
Abstract
Introduction:
Continuous prostacyclin infusion is the standard of care for pulmonary arterial hypertension, requiring central venous access devices where dwell time is critical but associated with complications.
Methods:
Retrospective 10-year case series of 18 adult pulmonary arterial hypertension patients managed through central venous access devices by a specialized multidisciplinary team.
Results:
Sixty-nine catheters were analyzed across 18 patients; median catheter survival estimated by the Kaplan-Meier method was 9.3 months (95% confidence interval (8.1–12)). Occlusion was the most frequent complication (1.20 per 1,000 catheter-days) and the leading removal reason across all device types. Catheter-related bloodstream infections occurred in four instances (0.22 per 1,000 catheter-days), with methicillin-susceptible Staphylococcus aureus as the only isolated pathogen. Catheter-related thrombosis was documented in two cases. Three catheters fractured, one of each device type.
Discussion:
Evidence on central venous access device outcomes in pulmonary arterial hypertension remains scarce in middle-income countries. The median dwell time observed in this series was shorter than that reported in high-income country cohorts, while catheter-related bloodstream infection and thrombosis rates were numerically lower than those documented in comparable series.
Conclusion:
In this descriptive 10-year case series from a middle-income country, long-term central venous access devices for continuous epoprostenol infusion in pulmonary arterial hypertension were associated with a prolonged dwell time and low complication rates under a structured multidisciplinary follow-up model. Larger multicenter studies are needed to confirm generalizability and identify determinants of catheter longevity.
Keywords
Introduction
Pulmonary hypertension (PH) is defined as a mean pulmonary arterial pressure ⩾20 mmHg at rest, confirmed by right heart catheterization. 1 Around 1% of population is affected by PH, with prevalence rising to up to 10% in people older than 65 years. 2 Although most of the current knowledge comes from High- Income Countries (HICs), about 80% of PH patients live in low-income and middle-income countries (LMICs), where evidence is limited. 3 Pulmonary Arterial Hypertension (PAH, Group 1) has a global prevalence of 192,000 cases in 2021. 4 Contrary to other groups of PH in which the underlying disease is the target of treatment, the cause of PAH is often unknown, leading to a high mortality rate (1.51 per 100,000 people in 2021). 5 Thus, efforts have focused on developing PAH specific drugs that extend transplant-free survival and reduce its high mortality.6,7 These therapies include prostacyclin analogs such as epoprostenol, which induce vasodilation, reduce inflammation, inhibit platelet aggregation, and reverse vascular remodeling. 8 These agents have been widely used since the late 1970s and have proven effective in reducing mortality in randomized clinical trials.9,10
Currently, parenteral delivery of epoprostenol (continuous intravenous infusion) through a Central Venous Access Device (CVAD) is the best strategy for pulmonary pressure reduction. 11 CVADs can be CICCs (centrally inserted central catheters), PICCs (peripherally inserted central catheter), or FICCs (Femorally inserted central catheter). 12 Device selection is complex, requiring clinicians to weigh patient-specific factors, expected therapy duration, and device availability. 13 In general, tunneled cuffed CICCs are preferred for long-term therapies, however, in patients with difficult access or coagulopathy PICCs are preferred as they are easier to place and monitor. 14
CVADs insertion is related to mechanical dysfunction and local infection; additionally, their dwell time is often associated with events such as bacteremia, thrombosis or catheter occlusion, with a reported overall rate of complications of 30%. 15 Several strategies have been developed to mitigate these risks: anticoagulation bridging protocols address periprocedural bleeding, 16 tunneling to separate the exit site from the puncture site reduces infection risk 17 and standardized tip location verification, primarily using intracavitary electrocardiography or echocardiography, to ensure optimal positioning. 18
In this context, complications related to CVADs play an essential role in therapeutic continuity. 19 This article presents a 10-year case series of 18 adult patients with PAH requiring CVADs for continuous prostacyclin infusion, managed by a structured multidisciplinary team. It has been reported in line with the PROCESS guidelines, checklist is provided in the Supplemental File 1. 20
Methods
This is a retrospective, observational case series conducted between 2016 and 2025. All adult patients with PAH who required CVADs for continuous prostacyclin infusion were selected through a consecutive sampling. They had their clinical follow-up and catheter management performed by a multidisciplinary team from two specialized centers in Bogotá, Colombia, comprising interventional radiologists, general surgeons, and specialized nursing staff trained in PAH-specific vascular access. The clinical protocol focused on weekly outpatient or inpatient monitoring, patient education, and standardized feedback loops to ensure catheter patency and early detection of complications.
Inclusion criteria and exclusion criteria
All adult patients (⩾18 years) with PAH receiving long-term epoprostenol infusion via CVADs at a specialized institution were included. No patients were excluded; missing data were reported as such. Eligibility criteria are displayed in the algorithm in (Supplemental Figure 1).
Pre-intervention patient optimization
Patients received close follow-up and symptomatic care until functional class was highly compromised, when they were evaluated and temporarily compensated by pulmonology, while waiting for the initiation of epoprostenol therapy.
Periprocedural antithrombotic management
Given that all patients were receiving long-term anticoagulation, a standardized periprocedural bridging protocol was applied. Warfarin was stopped when the team decided to insert the new catheter, and replaced with low-molecular-weight heparin until the INR reached a safe threshold for the planned procedure according to guidelines depending on the invasiveness of the procedure (the type of catheter that was going to be inserted). 16 Anticoagulation was withheld 24 h prior to the procedure and resumed 6 h after successful catheter placement.
Interventions
Device selection followed institutional criteria based on clinical and logistical factors. CICCs (Powerline and Broviac) were preferred for long-term epoprostenol infusion, given their tunneled configuration and Dacron cuff, which provides mechanical anchoring and reduces the risk of bacterial migration along the catheter tract. Powerline became the only CICC accessible as Broviac became unavailable. PICCs (PowerPICC) were selected when CICCs were unavailable or when anatomical constraints precluded safe CICC placement.
Both CICCs and PICCs were placed under sterile conditions. Ultrasound guidance was used in approximately 50% of CICC procedures; the remaining insertions were performed using anatomical landmark technique when ultrasound was unavailable. Puncture and exit sites are reported following the proposed definitions. 17
Tip location method differed by device type due to technological availability: PICCs were equipped with an integrated intracavitary electrocardiographic navigation system, the first-line method according to guidelines, which allowed real-time tip positioning guidance during insertion. 18 CICCs did not include this system; therefore, correct tip position at the cavoatrial junction was confirmed by post-procedural chest radiography with fluoroscopy.
CICCs
All CICCs were tunneled, with the retaining Dacron cuff positioned 3–5 cm from the skin exit site. Tunnel length, measured from the puncture site to the exit site, ranged from 5 to 10 cm. The preferred puncture site was the right subclavian vein through a long axis, in plane approach, and exit site was located on the infraclavicular chest wall. This configuration was intended to allow fibrous tissue growth around the cuff, reducing the risk of bacterial migration and displacement. However, when the catheter that was being replaced was placed in the subclavian vein, it was retired and the new CICC was inserted in the right axillary or internal jugular veins. Approaches and punctured vessels were defined according to Annetta et al. 21
Seldinger technique was employed: a metallic guidewire was advanced into the vessel and a dilator with a peel-away sheath was introduced. Once the required length from the exit site to the atriocaval junction was measured, a 4–5 Fr catheter was advanced using a tunneler. Adequate venous return was verified, and the catheter was secured with suture less stabilization devices.
PICCs
Vascular access was obtained under ultrasound guidance and upon successful cannulation a metallic guidewire was advanced, followed by the introduction of the dilator and the peel-away sheath. The catheter length was measured and adjusted according to the required distance to the cavoatrial junction.
Intracavitary electrocardiographic guidance was connected, and the patient was positioned to facilitate correct catheter advancement. The catheter was introduced and its trajectory was monitored addressing potential anatomical limitations, such as obstruction by previously implanted devices. The device was secured with suture less fixation devices.
Operator details
CICCs were placed by general surgeons with previous acquired learning curve and PICCs were placed by nurses trained to specifically position this type of device. The technique did not vary depending on the operator.
Quality control
Surgical technique was standardized for all CVADs and personnel through previous education and learning curve. Procedures were performed by trained healthcare professionals who belonged to the vascular access multidisciplinary team.
Infusion preparation
Epoprostenol was prepared by the specialized nursing team and dispensed to patients for continuous home administration via a portable elastomeric pump. Each drug reservoir was replaced by the patient every 48–72 h, yielding 2–3 self-managed changes per week. Patients were trained by the nursing team in aseptic reservoir replacement technique.
Post-operative care and follow-up
After the insertion, patients visited the institution each week to have their insertion site supervised in terms of local signs of infection or any other complications, and to receive education and feedback about CVADs care.
Complications definition
Accidental removal, displacement, Catheter-related bloodstream infection (CRBSI) and Catheter-related thrombosis (CRT) were defined according to international and institutional criteria in Supplemental File 3.
Complication management
Catheter occlusion was managed according to its severity. Flow was verified, and if a partial occlusion was identified, the operator flushed the catheter to restore it; in most cases, this management was successful. However, complete occlusions that did not respond to flushing were managed with catheter replacement, no thrombolytic lock therapy was administered. This is a potential limitation, as pharmacological restoration of patency was not attempted prior to device removal.
Data collection
Clinical data were retrospectively collected via institutional REDCap, a platform that allows creation of highly standardized, controlled data collection forms with adequate privacy.
Analysis
Analyzes were performed using R software. Continuous variables were reported as medians with interquartile ranges (IQR) due to non-normal distributions, and categorical variables as frequencies/percentages. Catheter dwell times were analyzed descriptively, with subgroups assessed by median duration.
Catheters were censored at the date of accidental removal, loss of follow-up, patient death, or administrative end of follow-up (December 12th, 2025). Given the descriptive nature of this study, no formal competing risks analysis was performed; censoring at death and accidental removal is acknowledged as a potential limitation.
Ethics
This study was approved by the institutional Ethics Committee in act No. 47 on December 10th, 2025 (Approval Number: IRB00007736). Given the retrospective, non-interventional nature of the study and the use of anonymized data, the Ethics Committee waived the requirement for informed consent.
Results
From January 2016 to July 2025, 18 patients underwent CVADs implantation for PAH management. The median age at first intervention was 31 years, and 61% of patients were female. The most common comorbidity was heart failure (33%). All patients were receiving anticoagulation therapy, the majority with warfarin. All patients had some degree of functional disability, with the majority (67%) presenting severe dyspnea according to Modified Medical Research Council Dyspnea Scale (mMRC). Immediate complications occurred in 17% of cases. Mortality during the follow-up period was 44% (n = 8). Clinical characteristics of all described patients are summarized in (Table 1).
Clinical characteristics of the 18 described patients.
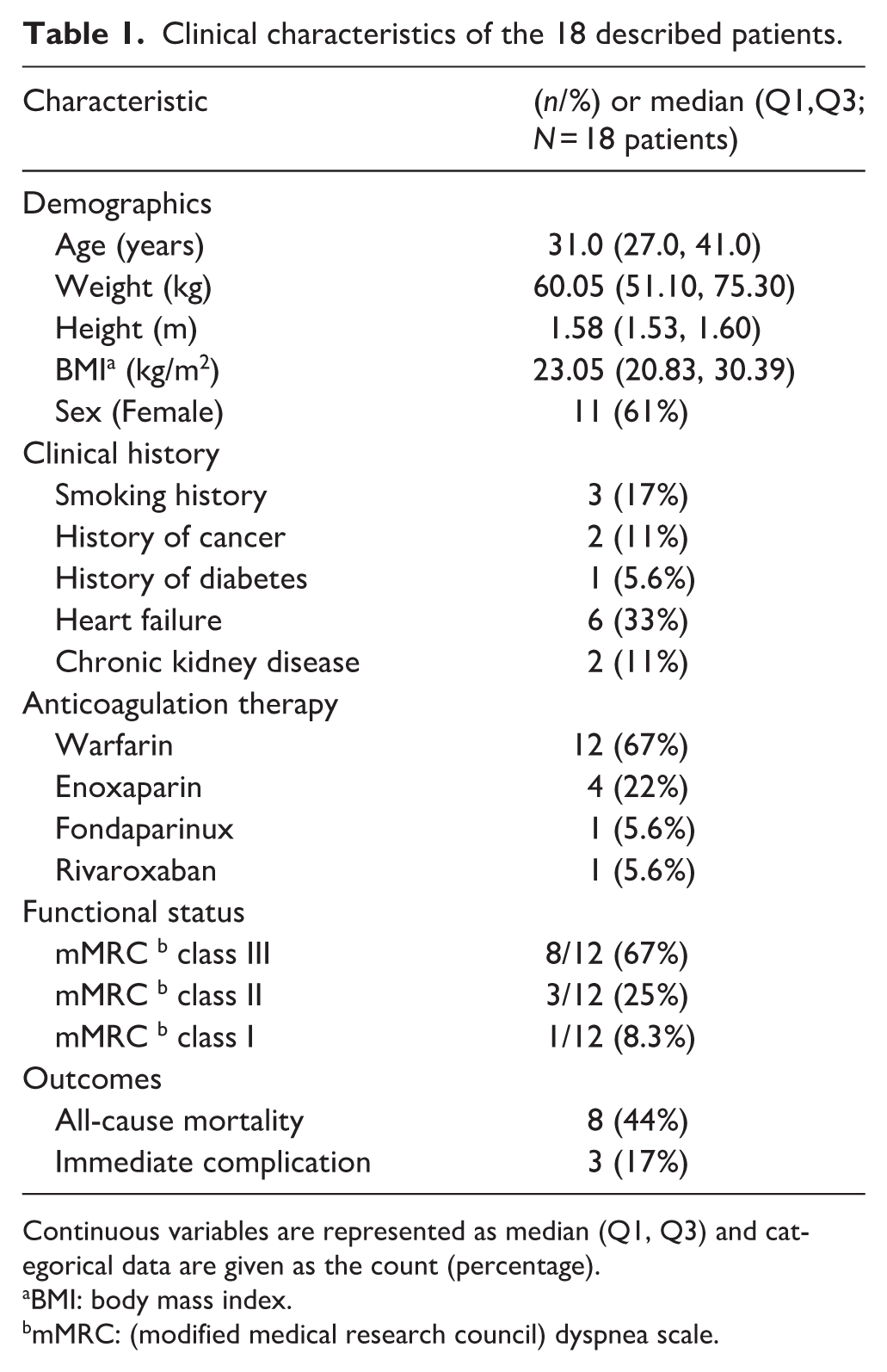
Continuous variables are represented as median (Q1, Q3) and categorical data are given as the count (percentage).
BMI: body mass index.
mMRC: (modified medical research council) dyspnea scale.
Sixty-nine catheters were analyzed during the observation time. Powerline and PowerPICC catheters were selected in similar proportions (43% and 39%, respectively), whereas Broviac catheters were used less frequently (17%). More than half of the catheters were placed in the subclavian vein, and nearly two-thirds were implanted by general surgeons. Catheter characteristics and removal reasons as counts are listed in (Table 2). To account for differences across device types, complication rates were expressed per 1,000 catheter-days and stratified by catheter type (Table 3).
Catheters characteristics including insertion details and immediate complications.
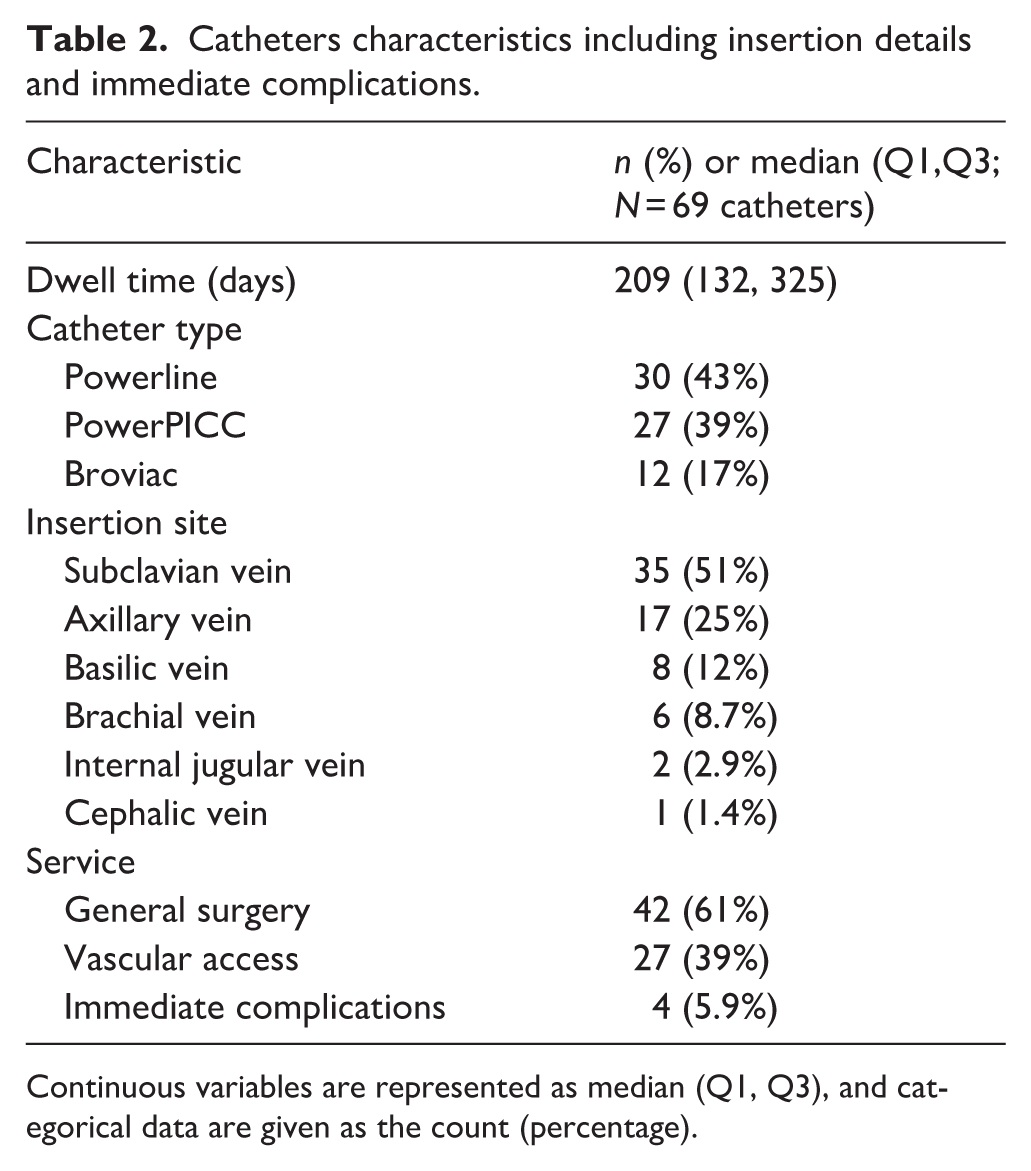
Continuous variables are represented as median (Q1, Q3), and categorical data are given as the count (percentage).
Complication rates per 1,000 catheter-days by catheter type.
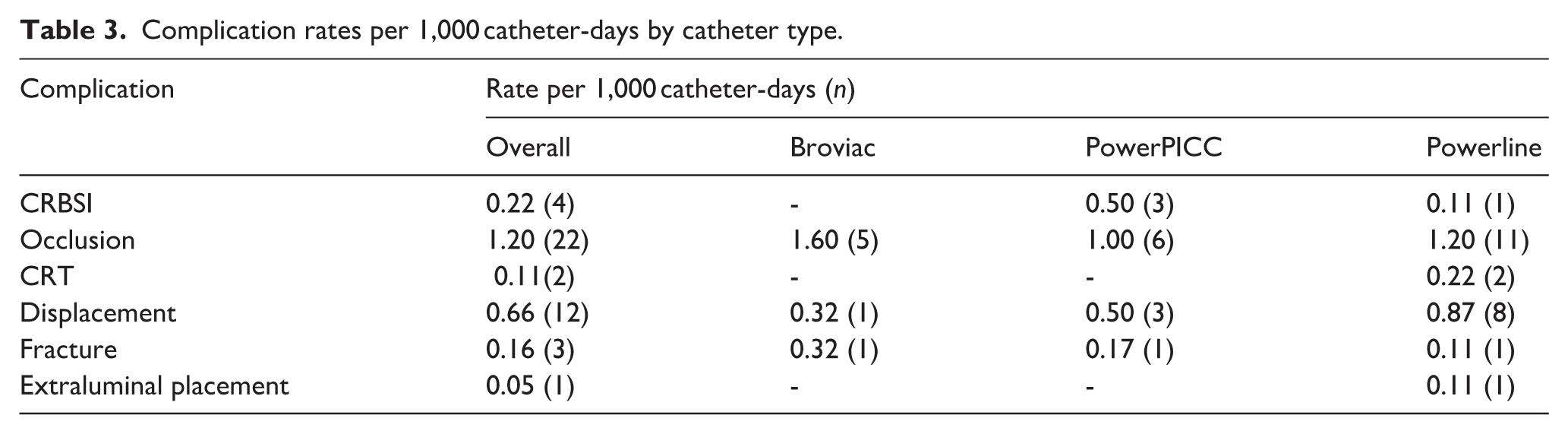
Occlusion was the most frequent complication overall (1.20 per 1,000 catheter-days, n = 22) and was documented across all device types; among catheter types, the rate in Broviac catheters was 1.60 per 1,000 catheter-days. Displacement was documented in 12 catheter episodes (0.66 per 1,000 catheter-days); the rate in Powerline catheters was 0.87 per 1,000 catheter-days. CRBSI was recorded in PowerPICC catheters at a rate of 0.50 per 1,000 catheter-days and in Powerline catheters at 0.11 per 1,000 catheter-days; no CRBSI events were recorded for Broviac catheters. Methicillin-susceptible Staphylococcus aureus was the only pathogen isolated. Three catheters were fractured, one of each type. One case of extraluminal placement was recorded (0.05 per 1,000 catheter-days).
Overall catheter survival was estimated using the Kaplan-Meier method (Figure 1). Overall catheter survival estimated by the Kaplan-Meier method was 9.3 months (95% CI 8.1–12). Survival probability declined most steeply during the first 12 months; the curve subsequently stabilized at approximately 20% of catheters remaining at risk between 18 and 24 months. (Figure 2) displays individual catheter trajectories for all 18 patients. Total follow-up duration was markedly heterogeneous across patients. Gray segments indicate periods of therapy interruption during which standard institutional follow-up was not performed. Deaths occurred predominantly among patients with shorter follow-up durations, whereas patients with longer trajectories ended with an active catheter at study closure. PowerPICC catheters had shorter dwell time (median 168 days) compared with Powerline (median 238 days) and Broviac (median 256 days). Although only one catheter was placed in the cephalic vein, it exhibited the longest dwell time (306 days). Catheters inserted in the internal jugular vein had the shortest duration, with a median of 94 days. Stratified analyses of catheter dwell time are presented in (Table 4).
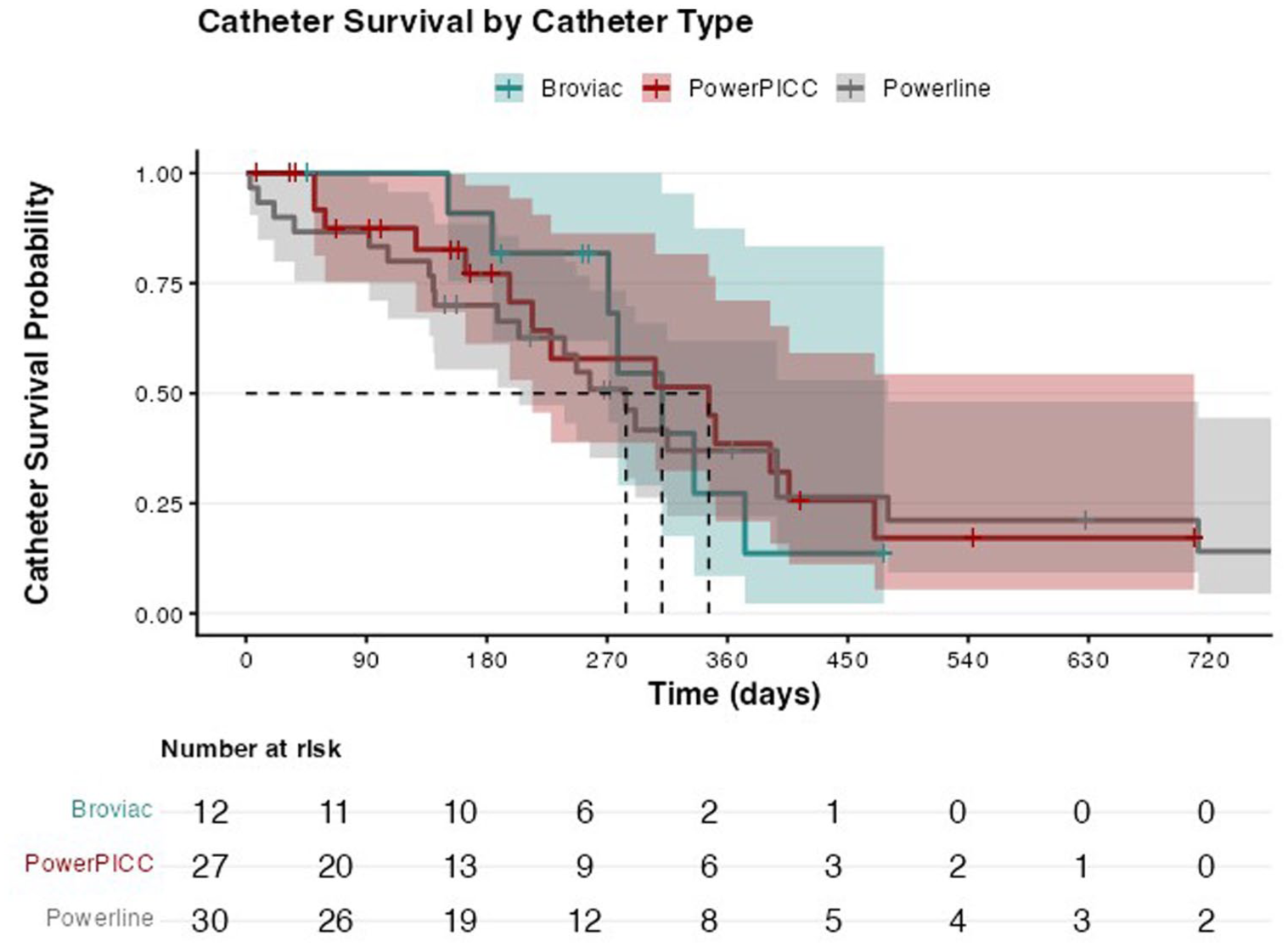
Kaplan Meier curve divided by catheter type.
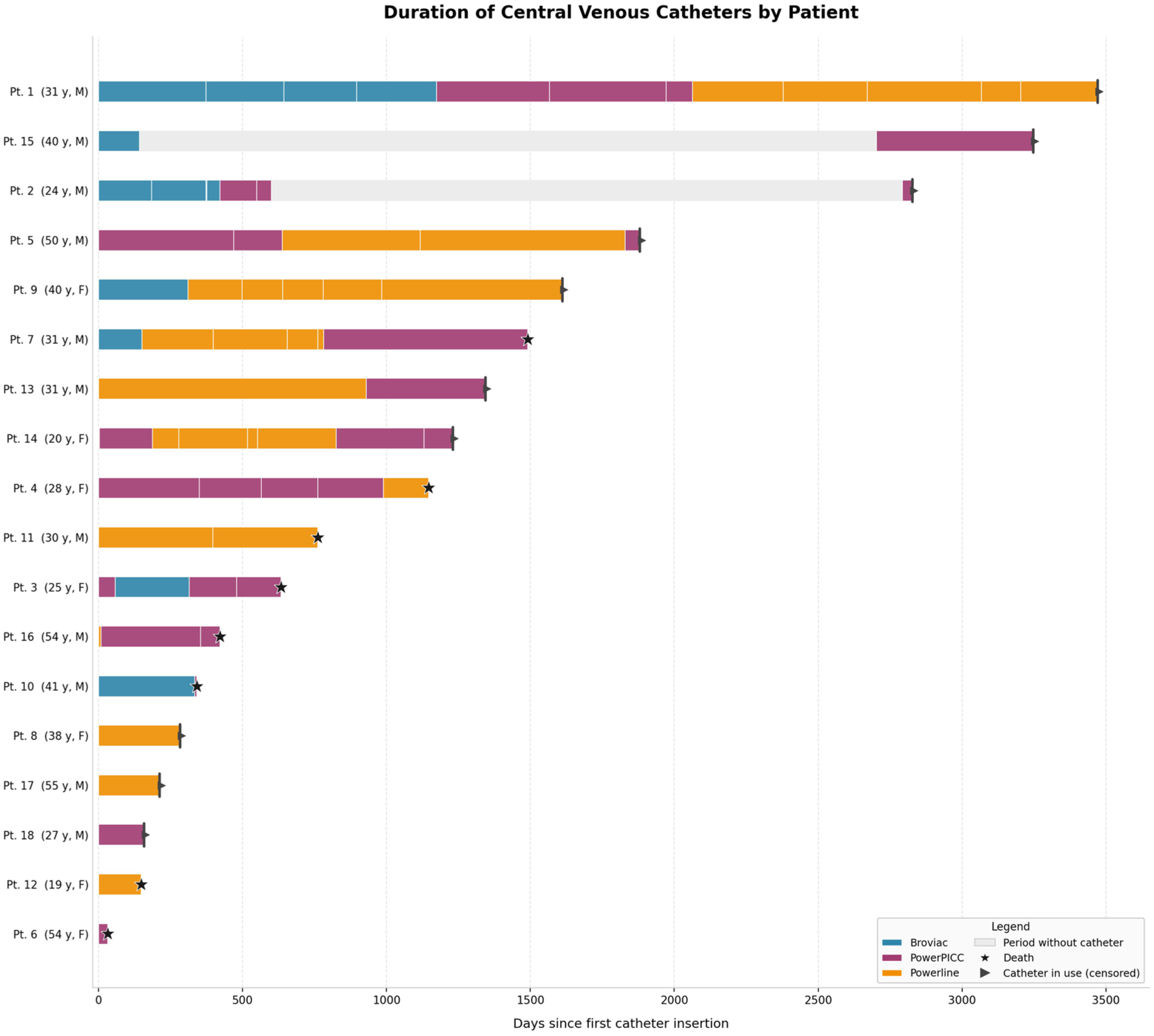
Swimmer plot depicting patients trajectory.
Median dwell time stratified by catheter type, insertion site and the service that did the insertion.
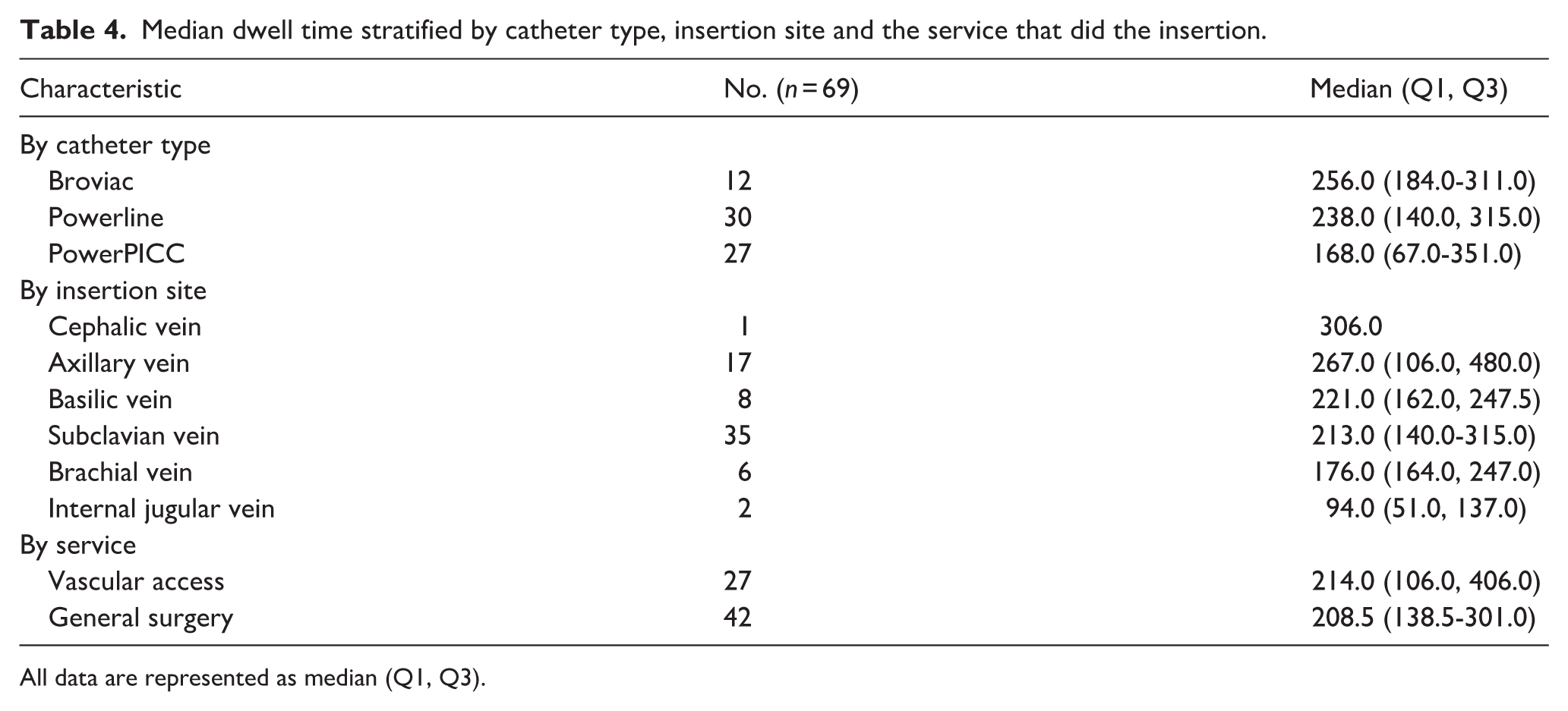
All data are represented as median (Q1, Q3).
Discussion
Treatments requiring long-term CVADs pose substantial clinical challenges, since catheter-related complications depend not only on correct insertion technique but also on patient education, daily care, and structured follow-up. 22 This 10-year case series of adult patients who underwent CVAD insertion for PAH management is set in a middle-income country (MIC), followed by an interdisciplinary team. Compared with prior case series, whose patients tend to be older (mean ages 46.8–56 years) and consistently predominantly female,19,23 this cohort was younger (median age 31 years) with 61% female patients. Regarding catheter longevity, the median dwell time in this study (209 days) was shorter than that reported in recent series from HICs. For instance, Hinojosa et al. 19 documented an overall median catheter duration of 329 days, noting that CICCs remained in situ significantly longer (median 484 days) than PICCs (194 days); yet it exceeded the mean durations of 43.8–58 days reported in prospective studies for other CVADs. 24
The overall CRBSI rate of 0.22 per 1,000 catheter-days observed in this series was lower than the rates reported in HICs, including 3.8 per 1000 catheter-days in the Corley et al. Australian cohort.25,26 The PowerPICC rate (0.5 per 1,000 catheter-days) was the highest among catheter types in this series, falling between the 3.4 per 1,000 catheter-days reported in the Australian cohort and the 0.11 per 1,000 catheter-days documented in the McManus et al. multicenter cohort; the Zheng et al. meta-analysis, which pooled data from 10 studies in HICs, reported a PICC-specific CRBSI rate of 0.77 per 1,000 catheter-days.24–26 Finally, the Powerline CRBSI rate of 0.11 per 1,000 catheter-days was lower than 5.0 reported for tunneled CICCs by Corley et al., 0.24 in McManus cohort, and 1.01 in Zheng metanalysis.24–26 These observations are descriptive and should be interpreted in the context of differences in study design, patient population, follow-up duration, and infection surveillance methods across series.
Regarding CRT, the overall rate of 0.11 per 1,000 catheter-days and the Powerline-specific rate of 0.22 per 1,000 catheter-days in this study were within the range of 0.017–0.205 per 1,000 catheter-days reported for implanted ports. 27 By contrast, a meta-analysis of adult intensive care settings reported a higher pooled incidence rate for CRT of 8.34 per 1,000 catheter-days, with tunneled CICCs, specifically hemodialysis catheters, reaching 26.6 per 1,000 catheter-days in that context. 28 Even though this study is descriptive, it was observed that the CRT rates are lower than the reported in other case series.
This study has limitations inherent to its retrospective, descriptive design. Thrombotic events could not be subclassified, as clinical records did not systematically capture the imaging or clinical criteria required for this distinction. The sample is small and derives from a single referral center; patients managed here likely represent a more complex population, with greater disease severity and complication burden than those seen in non-specialized settings, which may limit the generalizability of these findings. The absence of a control group precludes comparative inferences. Nevertheless, this study represents a meaningful contribution for LMIC settings, where access to specialized PAH care, continuity of follow-up, and the safe delivery of parenteral prostanoids are often constrained.
Conclusions
In this 10-year single-center case series from a MIC, continuous epoprostenol therapy delivered through long-term CVADs in adults with PAH showed a low rate of complications and a prolonged dwell time under a structured interdisciplinary follow-up model. Despite a shorter median dwell time, infectious complications were within ranges reported in the literature, though formal statistical comparisons were not performed due to the descriptive nature of this study. Additionally, no deaths were attributable to catheter complications. These findings support the implementation of standardized catheter care pathways to deliver complex parenteral prostacyclin therapy in resource-limited settings, although larger multicenter studies are needed to confirm generalizability and identify determinants of catheter longevity.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261457766 – Supplemental material for Outcomes of long-term central venous access devices in pulmonary arterial hypertension: A 10-year case series
Supplemental material, sj-docx-1-jva-10.1177_11297298261457766 for Outcomes of long-term central venous access devices in pulmonary arterial hypertension: A 10-year case series by Juan Gómez-Sandoval, Valeria Correa-Martinez, Javier Amaya-Nieto, Rafael Conde-Camacho and Carlos F. Román-Ortega in The Journal of Vascular Access
Supplemental Material
sj-docx-3-jva-10.1177_11297298261457766 – Supplemental material for Outcomes of long-term central venous access devices in pulmonary arterial hypertension: A 10-year case series
Supplemental material, sj-docx-3-jva-10.1177_11297298261457766 for Outcomes of long-term central venous access devices in pulmonary arterial hypertension: A 10-year case series by Juan Gómez-Sandoval, Valeria Correa-Martinez, Javier Amaya-Nieto, Rafael Conde-Camacho and Carlos F. Román-Ortega in The Journal of Vascular Access
Supplemental Material
sj-png-2-jva-10.1177_11297298261457766 – Supplemental material for Outcomes of long-term central venous access devices in pulmonary arterial hypertension: A 10-year case series
Supplemental material, sj-png-2-jva-10.1177_11297298261457766 for Outcomes of long-term central venous access devices in pulmonary arterial hypertension: A 10-year case series by Juan Gómez-Sandoval, Valeria Correa-Martinez, Javier Amaya-Nieto, Rafael Conde-Camacho and Carlos F. Román-Ortega in The Journal of Vascular Access
Footnotes
Acknowledgements
The authors thank the members of the vascular access team, the Fundación Cardioinfantil-Instituto de Cardiología and the Fundación Neumológica Colombiana.
Author contributions
The following statements are reported following the Contributor Roles Taxonomy (CRediT).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Ethics Committee (Approval No. 47 – December 10, 2025, IRB00007736).
Informed consent
Given the retrospective nature of this study the institutional Ethics commitee waived the requirement for informed consent. Patient confidentiality was maintained throughout the study, and all data were anonymized to protect patient privacy.
Data availability statement
Anonymized data may be made available upon reasonable request to the corresponding author, subject to institutional review and approval*.
Supplemental material
Supplemental material for this article is available online.
Artificial intelligence
During the preparation of this work the authors used Claude sonnet 4.5 to correct writing errors and improve the coherence of previously written ideas. In addition, the same tool was used to generate ![]() , with totally anonymized information as input. After using this tool, authors reviewed and edited the content as needed; all the authors take full responsibility for the content of the published article.
, with totally anonymized information as input. After using this tool, authors reviewed and edited the content as needed; all the authors take full responsibility for the content of the published article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.