
Abstract
Central venous occlusion is a prevalent cause of vascular access failure among hemodialysis patients, and endovascular treatment represents the preferred approach; however, intraoperative complications demand meticulous attention.1 We report a case of a 69-year-old male patient with end-stage diabetic nephropathy who had been undergoing maintenance hemodialysis via a left wrist arteriovenous fistula for 3 years. He presented with swelling of the left upper limb and face due to left brachiocephalic vein occlusion and underwent percutaneous transluminal angioplasty in conjunction with covered stent implantation under digital subtraction angiography guidance. After full stent deployment, the pull line became trapped during its withdrawal. We resolved the complication by stabilizing the stent with an angiographic catheter, preventing displacement and vascular injury. Unlike previously reported bailout techniques that require specialized balloon stabilization, this method utilizes a standard 5 F angiographic catheter—a readily available device in most interventional suites—to stabilize the stent edge and facilitate pull-line retrieval. This approach offers a simpler, more accessible alternative for managing this rare complication, particularly in resource-limited settings. In conclusion, Viabahn stent deployment with entrapment of the pull line is a rare complication. When pull line entrapment occurs, this technique can effectively resolve the complication while minimizing the risk of stent migration and vascular injury, provided that resistance is not excessive. Careful fluoroscopic monitoring and readiness to abort the procedure if significant resistance is encountered are essential.
Background
Percutaneous transluminal angioplasty (PTA) has become the preferred treatment for central venous stenosis in hemodialysis patients. Our center recently encountered a rare complication during Viabahn stent deployment for left brachiocephalic vein stenosis, in which the pull line was trapped between the stent and the vascular wall. Through an innovative approach of withdrawing the delivery rod and threading the pull line through a 5 F angiographic catheter to secure the stent edge, the pull line was successfully retrieved. This case report aims to comprehensively document the details of this case, extract valuable insights, and offer practical guidance for clinical practice to mitigate the risk of similar complications.
Pull-line entrapment during Viabahn deployment is a rare but potentially catastrophic complication with limited reported experience in the literature. To date, most published reports have focused on deployment failures in aortic or peripheral arterial applications, with central venous deployment complications remaining largely undocumented. Eilenberg et al. described the only previously reported bailout technique for Viabahn pull-line entrapment, which occurred during branched thoracic endovascular aortic repair. 2 Their successful management employed a modified 5 F Lindh catheter (side-hole catheter) combined with balloon stabilization to separate the locked pull line from the stent graft. While effective, this approach requires specialized catheter modifications and additional balloon catheters, which may not be readily available in all clinical settings, particularly in urgent scenarios or resource-limited environments.
The present case adds new knowledge in three key aspects: (1) to our knowledge, it represents the first reported case of pull-line entrapment during central venous (brachiocephalic vein) Viabahn deployment in a hemodialysis patient; (2) it demonstrates a simplified bailout technique utilizing only a standard 5 F angiographic catheter, eliminating the need for specialized equipment or additional balloon catheters; and (3) it provides practical guidance applicable to resource-limited settings where immediate access to specialized bailout tools may be unavailable. This case therefore may help fill a gap in the literature regarding manageable, low-resource alternatives for this rare but serious complication. The following case illustrates this complication and our management approach.
Case presentation
A 69-year-old male patient was admitted to our hospital on November 20, 2023, with the complaints of “undergoing maintenance hemodialysis via a left wrist arteriovenous fistula (AVF) for over 3 years and swelling of the left face and upper limb for half a year.” The patient had an 8-year history of diabetes mellitus. The patient underwent left forearm AVF creation in May 2020. The AVF matured 6 weeks post-operation and was subsequently utilized for hemodialysis. Notably, the patient had not undergone hemodialysis prior to AVF creation; this was his first vascular access. However, 6 months prior to admission, the patient developed swelling of the left face and upper limb.
Physical examination on admission: An old surgical scar was visible ~4 cm above the left forearm wrist crease. The AVF exhibited a palpable thrill, and a distinct vascular murmur was audible. The left upper limb and the left side of the face were swollen. No obvious varicose veins were detected on the chest wall. The skin temperature of the left hand was slightly lower, and there was no tenderness.
Imaging evaluation: CT angiography revealed that the left brachiocephalic vein was compressed and occluded, with collateral formation, which was consistent with the diagnosis of central venous occlusion (Figure 1).
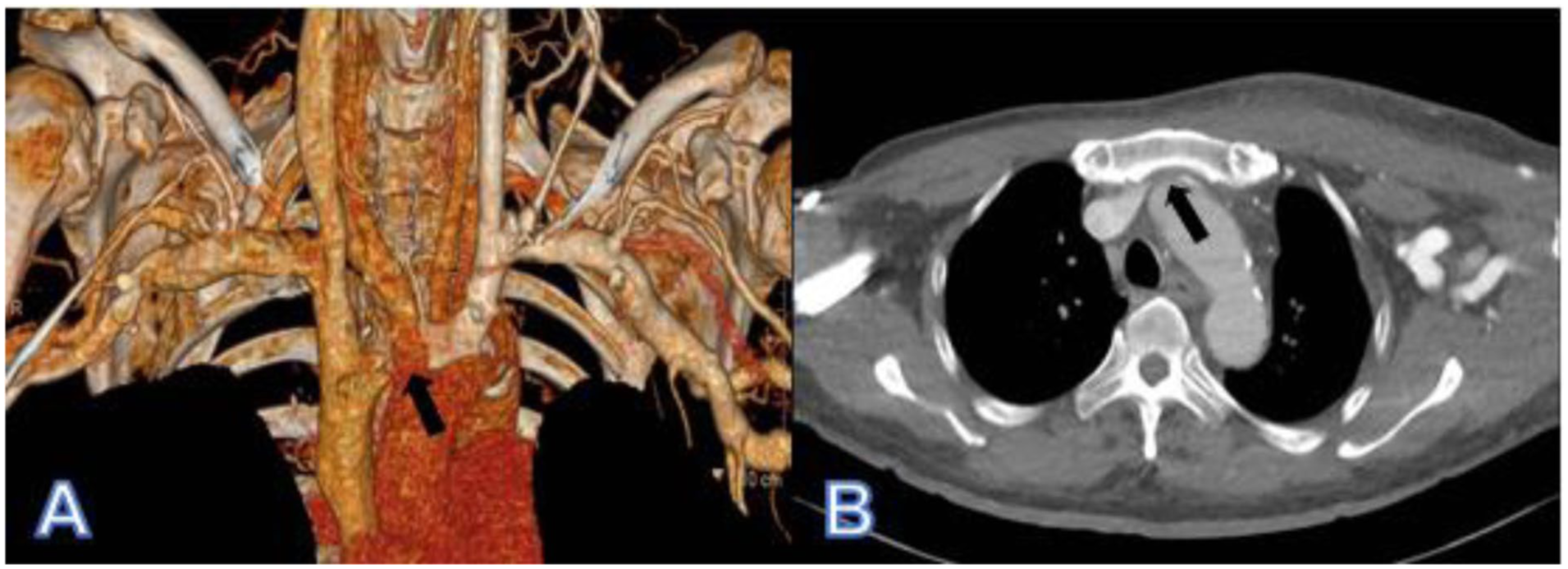
CT angiography demonstrates the compression and occlusion of the left brachiocephalic vein: (a) 3D reconstruction of CT angiography showing the occlusion of the left brachiocephalic vein and (b) cross-sectional view of CT angiography depicting the compressed and occluded left brachiocephalic vein. The black arrow indicates compression and occlusion of the left brachiocephalic vein.
Operational procedure
The patient was placed in the supine position. The left upper limb was routinely disinfected, surgical draped, and locally anesthetized. Under ultrasound guidance, the left forearm AVF was punctured, and a 6 F vascular sheath was inserted. Guided by digital subtraction angiography (DSA), a 0.035-inch guidewire was advanced along the vascular sheath into the left brachiocephalic vein, and a 5 F angiographic catheter was introduced along the guidewire. Angiography via the catheter confirmed the occlusion of the left brachiocephalic vein (Figure 2(a)). Subsequently, the vascular sheath was exchanged for a 12 F one. After the guidewire traversed the occluded lesion, balloons with diameters of 7 mm × 6 cm (Dingke Medical Technology (Suzhou) Co., Ltd., Suzhou, China; Figure 2(b) and (c)) and 12 mm × 6 cm (Boston Scientific Corporation, Marlborough, MA, USA; Figure 2(d) and (e)) were used sequentially for PTA. After predilation, a Super-stiff guidewire was advanced, and a 13 mm × 5 cm GORE VIABAHN endoprosthesis (W.L. Gore & Associates, Inc., Flagstaff, AZ, USA) was positioned at the lesion site over the guidewire. Following confirmation of stent placement, the pull line was used to deploy the stent. During deployment, a slight hesitation in the pull line was noted. Upon further traction, the pull line was trapped and could not be withdrawn. Additional force applied to the pull line resulted in severe chest pain for the patient, prompting immediate cessation of traction. The manufacturer was notified, and it was determined that the pull line was likely jammed between the stent graft and the vascular wall (Figure 3(a)).
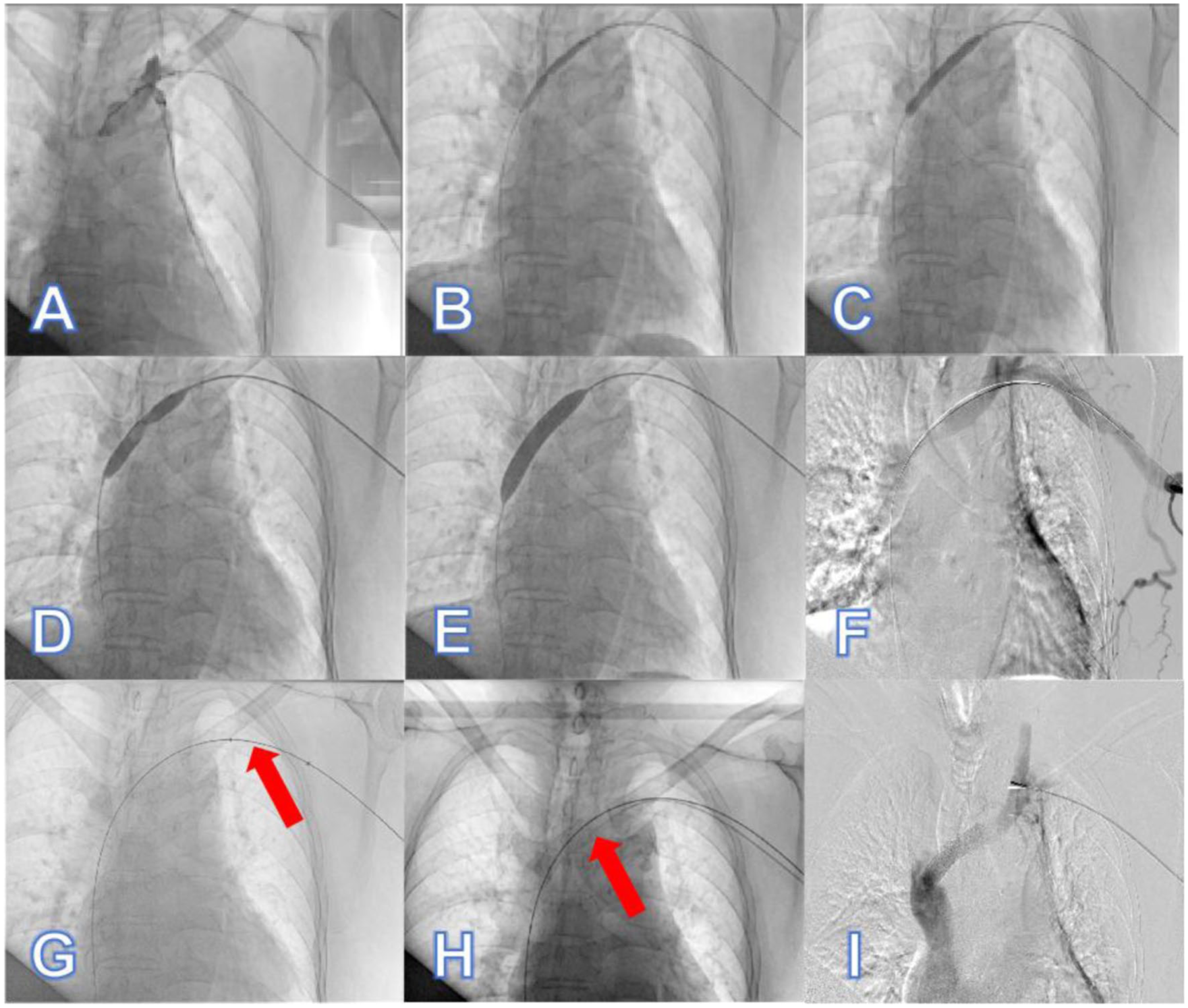
Operational procedure: (a) DSA angiography confirms occlusion of the left brachiocephalic vein, (b, c) balloon angioplasty of the occluded segment with a 7 mm × 6 cm balloon, (d, e) balloon angioplasty of the occluded segment with a 12 mm × 6 cm balloon, (f) angiography after balloon angioplasty, (g) after full stent deployment, the pull line was trapped during withdrawal, preventing retrieval of the delivery system (The red arrow indicates the delivery shaft that has not been withdrawn after stent deployment), (h) the pull line is threaded through an angiographic catheter, which is advanced to the stent edge to stabilize the stent and prevent movement (The red arrow indicates that the angiographic catheter is pushed to the edge of the stent), and (i) final angiography after successful retrieval of the pull line, demonstrating stable stent positioning and no contrast extravasation.
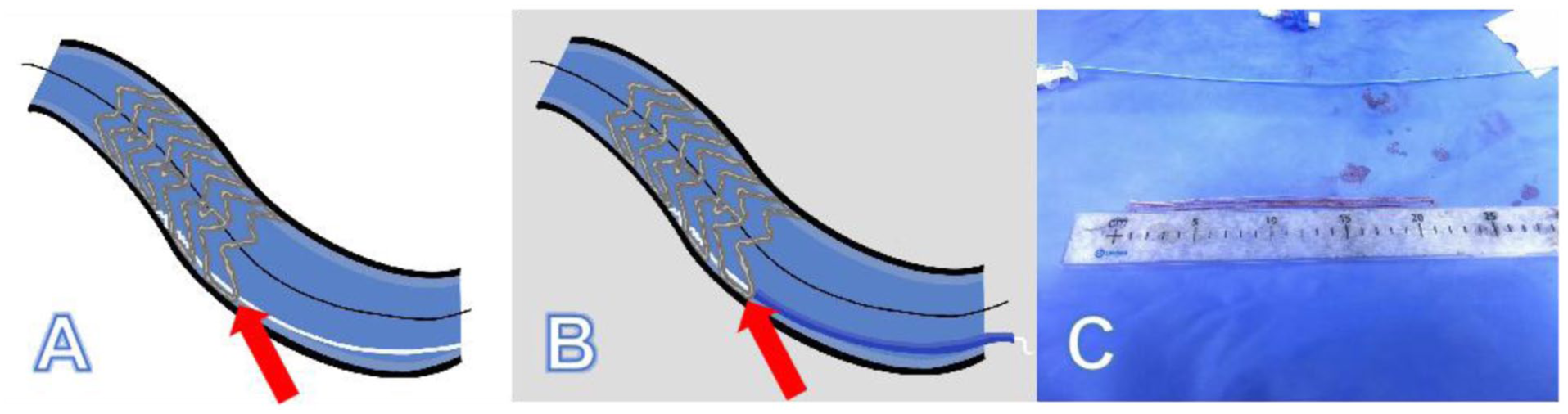
Schematic illustration of the jammed pull line and its removal: (a) The red arrow indicates that the stent pull line was stuck between the vessel wall and the stent, (b) The red arrow indicates that the angiographic catheter fixing the edge of the stent, and (c) the removed stent pull line.
Innovative treatment strategy
The delivery rod was withdrawn, and an angiographic catheter was advanced over the guidewire to the stent site. The length from the vascular sheath to the stent was measured, and the excess portion of the angiographic catheter was trimmed.
The pull line was then slowly advanced through the lumen of the angiographic catheter. To facilitate this step, the operator gently manipulated the pull line while keeping the catheter stationary; if resistance was encountered, a 0.014-inch guidewire could be inserted alongside the pull line to create a pathway or to gently push the line through the catheter lumen.
Once the pull line passed through the catheter, the angiographic catheter was advanced to the edge of the stent over the pull line. The catheter tip was positioned to abut the stent edge, providing forward counter-pressure that stabilized the stent during subsequent line retrieval (Figure 3(b)). This step was performed under continuous fluoroscopy to confirm that the catheter did not displace the stent.
The pull line was then carefully withdrawn under DSA guidance to monitor for stent displacement and assess the patient’s chest pain. The pull line was successfully retrieved. Immediate post-procedure angiography demonstrated stable stent positioning with no contrast extravasation (Figure 2(i)).
Notably, in this case, the pull line entrapment occurred after the stent was fully deployed and had achieved stable apposition to the vessel wall. Consequently, the delivery rod was no longer mechanically coupled to the stent and could be withdrawn normally without risk of stent migration.
The edema of the left face and upper limb of the patient completely resolved within 24 h after the operation. After 15 months of follow-up, there was no recurrence of swelling in the left face and upper limb, and the AVF function remained stable. Given the absence of established guidelines for antithrombotic therapy following venous stenting and the patient’s inherent bleeding risk due to hemodialysis, the decision was made not to administer routine anticoagulation or antiplatelet therapy post-procedurally. The patient was closely monitored for signs of stent thrombosis.
Discussion
This case report describes a rare complication of Viabahn stent deployment—pull line entrapment after full stent expansion—and presents a simple, resource-conscious bailout technique using only a standard angiographic catheter. Beyond describing the technical solution, this case offers an opportunity to analyze the mechanistic basis of this complication and derive insights that may inform clinical practice and future device design.
Central venous stenosis is a common complication in hemodialysis patients, with a complex pathogenesis potentially related to vascular device use (such as central venous catheter and pacemaker implantation), hemodynamic changes, and external compression.3–8 In this case, left brachiocephalic vein stenosis caused swelling in the left upper limb and face. The anatomical location prone to compression and the patient’s hyperglycemic state due to diabetic nephropathy may have been primary contributors.4,6,7
The entrapment of the pull line in this case may be understood at three interconnected levels: At the macro-anatomical level, the left brachiocephalic vein may possess unique geometric features that could predispose to deployment complications. It follows a tortuous course as it traverses the retrosternal space, where it may be susceptible to external compression between the sternum and the great arteries.4,7,9,10 Following balloon dilation of a chronic occlusion, the vessel wall may exhibit acute elastic recoil—a phenomenon well-documented in venous lesions, particularly at sites of external compression.11,12 We hypothesize that such recoil occurred rapidly after balloon deflation, reducing the lumen diameter before the stent was fully expanded and trapping the pull line between the stent fabric and the vessel wall.
At the tissue level, the patient’s underlying diabetic nephropathy likely contributed to altered vascular biomechanics. Chronic hyperglycemia induces endothelial dysfunction, advanced glycation end-product accumulation, and increased vascular stiffness.10,13 In dialysis patients, central veins often exhibit fibrotic changes from prior catheter placements and repeated wall stress from high-flow AVF.7,14 These pathological changes reduce vessel compliance and may increase the tendency for irregular, non-uniform recoil following dilation.
At the procedural level, the Viabahn’s pull-line deployment mechanism requires smooth, continuous traction for optimal results. If the pull line encounters resistance—whether from vessel wall irregularity, acute recoil, or friction against the stent fabric—the deployment force may become uneven. In our case, we hypothesize that acute elastic recoil created a focal narrowing that contacted the pull line before the stent was fully expanded, effectively pinning it against the vessel wall.
Understanding the mechanism of entrapment may help explain why our technique succeeded. The trapped pull line was pinned between the stent and the vessel wall by elastic recoil. Simply pulling on the line would risk tearing the stent fabric, displacing the stent, or injuring the vessel. By advancing a trimmed angiographic catheter over the guidewire to abut the stent edge, we achieved three mechanical effects:
Stent stabilization: The catheter provided forward counter-pressure, preventing the stent from being pulled toward the operator during line retrieval.
Vessel wall tenting: The catheter tip gently displaced the vessel wall away from the stent edge, creating space for the trapped line to be released.
Controlled line pathway: Threading the pull line through the catheter created a protected channel, preventing the line from re-engaging with the stent or vessel wall during withdrawal.
This approach may differ mechanistically from previously reported balloon fixation techniques. Balloon inflation applies radial force inside the stent, which may stabilize the device but also subjects the vessel wall to additional barotrauma and does not address the direct pinching of the line between stent and wall. Our catheter-based method may address the entrapment mechanism more directly by intervening at the interface where the line is trapped, without adding radial stress to the vessel.
A brief review of the literature reveals several approaches to Viabahn deployment complications. Eilenberg et al. described using a modified side-hole catheter combined with balloon fixation to release a locked deployment line during branched thoracic endovascular aortic repair. 2 To our knowledge, no previous report has described a technique using only a standard, modified angiographic catheter to stabilize the stent and retrieve a trapped pull line in the venous circulation. The simplicity and universal availability of this method may make it particularly valuable in resource-limited settings or as a first-line attempt before escalating to more complex interventions.
Based on our experience with this single case, we offer the following observations that may assist clinicians facing similar complications:
When to consider this technique: If pull line entrapment occurs after full stent deployment, and the line is intact and accessible, the catheter-based approach may be attempted under continuous fluoroscopic guidance, provided the resistance to gentle traction is not excessive.
Safety caveats: The pull line should be withdrawn slowly and gently. If significant resistance is encountered, traction must be halted immediately. The operator should have a low threshold for considering alternative bailout strategies, including surgical conversion, if the line cannot be retrieved with minimal force.
Preventive considerations: Based on our hypothesized mechanism, factors that may reduce entrapment risk include: (1) adequate predilation to minimize acute recoil, (2) smooth, uninterrupted pull line traction during deployment, and (3) careful patient selection, recognizing that heavily calcified or fibrotic vessels may pose higher risk. However, these are theoretical considerations derived from a single case and require validation.
This study is limited by its single-case nature and short-to-medium-term follow-up (15 months). Future validation of this technique’s applicability will require multicenter studies. Additionally, emerging technologies such as drug-coated balloons and stents, which inhibit neointimal hyperplasia and reduce restenosis risk, may offer improved patency rates.15–17 Biodegradable stent grafts could further minimize complications and warrant exploration in central venous lesions.
In conclusion, pull-line entrapment after Viabahn stent deployment is a rare but potentially serious complication. Understanding its likely mechanism—acute elastic recoil pinning the line between stent and vessel wall—may guide rational bailout strategies. The technique described here, using only a standard angiographic catheter to stabilize the stent and retrieve the trapped line, offers a simple, resource-conscious option that could be considered when this complication arises. However, these observations derive from a single case, and clinicians should exercise judgment based on individual patient anatomy, the degree of resistance encountered, and available resources. Further research is needed to establish optimal management strategies for this uncommon but challenging complication.
Footnotes
Author contributions
Yafei Bai and Na An wrote the manuscript. Mingzhi Xu and Na An collected the clinical data. Hong Li and Ruman Chen revised and finalized the manuscript. All the authors have read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project supported by Hainan Province Clinical Medical Center.
Ethical approval
All procedures performed in this study involving human participants were in accordance with the ethical standards of the institutional or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
We obtained written informed consent from the patient, as well as his legally authorized representative, for the publication of this case report. Approval for publication was obtained from the Ethics Committee of Hainan General Hospital, China.
Data availability statement
No datasets were generated or analyzed during the current study.