
Abstract
An arteriovenous fistula (AVF) is the preferred permanent vascular access for long-term hemodialysis (HD) in patients with chronic kidney disease (CKD). Once adequately matured, an AVF provides usability over a long period of time. However, in rare cases, patients may develop fistula dysfunction accompanied by forearm swelling and/or signs of tissue injury with ischemic features in the setting of venous hypertension. This report presents three cases of patients with wrist AVFs who developed forearm venous hypertension and hand ulcers secondary to venous occlusion in the proximal forearm, an uncommon etiology of hand ischemia. These cases highlight the importance of a comprehensive clinical evaluation and timely intervention to alleviate symptoms while preserving vascular access integrity.
Keywords
Introduction
Venous hypertension in patients with arteriovenous access can be secondary to central venous pathology, 1 or due to peripheral forearm venous outflow obstruction. While generalized arm swelling is typical in central occlusion, edema is typically confined to the hand and forearm in cases of peripheral venous outflow obstruction. These obstructions may arise due to stenoses in the veins around the elbow, leading to venous hypertension distal to the obstruction. 2
In addition to swelling and access dysfunction, venous hypertension resulting from arteriovenous (AV) access can lead to significant tissue injury, including pain, edema, and, in severe cases, ulceration and necrosis.3,4 A related clinical entity with similar features, dialysis access-induced ischemia syndrome (DAIIS), is a well-recognized complication of vascular access and is classically attributed to reduced distal arterial perfusion, most commonly due to steal physiology or impaired inflow.
Elevated venous pressure may impair capillary perfusion and oxygen delivery, resulting in ischemia-like tissue injury despite preserved arterial inflow. This supports a potential overlap between venous hypertension and access-related ischemia, presented here as a pathophysiological hypothesis.
In this paper, we present three cases of localized swelling in the forearm and hand associated with venous outflow stenosis, leading to venous hypertension and subsequent tissue injury. We emphasize venous hypertension as the dominant mechanism while exploring its potential relationship with ischemia-like injury. We also describe the salvage techniques employed to treat this limb-threatening condition while preserving the integrity of the fistula.
Case 1
A 25-year-old male, with CKD secondary to hypertension presented with the complaint of left arm swelling of 3 months duration. The patient had a left radio-cephalic fistula created 3 years prior. On examination, there was marked swelling of the left forearm and hand along with blackish discoloration and non-healing ulcers on the second, third, and fourth fingers. The radial and ulnar pulses were palpable; sensory and motor functions were intact. There were multiple dilated veins in the forearm and hand including a prominent side branch of the cephalic vein. The fistula was pulsatile on palpation. Ultrasonography showed an ~8 cm occluded segment of the cephalic vein in the mid-forearm and poor collateral outflow to the upper arm. Above the occlusion, there was a dilated cephalic vein with good continuity proximally up the arm. The mentioned prominent dorsal branch of the cephalic vein present distal to the occlusion had fistulous flow. Duplex assessment of the radial and ulnar arteries confirmed normal arterial inflow.
Given the presence of venous hypertension in the hand due to the side branch, the operative plan was to establish a new outflow pathway to the upper arm, aiming to salvage both the fistula and the hand. This was achieved by utilizing the mentioned prominent vein of the forearm as a bypass for the occluded segment (Figure 1), thereby stopping the fistulous backflow into the hand. Intraoperative assessment confirmed that the dorsal venous branch could be mobilized to the proximal vein without tension, allowing construction of a functional venous bypass by swinging it up and anastomosing it to the proximal cephalic vein.
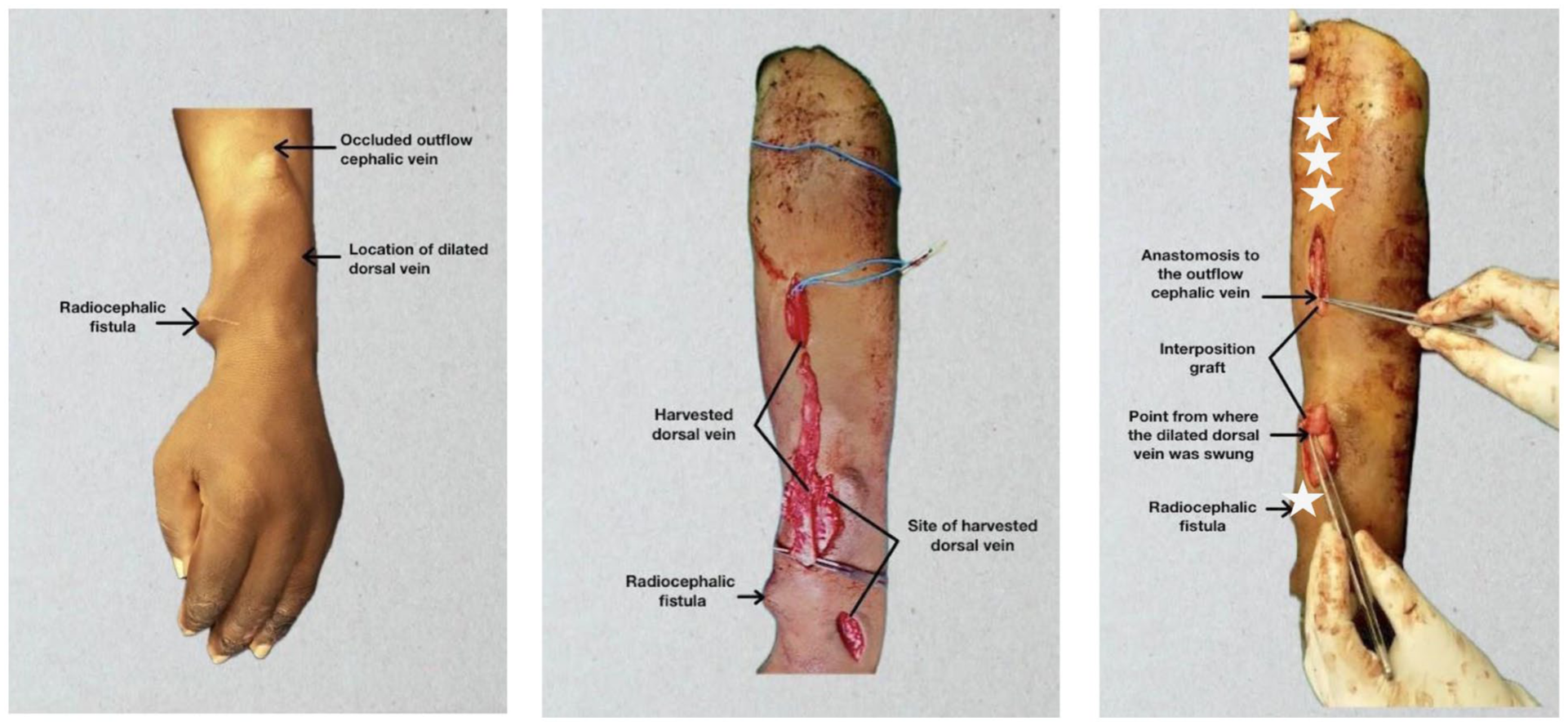
Preoperative and intraoperative pictures. The postoperative cannulation site is marked (*)
On follow-up, there was an excellent thrill and bruit in the fistula with a marked reduction of the swelling. The access was functioning well; because of the preoperatively matured areas (distally close to the radiocephalic anastomosis and along the proximal lower arm, marked “*” in Figure 1) cannulation was possible so that no central catheter as a bridging tool was necessary. After 4 weeks the fistula could be punctured along the whole lower arm. Due to the reduced venous pressure the ulceration in the fingers resolved.
Case 2
A 21-year-old female with CKD secondary to hypertension presented with a 2-month history of swelling in the left forearm and hand. In addition, she had significant ulceration on the dorsum of the hand (Figure 2). The patient had a left radio-cephalic fistula created 3 years prior. The pulses were palpable, and sensation intact. The fistula was pulsatile. Both of these findings were consistent with venous outflow obstruction. Ultrasonography revealed a 10 cm occluded segment of the cephalic vein in the proximal forearm and a dilated venous branch coming off the cephalic vein coursing towards the dorsum of the hand. This explained the swelling and the dysfunction of the hand. The upper arm basilic vein had good continuity proximally. Duplex assessment of the radial and ulnar arteries confirmed normal arterial inflow.
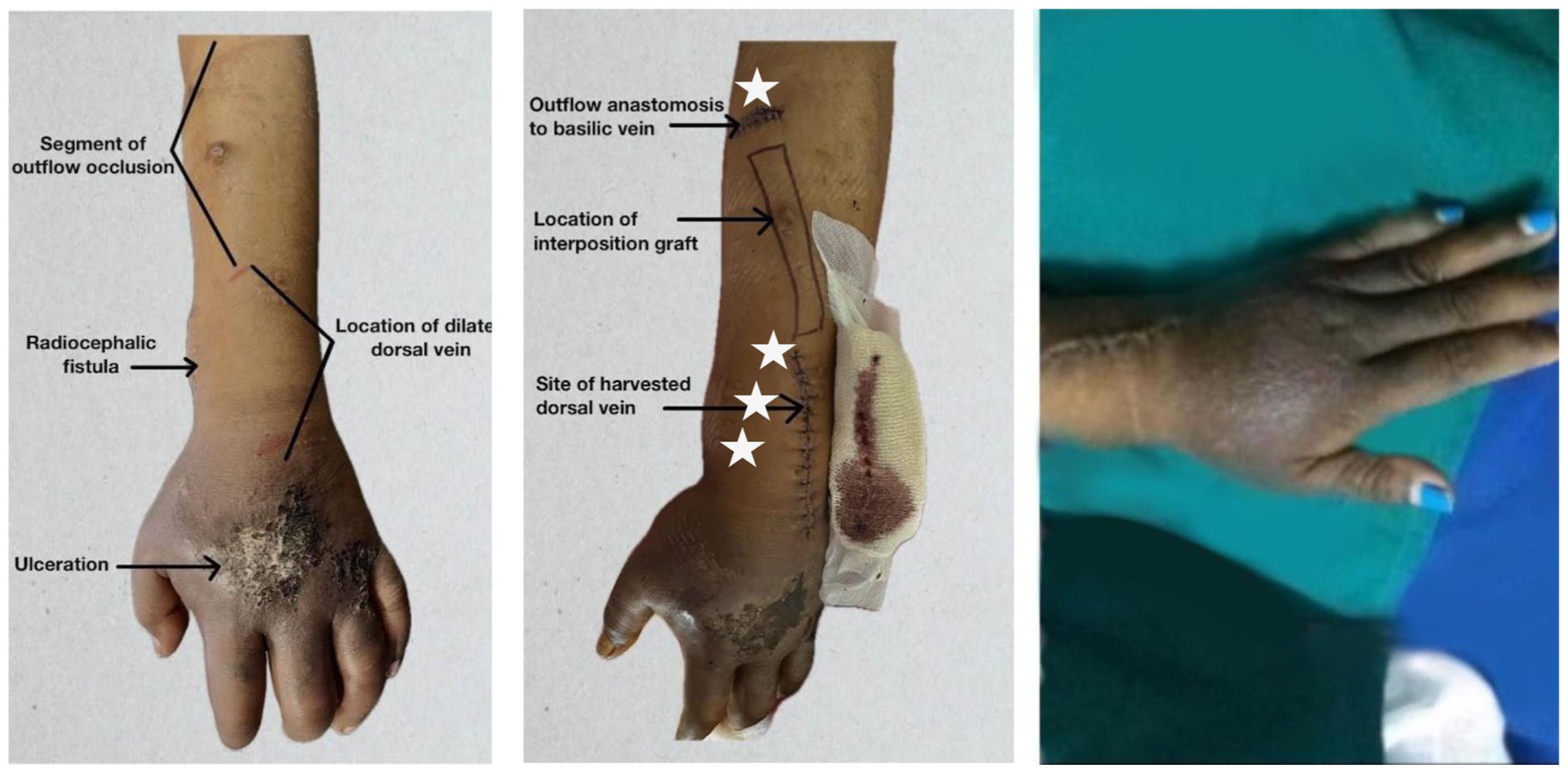
Preoperative, 24 h postoperative, and 2 weeks postoperative pictures. The postoperative cannulation site is marked (*)
Intraoperative assessment confirmed that the dorsal venous branch could be mobilized to the proximal vein, allowing construction of a functional venous bypass. However, different from Case 1, the vein had to be translocated instead of just swinging it up, as the long segment-stenosis was located more proximally in the forearm and therefore needed bypassing. Similar to Case 1, the reconstruction provided a new outflow for the fistula, thereby reducing the venous flow into the hand.
Following the operation, there was a noticeable reduction in hand swelling, and the ulcers healed within 2 weeks. Similar to Case 1, the already matured areas (at the distal and proximal aspect of the lower arm, marked “*” in Figure 2) allowed for sufficient cannulation, thereby avoiding a central catheter as bridging tool. On 1-month follow-up, the fistula was useable along the whole distance of the lower arm.
Case 3
A 52-year-old female with a 6-year history of chronic kidney disease had a left radiocephalic arteriovenous (AV) fistula created in the hand 1.5 years ago, which was being used for hemodialysis, but the flow during dialysis in the last 6 months had been decreasing over time. She also mentioned a 5-month history of progressive swelling of the left forearm and hand, associated with pain, blackish discoloration, and ulceration over the dorsum of the fingers (Figure 3).

Preoperative and 2 weeks postoperative pictures.
On presentation, examination revealed marked edema of the left forearm and hand with dorsal finger ulceration. Radial and ulnar pulses were palpable, and motor and sensory functions were intact. The radiocephalic fistula was pulsatile.
Duplex assessment of the radial and ulnar arteries confirmed normal arterial inflow. There was a 4 cm stenotic segment of the cephalic vein in the proximal forearm. The antecubital cephalic vein, along with the had matured, and the cephalic vein proximal to the stenosis was dilated and continuous. Multiple venous collaterals were observed coursing toward the dorsum of the hand, originating from the fistula vein distal to the stenosis. However, unlike the previous cases, there was no single dominant vein suitable for bypass or “swinging” to salvage the radiocephalic fistula. To address symptomatic venous hypertension and DAIIS, the radiocephalic fistula had to be ligated. A new brachiocephalic AV fistula was created at the elbow, taking advantage of the already matured cephalic vein which made immediate cannulation possible. Two weeks after ligation, there was a marked reduction in swelling of the hand and forearm (Figure 3). The patient continued successful hemodialysis through the newly created left brachiocephalic fistula.
Discussion
Upper extremity swelling in patients with vascular access is commonly caused by central venous occlusion, particularly in the subclavian, innominate veins, and superior vena cava. 1 It is often related to previously inserted central venous catheters for dialysis. 1 Typical presentations include swelling of the entire upper extremity and, in some cases, the face. Clinical examination, duplex ultrasound, and, if necessary, angiography allow for an unambiguous diagnosis.
In our patients, swelling and pain were localized to the hands and forearms, accompanied by areas of skin necrosis. Clinical investigation and duplex ultrasound ruled out central stenosis. We interpreted this distinct pattern as a manifestation of a distal venous outflow obstruction with resultant venous hypertension as the mechanism of tissue injury in these cases. However, as the development of hand necrosis after creation of a dialysis access raises the question of an underlying dialysis access induced ischemia-syndrome (DAIIS), this needs further discussion. As currently defined, DAIIS occurs due to arterial hypoperfusion, that is, when vascular access diverts arterial blood away from the distal extremity or impaired arterial flow due to sclerosis,5,6 leading to reduced perfusion and ischemia. Our patients had similar clinical findings as described in DAIIS stage IV, 6 although the underlying mechanism was obviously driven by venous hypertension due to outflow obstruction, rather than arterial blood diversion or arterial obstruction due to sclerosis. 5 The elevated venous pressure disrupts normal hemodynamics, impairing tissue perfusion and causing ischemic symptoms in the affected limb. 5 As a result, patients may experience pain and swelling, which, if untreated, can progress to ulceration or even gangrene7–9—complications observed in our case as well. At the microcirculatory level, elevated venous pressure may reduce capillary perfusion gradients and impair oxygen delivery, potentially resulting in ischemia-like tissue damage despite preserved arterial inflow. This may provide a mechanistic explanation for the overlap in clinical presentation between venous hypertension-related tissue injury and DAIIS. We present this as a pathophysiological hypothesis rather than a redefinition of existing classifications. However, our previously proposed classification of DAIIS (at that time incorrectly termed dialysis shunt-associated steal syndrome, DASS) supported the multifactorial nature of ischemia. 6 As DAIIS should be understood as a complex clinical entity, and while arterial insufficiency remains the predominant mechanism, our findings suggest that venous hypertension may contribute to similar patterns of tissue injury through microcirculatory compromise and therefore might be considered to share features with DAIIS. In any way, recognizing this potential overlap is important, as it influences both diagnostic evaluation and management strategies.
A comprehensive evaluation is crucial to accurately diagnose the location and cause of venous occlusion. This typically includes a thorough physical examination, ultrasonography,10,11 and when necessary, imaging studies such as a fistulogram. 12 In our cases, ultrasonography revealed occlusion of the cephalic veins with poor collateral outflow from the forearm. Duplex assessment of the radial and ulnar arteries in all patients confirmed normal arterial inflow, supporting the conclusion that venous hypertension, rather than arterial insufficiency, was the primary driver of tissue injury. Since the diagnosis was established based on physical examination and ultrasound findings, we did not pursue further imaging with a fistulogram.
For the salvage of a fistula, both surgical and endovascular interventions are available, with comparable efficacy. 13 Balloon angioplasty is a common method to treat outflow occlusion in dialysis access; however, it may not always be effective, particularly in cases where the stenosed segment is too long for balloon dilation 14 or when stenosis recurs. 15 In such instances, surgical interventions would offer superior long-term outcomes. In our cases, the outflow stenosis was extensive, measuring 4–10 cm, which rendered balloon angioplasty unfeasible. 14
Given these factors, we chose surgical intervention to address both the outflow stenosis and the venous hypertension. The dilated distal vein was utilized as a venous interposition graft, thereby creating a new outflow route. This approach effectively relieved the venous hypertension and salvaged the fistula, restoring normal blood flow. Functional adequacy of the access was confirmed postoperatively, with all patients achieving dialysis blood flow rates exceeding 400 mL/min, supporting continued effective hemodialysis which in all cases made immediate cannulation of matured fistula-segments possible. It has to be noted, though, that in similar cases central catheters might be implanted as bridging-tool. The surgical approach to address these complicated cases is anatomy-dependent. Swinging of the dorsal vein may not be feasible in patients without a sufficiently developed dorsal venous branch or with inadequate proximal venous outflow. Accordingly, in one patient the fistula had to be ligated, necessitating the creation of a new one.
Conclusions
Proximal forearm venous occlusion is a rare but significant cause of venous hypertension-related tissue injury in patients with arteriovenous access, potentially leading to severe complications such as ulceration and necrosis. Although these manifestations may overlap clinically with dialysis access-induced ischemia syndrome (DAIIS), our findings support venous hypertension as the dominant underlying mechanism. In the management of outflow stenosis in dialysis fistulas, using a dilated distal vein as a venous interposition graft provides a dual benefit: it alleviates stenosis, thereby preserving fistula function, while also addressing venous hypertension. This approach not only restores access function but also reverses the underlying hemodynamic disturbance responsible for tissue injury. Further studies are required to determine whether this entity should be incorporated into the current conceptual framework of DAIIS.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Consent was taken from all cases for publication. Signed consent forms can be produced by the authors if required by the journal.