
Abstract
Background:
The most common causes of early primary failures of a vascular access (VA) is related to small caliber vessels. Weight gain between dialyses expands both extracellular and blood volume, which may lead to rises in intravascular filling and vessels caliber. If patients presented after weekend, their weight and probably volemia would be higher. We hypothesized that preoperative volume status may influence vascular filling and vessels diameter with a significant impact on VA outcomes.
Methods:
A clinical, prospective, randomized, open-label, single-center within-patient physiological crossover evaluation trial. Inclusion criteria: age 18–80 years, under regular hemodialysis (three per week) Exclusion criteria: >3 sessions/week, heart failure (HF), and acute pulmonary edema on the previous year. Before the last-week session, patient’s clinical parameters were recorded. BIA and ultrasound vascular mapping were performed. After this first evaluation, dry weight was increased 0.5 kg, and after weekend, the same protocol was conducted. Primary end point was to compare vein diameters.
Results:
One hundred twenty-six vessels were evaluated (84 veins and 42 arteries) from 21 patients. Mean age was 69 ± 10 years and 52% female. Other than humeral arterial blood flow, every parameters evaluated through ultrasound mapping significantly increased (p < 0.05), however, most patients had a mild-moderate OH (86%–90%). Patient-level paired analysis confirmed a significant increase in mean venous diameter after volume expansion (p = 0.002). No complications were reported.
Conclusions:
Preoperative volume status appears to be an underrecognized and potentially modifiable determinant of vascular access conditions. Mild preoperative volume expansion was associated with increased venous diameter, a surrogate for AVF feasibility and maturation. BIA and lung ultrasound may be future tools that combined to vascular ultrasound could be a safe and effective way to optimize and evaluate preoperative conditions to improve VA outcomes. Future multicenter prospective studies should assess whether preoperative volume optimization translates into improved AVF creation, maturation, and long-term patency outcomes.
Introduction
A functional vascular access is essential for effective hemodialysis and remains a major determinant of morbidity and survival in end-stage kidney disease.
Despite advances in surgical technique and preoperative mapping, early failure of arteriovenous fistulas (AVFs) remains common and is strongly associated with small vessel caliber. 1 Nevertheless, other factors like vasospasm, hypotension, and peripheral vasoconstriction may contribute to early thrombosis.
It is well known in microvascular surgery that hypervolemic hemodilution improves blood flow and peripheral tissue oxygenation, as well as decreases total blood viscosity. The role of volume status in the creation of vascular access has received little attention.
We hypothesized that preoperative volume status influences vascular dimensions and may represent a modifiable factor to improve vascular access outcomes.
Methods
Protocol
The study was designed as a prospective within-patient physiological crossover evaluation in which each patient underwent vascular assessment under two different volemic conditions.
Participants
Inclusion criteria:
Age 18–80 years
Maintenance hemodialysis (three sessions per week)
No history of congestive heart failure
No acute pulmonary edema in the previous year
Exclusion criteria:
More than three dialysis sessions per week
Congestive heart failure
Recent pulmonary edema
Before the last-week session, patient’s clinical parameters like age, weight, residual diuresis, and BP were recorded. Then, bioimpedance spectroscopy, and ultrasound vascular mapping were performed to each patient.
Bioimpedance spectroscopy was performed with the body composition monitor (BCM), Fresenius Medical Care according to specific instructions.
Ultrasound vascular mapping was systematically performed on the arm without a functioning vascular access. Patients with prior major vascular injury, previous vascular access creation, or central venous stenosis affecting the evaluated limb were not included. Ultrasound mapping was performed under standardized conditions, including the same warm-room environment, patient positioning, tourniquet application, and anatomical reference points. Measurements were obtained at exactly the same predefined locations, which were marked and photographically documented. All examinations were performed by the same experienced operator, minimizing interobserver variability. Echographic study was performed by a Siemens Acuson X150 Ultrasound device. Diameters were recorded with cross section B-mode for radial and humeral arteries, as well as for distal radiocephalic, medium third radiocephalic, cephalic, and basilic veins. Blood flow of the humeral artery was also calculated through the formula Qa (ml/min) = TAV (cm/s) x D (cm) x 60 (7). Exact measuring locations were marked and a photo was taken to re-evaluate at exactly the same spots.
After this first evaluation, patient’s dry weight was increased 0.5 kg by adjusting ultrafiltration on that session before weekend. The 0.5 kg dry weight increase was selected as a conservative and clinically safe intervention intended to induce mild extracellular volume expansion while minimizing the risk of symptomatic fluid overload. A standardized increment was applied to all patients in order to reduce protocol variability and maintain consistency between evaluations.
Before the next session, after weekend, the patient was again submitted to the same protocol, including clinical evaluation, bioimpedance spectroscopy, as well as, ultrasound mapping (Figure 1).
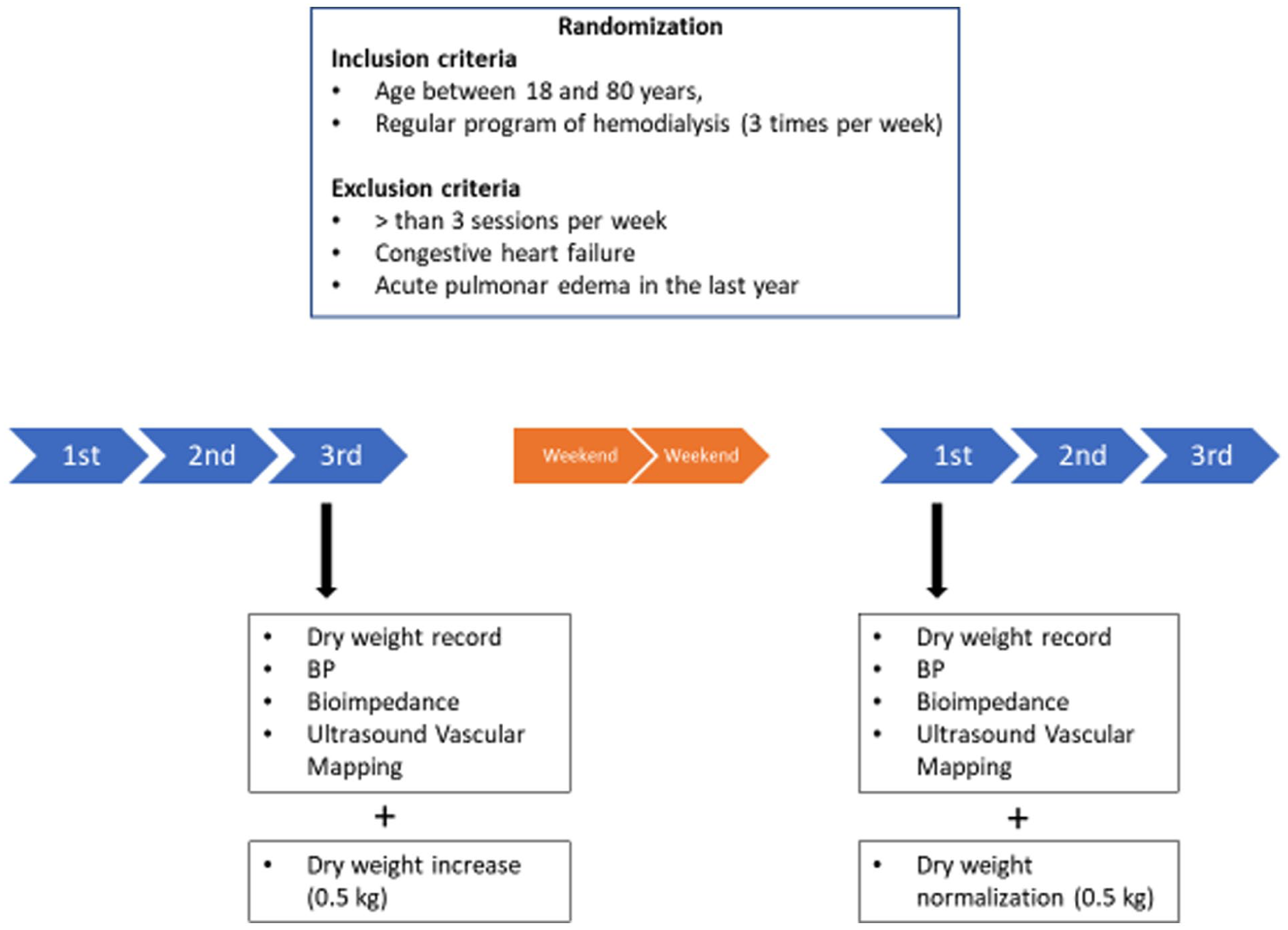
Protocol.
The primary endpoint was to compare vein diameters. In addition to vessel-level analyses, patient-level paired analyses were performed by calculating the mean venous diameter for each patient before and after volume expansion in order to account for intra-patient clustering of vascular measurements.
Secondary endpoints were to compare arteries diameters and humeral blood flow (BF), systolic blood pressure (SBP), diastolic blood pressure (DBP), and bioimpedance parameters linked to fluid status like OH, extracellular water (ECW), intracellular water (ICW), and total body water (TBW).
The trial was submitted to approval by the local ethics committee and was be performed according to the principles of the Declaration of Helsinki. Written informed consent was obtained for all patients before participation.
Results
One hundred twenty-six vessels were evaluated (84 veins and 42 arteries) from 21 patients that were randomized. Mean age was 69 ± 10 years and 52% were female.
The primary end point was achieved. All evaluated venous diameters significantly increased after volume expansion (p < 0.05), including: distal radiocephalic vein, median cubital vein, cephalic vein, and basilic vein (Table 1 and Figure 2).
Vessels diameters before and after volume adjustment.
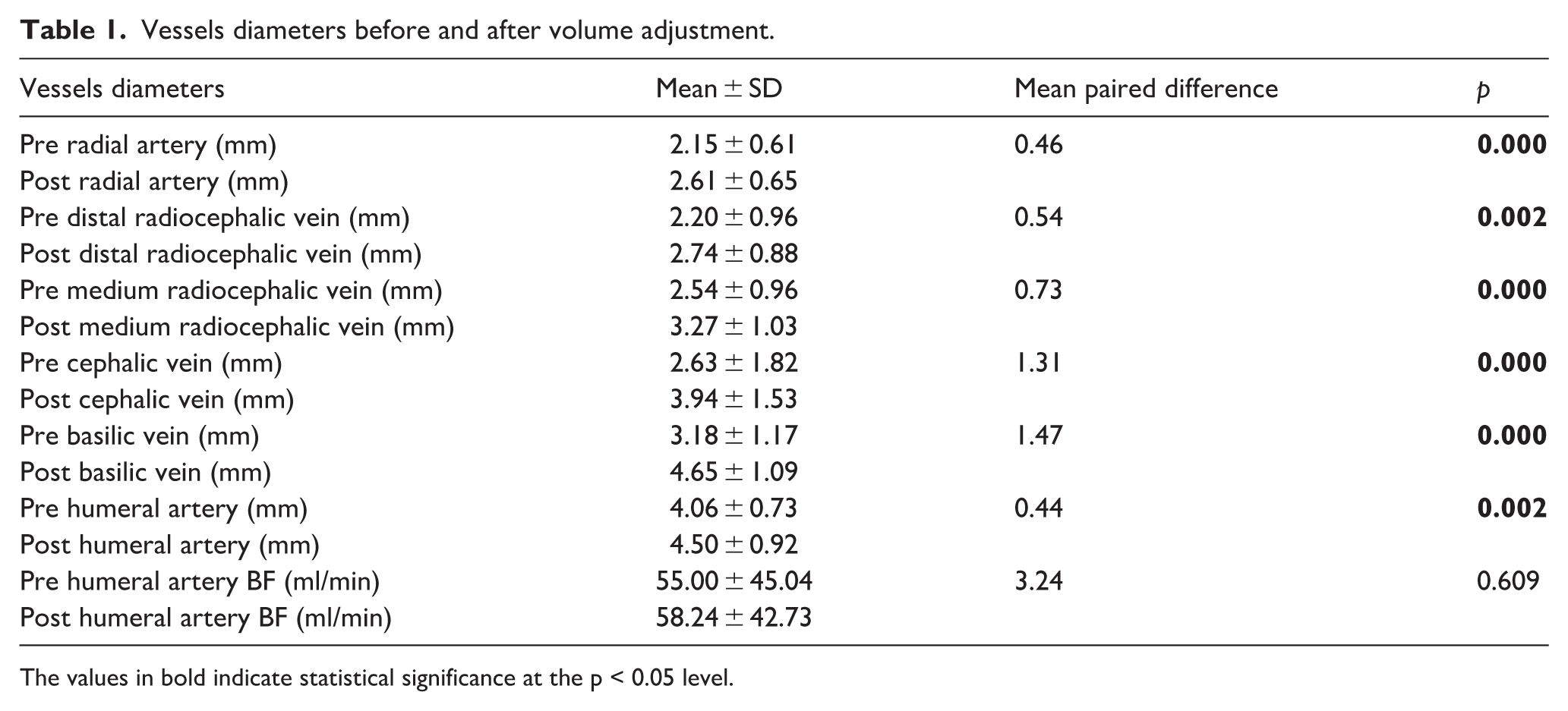
The values in bold indicate statistical significance at the p < 0.05 level.
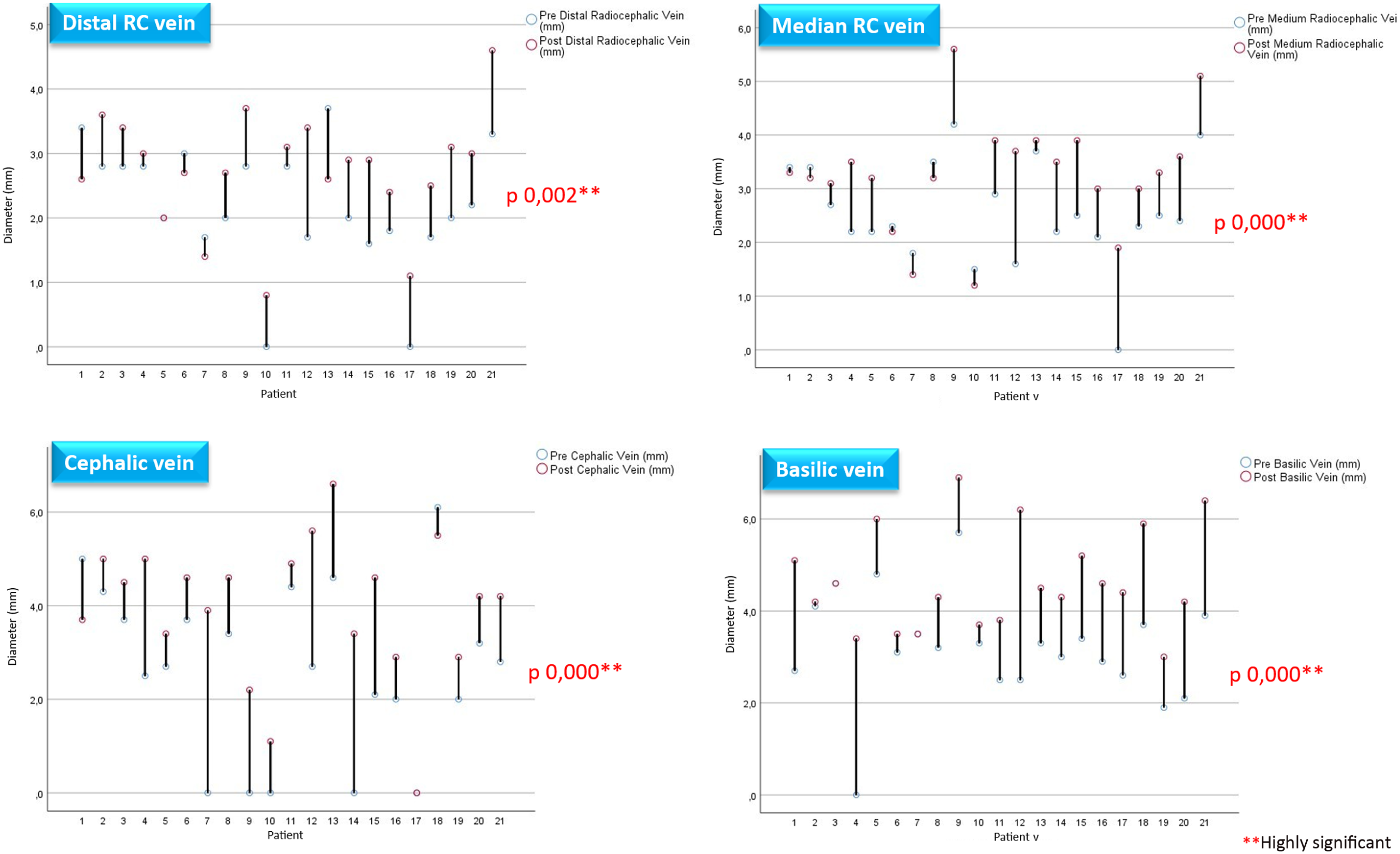
Veins diameters before and after volume adjustment.
Patient-level paired analysis confirmed a significant increase in mean venous diameter after volume expansion (p = 0.002).
Other than humeral arterial blood flow, every parameters evaluated through ultrasound mapping significantly increased (p < 0.05) after dry weight adjustment (increase of 0.5 kg) plus the inter-dialytic weight gained after weekend (Table 1).
Most of the results showed a highly statistical significance (p < 0.001; Table 1 and Figure 2).
The weight gained after ultrafiltration adjustment (dry weight increase of 0.5 kg) and weekend was highly significant (p < 0.001). In this setting, overhydration (OH), extracellular water (ECW), and their ratio OH/ECW significantly increased (p < 0.05; Table 2).
Volume assessment measurements.
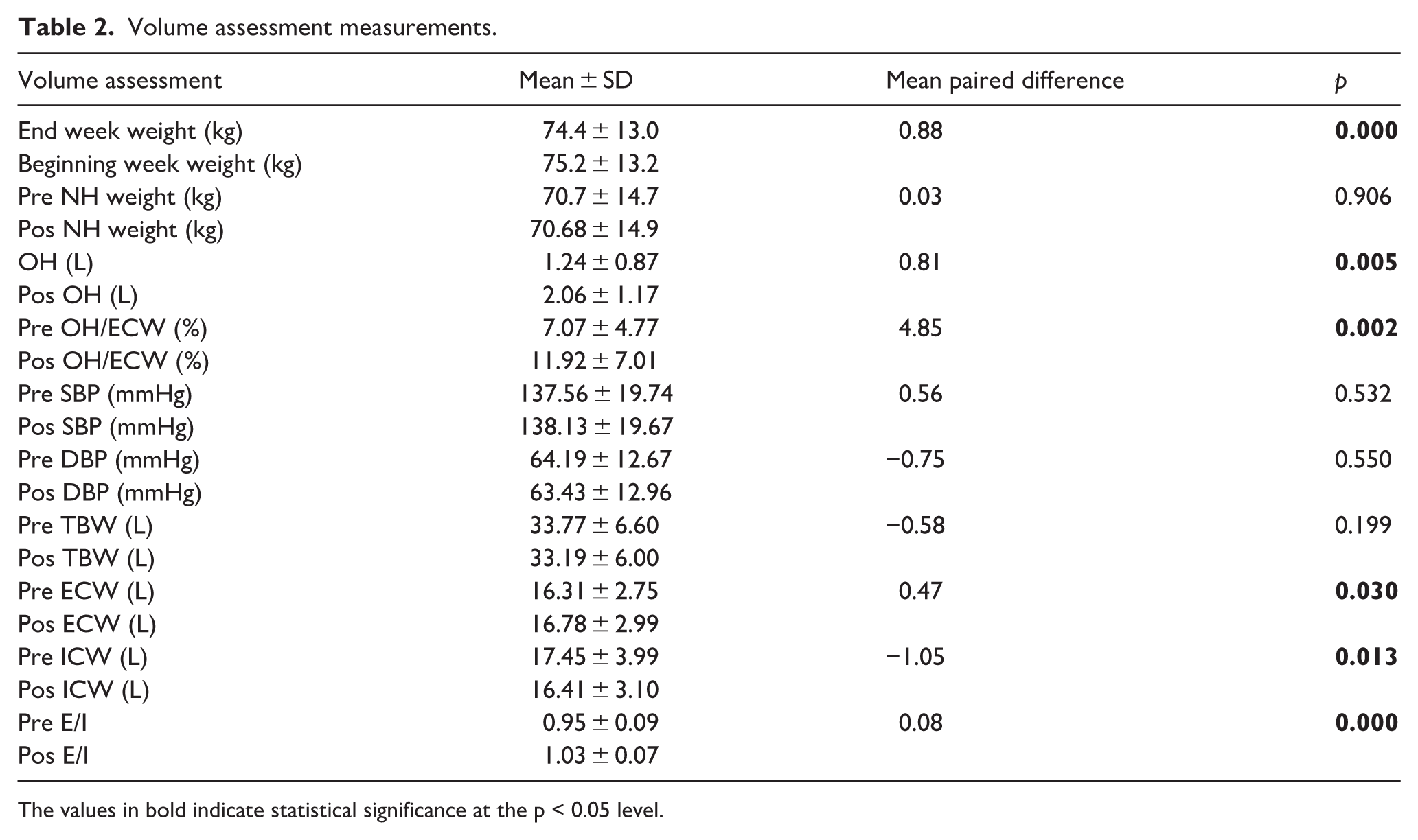
The values in bold indicate statistical significance at the p < 0.05 level.
Surprisingly, both systolic and diastolic blood pressure haven’t changed significantly. Moreover, total body water (TBW) remained similar, probably due to the significant decrease in the intracellular water (ICW; Table 2).
Most patients remained within mild-to-moderate overhydration (86%–90%).
No cardiovascular or other complications reported.
Discussion
Vascular access dysfunction remains a leading cause of morbidity in hemodialysis patients, and early failure is multifactorial.2,3
Recent studies have reinforced the importance of patient-specific and modifiable factors, including vascular biology and hemodynamic conditions.4,5
Although the most common causes of failure are related to small vessel diameter, other factors related to hemodynamics and perioperative fluid therapy, such as hypotension, peripheral vasoconstriction, vasospasm, and edema can contribute significantly to failure. 6
It is well known in microvascular surgery that hypervolemic hemodilution improves blood flow and peripheral tissue oxygenation, as well as decreases total blood viscosity. 6
Oxygen transport can be augmented by increasing circulating blood volume and maintaining low peripheral vascular resistance. 6
Volume status is a central component of hemodialysis care. 7 However, its role in the creation of vascular access has received little attention.
Since intravascular water is in equilibrium with the interstitial compartment, any change in extracellular fluid volume will affect both compartments.7,8 Therefore, interdialytic weight gain leads to expansion of intravascular and extracellular compartments, potentially increasing vascular filling and diameter.7,8
Fluid therapy is limited in dialysis patients, but interdialytic fluid intake expands extracellular and blood volume, which may increase vessel caliber. 8
This study suggests that mild preoperative volume expansion significantly increases venous diameter, one of the strongest and most consistently recognized predictors of AVF feasibility and maturation. The observed increase in venous diameter despite stable blood pressure and humeral arterial blood flow may be explained by the high compliance and capacitance properties of the venous system, in which mild extracellular volume expansion can enhance venous filling and vascular distensibility without necessarily producing major systemic hemodynamic changes. Furthermore, the increase in extracellular water associated with a relative reduction in intracellular water may reflect redistribution between fluid compartments, potentially contributing to increased vascular filling and reduced peripheral vasoconstriction.
Although the present study did not directly evaluate vascular access creation, maturation, or long-term patency outcomes, the observed physiological changes may have relevant clinical implications, given the well-established association between vessel caliber and vascular access success. Nevertheless, these findings should be interpreted cautiously, and prospective outcome-based studies are required to confirm whether optimization of preoperative volume status translates into improved vascular access outcomes. 9
Volume assessment remains particularly challenging in dialysis patients, and emerging evidence supports multimodal approaches combining bioimpedance and ultrasound to improve evaluation of fluid status. Moreover, bioimpedance-guided management has been associated with improved clinical outcomes, including reduced mortality.10–14
In this context, our results suggest that bioimpedance may also have a potential role in perioperative optimization of volume status before vascular access creation. The observed increase in venous diameter under mild volume expansion raises the possibility that strict achievement of “dry weight” immediately before vascular mapping may not always represent the optimal physiological condition for vascular assessment in selected patients. Given that vascular diameter is one of the strongest predictors of AVF feasibility and maturation, temporary controlled mild hypervolemia may potentially improve vascular mapping conditions and increase eligibility for native AVF creation. However, these findings should be interpreted cautiously, as direct vascular access outcomes were not evaluated in the present study.
Importantly, this strategy appeared safe in our cohort, with no significant hemodynamic instability or cardiovascular complications observed. Future studies may further explore individualized approaches to preoperative volume optimization by integrating multimodal assessment tools, including body composition analysis, baseline hydration status, cardiovascular tolerance, and patient comorbidities, in order to better tailor volemic expansion strategies to individual physiological profiles.
The present study should be interpreted within the context of its exploratory physiological design, relatively small sample size, and single-center setting. Furthermore, although vascular diameter is a well-established predictor of AVF feasibility and maturation, direct vascular access outcomes were not assessed and therefore the clinical implications of these findings require confirmation in prospective outcome-based studies. Furthermore, the absence of more detailed vascular characterization, including assessment of arterial stiffness, vascular calcification, and vessel wall properties, limits mechanistic interpretation of the observed findings and should be addressed in future studies.
Conclusion
Preoperative volume status appears to be an underrecognized and potentially modifiable determinant of vascular access conditions. Mild preoperative volume expansion was associated with increased venous diameter, an established predictor of AVF feasibility and maturation. However, because this study did not evaluate vascular access outcomes directly, the clinical implications of these findings remain speculative. Future multicenter prospective studies should assess whether preoperative volume optimization translates into improved AVF creation, maturation, and long-term patency outcomes.
Footnotes
Acknowledgements
No.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.