
Abstract
Stent placement for venous stenosis is common in patients with arteriovenous fistulas. However, infection of a central venous stent with subsequent brachiocephalic pseudoaneurysm formation presents a complex and high-risk scenario. While infected graft removal is ideal, management is challenging due to difficulties in extracting deep stents, irrigating the infected focus, and handling infected pseudoaneurysms. Documented experience on managing such conditions is lacking. A 64-year-old female maintenance hemodialysis patient with a dialysis vintage of 3.5 years, currently using a right jugular tunneled catheter, had received eight sequential stents from the left innominate to axillary vein for recurrent central venous stenosis. One month before admission, an infection developed in the left axillary region, involving the peri-stent space around the axillary venous stents. Computed tomography (CT) angiography revealed extensive peri-stent purulence eroding into the brachiocephalic artery, forming a pseudoaneurysm. The patient had a left ventricular ejection fraction (LVEF) of 31%. Enterobacter cloacae was cultured. Limited debridement was performed via an axillary approach: loosened stents were removed, deeper stents were left in place, and the pseudoaneurysm was not directly addressed. To minimize systemic spread and heart failure exacerbation, a “manual low-pressure drip-and-gentle aspiration” technique was used for irrigation and drainage with normal saline only, avoiding continuous suction. Postoperatively, septic symptoms resolved, infection parameters improved, and the pseudoaneurysm remained stable. The patient was discharged with a partially retained stent and drainage tube on long-term antibiotics. For patients with central venous stent infection and poor physiological reserve, “palliative debridement with restricted drainage” is a feasible salvage approach. This case highlights the catastrophic potential of infection after long-segment central venous stenting, underscoring the paramount importance of prevention.
Keywords
Introduction
Central venous stenosis is a common complication in hemodialysis patients with arteriovenous fistulas, often requiring endovascular stent placement to maintain vascular access patency. 1 While technically successful in most cases, stent infection remains a rare but devastating complication. Current literature reports an incidence of <1%. 2 In non-coronary bare-metal stent infections, the overall mortality rate is 22.9%, and mortality rises to 14.3% when antibiotic therapy is used alone. 2
Complete endothelialization of a stent typically requires 4–6 weeks. 3 Before that, the exposed metal surface can serve as a nidus for bacterial seeding. Hemodialysis patients face additional risk factors, including repeated needle punctures and compromised immunity, which may increase the likelihood of stent infection. 2
When infection occurs, current guidelines recommend complete surgical removal combined with targeted antibiotic therapy. 4 However, this standard approach is often impractical in patients with severe comorbidities, such as end-stage heart or renal failure, who cannot tolerate major surgical procedures like thoracotomy. Moreover, the complexity escalates dramatically when infection extends beyond the stent lumen to involve adjacent arteries, forming an infected pseudoaneurysm—a condition carrying an immediate risk of fatal hemorrhage.
Here, we report a hemodialysis patient with an infected long-segment central venous stent that eroded into the brachiocephalic artery, creating a pseudoaneurysm, against a background of severe cardiac dysfunction (LVEF 31%). We present a systematic analysis of the key management dilemmas encountered and describe a novel irrigation technique as a potential salvage strategy.
Case report
A 64-year-old female with end-stage renal disease on maintenance hemodialysis presented to our institution. Over the preceding 3.5 years, due to recurrent central venous stenosis following a left upper limb arteriovenous fistula creation, the patient had undergone sequential placement of eight stents along the left axillary to innominate venous pathway. Of these, seven were covered stents and one was a bare-metal stent. Specific brand and size information for the stents placed at the outside hospital could not be retrieved. Her history was notable for the development of low-grade fever 1 week after the initial stent placement. Although she was discharged following antibiotic therapy, she experienced persistent, recurrent low-grade fevers thereafter.
Approximately 1 month prior to admission, she developed left axillary pain and fever during hemodialysis sessions, leading to a diagnosis of stent infection. Management prior to transfer included ligation of the arteriovenous fistula, establishment of a new dialysis access via the right internal jugular vein, treatment with full-dose piperacillin–tazobactam, and incision and drainage of a local abscess in the left axillary region. Despite these interventions, the infection failed to resolve, with persistent wound discharge, prompting her referral to our center. The infection was localized to the deep tissue of the left axillary region, surrounding the previously placed venous stents. On admission, the patient appeared chronically ill and lethargic, with a body temperature fluctuating between 38 °C and 38.8 °C. Transthoracic echocardiography revealed a left ventricular ejection fraction (LVEF) of 31%, accompanied by pulmonary hypertension (systolic pulmonary artery pressure (SPAP): 48 mmHg). Ultrasonography demonstrated multiple abscess formations surrounding the axillary venous stents and significant regional lymphadenopathy (Figure 1). Computed tomography (CT) scans showed dilation of the ascending aorta (maximum diameter: 48 mm) and extensive purulent fluid collection around the left innominate venous stents. Notably, the infection had eroded into the brachiocephalic artery, resulting in an infected pseudoaneurysm measuring ~11 × 6 mm (Figure 2(a) and (b)).
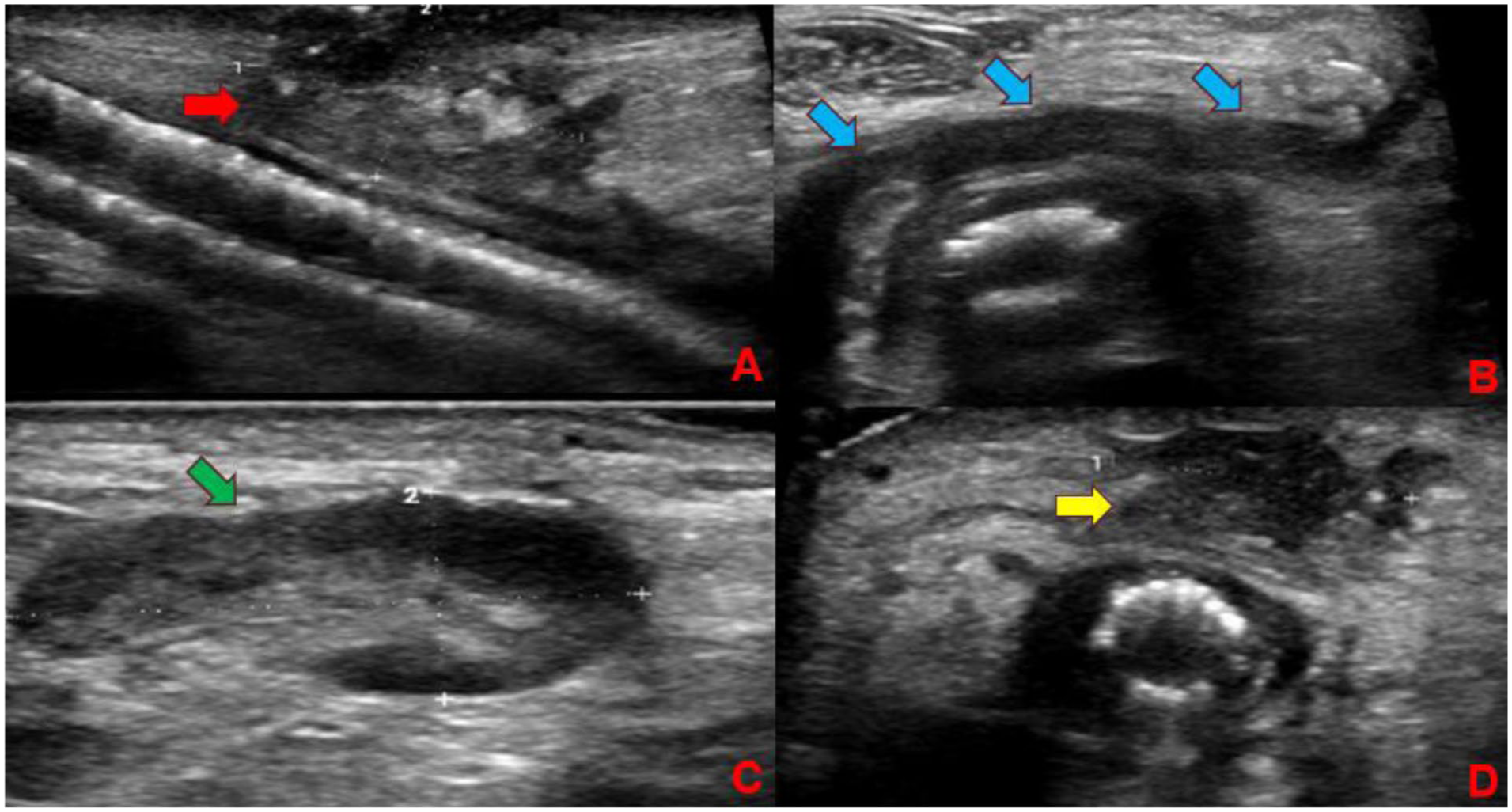
Color Doppler ultrasound findings of the axillary venous region: (a) Extensive purulent fluid collection (red arrow) is observed surrounding the covered stents, (b) a transverse view of the axillary vein reveals a formed peri-stent abscess cavity (blue arrow), (c) enlarged lymph nodes (outlined in green) are noted in the adjacent axillary area, and (d) the largest focus of abscess identified on transverse section examination is indicated.
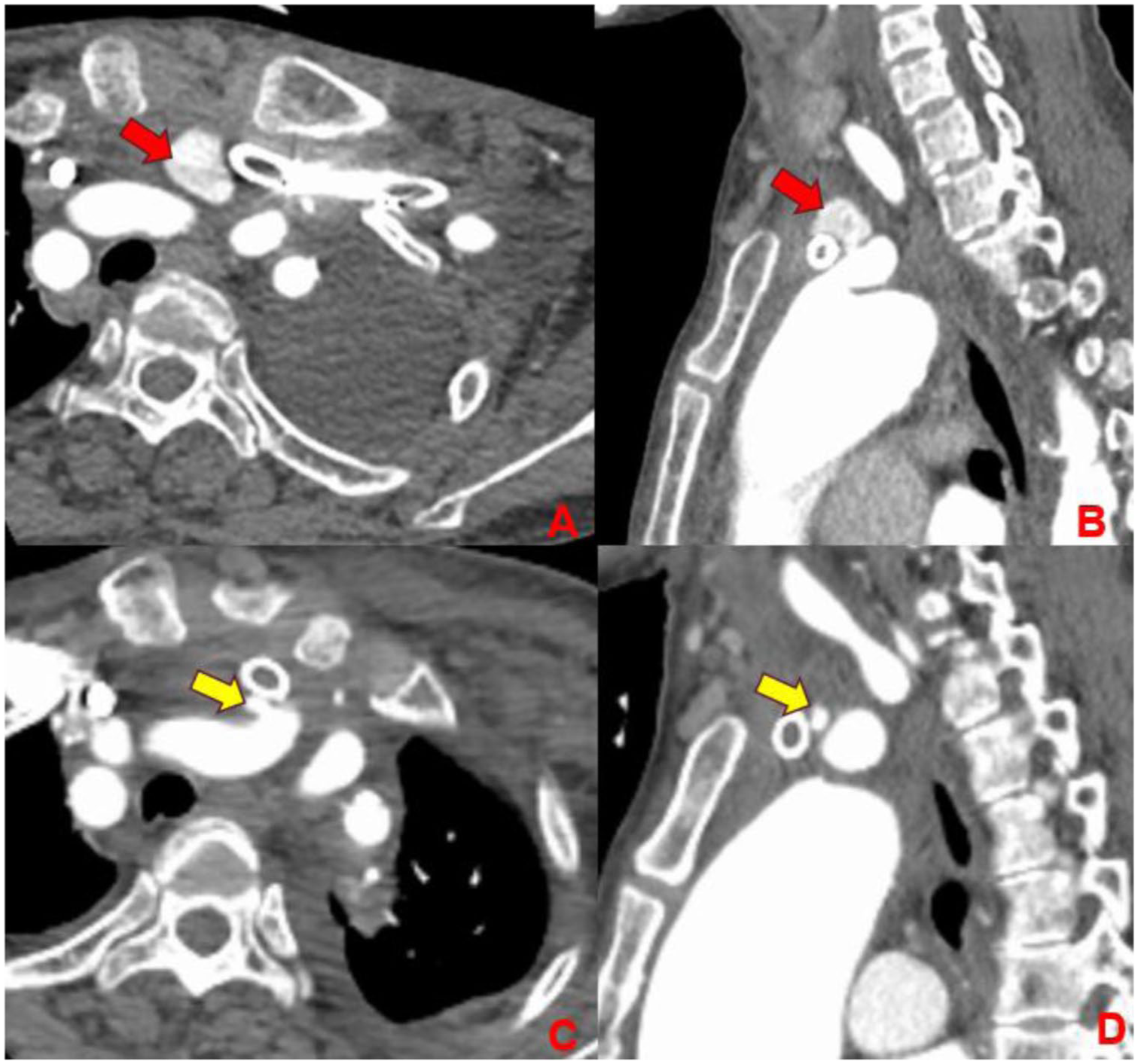
Preoperative and postoperative CT findings: (a) axial CT image shows an infection-induced pseudoaneurysm adjacent to the brachiocephalic artery, (b) sagittal CT image demonstrates the close anatomic relationship between the pseudoaneurysm and the stent within the brachiocephalic vein, (c) follow-up axial CT after stent removal and completion of antibiotic therapy shows reduction in the size of the infected pseudoaneurysm, and (d) on the corresponding postoperative sagittal image, the pseudoaneurysm is notably diminished at its maximum-diameter level. In the images, the red arrow indicates the pseudoaneurysm at initial presentation, and the yellow arrow indicates the pseudoaneurysm on follow-up imaging after treatment, showing reduction in size.
Given the failure of prior anti-infective therapy, the ongoing risk of fatal arterial rupture, and the patient’s severely compromised cardiac function precluding tolerance for thoracotomy, a multidisciplinary team decided to proceed with a minimally invasive, limited debridement via a trans-axillary venous approach under local anesthesia. After layered dissection and exposure of the axillary vein, consistent with preoperative CT findings showing extensive thrombosis from the subclavian to the axillary vein, the axillary vein was found to be chronically occluded upon exposure. The distal end of the axillary vein was identified and occluded with a vascular clip. The vein was then transected transversely. No significant bleeding was encountered, consistent with the chronic thrombotic occlusion. A total of seven stents (six covered and one bare-metal) were successfully removed in continuity, facilitated by the presence of copious pus and minimal adhesion between the stents (Figure 3). The explanted stents were heavily coated with purulent material. Substantial amounts of pus within the axillary region were evacuated using suction. Loose necrotic tissue adherent to the stent surface and abscess cavity was gently debrided using forceps, and additional suspicious necrotic tissue was sharply excised using a scalpel. To achieve local debridement while minimizing the risk of flushing infected debris into the central circulation, the surgeon employed a modified “manual low-pressure drip-and-aspiration” technique (Figure 4). Briefly, based on the length of the removed stents and the apparent distribution of abscesses, a trimmed suction catheter connected to a syringe was carefully advanced ~15 cm into the axillary vein. Controlled irrigation was then performed from the proximal to distal direction using manually instilled low-pressure saline combined with gentle aspiration to avoid systemic dissemination of infected material. The deepest stent (a Viabahn covered stent) was not forcibly removed due to prohibitive anatomical risks. Following irrigation until the effluent ran clear, a drainage tube was placed into the residual abscess cavity (adjacent to the thrombosed vein), and the wound was closed primarily. The patient’s infectious symptoms and laboratory markers improved rapidly postoperatively. Follow-up CT scans obtained at 1 week postoperatively demonstrated significant reduction in the size of the abscess cavity, and shrinkage of the pseudoaneurysm to 7 × 4 mm, and no significant progression of ascending aortic dilation. Intraoperative pus culture confirmed Enterobacter cloacae. The patient received targeted antibiotic therapy, became afebrile within 1 week, and showed marked improvement in her mental status. She was discharged with the drainage tube in place and arrangements made for continued outpatient antibiotic therapy.
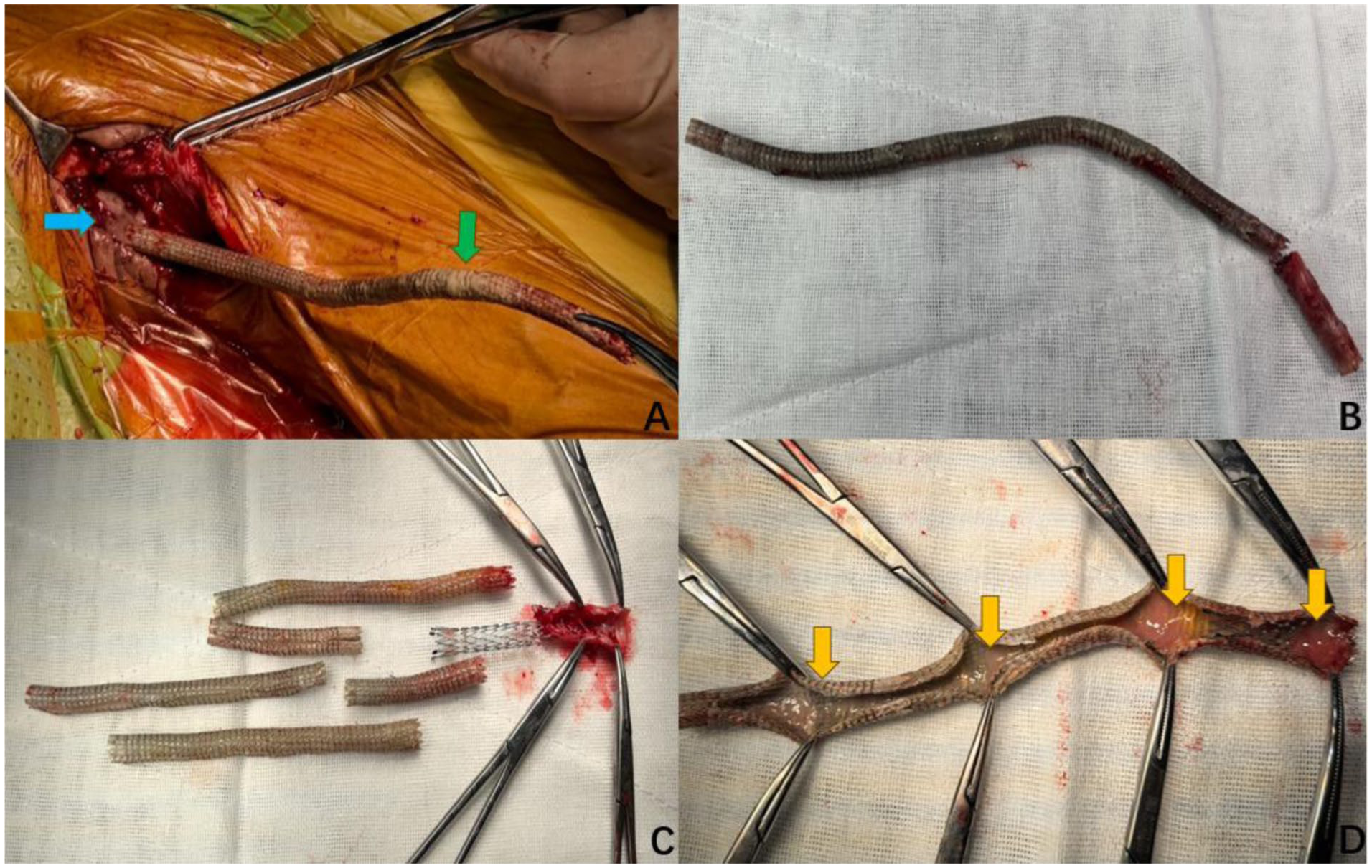
Process and status of stent removal: (a) the axillary vein was exposed through layered dissection, transected transversely, and carefully withdrawn using forceps. Copious pus was observed coating the stent surface (most prominently indicated by the green arrow in (a)). Following extraction of the stent tip, a significant amount of pus exuded from the transected vessel (blue arrow in (a)), (b) the retrieved, intact long-segment stent, (c) upon sequential separation, the individual stents are visible, comprising six covered stents and one bare-metal stent, and (d) a sectioned stent reveals residual purulent material on its luminal surface (yellow arrow).
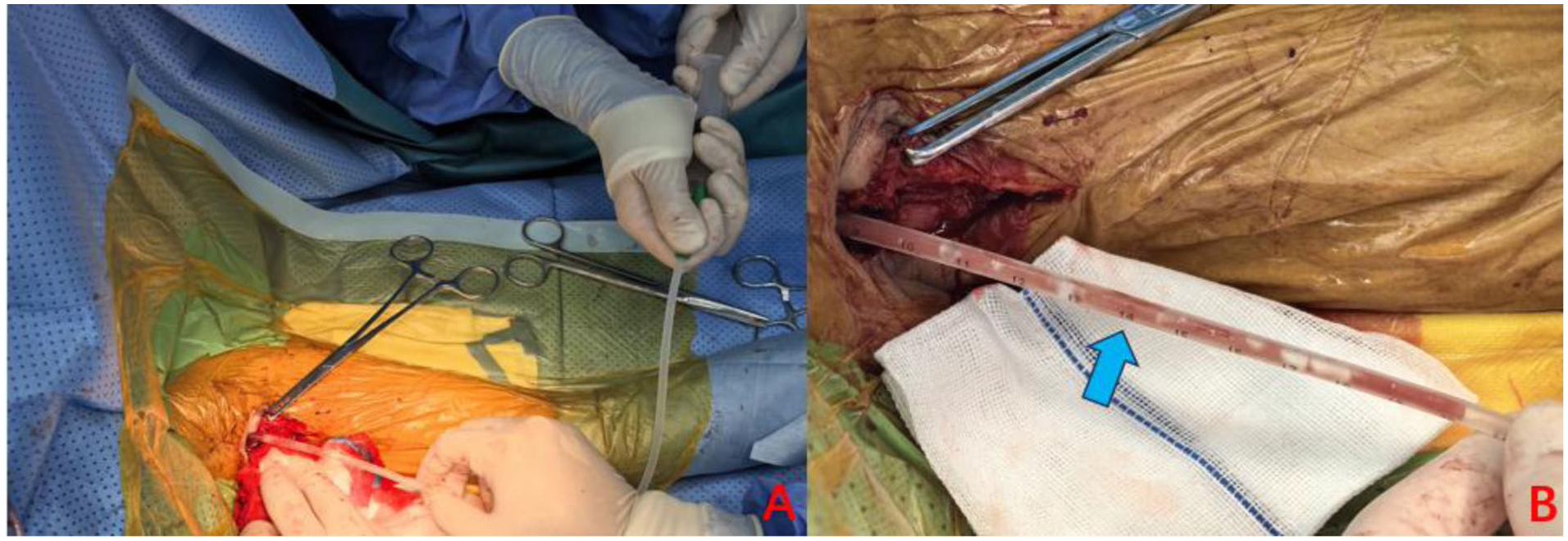
Intraoperative photograph demonstrating the manual low-pressure irrigation technique: (a) a suction catheter connected to a 10-mL syringe was used for the slow instillation of normal saline combined with gentle aspiration, achieving controlled irrigation and drainage and (b) based on preoperative imaging and the length of stents removed intraoperatively, the extent of the abscess cavity was accurately estimated. The insertion depth of the catheter was strictly controlled according to its centimeter markings, ensuring the tip remained within the target cavity and avoiding inadvertent advancement into the central vein. Limited, segmental irrigation was performed based on the distribution of purulent material until the aspirate became clear. In the image, the blue arrow indicates the centimeter markings on the catheter, which served as depth markers to guide insertion.
Discussion
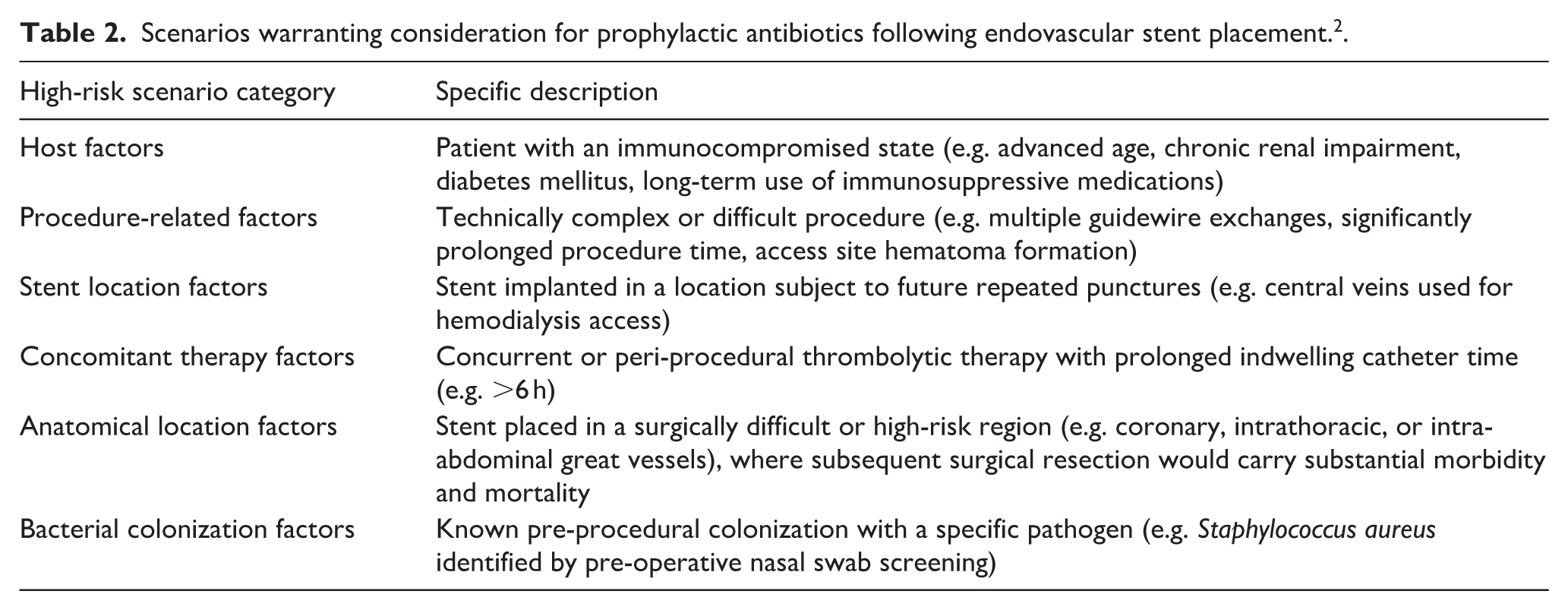
The present case illustrates several challenges that extend beyond the typical presentation of stent infection. Early symptoms of stent infection are often non-specific (e.g. fever, unexplained bacteremia), making timely clinical recognition challenging. Hemodialysis patients have additional risk factors for stent infection (Table 1), including repeated needle punctures and compromised immunity. In our case, the identified pathogen was Enterobacter cloacae. This organism has a propensity to form biofilms on intravascular devices such as catheters and stents, which impedes antibiotic penetration and efficacy. 5 Furthermore, it exhibits intrinsic resistance to several antibiotic classes and can produce extended-spectrum β-lactamases (ESBLs) and even carbapenemases, rendering eradication exceedingly difficult. 6 Given the onset of unexplained low-grade fever ~1 week after the initial stent placement and the nosocomial nature of this pathogen, we speculate that the infection likely originated from intraoperative device contamination or, alternatively, translocation of gut flora secondary to the patient’s immunocompromised state. This highlights the critical need for clinicians to maintain a high index of suspicion and consider stringent protocols for prophylactic antibiotic use in high-risk scenarios (Table 2) to prevent late-onset stent infections.
Risk factors for bare-metal stent infection. 2
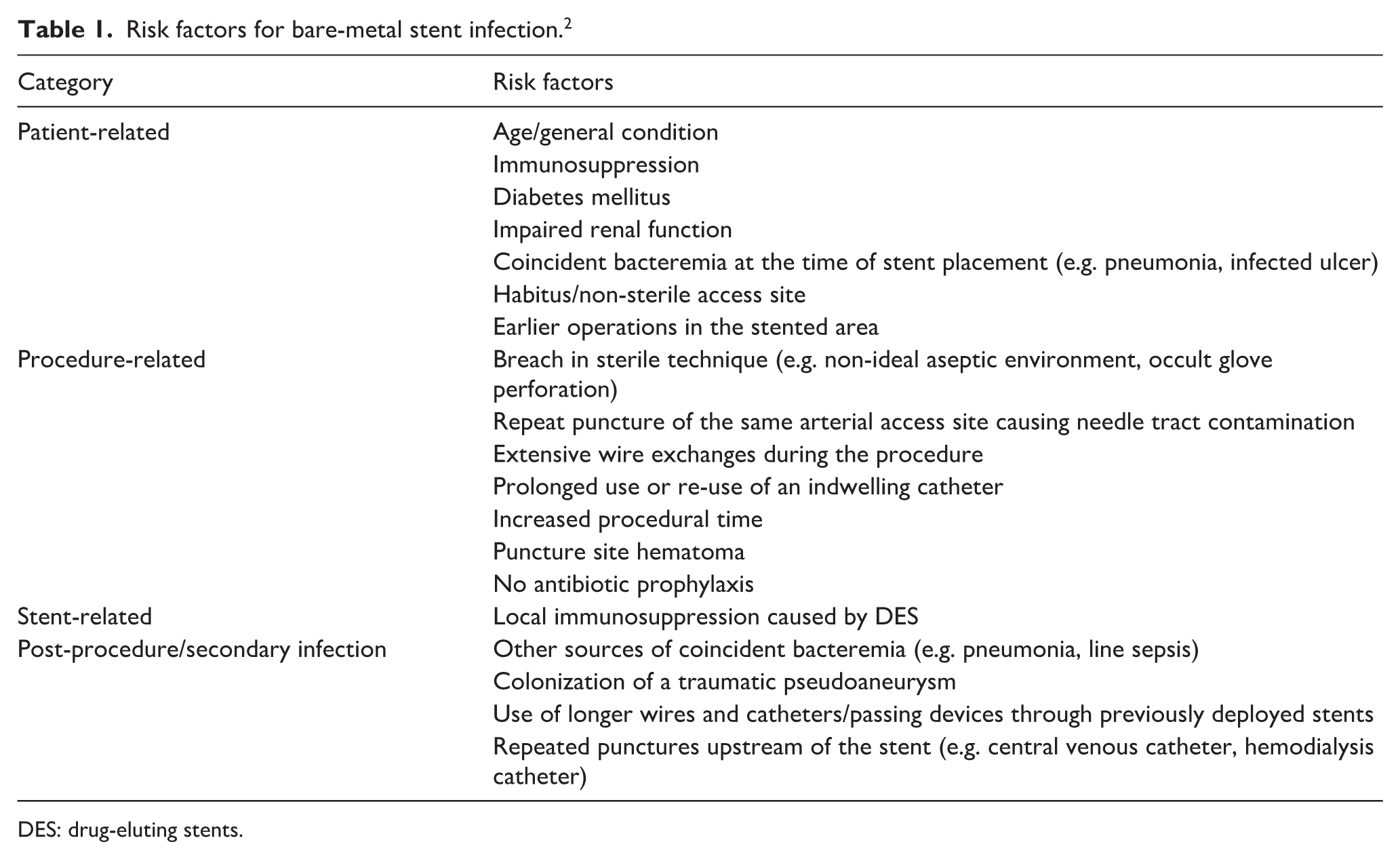
DES: drug-eluting stents.
Scenarios warranting consideration for prophylactic antibiotics following endovascular stent placement. 2 .
Currently, no standardized protocol exists for the management of infected stents. Existing experience suggests that for patients in good general condition, an extended course of antibiotics may be attempted in an effort to salvage the stent. However, once an established infection is present, anti-infective therapy alone is often insufficient, and surgical removal typically becomes the definitive treatment. 4 For severe arterial stent infections, the recommended approach is graft excision combined with in situ vascular reconstruction, utilizing materials such as rifampicin- or silver-coated prosthetic grafts, fresh arterial allografts, or autologous veins. 3 In contrast, the patient in the present case was dialysis-dependent and presented with severely compromised cardiac function, precluding tolerance for thoracotomy under general anesthesia. Thus, only limited debridement and drainage were feasible. Only a few reported cases describe the management of venous stent infections in hemodialysis patients: a 29-year-old patient with a covered stent in the cephalic arch (infected with Pseudomonas aeruginosa) was successfully treated by surgical removal 4 ; a patient with a bare-metal stent in the right subclavian vein (infected with Staphylococcus aureus) was cured after 9 weeks of intravenous antibiotics combined with anticoagulation, followed by the establishment of a new long-term access remote from the infection site 7 ; and another patient with bare-metal stents in the right innominate and subclavian veins (also S. aureus) achieved infection control after 6 weeks of local, high-concentration antibiotic infusion via a catheter placed within the stent lumen, in addition to systemic therapy. 8 These strategies are applicable only when the infection is relatively localized and the patient retains adequate physiological reserve. Our case, however, was considerably more complex and critical. It involved a highly resistant pathogen, infection of multiple consecutive central venous stents, extensive purulent accumulation, and erosion into the brachiocephalic artery with formation of a pseudoaneurysm. This confluence of factors presented a series of formidable clinical dilemmas, as systematically outlined in Figure 5. Ultimately, the strategy of limited debridement and controlled irrigation adopted in this case successfully improved the patient’s outcome.
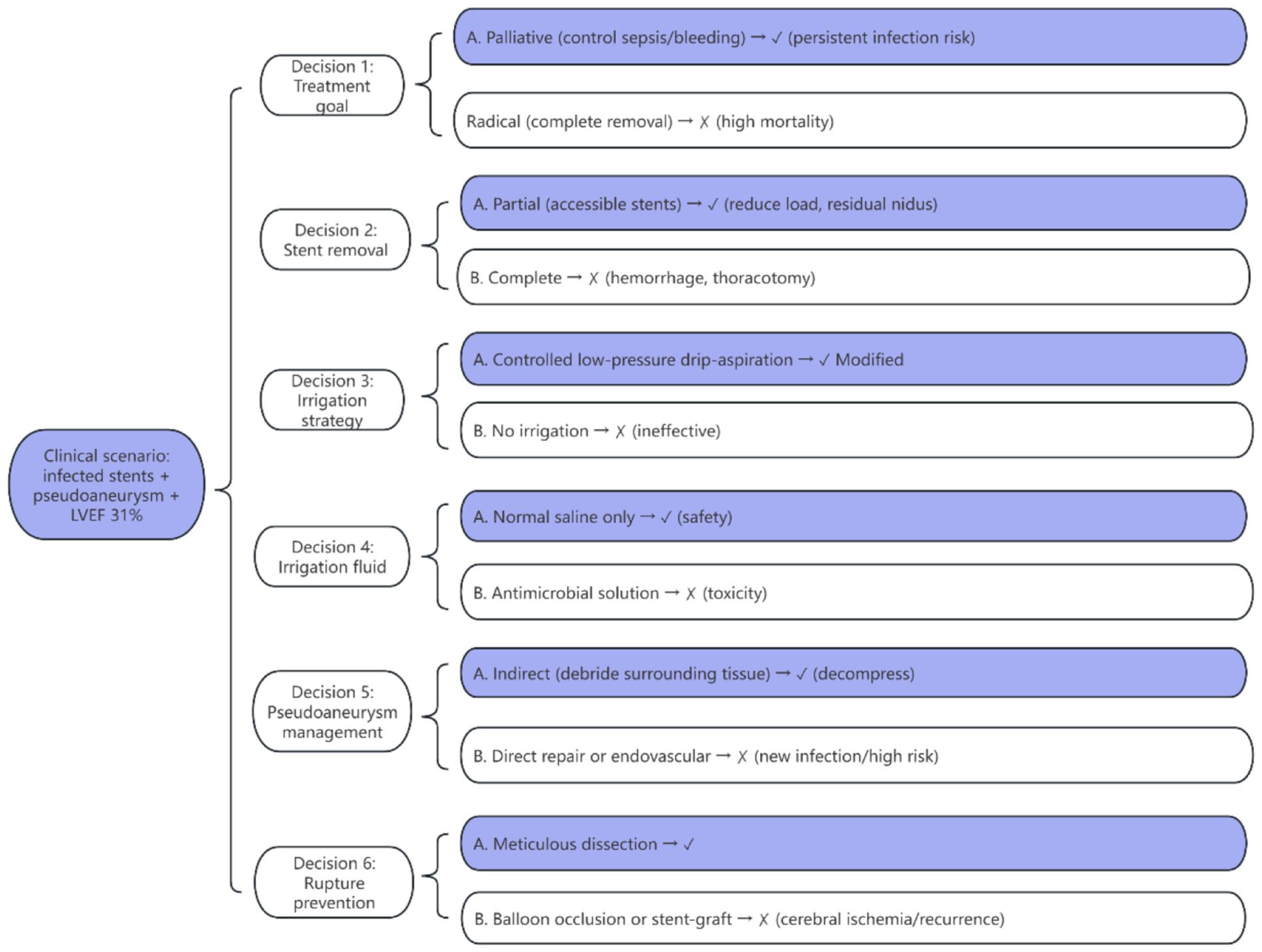
Decision-making algorithm for infected central venous stents with brachiocephalic pseudoaneurysm and severe cardiac dysfunction (LVEF 31%). The algorithm sequentially addresses six clinical dilemmas. For each dilemma, two options (a, b) are presented with their associated risks, followed by the final decision.
Post-discharge follow-up at 45 days revealed clinical improvement: the patient remained afebrile, denied chest pain, procalcitonin decreased from 1.15 to 0.6 ng/mL, and mental status improved. Mild serous discharge from the original sinus tract persisted but was decreasing. Repeat imaging was declined, so long-term pseudoaneurysm stability remains unconfirmed. However, the primary goal was not direct aneurysm repair but reduction of the perivascular infectious burden (decompression). Persistent infection would have accelerated arterial wall destruction and pseudoaneurysm rupture; thus, controlling the infection was the essential first step.
Regarding the concern about retained foreign material and biofilm-forming Enterobacter cloacae: complete sterilization is unlikely. However, surgical debridement and drainage directly reduced the bacterial load and disrupted the biofilm microenvironment by removing the stable matrix that supports biofilm maturation. 9 Residual bacteria, now in a dispersed state, have been shown to exhibit higher susceptibility to antibiotics compared with their biofilm-embedded counterparts. 10 Although local antibiotic concentrations were not measured, the marked clinical response indicates that systemic antibiotics became sufficient after the bioburden was reduced by debridement and drainage. The observed clinical and laboratory improvements provide evidence that the infection was controlled to a low-activity state, even without complete eradication. Long-term suppressive antibiotics and surveillance remain warranted. Without intervention, progression of sepsis and pseudoaneurysm rupture would have been inevitable. Therefore, despite its imperfections, the current outcome represents a survival benefit in an otherwise highly morbid scenario.
This case offers several critical insights for clinical practice: First, the implantation of central venous stents should adhere strictly to established indications and be performed under the highest standards of aseptic technique. Prophylactic antibiotics should be strongly considered for high-risk patients. Once infection occurs, it can precipitate devastating complications such as deep-seated abscesses and erosion into adjacent arteries, making subsequent management exceedingly difficult. Second, a high index of suspicion for stent infection is warranted in any patient presenting with unexplained fever, particularly within the 4- to 6-week post-procedural window for endothelialization. A systematic review of potential intraoperative contamination, prompt blood cultures, early initiation of empirical broad-spectrum antibiotics, and timely imaging (CT or MRI) to assess the peri-stent area are essential to avoid diagnostic delays and the progression to suppurative complications. 11 Finally, when managing a complex central venous stent infection with abscess formation, a meticulous risk-benefit analysis is paramount. It may be necessary to deliberately downgrade the treatment objective from “anatomic cure” to “infection control.” Accepting an imperfect outcome—such as leaving a deeply seated infected stent in situ—can be a prerequisite for patient survival. A strategy of limited debridement to reduce the infectious burden may create a therapeutic window for targeted antibiotics to become effective and could potentially facilitate a definitive surgical intervention at a later stage.
Conclusion
For patients with central venous stent infection and poor physiological reserve, a strategy of “palliative debridement combined with restricted drainage” represents a feasible salvage approach. This case also serves as a critical warning that infection following the implantation of long-segment central venous stents can be catastrophic, underscoring the paramount importance of prevention.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This case report was granted an ethics approval waiver by the Institutional Review Board of South China Hospital Affiliated to Shenzhen University since it contains no identifiable patient information and retrospectively analyzes anonymized clinical data. All imaging and clinical materials were fully de-identified prior to analysis.
Informed consent
Informed verbal consent was obtained from the patient to publish the information and images anonymously.