
Abstract
Background:
Intravenous therapy involves high-volume, invasive procedures that are inherently associated with patient discomfort and distress. When not managed optimally, such procedures can directly impact treatment efficacy and carry risks of severe complications. Intravenous therapy quality monitoring is essential for patient safety, yet standardized, practical tools for hospital-wide audits remain a critical gap.
Objective:
This study aimed to develop and refine a practical, electronic quality assessment tool for hospital-wide intravenous therapy surveillance, and to evaluate its feasibility in clinical practice. This is Phase I of a larger project; Phase II will apply the tool to identify outcome gaps and drive improvement.
Methods:
A multidisciplinary team developed the initial Hospital Intravenous Therapy Quality Assessment Tool (HIT-QAT) based on international and national standards. The tool underwent 14 iterative refinement cycles through hospital-wide cross-sectional surveys from June 2016 to May 2023. Each cycle involved: pilot testing, standardized auditor training, full-scale audit, data analysis, feedback sessions, and tool revision. Feasibility metrics included audit completion time, data completeness, and user acceptance.
Results:
The finalized HIT-QAT structure comprises seven sections: Introduction, Infusion Status Basics, Medication Usage, Vascular Access Device (VAD) Selection, VAD Insertion & Management (Butterfly devices, Peripheral intravenous catheter (PIVC), Midline catheter, CVC, PICC, PORT, Other devices), Infusion Device Usage, Instructions. HIT-QAT is an electronic, mobile-accessible survey with automated skip logic. Across 14 audits conducted from 2016 to 2023, A total of 22,789 VADs were assessed by 67–76 trained audit liaisons per cycle. All audit liaisons completed a standardized 1-h training with zero resistance.
Conclusion:
The HIT-QAT is a feasible, practical, and efficient electronic tool for hospital-wide intravenous therapy quality assessment. This paper reports Phase I: tool design, refinement, and feasibility testing. Future studies (Phase II) will apply the tool to systematically identify practice deficiencies, track outcomes, and evaluate quality improvement interventions.
Key messages
What is already known on this topic—summarize the state of scientific knowledge on this subject before you did your study and why this study needed to be done Although INS Infusion Therapy Standards of Practice and China’s Nursing Practice Standards for Intravenous Therapy guide clinical practice—and prior studies addressed infusion medication use, nurses’ complication knowledge, and outpatient assessment tools—no standardized instrument exists for auditing infusion quality or identifying improvement opportunities.
What this study adds—summarize what we now know as a result of this study that we did not know before This study design, refine, and assess the feasibility of a practical Hospital Intravenous Therapy Quality Assessment Tool (HIT-QAT). The tool demonstrates significant practical value for clinical infusion quality management.
How this study might affect research, practice or policy—summarize the implications of this study
Research Implications Standardized Metrics: Provides a validated framework for quantifying infusion therapy quality, enabling cross-institutional comparisons and meta-analyses. Methodological Innovation: Demonstrates how iterative refinement (14 cycles) can transform clinical guidelines into actionable audit tools, offering a model for other quality improvement initiatives.
2. Clinical Practice Implications Real-Time Quality Monitoring: Enables rapid (<2 min/bed), electronic audits to identify. Targeted Interventions: Data-driven reports direct quality improvement resources to high-risk areas.
Introduction
From a hospital-wide infusion therapy quality management perspective, intravenous therapy is characterized not only by its high utilization volume and invasive nature, but also by its direct implications for patient discomfort and distress, therapeutic outcomes, and the risk of severe complications.1–5 Evidence indicates poor adherence to safe injection and infusion practices, with non-compliance predominantly involving: Aseptic technique (79%), rubber septum disinfected with alcohol (66%), labeling of all intravenous therapy lines and medications with date and time (83%), compliance with multidose-vial policy (77%), Multidose vials for single-patient use (84%), Sharp disposal safety (84%), using trays instead of clothing/pockets to carry medications (81%). 6
Although INS Infusion Therapy Standards of Practice and China’s Nursing Practice Standards for Intravenous Therapy guide clinical practice—and prior studies addressed infusion medication use,7–9 nurses’ complication knowledge,10,11 and outpatient assessment tools 12 —no standardized instrument exists for auditing infusion quality or identifying improvement opportunities.
The primary objective of this study was to develop and iteratively refine a practical, electronic quality assessment tool for hospital‑wide intravenous therapy surveillance, and to evaluate its feasibility (audit time, data completeness, user acceptance) in real‑world clinical settings.
Importantly, this study does not aim to comprehensively analyze clinical outcomes or quality gaps identified by the tool. That constitutes a separate second phase of our research program, which will be reported in future publications. The present manuscript focuses solely on Phase I: tool creation, refinement, and feasibility validation.
This study represents Phase I of a larger research program: the development and feasibility testing of the HIT-QAT. Phase II will involve systematic analysis of audit‑identified quality gaps, longitudinal trends, and the impact of targeted interventions. The current paper does not present outcome data but instead establishes the tool itself as a practical, ready‑to‑use instrument for hospital‑wide quality surveillance.
Methods
Basis for the initial design of the Intravenous Therapy Assessment Tool
Core members of the hospital’s Intravenous Therapy Team (IV Team) designed the initial Hospital Intravenous Therapy Quality Assessment Tool (HIT-QAT). This tool was based on the current state of intravenous therapy practice within the hospital, combined with the Nursing Practice Standards for Intravenous Therapy (WS/T 433-2013) 13 and the Infusion Nursing Standards of Practice (2011 edition). 14 The question structure of the initial HIT-QAT primarily encompassed five categories: (1) Inappropriate VAD selection; (2) Incorrect puncture site selection; (3) Catheter Maintenance; (4) Transparent dressing securement and Maintenance; (5) Occurrence and management of complications.
Iterative refinement process of the HIT-QAT
The HIT-QAT was developed and refined through a structured, 7-stage iterative cycle (Figure 1), repeated across 14 hospital-wide audits from 2016 to 2023. This cycle ensures that tool evolution was directly driven by clinical data and frontline feedback.
(1) Schedule audits
Set dates for hospital-wide audits. Audits were scheduled approximately twice per year (every 4–8 months) over the study period from June 2016 to May 2023. The schedule was occasionally adjusted (e.g. reduced frequency during the COVID-19 pandemic in 2020–2021) due to hospital operational constraints.
(2) Conduct Pilot Survey
A pilot survey was conducted prior to each formal audit cycle, following every major revision of the HIT-QAT. The initial pilot survey was carried out in June 2016 to test the electronic questionnaire’s skip logic, data completeness, and field usability. Subsequent pilots involved 60–100 patients from 2–3 representative nursing units to verify revised items and functionality before each full-scale hospital audit. Minor wording adjustments were made based on pilot feedback.
(3) Pre-audit training
One Intravenous Therapy Specialist Nurse per nursing unit is designated to attend the pre-audit training session. Training content includes: Audit procedures, Operation guidelines for the HIT-QAT, Key considerations, Material preparation protocols, Staff allocation plans (either one Audit Liaison per nursing unit or paired liaisons jointly auditing two units). Each pre-audit training session lasts exactly 1 h.
(4) Implement Formal Intravenous Therapy Assessment Survey
Audit Liaisons visit assigned units during morning hours to evaluate every VAD per patient, document and photograph each VAD, and submit consolidated photos to the IV Team.
(5) Organize Data & Generate Quality Audit Report
The IV Team compiles and analyzes hospital-wide VAD audit data to generate a Quality Audit Report. The report structure includes: background, objectives and tools, current practice overview, problem analysis, and solutions.
(6) Convene Hospital-Wide Intravenous Therapy Quality Feedback Session
The IV Team convenes a hospital-wide debriefing meeting with all Intravenous Therapy Audit Liaisons to review audit findings from high-risk nursing units, identify nursing deficiencies in vascular access management, and report complications. Subsequently, the IV Team organizes targeted quality improvement (QI) activities to address these issues. 15
(7) Refine HIT-QAT Based on Findings
The HIT-QAT underwent continuous, evidence-based refinement across 14 audit cycles. Each revision was a direct response to specific operational challenges and clinical gaps identified through quantitative data and frontline feedback, ensuring the tool evolved in step with practical necessity.
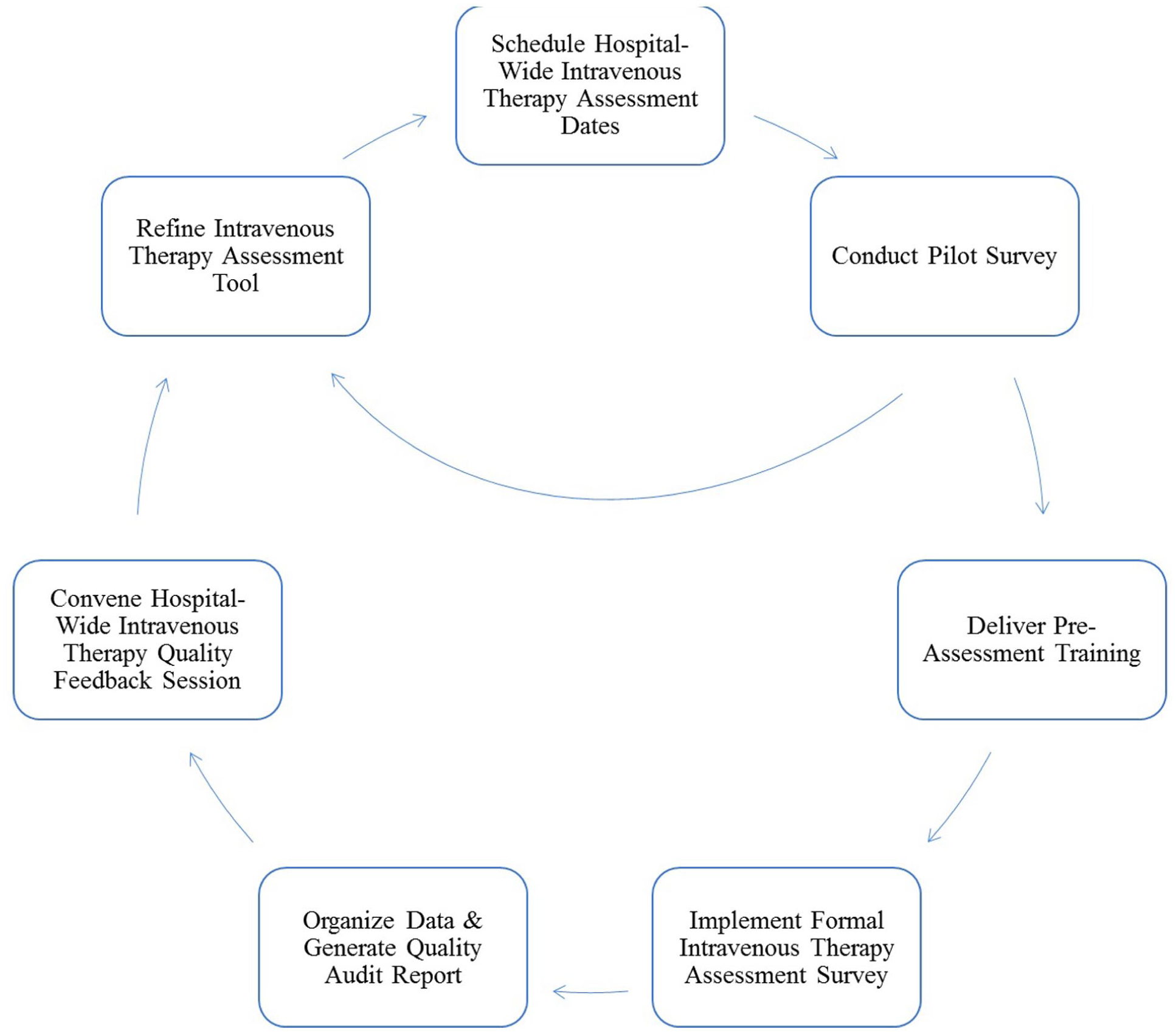
Iterative refinement process of the Hospital Intravenous Therapy Quality Assessment Tool (HIT-QAT).
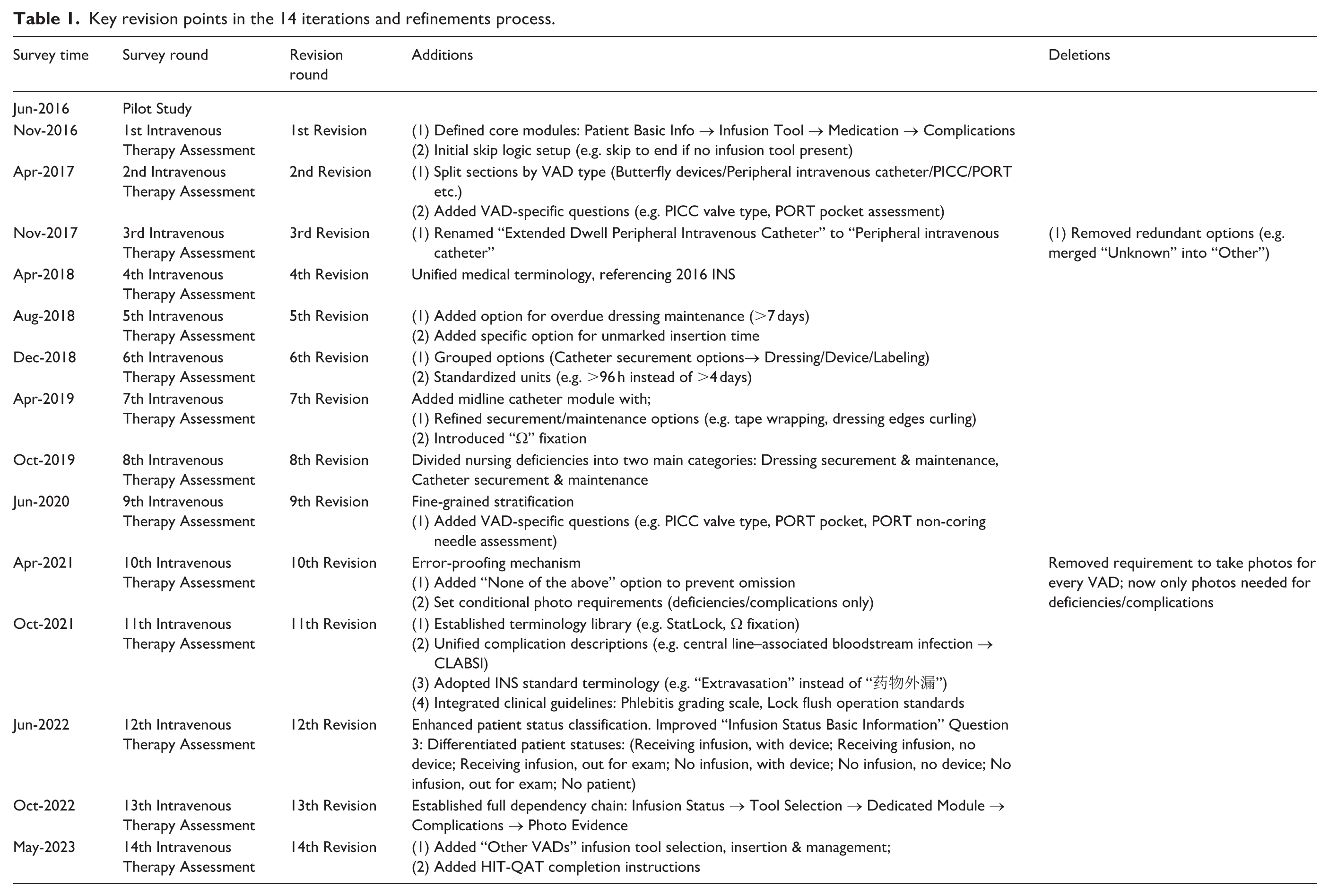
For instance, early audits revealed inconsistent documentation of peripheral catheters (e.g. “Extended Dwell” vs standard Peripheral intravenous catheter (PIVC)), prompting a unification of terminology in the 3rd revision to ensure data reliability. To capture latent management failures, the 5th revision introduced explicit options for “overdue dressing maintenance (>7 days)” and “unmarked insertion time,” transforming subjective oversight into measurable audit items. As clinical practice advanced, the addition of a dedicated midline catheter module in the 7th revision enabled standardized assessment of this increasingly utilized device.
Subsequent iterations focused on enhancing efficiency and precision. Auditor feedback on excessive workload led to a pivotal conditional photo requirement in the 10th revision, mandating images only for defects or complications, thereby streamlining the audit process without compromising data integrity. To resolve variability in complication reporting, the 11th revision embedded a visual phlebitis grading guide and adopted standardized INS terminology (e.g. “Extravasation”), significantly improving inter-rater agreement. Finally, the 12th revision refined patient status classification into seven distinct categories, allowing for nuanced analysis of resource utilization and patient flow.
All revisions were made concurrently with updates to key guidelines, including the INS Infusion Therapy Standards of Practice (2016 editions and 2021 editions),16,17 nursing practice standards for intravenous therapy (WS/T 433-2023), 18 and the Guidelines for the Prevention of Intravascular Catheter-related Infections (2011 edition) by CDC/Healthcare Infection Control Practices Advisory Committee (CDC/HICPAC). 19
Electronic implementation and practical features
To realize its practical utility for hospital-wide audits, the HIT-QAT was implemented as an electronic survey on a secure, cloud-based questionnaire platform (Wenjuanxing, www.wjx.cn). This digital format was pivotal for enforcing the complex skip logic and ensuring data completeness during large-scale audits.
Key features of the electronic implementation include:
(1) Automated Skip Logic: The platform’s built-in logic functions automatically presented or hid questions based on previous responses (e.g. displaying the PICC-specific module only if “PICC” was selected as the vascular access device). This eliminated auditor error in navigating the questionnaire and guaranteed that all conditional data were captured.
(2) Device Independence & Field Usability: The survey was accessible via a unique, permanent URL on any internet-connected device, including tablets and smartphones used by auditors at the bedside. A corresponding QR code (Supplemental Figure S1) further facilitated rapid access in clinical settings.
(3) Data Integrity Safeguards: Mandatory completion of key fields (e.g. VAD type, presence of complications) was enforced before submission, preventing inadvertent omission of critical data—a feature not possible with paper-based audits.
(4) Immediate Consolidation: All data and uploaded photographic evidence were instantly consolidated into a central database, enabling real-time data cleaning and analysis by the research team.
The final versions of the electronic questionnaire in both English and Chinese are permanently available for review via the following links: https://v.wjx.cn/vm/tHy2ryd.aspx# (English); https://v.wjx.cn/vm/OZCGNaP.aspx# (Chinese). A screenshot illustrating the user interface is provided in Supplemental Figure S1.
Feasibility validation for the HIT-QAT
(1) Mean Audit Duration
We calculated audit duration per bed (seconds) and per nursing unit (minutes) using data from the last five audits (stabilization period). The mean audit duration (seconds per bed, minutes/nursing unit) evaluates operational feasibility.
(2) Data Completion Rate
Analyze missing data patterns and completion rates during tool implementation to assess clinical viability.
(3) Audit Liaison Training Duration and Acceptance
Evaluate pre-audit training time for Audit Liaisons and document resistance incidents to determine tool acceptance levels.
Results
Final structure and content of the HIT-QAT
The finalized structure of the HIT-QAT comprises seven sections: Introduction, Basic Information on Infusion Status (3 items), Medication Usage Status (2 items), VAD Selection (1 item), VAD Insertion and Management (Butterfly Device Insertion and Management (4 items), PIVC Insertion and Management (7 items), Midline Catheter Insertion and Management (8 items), CVC Insertion and Management (8 items), PICC Insertion and Management (9 items), PORT Insertion and Management (7 items), Other VADs Insertion and Management (1 item)), Status of Infusion Equipment Usage (2 items), and Instructions. The structural diagram of the HIT-QAT is shown in Figure 2. The full HIT-QAT is provided in the Supplemental Appendix.
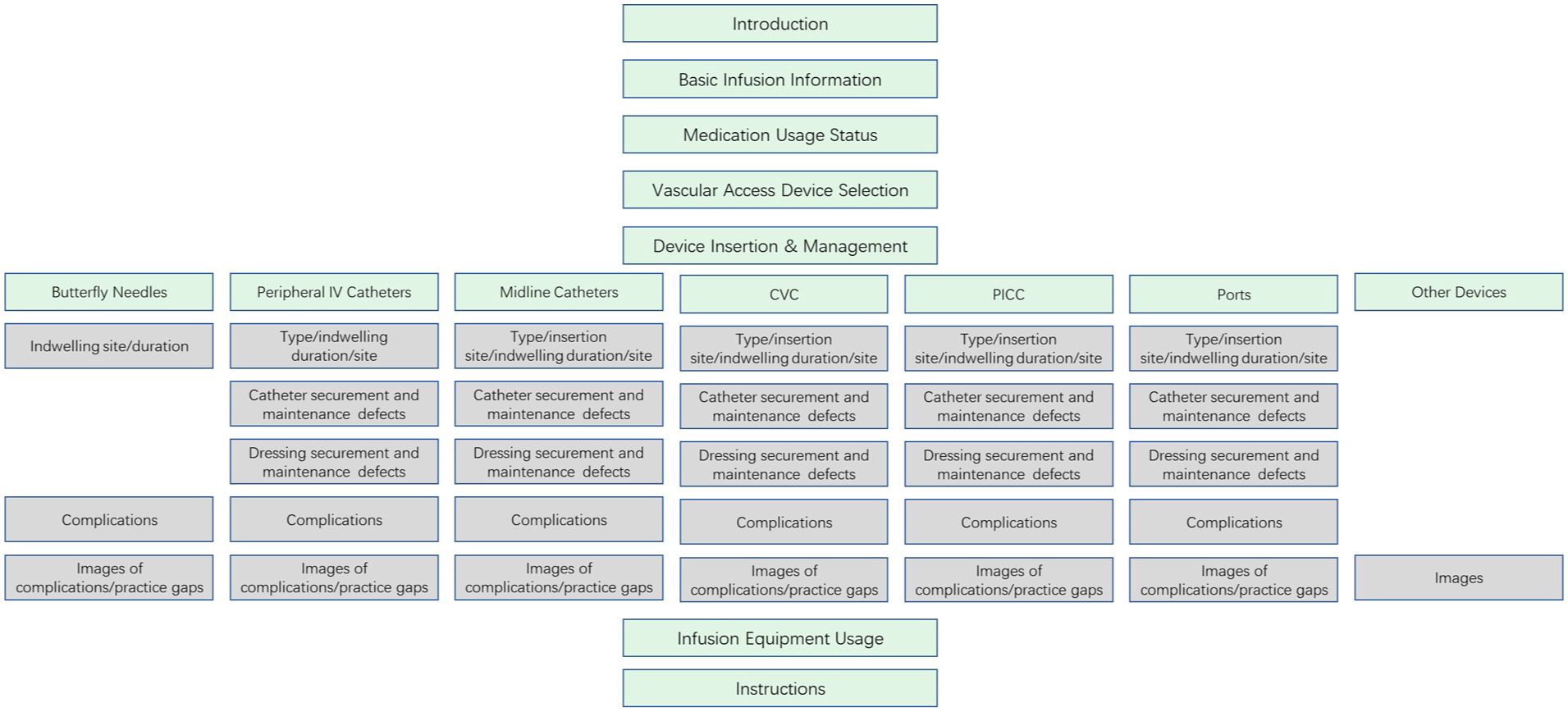
Structural diagram of the HIT-QAT.
Key changes in the iterative process
Critical revision points during the 14 refinement iterations are detailed in Table 1.
Key revision points in the 14 iterations and refinements process.
Feasibility validation
Audit duration for intravenous therapy assessment
Audit duration data from Audits 10 through 14 were analyzed to calculate audit duration per bed (seconds) and per nursing unit (minutes; Table 2).
Audit duration per bed and per nursing unit for intravenous therapy assessment.
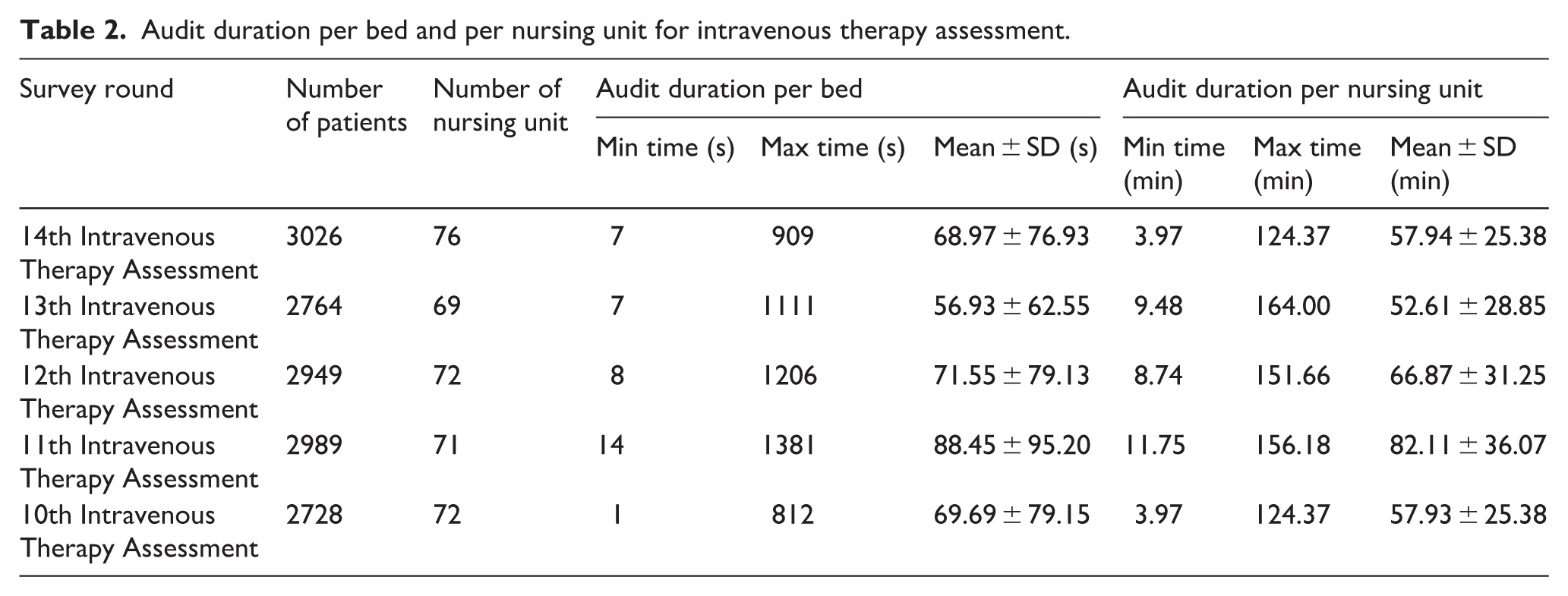
The substantial standard deviation in audit time reflects the inherent and expected clinical heterogeneity encountered during hospital-wide audits, rather than inconsistency in the tool itself. This variability is attributable to several predictable factors:
(1) Complexity of the VAD: A bed with a simple PIVC and no complications could be audited in under 60 s (e.g. verifying site and dressing). In contrast, auditing a patient with a multi-lumen central line (e.g. a PICC or CVC) necessitated a comprehensive check of each lumen’s securement, dressing, and flushing compliance, often requiring 3–5 min or more. For beds that were empty or with patients not receiving intravenous infusion therapy, the HIT-QAT allowed for rapid completion (often within 10–20 s) by answering a few screening questions before closing the audit.
(2) Presence and Number of Deficiencies/Complications: Beds with no issues required minimal documentation (a few clicks for “no deficiencies”). However, if the HIT-QAT identified a problem (e.g. phlebitis, loose dressing), the audit process automatically triggered mandatory documentation of specifics and photographic evidence upload, which significantly extended the time.
(3) Patient Factors and Environment: Audits on alert, communicative patients who could provide history were faster than on sedated or critically ill patients where all information had to be meticulously gathered from charts and physical assessment. Audits in crowded or high-acuity units (e.g. ICU) also naturally took longer.
(4) Auditor Familiarity: While all auditors received standardized training, a natural learning curve existed. Times typically stabilized after the first few audits of each cycle.
Data completion rate
An electronic data collection system was implemented, requiring Audit Liaisons to record VAD information using mobile devices. All fields in the electronic form were mandatory, ensuring a 100% completion rate through enforced response requirements.
Audit Liaison training duration and acceptance
A standardized 1-h group training session was conducted for all Audit Liaisons before each audit. Each nurse serves as the unit’s Intravenous Therapy Specialist Nurse. The IV Team resolved on-site issues in real-time, with no resistance incidents documented.
Key audit findings, impact, and illustrative case
A detailed breakdown of the audit scope is provided in Supplemental Table S2. In brief, each of the 14 audits covered 67–76 nursing units, with 1 designated auditor per unit depending on unit bed capacity. Across all audits, a total of 22,789 VADs were assessed, of which 19,093 (83.79%) PIVCs.
To substantiate the practical value of the HIT-QAT, we first summarize the spectrum of quality issues it identified across 14 audits, followed by a detailed case study demonstrating the complete audit-to-improvement cycle.
Spectrum of Prevalent Quality Deficiencies. Analysis of over 20,000 VAD assessments revealed consistent patterns of practice gaps. Table 3 ranks the top five quality deficiency categories by their overall weighted prevalence.
Top 5 quality deficiencies identified across 14 hospital-wide audits (June 2016–May 2023).
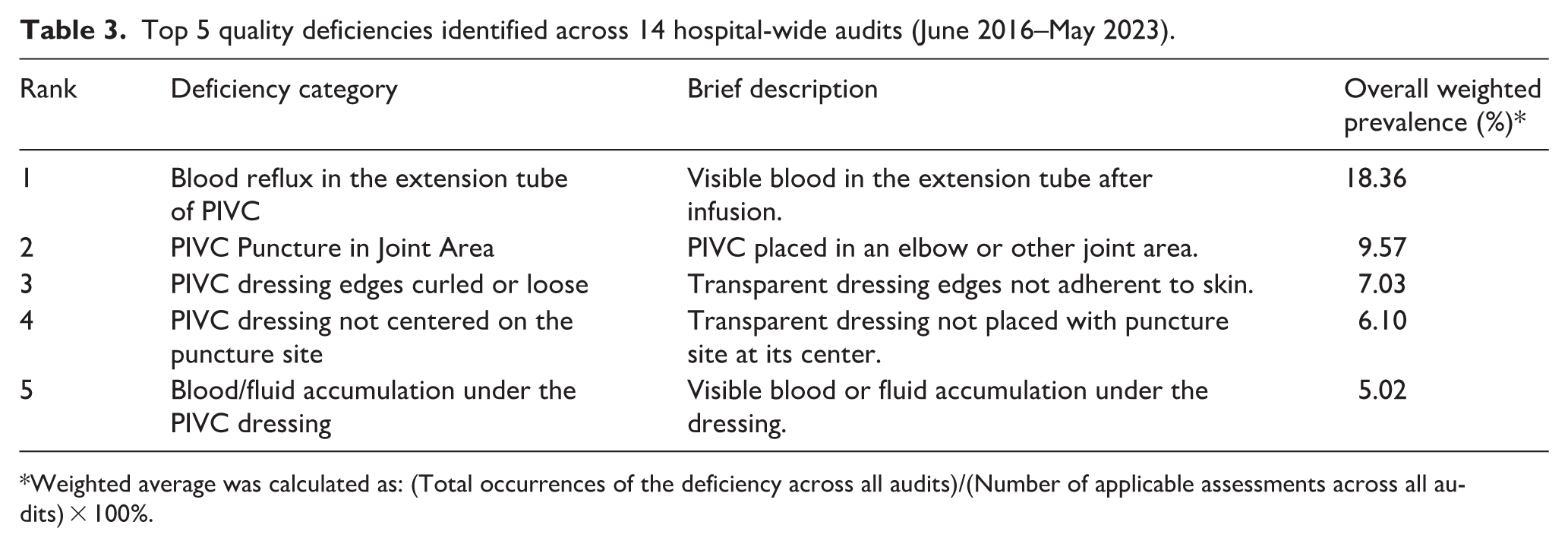
Weighted average was calculated as: (Total occurrences of the deficiency across all audits)/(Number of applicable assessments across all audits) × 100%.
To demonstrate the utility of the HIT-QAT in identifying specific, actionable quality gaps and monitoring the impact of targeted interventions, we present a longitudinal analysis of one key nursing-sensitive indicator: blood reflux in the extension tube of PIVCs. This defect was selected as an illustrative case because it is a common, directly observable issue that reflects compliance with post-infusion management protocols and is associated with increased risks of occlusion and infection.
Across the 14 hospital-wide audits conducted from June 2016 to May 2023, a total of 20,175 PIVC assessments were performed. The HIT-QAT enabled systematic tracking of this defect, as summarized in Figure 3. The complete numerical dataset for this analysis is provided in Supplemental Table S2. This closed-loop process—audit, feedback, intervention, and re-audit—exemplifies the HIT-QAT’s operational utility in driving tangible quality gains.
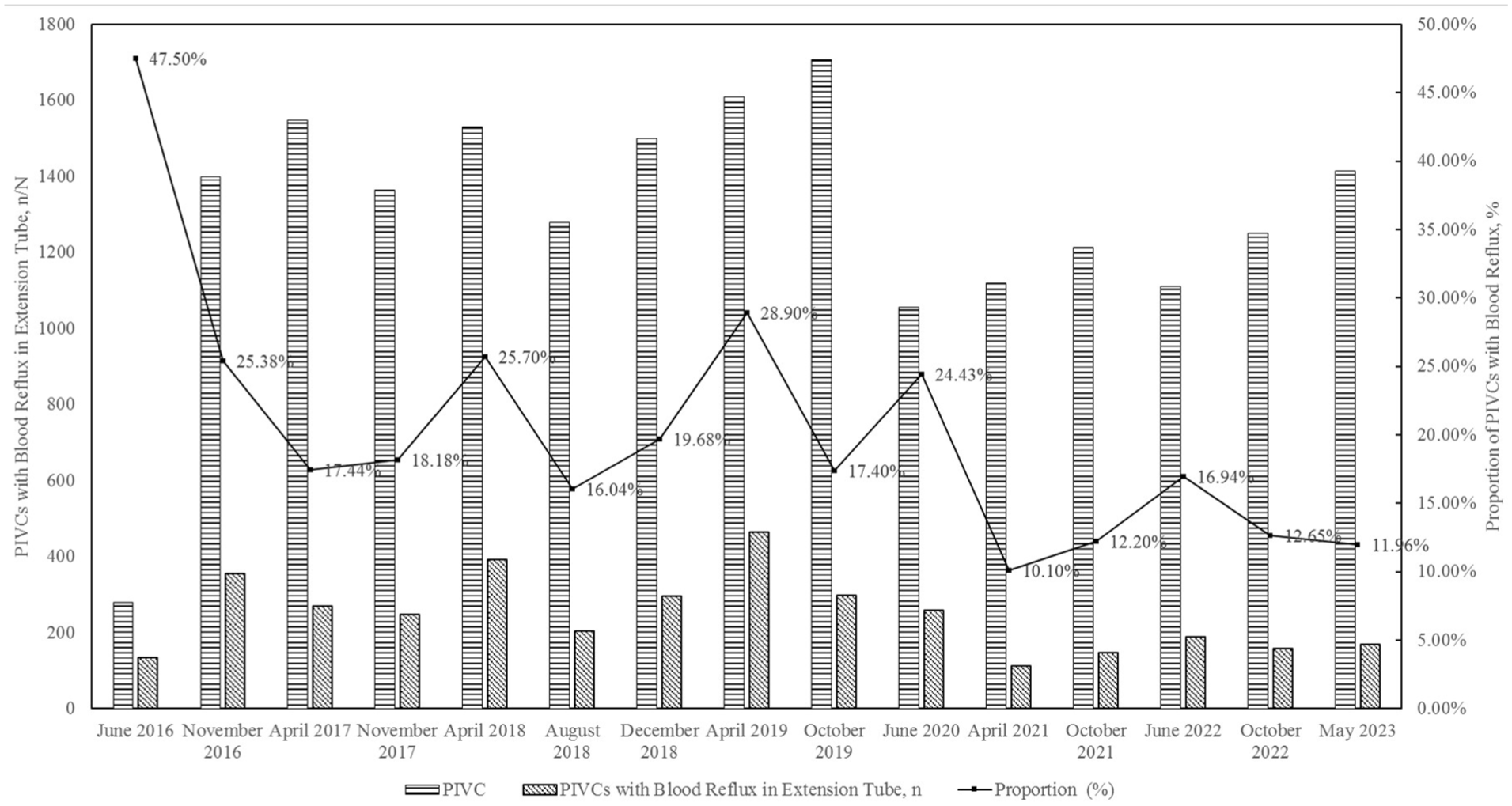
Trend in the proportion of peripheral intravenous catheters (PIVCs) with blood reflux in the extension tube across 14 audit cycles.
The effectiveness of this hospital-wide, data-driven audit and feedback model is supported by our prior research. In a previous study utilizing a similar methodology of repeated cross-sectional audits, we successfully guided interventions that led to a dramatic reduction in the use of high-risk winged metal needles (from 13% to 0.5%) and a 70.4% decrease in needle-stick injuries over 4 years. 15 This historical success underpins the rationale that the HIT-QAT, as a more comprehensive and digital tool, is built upon a proven framework for achieving measurable quality improvement in intravenous therapy.
Discussion
Tool innovation
Quality monitoring of infusion therapy is critical for improvement.
The HIT-QAT 15 was developed explicitly to fill this unique niche of hospital-wide, inpatient-focused quality surveillance. Synthesizing evidence from key guidelines—including nursing practice standards for intravenous therapy (WS/T 433-2013, WS/T 433-2023),13,18 Infusion nursing standards of practice (2011 editions), 14 Infusion Therapy Standards of Practice (2016 and 2021 editions)16,17—and incorporating frontline clinical expertise, it digitizes and operationalizes quantitative quality management. Unlike more complex instruments, the HIT-QAT prioritizes clinical utility and feasibility, requiring less than 2 min per bed-audit while encompassing critical safety indicators from device selection to complication documentation.
This comprehensive, inpatient-focused scope provides distinct value for nursing and hospital management. The HIT-QAT enables the systematic tracking of VAD utilization patterns, unit- and hospital-wide nursing practice deficiencies, and complication rates within a single, standardized audit. By generating these actionable, benchmarkable data, it supports targeted resource allocation and drives quality improvement initiatives across the entire inpatient care continuum—a function that specialized, context-specific tools are not designed to perform.
Continuous improvement value
As infusion technology evolves, HIT-QAT dynamically integrates updated guidelines (e.g. INS standards). Iterative refinement transforms a static checklist into a dynamic quality tool. For example, adding visual guides reduced interpretation errors, demonstrating responsiveness to frontline needs (planned future work). Its open-access design promotes shared advancement in infusion quality management.
Operational feasibility
The electronic HIT-QAT enables rapid audits via mobile devices (mean: 68.97 ± 76.93 s per bed). This metric, measured for feasibility rather than as an outcome to minimize, shows broad adaptability—from seconds for screening to minutes for complex cases. Statistical analysis of audit data generates targeted reports, directing quality improvement (QI) interventions for high-risk units, deficiencies, and complications. High completion rates (89.90%) and short audit times confirm operational viability, enabling sustainable hospital-wide monitoring without burdening staff. The electronic mandatory fields ensured 100% data completeness for all core variables (e.g. VAD type, presence of complications) in every submitted audit record. Additionally, the overall survey completion rate (patients successfully audited/total eligible inpatients) was 89.90% across the 14 audits, reflecting the feasibility of conducting hospital-wide audits within the scheduled time. The consistent ability to complete hospital-wide audits within planned windows demonstrates its operational viability for sustainable quality monitoring.
Limitations and future directions
This study has several limitations. Most importantly, while the iterative development with clinical experts establishes strong content and face validity for the HIT-QAT, its psychometric validation remains incomplete. We did not conduct formal testing for inter-rater reliability (i.e. the consistency between different auditors scoring the same patient) or criterion validity (i.e. correlation with a gold-standard assessment or hard clinical outcomes). Consequently, the high data completion rate, though essential for feasibility, primarily reflects the electronic mandatory fields and does not by itself confirm measurement reliability.
Notwithstanding these limitations, the HIT-QAT’s development was rigorously grounded in both international (INS) and Chinese national intravenous therapy standards,13,14,16–18 and its practical utility is preliminarily evidenced by its ability to identify prevalent quality gaps and track improvements over time, as demonstrated in Section ‘Key audit findings, impact, and illustrative case’.
To address these limitations and fully establish the HIT-QAT as a robust measurement instrument, we propose the following validation roadmap:
(1) Inter-Rater Reliability Study: A dedicated study will quantify agreement between independent auditors using statistics such as Cohen’s kappa for categorical items, establishing the tool’s consistency in real-world use.
(2) Multicenter Validation: Applying the HIT-QAT across diverse hospital settings will test its generalizability, assess construct validity, and generate benchmark data.
(3) Detailed analyses of temporal trends, risk factors, intervention effectiveness, and predictive validity (e.g. whether HIT-QAT scores correlate with phlebitis rates) are beyond the scope of this tool‑development paper and will be reported in a separate forthcoming manuscript (Phase II).
Conclusion
The HIT-QAT introduced in this study is grounded in the INS Infusion Therapy Standards of Practice and China’s Nursing Practice Standards for Intravenous Therapy. Through iterative development, refinement, and feasibility validation, this tool demonstrates significant practical value for clinical infusion quality management. This paper reports Phase I: tool design, refinement, and feasibility testing. Future studies (Phase II) will apply the tool to systematically identify practice deficiencies, track outcomes, and evaluate quality improvement interventions.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261459888 – Supplemental material for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility
Supplemental material, sj-docx-1-jva-10.1177_11297298261459888 for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility by Huapeng Lu, Qigui Xiao, Fuhui Sui, Lan Lang, Yali Sun, Nan Hao, Jieqiong Li and Xia Xin in The Journal of Vascular Access
Supplemental Material
sj-docx-2-jva-10.1177_11297298261459888 – Supplemental material for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility
Supplemental material, sj-docx-2-jva-10.1177_11297298261459888 for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility by Huapeng Lu, Qigui Xiao, Fuhui Sui, Lan Lang, Yali Sun, Nan Hao, Jieqiong Li and Xia Xin in The Journal of Vascular Access
Supplemental Material
sj-docx-3-jva-10.1177_11297298261459888 – Supplemental material for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility
Supplemental material, sj-docx-3-jva-10.1177_11297298261459888 for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility by Huapeng Lu, Qigui Xiao, Fuhui Sui, Lan Lang, Yali Sun, Nan Hao, Jieqiong Li and Xia Xin in The Journal of Vascular Access
Supplemental Material
sj-jpg-1-jva-10.1177_11297298261459888 – Supplemental material for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility
Supplemental material, sj-jpg-1-jva-10.1177_11297298261459888 for Developing a practical Hospital Intravenous Therapy Quality Assessment Tool: Design, refinement, and feasibility by Huapeng Lu, Qigui Xiao, Fuhui Sui, Lan Lang, Yali Sun, Nan Hao, Jieqiong Li and Xia Xin in The Journal of Vascular Access
Footnotes
Acknowledgements
The design, refinement, and validation of HIT-QAT evolved over its decade-long development. We extend gratitude to all members of the IV Team at the First Affiliated Hospital of Xi’an Jiaotong University for their dedicated efforts. Special recognition is given to intravenous therapy experts Qinling Yang and Pingli Guo for their leadership of the IV Team and their exceptional contributions spanning over 40 years in nursing care and infusion therapy.
Author contributions
HL contributed to the design, acquisition, analysis, interpretation of data, as well as the drafting of the manuscript. SF, LL, and SY contributed to the design, acquisition, analysis, interpretation of data, and critical revision of the manuscript. HN, LJ, and XX contributed to the interpretation of data and critical revision of the manuscript. LH and XQ had full access to all the study and took responsibility for the integrity and accuracy of the data analysis.
Data availability statement
All data generated or analyzed during this study are included in this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Fundamental Research Funds of the First Affiliated Hospital of Xi’an Jiao Tong University (2021HL-17) for funding this study.
Ethical approval
This study was approved by the institutional review board of the First Affiliated Hospital of Xi’an Jiaotong University (NO.XJTU1AF2021LSK-385).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.