
Abstract
Central venous occlusion (CVO) is a common complication in hemodialysis patients. The Surfacer Inside-Out Access Catheter System is designed to gain access through previously occluded right-sided central veins. We report a case of a 74-year-old heart transplant recipient with end stage kidney disease and multiple failed dialysis accesses who developed bilateral upper CVO and femoral catheter dependence and underwent right internal jugular re-canalization with Surfacer Inside-Out technology. To our knowledge, this is the first successful tunneled dialysis catheter (TDC) insertion using Surfacer technology in a heart transplant recipient. These patients are at risk of anastomotic stenoses as a complication after cardiac transplantation. This, coupled with the fact that long-term steroid use has been associated with vascular fragility, leads to increased risk of vascular complications in endovascular interventions. But in patients with exhausted vascular access from CVO, insertion of TDC with Surfacer technique is safe and feasible.
Keywords
Introduction
Dialysis remains a vital lifeline for patients with end-stage kidney disease (ESKD) and establishing a working dialysis access is necessary for effective treatment. In patients undergoing hemodialysis (HD), longevity on dialysis is directly related to the quality of dialysis, which in turn depends on the reliability and integrity of the dialysis access. 1 Choosing the correct type of access should be individualized, considering patient-specific factors such as vascular anatomy, comorbidities, and patient preferences. Arteriovenous fistula (AVF) remains the preferred access over arteriovenous graft (AVG) because of their lower infection rate, fewer thrombosis events, and superior long-term patency. While the USRDS reports that 85% of dialysis patients utilize central venous catheters (CVC) upon HD initiation, this modality is least preferred due to its myriads of complications. These include thrombosis, infections, and central venous occlusion (CVO), ultimately leading to significant morbidity and mortality in HD patients. 2
Central venous stenosis (CVS) occurs frequently among HD patients, and this has been strongly associated with long-term CVC placement. Multiple mechanisms have been proposed for the development of CVS, including CVC-induced trauma to the venous endothelium causing secondary inflammatory damage. As a foreign body with turbulent blood flow, CVC incites an inflammatory response and stimulates intimal hyperplasia. 3 Chronic CVS can then cause thrombosis and fibrosis, resulting in occlusion of the central vein at the site of the stenosis. As a result, CVO can cause AVF dysfunction and preclude future vascular access in the upper extremities, depending on the location of the occlusion, due to lack of outflow. 4 Endovascular intervention remains the mainstay of treatment in HD patients with CVO. Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines recommend an attempt at CVO recanalization with angioplasty or stenting.1,3 Other standard solutions for obstructing thoracic central veins include establishing femoral access or placing an upper extremity Hemodialysis Reliable Outflow (HeRO) graft. A newer alternative method for gaining central venous access in patients with CVO is the Surfacer Inside-Out Access Catheter System. 5 The device permits placement of CVC for patients with CVO by recanalization of the occluded right sided central veins using a delivery system that is introduced through the right femoral vein all the way to the level of occlusion via inferior vena cava (IVC), right atrium, and the superior vena cava (SVC). After traversing the occlusion, it directs a needle wire from the occluded right internal jugular (RIJ) vein to come out through the skin in the supraclavicular fossa in an inside-out fashion. 3
We discuss a case of a heart transplant recipient complicated by ESKD with multiple failed dialysis access attempts who eventually developed bilateral upper CVO. The patient underwent RIJ tunneled dialysis catheter (TDC) placement after right central veins re-canalization with the Surfacer Inside Out technology.
Case description
A 75-year-old male with a past medical history of chronic kidney disease (CKD), peripheral vascular disease, and ischemic cardiomyopathy underwent an orthotopic heart transplant (OHT). His post-transplant clinical course was complicated by an acute kidney injury in the setting of CKD that required dialysis initiation. Due to the urgent need for dialysis, he underwent a RIJ TDC insertion. His kidney function never recovered, and he continued to require dialysis. Six months after his transplant, he underwent right forearm loop AVG creation. Unfortunately, in 2 months, his AVG thrombosed, to which he underwent thrombectomy, but continued to have recurrent thrombosis leading to AVG failure. Subsequently, a new RIJ TDC was inserted. About a year after being on HD, the patient was transitioned to peritoneal dialysis (PD). He continued to do PD for a year and then developed PD catheter-associated infection that required PD catheter removal. He was then transitioned back to HD for the next 1.5 years. During this time, he had multiple catheters placed and removed both on the right and left internal jugular veins. He also had failed AVGs on both upper extremities. He ultimately developed thrombosis of both the right and left internal jugular veins. Hence, a right femoral TDC was placed. At this point, the possibility of right internal jugular vein re-canalization using Surfacer Inside-Out System and subsequent RIJ TDC placement was discussed with the patient. The patient preferred to get rid of the catheter in the groin and consented to proceed with an evaluation for suitability for the Surfacer procedure. With history of OHT, we considered factors like IVC and SVC anastomoses, orientation of the transplanted heart and its angle with the IVC and SVC, and the effect of long-term steroids on the health of endocardium and vessel endothelium. As part of the work up, patient underwent a neck, chest, abdomen, and pelvis computed tomography (CT) angiogram to evaluate the level of occlusion in the right central venous system, the degree of curvature and tortuosity of the inferior and superior vena cava, and presence of any stenosis at the anastomoses. This showed occlusive stenosis of the distal RIJ with extension to the brachiocephalic confluence on the right and an occluded left brachiocephalic vein. There was a stenosis noted in the superior vena cava anastomosis with the transplanted heart (Figure 1). With this evidence of CVO and the patient being at high risk of infection with chronic immunosuppression, it was important to minimize this risk by establishing access on the chest and avoiding the groin area. At this time, the patient was deemed a candidate for the Surfacer Inside Out Access Catheter System. A written consent was obtained from the patient before the start of the procedure.
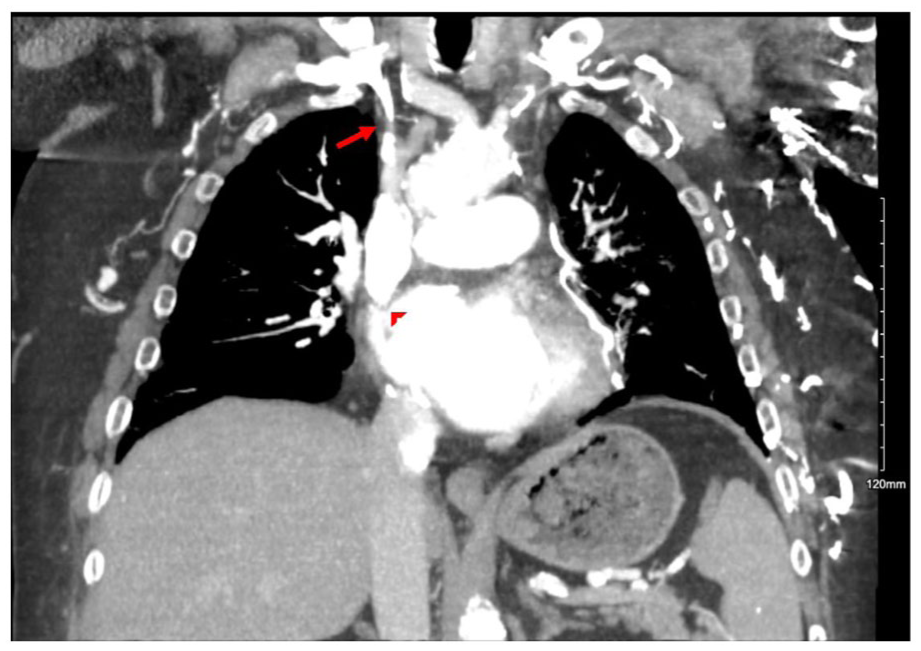
Chest CT angiogram revealing occlusion of the right brachiocephalic vein causing type 3 occlusion (red arrow) and stenosis at the superior vena cava—right atrium junction (arrowhead).
Under general anesthesia, the patient was prepped and draped in the usual sterile fashion, overlying the right side of the neck and chest, and the right groin. The right femoral vein was accessed under ultrasound guidance. Then a guidewire was advanced through the inferior vena cava (IVC) and right atrium (RA), all the way up to the obstruction at the right brachiocephalic vein. A 12 French (Fr) braided sheath was introduced over the wire and advanced to the upper IVC. Then, an angiogram was performed, which confirmed a straight IVC with no stenosis at the IVC–RA junction (Figure 2(a)). Next, an angled glide catheter was advanced over the wire up to the obstruction in the right brachiocephalic vein. A catheter angiogram revealed 50% stenosis at the anastomosis of the superior vena cava (SVC) with the transplanted heart. A 10 Fr sheath that accompanied the Surfacer device was advanced over the wire, but difficulty was encountered advancing it through the RA–SVC junction. Angioplasty was performed at the level of the RA–SVC junction stenosis with a 16 × 40 mm balloon (Figure 2(b)). Post-intervention, the 10 Fr sheath was advanced through the SVC–RA junction without any further difficulty. The tip of the sheath was placed at the occlusion in the right brachiocephalic vein. Then, the guidewire was removed, and the Surfacer device was inserted through the 10 Fr sheath and slowly advanced under fluoroscopy guidance all the way to the occlusion. Then the sharp end of the device was pushed through the occlusion to end in the right IJ vein above the clavicle (Figure 2(c)). Under fluoroscopic guidance, in craniocaudal angle, the needle hole in the tip of the device was aligned to the center of the skin target in the supraclavicular fossa. Then the sharp needle wire of the Surfacer system was pumped through the vein to come out of the skin in the supraclavicular fossa. A dilator peel-away sheath combination was inserted over the sharp end of the wire. Then the Surfacer device was pulled back along with the dilator peel- away sheath combination resulting in the sheath crossing through the occlusion. Surfacer device was removed, and a TDC was inserted through the peel away sheath (Figure 2(d)). The patient tolerated the procedure well and did not develop any immediate complications. There was no incidence of catheter dysfunction requiring an exchange of the catheter or catheter related infection post operatively.
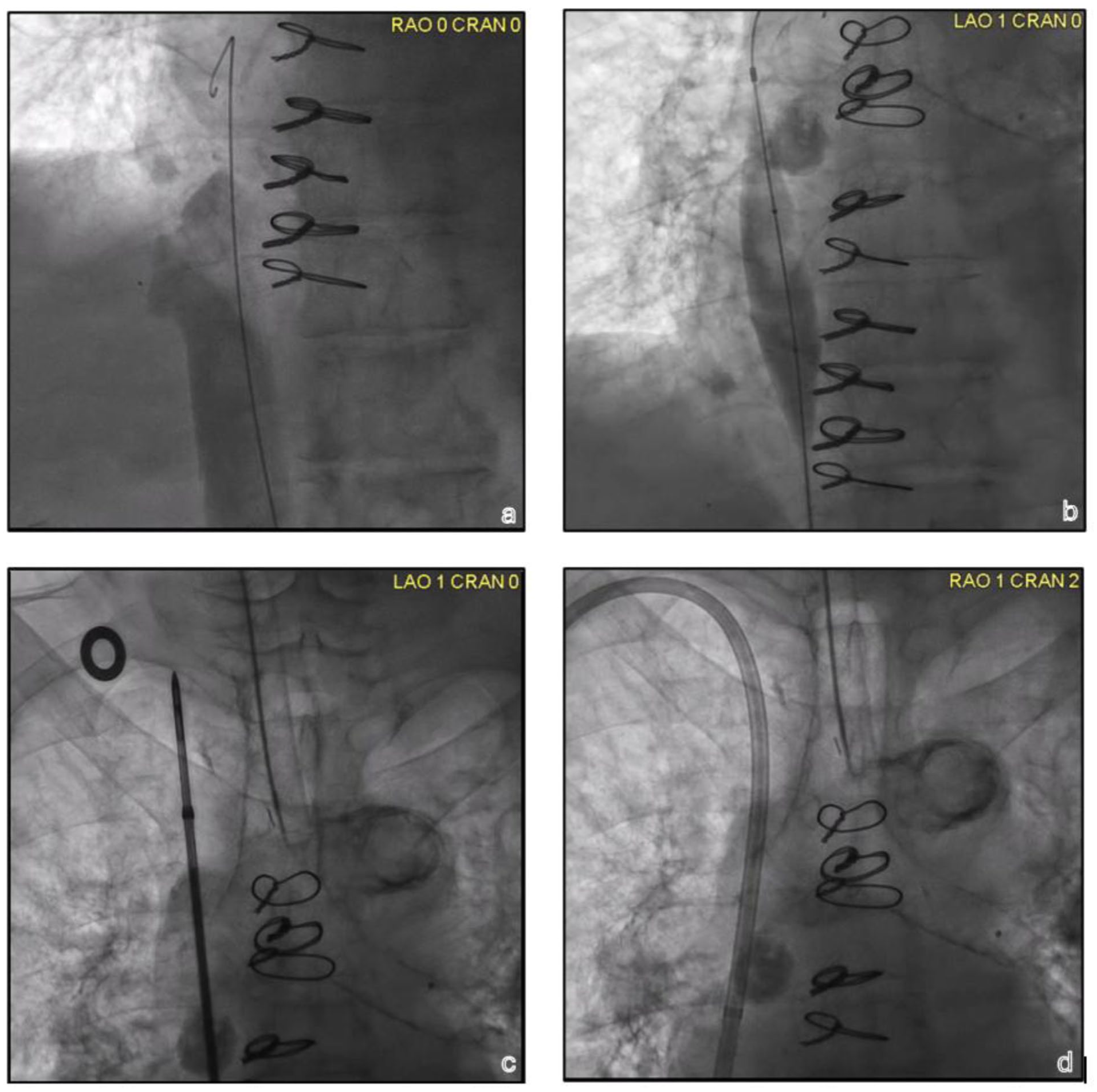
Intraoperative venography and fluoroscopy images: (a) angiogram was performed which confirmed a straight IVC with no stenosis at the IVC–RA junction, (b) angioplasty at the level of the RA–SVC junction stenosis illustrated by the waist, corresponding to the CT angiogram finding, (c) Surfacer device advanced through the occlusion at the right brachiocephalic vein, and (d) tunneled dialysis catheter placement at the cavo-atrial junction.
Discussion
Thoracic central venous occlusion (TCVO) in hemodialysis patients commonly occurs in the setting of prior central venous catheters, resulting in chronic and repetitive endothelial injury and neointimal hyperplasia, organized mural thrombus, or fibrosis. 5 Clinical symptoms of TCVO are dependent on the location and the development of collateral circulation. They could range from being completely asymptomatic, as in superior vena cava (SVC) occlusion with azygos vein drainage, to ipsilateral severe arm swelling or prolonged bleeding in subclavian vein stenosis, or bilateral facial and arm swelling in case of bilateral brachiocephalic (BC) vein or SVC occlusion without adequate azygous vein drainage. 6 There are various classifications to describe patterns of TCVO. One of the classifications is defined by the Society of Interventional Radiology reporting standards for TCVO by anatomical location. Type 1 is the obstruction of the RIJ vein with or without the obstruction of the LIJ or one subclavian vein. Type 2 is obstruction of RIJ with extension into the BC vein. Type 3 is obstruction of bilateral BC veins with involvement of SVC. Type 4 is obstruction of the entire SVC preventing flow to RA. 7 HD catheters are often inserted into the IJ veins, with the catheter tip usually at the cavo-atrial junction, hence, occlusion can occur at any location along the BC veins and SVC. As in our patient, he developed 100% stenosis of both the right and left BC veins due to chronic use of TDCs, corresponding to type 3 TCVO. Endovascular treatment with angioplasty and stenting, performed under fluoroscopic guidance, has become the standard of care for SVC obstruction but may not always be successful.1,7
There are several techniques used to perform orthotopic heart transplant (OHT), such as bicaval and biatrial anastomotic techniques. Our patient underwent OHT with the bicaval anastomosis involving complete resection of the recipient’s right atrium and primary anastomosis of the superior and inferior venae cavae with donor right atrium. A meta-analysis by Zijderhand et al. revealed that bicaval OHT results in more favorable outcomes than biatrial OHT, including mortality. A rare complication associated with bicaval OHT is the obstruction of the SVC or the IVC at the anastomosis. 8 As in our patient, he was noted to have stenosis at the SVC–RA anastomosis. Fortunately, this responded to angioplasty, and we could reduce the stenosis and advance our Surfacer device. Forcing the device through a stenosed area could increase the risk of serious injury to vessels which could be fatal in case of RA–SVC junction rupture.
Another concern in our patient was that he was on chronic immunosuppressive medications, including steroids. Chronic steroid use is thought to increase vascular complications with percutaneous interventions due to their effect on vascular fragility and wound healing. One probable theory where wound healing is affected by corticosteroids is through the inhibition of transforming growth factor-β and insulin-like growth factor, which, in turn, decrease the amounts of hydroxyproline, a surrogate marker for the synthesis of collagen, resulting in a less compliant vessel with poor elasticity. Furthermore, chronic steroid therapy significantly inhibits the proliferation of endothelial progenitor cells that participate in neovascularization and aid in wound healing by moving to areas of injury and regulating repair by excreting proangiogenic factors. 9 In a prospective study by Ellis et al., they compared patients on long-term steroids and those not taking steroids who underwent coronary angioplasty. Their analysis revealed that those taking steroids had a threefold risk of major vascular complications. 10 Although this study addressed arterial lesions, it sheds some light on the detrimental effects of steroids and immunosuppressive medications on the cardiovascular system.
Heart transplant recipients are at risk of anastomotic stenoses as a complication after cardiac transplantation. This, coupled with vascular fragility and poor wound healing associated with long-term steroid use, leads to an increased risk of vascular complications in percutaneous interventions. However, such as in our patient, who have exhausted vascular access from CVOs, insertion of TDC with the Surfacer technique proved to be safe and feasible. After successful recanalization of the central veins and placement of a CVC, it can be converted into a HeRO graft. In patients with CVO, even after recanalization with Surfacer, placement of an AVF or AVG may not be successful or may result in worsening signs and symptoms of CVO due to a much higher flow through the circuit than what the occluded central venous system can handle. Conversion of CVC into a HeRO graft will provide the patient with reliable AV access without developing severe clinical features of CVO and will also help get rid of the CVC which has higher risk of infection. If a patient with CVC placed via Surfacer technique gets a successful kidney transplant, they will no longer need the catheter. Removal of the catheter may result in recurrence of the central venous occlusion. In this situation, it is prudent to monitor for any signs of CVO recurrence which should prompt immediate plan for an angiogram with interventions like angioplasty or endovascular stent placement to maintain the patency of the recanalized central veins.
Conclusion
To our knowledge, this is the first reported successful TDC insertion using the Surfacer Inside-Out technology in a heart transplant recipient. With successful central venous access placement with the Surfacer Inside-out Catheter Access System, we could keep dialysis access through the RIJ vein. This could not only prevent groin access but can also keep the contralateral central veins intact for future medical needs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required per University of Wisconsin—Madison Institution Review Board.
Informed consent
Written informed consent was obtained from the patient at the time of the procedure including for images.