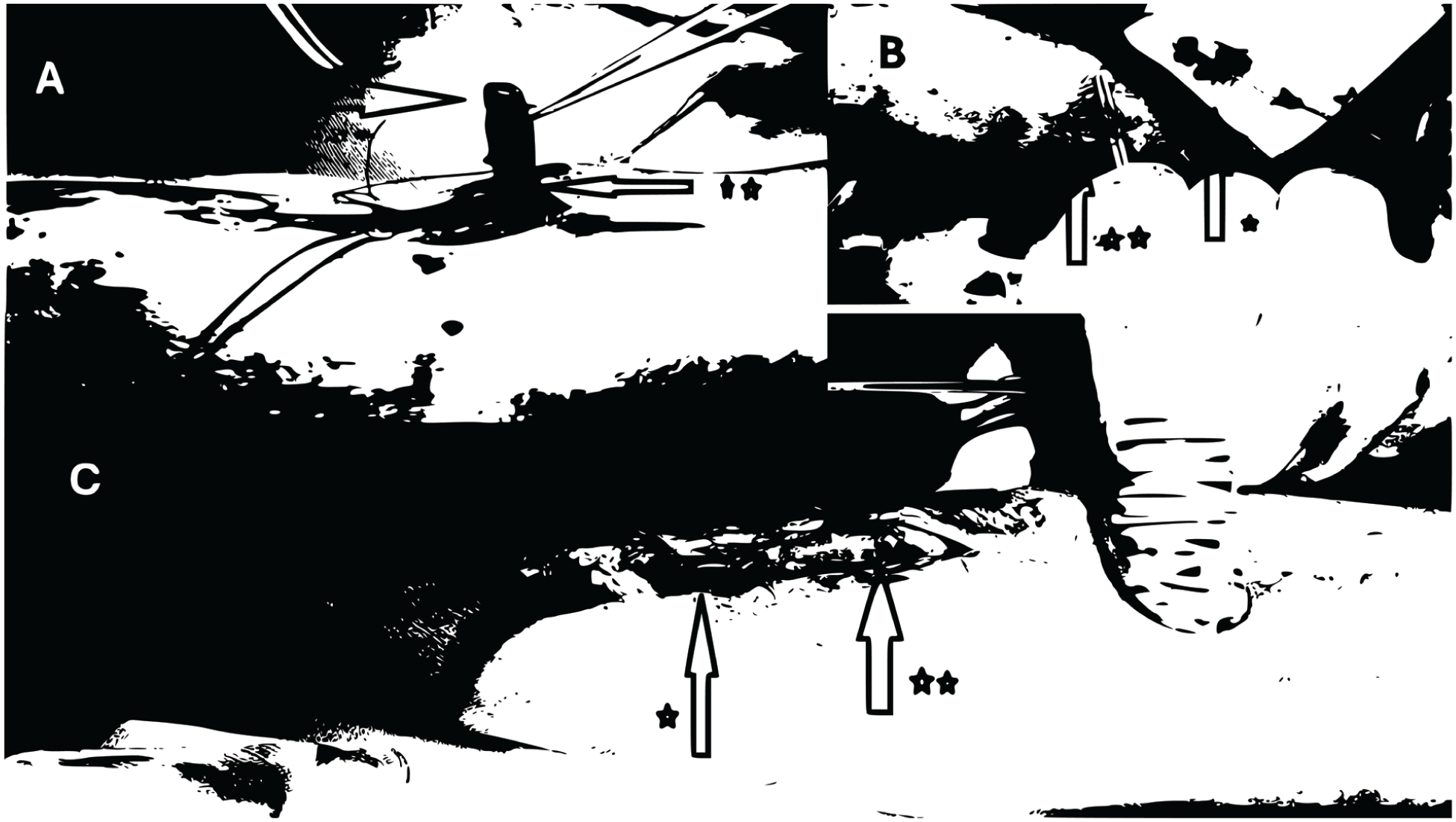
Mechanical and rotational thrombectomy techniques: (a) surgical thrombectomy procedure (*: extracted thrombus plug; **: venotomy site**), (b) application of a thrombectomy catheter (*: extraction device and captured clot; **: vessel access point), and (c) manual compression and clearance of the thrombus burden (*: manually expressed thrombus; **: cleared venous segment)**.
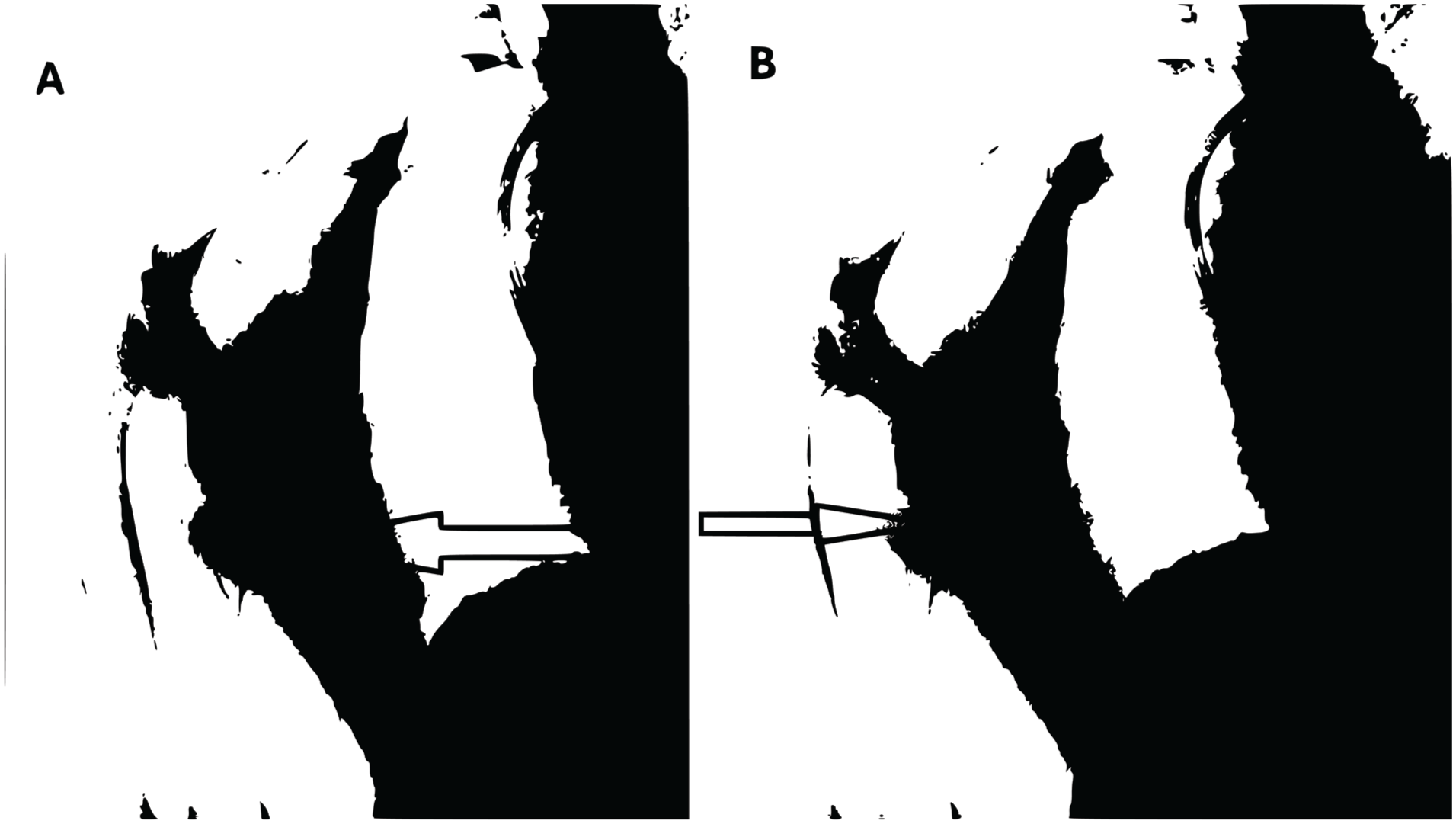
Radiographic diagnosis of cephalic arch obstruction: (a and b) angiographic images demonstrating high-grade stenosis/obstruction at the cephalic arch (*: point of critical stenosis at the cephalic arch**)**.
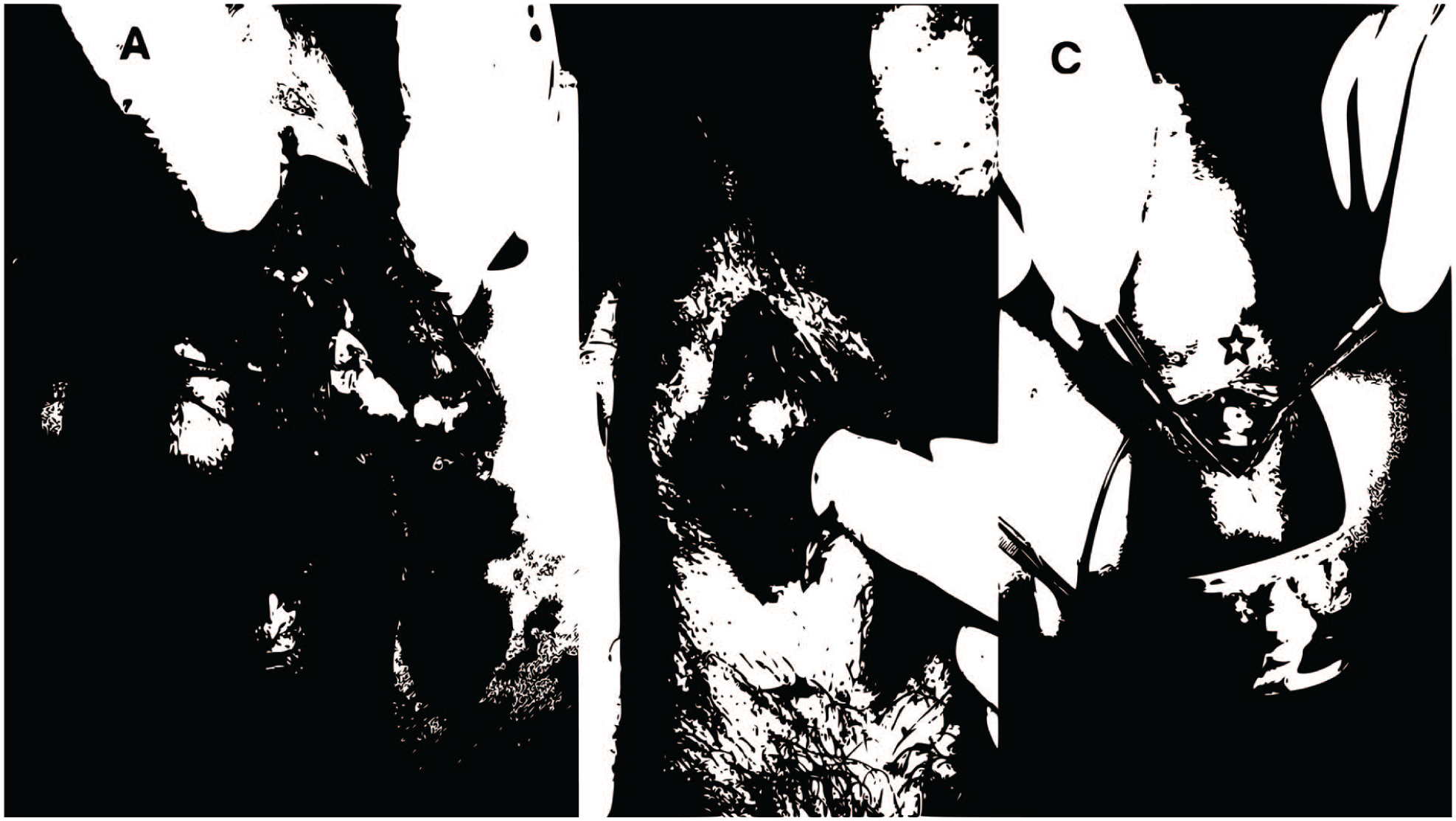
Diverse anatomical presentations of arteriovenous aneurysms: (a) distal radial arteriovenous aneurysm (*: aneurysmal sac; **: adjacent dissected vessel**), (b) classic radial artery aneurysm (*: exposed aneurysm), and (c) aneurysm located at the anatomical snuff-box (*: aneurysm)**.
Surgical salvage of an arteriovenous aneurysm. Macroscopic view of the resected aneurysmal sac and attached vessels after complete surgical excision (*: proximal native vessel/artery; **: completely excised aneurysmal sac**)**.
Statistical Analysis
Data analysis was performed using SPSS v25.0. The primary endpoint was the primary patency rate at 1 year after intervention, and the secondary endpoint was the need for reoperation of the same fistula within 1 year. Patency rates were calculated using Kaplan-Meier survival analysis. Comparisons between groups were made using the Chi-Square test. A p-value of <0.05 was considered statistically significant.
Results
When the demographic data of the study cohort were examined, male gender dominance (61%, n = 547) was observed, and the female patient rate was determined to be 39% (n = 349). The mean age of the patients was 59.2 ± 12.7 years. When etiological factors were examined, diabetes mellitus (42%) was the most frequently observed comorbidity, followed by hypertension (28%; Table 1). Regarding hemodynamic parameters, preoperative Doppler ultrasonography evaluations demonstrated that even among patients with high thrombus burdens who presented prior to complete occlusion, access flow rates consistently remained below 2 L/min, distinguishing them from true high-flow megafistulas.
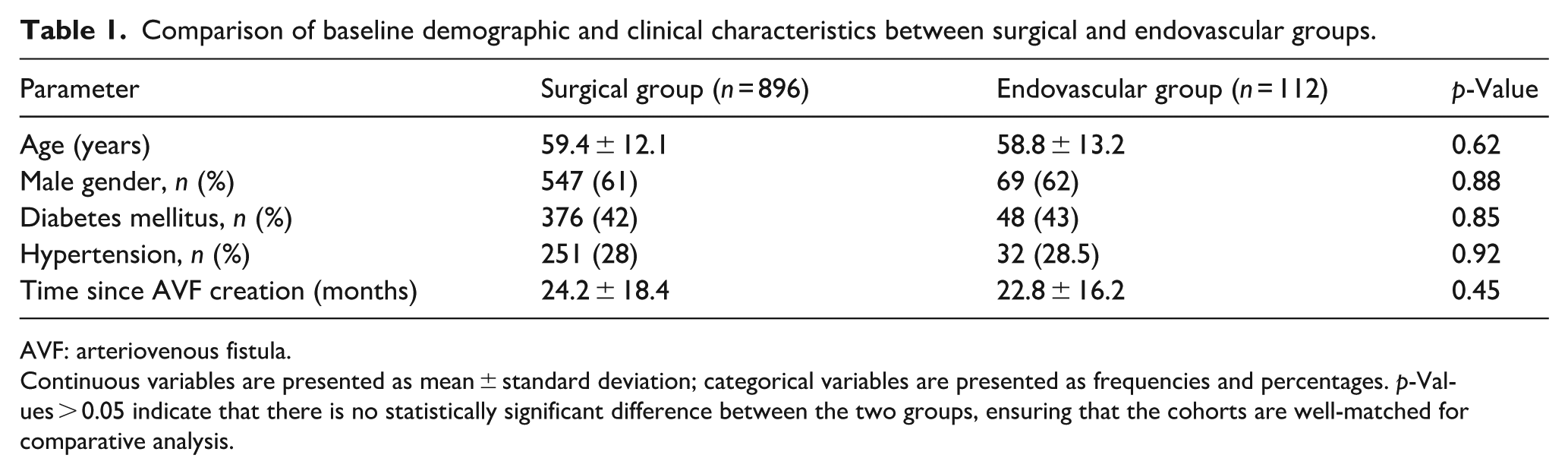
Comparison of baseline demographic and clinical characteristics between surgical and endovascular groups.
AVF: arteriovenous fistula.
Continuous variables are presented as mean ± standard deviation; categorical variables are presented as frequencies and percentages. p-Values > 0.05 indicate that there is no statistically significant difference between the two groups, ensuring that the cohorts are well-matched for comparative analysis.
In the surgical group (n = 896), the 1-year primary patency rate was 78.6% (704/896). The secondary patency rate, calculated including reoperated patients, was 89.8%. The total reoperation rate was determined to be 11.3%. Subgroup analyses according to surgical indications are presented in Table 2.
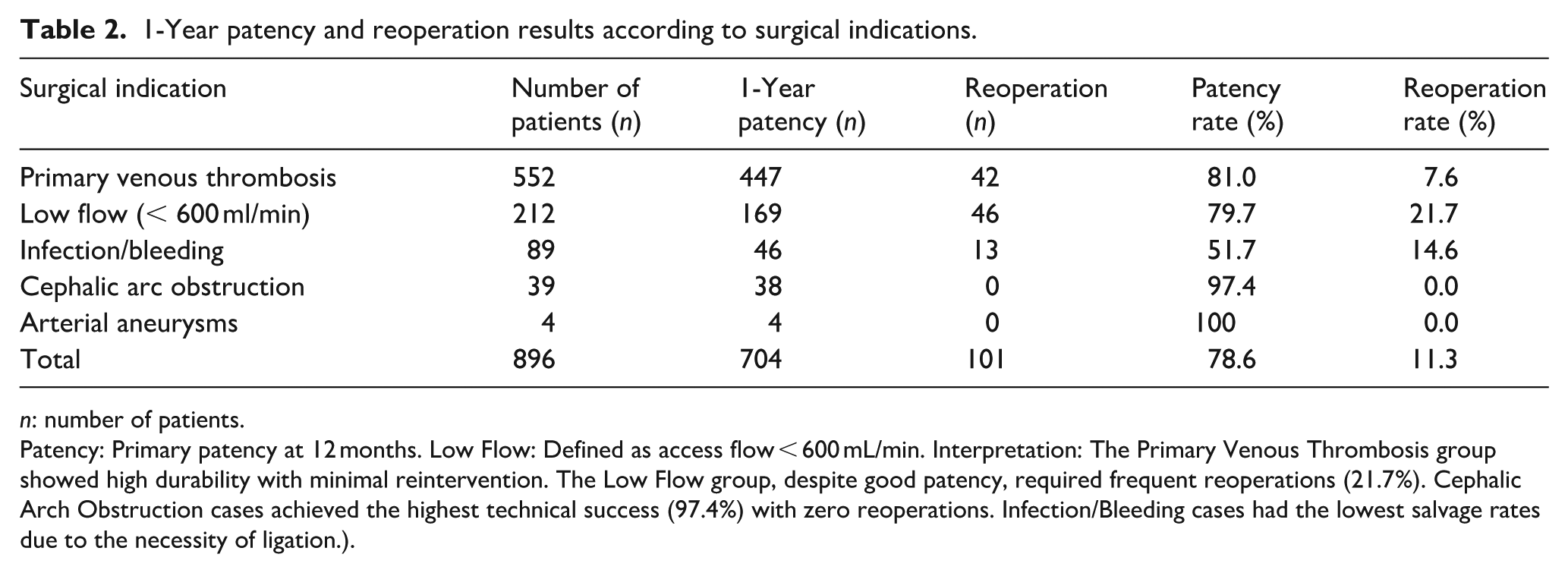
1-Year patency and reoperation results according to surgical indications.
n: number of patients.
Patency: Primary patency at 12 months. Low Flow: Defined as access flow < 600 mL/min. Interpretation: The Primary Venous Thrombosis group showed high durability with minimal reintervention. The Low Flow group, despite good patency, required frequent reoperations (21.7%). Cephalic Arch Obstruction cases achieved the highest technical success (97.4%) with zero reoperations. Infection/Bleeding cases had the lowest salvage rates due to the necessity of ligation.).
When the 1-year results of the surgical and endovascular groups were compared, a significant difference was observed (Table 3). While primary patency was 78.6% in the surgical group, this rate remained at 24.0% in the endovascular group (p < 0.001). Although the secondary patency rate reached 78.0% in the endovascular group, this success was achieved with a high number of repetitive interventions (Figure 8).
Comparative analysis of surgical and endovascular methods.
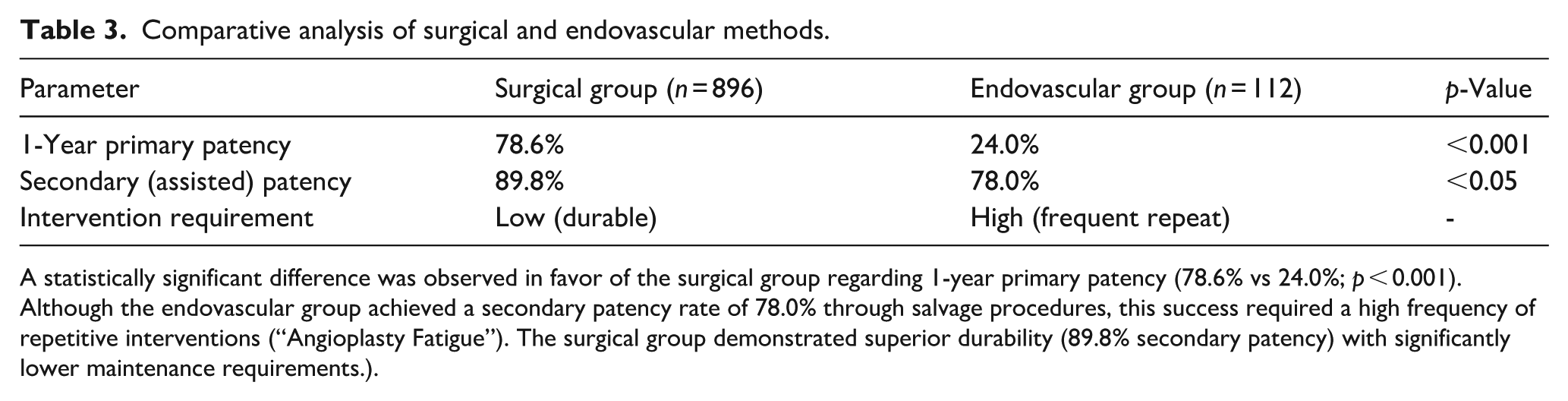
A statistically significant difference was observed in favor of the surgical group regarding 1-year primary patency (78.6% vs 24.0%; p < 0.001). Although the endovascular group achieved a secondary patency rate of 78.0% through salvage procedures, this success required a high frequency of repetitive interventions (“Angioplasty Fatigue”). The surgical group demonstrated superior durability (89.8% secondary patency) with significantly lower maintenance requirements.).
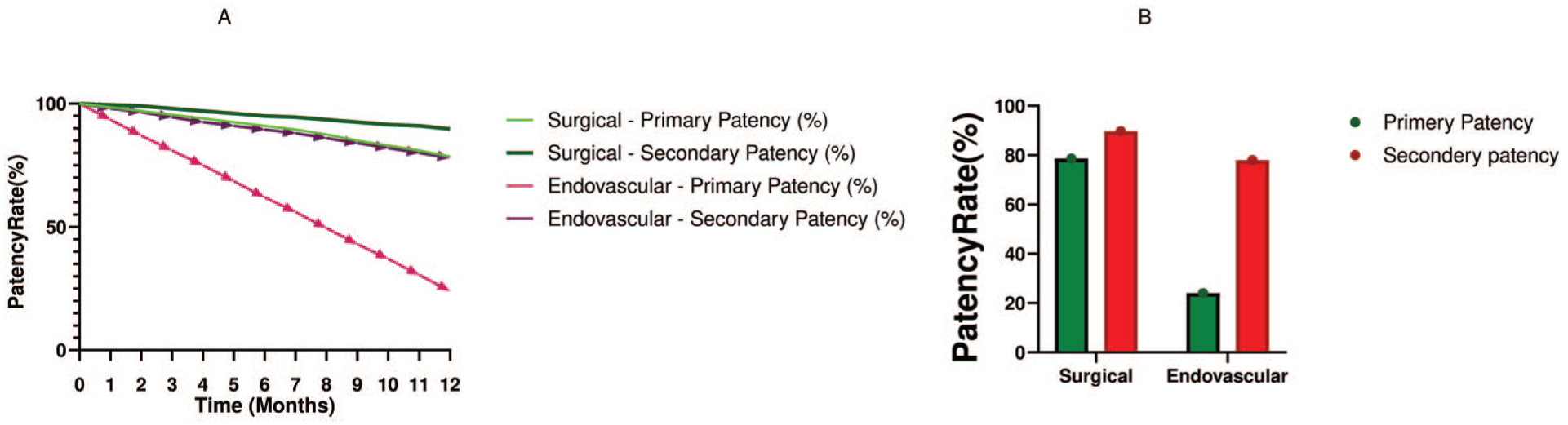
Statistical outcomes of vascular access interventions. Kaplan-Meier estimates of primary and secondary patency rates at 12 months. (a) Surgical Group: Primary patency 78.6% (Solid Green), Secondary patency 89.8% (Dashed Green). (b) Endovascular Group: Primary patency 24.0% (Solid Red), Secondary patency 78.0% (Dashed Red). Note: A statistically significant difference was observed in primary patency rates in favor of the surgical group (Log-rank test, p < 0.001).
The overall complication burden remained low. In the early period (<30 days), incision site hematoma was observed at a rate of 3.2%, minor bleeding at 2.7%, and superficial infection at 1.8%. Procedural safety was confirmed with a perioperative mortality rate of 0.3% (n = 3). No significant difference was detected between the groups in terms of major complications (Figure 9). Patients were closely monitored for arterial “steal” syndrome in the postoperative period. In the surgical group, the rate of major steal syndrome leading to distal extremity ischemia was found to be very low at 1.2% (n = 11); these patients were managed with “remodeling” techniques (Distal Revascularization and Interval Ligation/Proximalization of Arterial Inflow). Procedure-related permanent nerve injury or major limb loss was not observed in either group.

Clinical complications of arteriovenous fistula dysfunction: (a) cephalic arch thrombosis, (b) high-flow AVF associated with significant limb edema, (c) low-flow state in the access arm, and (d) post-procedural or spontaneous hematoma at the AVF site.
Discussion
The most striking finding of this study is the distinct superiority of surgical revision compared to endovascular methods in providing long-term patency and reducing the need for repetitive interventions in the management of complicated arteriovenous fistulas (AVF). Although current guidelines recommend autologous fistulas as the “first choice” due to low complication rates,3,4 meta-analyses indicate that primary patency rates of fistulas are still below desired levels. 7 Data obtained from our large series (n = 1008) reveal that the surgical approach—particularly in cases with high thrombus burden, cephalic arch stenosis, and recurrent lesions—is a more durable “salvage” strategy than minimally invasive methods, contrary to some views in the current literature.
The 81.0% primary patency rate obtained in our surgical thrombectomy group represented a statistically significant improvement compared to the 24.0% rate of the endovascular group. The fundamental reason for this difference is that thrombosis is not a cause, but a consequence of the underlying anatomical stenosis. It is known that the vast majority of fistula failures originate from neointimal hyperplasia-based venous stenoses5,6,11 and that 64% of stenoses in radiocephalic fistulas are located in the first 3 cm juxtaanastomotic segment after the anastomosis. 12 While endovascular methods—such as the paclitaxel-coated balloons and bare metal stents utilized in our cohort—primarily dilate this fibrotic segment, the surgical revision we applied (resection and/or re-anastomosis) physically eliminates the pathology, providing a definitive “debulking” and “volume reduction” effect. While some studies have reported 1-year primary patency rates remaining around 50% following standard endovascular interventions, 13 contrary to our thesis, some publications have reported that primary patency is higher after endovascular interventions compared to surgery. 14 The high success rate in our surgical series highlights the importance of correct surgical technique and proper patient selection based on macroscopic pathology. This aligns with recent literature emphasizing that individualized vascular access planning is crucial for optimizing hemodialysis outcomes, as a uniform approach cannot address the complex heterogeneity of these patients. 15
To accurately contextualize the high absolute number of primary venous thrombosis cases (n = 552) in our cohort, the regional healthcare dynamics must be understood. Our hospital serves as the sole tertiary referral center for a region comprising eight peripheral hemodialysis units. While ideal vascular access surveillance includes routine dynamic flow monitoring, resource constraints in these peripheral centers often preclude such preemptive screening. Consequently, the vast majority of our patients were “late referrals” arriving at our emergency department only after acute thrombosis had already occurred. These events were predominantly triggered by unrecognized progressive stenoses missed during routine peripheral dialysis, compounded by episodes of intradialytic hypotension and severe vascular calcification. Because the massive clot burden in these late referrals almost universally extended across multiple anatomical segments, pinpointing a single culprit stenosis for endovascular treatment was frequently unfeasible, further validating our surgical extraction protocol.
Cephalic arch stenoses are one of the areas where endovascular treatments are most prone to failure. Bennett et al. 16 divided the cephalic arch into four anatomical regions (domains) and determined that stenoses develop most frequently in Domain IV (i.e. the final turn where the cephalic vein drains into the axillary vein). This anatomical localization validates the logic of our surgical approach, as we bypass this high-resistance terminal segment (Domain IV) with the transposition procedure we perform. Whereas endovascular methods struggle to maintain patency at this stressful junction due to high elastic recoil risk, results are frequently characterized in the literature as “disappointing.”17,18 The 97.4% technical success achieved in our cephalic arch group proves that surgery is the most effective method to break the mechanical resistance in this region (Figure 6). This exceptionally high success rate must be viewed through the lens of open surgical transposition and bypass. Instead of attempting to percutaneously dilate a highly resistant, fibrotic, and anatomically constrained venous segment—which is notoriously plagued by elastic recoil—our surgical team completely bypassed or physically eliminated the pathological bottleneck. It has been shown that the surgical approach reduces the endovascular intervention burden from 1.9 to 0.4 per patient per year. 19 Our results confirm that surgery offers the most permanent solution by preventing frequent repetitive balloon sessions.
The most significant disadvantage of endovascular methods is the burden of repetitive interventions required to sustain patency. According to our observations, especially in the presence of high thrombus burden, even if aspiration methods are used, the character of the aspirate (dense fibrin clusters, etc.) significantly reduces the success of the procedure. This clinical observation coincides with literature data. Large-scale prospective studies have reported that even mature fistulas require additional interventions to maintain patency in 47.5% of cases. 20 It has also been emphasized by Tessitore et al. 21 that the surgical approach reduces the need for intense surveillance and “angioplasty fatigue.” Current systematic reviews and meta-analyses also reveal that the primary patency rate of endovascular methods is significantly lower compared to surgery (OR: 0.34) and the number of interventions required to maintain patency is 1.73 times higher than surgery. 22
Our preference for surgery in our low-flow group, despite the high reoperation rate, is for patient survival; since AVF use reduces mortality risk even in diabetic patients. 23 Surgery is also the safest harbor in late-term complications such as aneurysm, venous hypertension, and steal syndrome. Pasklinsky et al. 24 stated that surgical repair (aneurysmorrhaphy/resection) in true aneurysms is the safest way to salvage the fistula (Figure 1). In a large series of 139 complications where other methods failed, it has been shown that surgical “salvage” procedures provide over 80% success and directly improve patients’ quality of life. 25 In case of infection, due to fatal systemic complication risks such as pleuritis,26,27 radical surgical excision of the infected tissue is a strategic decision that saves not only the vessel but also the patient’s life.
Vascular access management is a multidisciplinary team effort consisting of nephrologists, surgeons, and radiologists. 28 Our preference for surgical revision over endovascular intervention in these complex phenotypes does not reflect a lack of endovascular competence. Rather, it demonstrates our dedicated cardiovascular team’s profound understanding of endovascular limitations when facing massive, organized thrombus burdens in a center lacking percutaneous aspiration devices, or when dealing with elderly patients exhibiting rock-hard calcifications. Opting for a definitive, single-stage surgical solution is a conscious, patient-centric strategy designed to ensure immediate postoperative dialysis, thereby protecting the patient from the severe morbidity and infection risks of temporary central venous catheters and the crippling psychological and financial burden of repeated endovascular “boomerang” failures. In light of current guidelines, 8 the results of our study demonstrate that surgical revision in patients with particularly high thrombus burden, cephalic arch problems, or frequently recurring stenoses offers superior patency rates and lower need for re-intervention compared to endovascular methods. The preference for a minimally invasive approach should not cause a compromise in the patient’s long-term vascular health and quality of life.
Conclusion
Our study confirms that surgical revision is significantly superior to endovascular methods, offering superior long-term patency and reduced intervention frequency; thus, it remains the gold standard for complex arteriovenous fistula dysfunctions involving high thrombus burden or cephalic arch stenosis. By providing a definitive, single-stage resolution that permits immediate postoperative cannulation, surgical revision effectively minimizes catheter dependence and relieves the heavy socioeconomic burden associated with repetitive endovascular interventions.
Clinical recommendations
In light of our data, surgical revision should be considered the primary treatment option for total occlusions with a high thrombus burden and cephalic arch stenoses to prevent the loss of time and resources. Endovascular methods should be reserved for patients who are not suitable surgical candidates or those with prohibitive perioperative risks. Consequently, the treatment algorithm should be centered on the principle of “The Most Accurate and Durable Access for the Patient” based on objective morphological data, rather than a default “Endovascular First” approach.
Strengths and limitations
Strengths of the study
The principal strength of this study is the high degree of homogeneity in patient management. The study cohort was derived from a substantial pool of 4500 vascular access procedures performed at a single tertiary center. Crucially, every stage—from the creation of the initial access route to the management of complications and subsequent revisions—was performed by the same surgical team. This continuity of care effectively eliminated inter-operator variability and ensured high technical standardization. Furthermore, the longitudinal management of the entire fistula life cycle by a single team allowed for a comprehensive understanding of each patient’s unique anatomical and hemodynamic challenges, thereby optimizing the decision-making process for salvage procedures.
Limitations
The main limitations of our study are its retrospective design and its reliance on a single-center experience, which may reflect specific institutional protocols in patient selection and treatment. Another significant limitation is the numerical imbalance between the surgical and endovascular groups. As this study is not a randomized controlled trial (RCT) but a retrospective analysis of “real-world evidence,” an inherent selection bias may be present. For instance, endovascular methods might have been preferred for patients with higher surgical risks or more complex lesion morphologies. While we acknowledge these factors, our results provide substantial clinical insights based on a large-scale patient population. Future randomized controlled trials or multi-center analyses utilizing propensity score matching are warranted to provide more definitive evidence in comparing the long-term outcomes of these two modalities.
Footnotes
Acknowledgements
We offer our deepest respect and gratitude to all our healthcare colleagues whom we lost in the Hatay earthquake.
Author’s note
All authors were actively working at Hatay Education and Research Hospital during the study period (2015-2022). Current affiliations reflect their present academic positions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.