
Abstract
Background:
Reliable vascular access is required for hemodialysis (HD). Central venous catheters (CVC) can be used immediately, but are traditionally associated with increased mortality compared to arteriovenous fistulas or grafts (AVF/AVG). Immature fistulas or grafts may or may not become usable; their impact on long-term mortality or transplant has not been defined.
Methods:
Adult incident HD patients entering the United States Renal Data System between 1/2018 and 12/2019 were identified, and included if still on HD at day 90. Initial dialysis accesses were categorized as mature AVF/AVG, CVC-only, or CVC with an fistula or graft that was not ready for use (CVC-plus). Cox models were used to examine the associations between access type and patient mortality, and logistic models for kidney transplant waitlist appearance, using propensity-matched samples. CVC-plus was the reference group for all models.
Results:
Among 214,673 patients, 66% had CVC-only, 15% CVC-plus, and 19% AVF/AVG. Over median follow up of 30 months, 45% died and 5% received kidney transplants. Compared to patients with CVC-plus, having CVC-only was associated with increased death (HR = 1.31, 95% CI = 1.29–1.35, p < 0.001) but similar rates of kidney transplantation (HR = 1.01, 95% CI = 0.97–1.14, p = 0.20), despite more waitlisting. Having AVF/AVG was associated with decreased death (HR = 0.81, 95% CI = 0.79–0.83) and increased transplantation (HR = 1.39, 95% CI = 1.30–1.50), p < 0.001 for both.
Conclusions:
Initiating HD with CVC-plus was advantageous compared to CVC-only, but outcomes were inferior to those of patients initiating HD with mature AVF/AVG.
Keywords
Introduction
Hemodialysis (HD) cannot be performed without reliable access to the bloodstream. Under ideal conditions, patients with chronic kidney disease are referred for vascular access before requiring dialysis, to allow the access to have become usable prior to initiation of hemodialysis. 1 Surgeons may create an arteriovenous fistula (AVF) from arteries or veins, or a graft (AVG) that uses synthetic materials.
Unfortunately, these ideal conditions are infrequently met. In 2024, 20% of HD patients in the United States initiated HD with a working AVF or AVG; the remaining 80% required placement of a central venous catheter (CVC) in order to start treatments. 2 While CVCs are readily available, immediately ready for use, and avoid the need for percutaneous needle puncture, they unfortunately predispose patients to serious line-associated infections and permanent damage to blood vessels, potentially impeding success of future vascular access options.3,4 Indeed, patients are often reluctant to undergo access surgery and providers may not always have the time or communication skills needed for the thorough education and discussion required to persuade them. Widespread use of other vascular access devices, especially peripherally inserted central catheters, compromises native veins needed for a functional AVF.5,6 The situation is further complicated by timing considerations: surgical sites require time to heal, and AVFs need to mature into usability, a process that fails to occur for 20%–60% of patients.6,7
Among patients initiating HD with CVC, some have an AVF or an AVG that was constructed prior to the development of end-stage kidney disease (ESKD) that is patent but not ready for use. This could be due to any combination of late referral, late surgery, delayed access maturation, surgical complications, or early thrombosis. 5 Earlier work by our group showed that patients who had a non-functional AVF or AVG had lower 1-year mortality, were more likely to transition to a functioning AVF/AVG, and had shorter CVC exposure (3–4 months vs 6 months) compared with patients who started hemodialysis with a CVC as their sole vascular access. 8 However, data is lacking regarding the long-term outcomes associated with presence of an non-functional AVF or AVG. For these reasons, we sought to define HD patient survival and kidney transplant waitlisting in the Medicare population based on the vascular access sites present at the time of incident HD for ESKD.
Methods
United States Renal Data System (USRDS) files were used to identify adult patients (age ⩾ 18 years) who initiated HD as their first ESKD treatment between January 1, 2018 and December 31, 2019, with follow up through 12/31/2022. The research protocol was approved by the Institutional Review Board of the University of Chicago with a waiver of informed consent for a limited dataset (IRB approval #23-1936) on December 12, 2023. The clinical and research activities being reported have been conducted in accordance with the Declaration of Helsinki. Analysis was restricted to patients for whom the vascular access used on the first day of treatment could be identified. Patients who recovered kidney function or were withdrawn from hemodialysis within 90 days were excluded in order to eliminate instances of reversible acute kidney injury and early mortality due to factors unrelated to vascular access.
Using the information provided from this data, initial vascular access was categorized as: (1) functional arteriovenous fistula or graft (“AVF/AVG”); (2) central venous catheter as the sole access (“CVC-only”); or (3) central venous catheter with the presence of an AVF or AVG that was not yet functional (“CVC-plus”). Patient characteristics at the time of treatment initiation were collected including: age, sex, self-reported race, body-mass index (BMI), serum albumin, hemoglobin, estimated glomerular filtration rate (eGFR), primary kidney failure diagnosis (hypertension, diabetes, and other), and whether patients had exposure to nephrology care or dietary care prior to ESKD. Comorbid conditions were categorized as: cancer, cardiac disease, chronic obstructive pulmonary disease (COPD), diabetes, disabled status, hypertension, tobacco use, stroke, and drug and alcohol use disorders.
Statistical analysis
Clinical characteristics were reported for the entire cohort and by initial vascular access categories. Initially, unadjusted and adjusted models were constructed for the entire study population. To address imbalances between baseline comorbid conditions and pre-ESKD nephrology care as potential confounders, propensity score matching was undertaken. Two separate propensity-matched subsets were created using logistic regression models with initial vascular access as the dependent variable. One subset compared CVC-only to CVC-plus and the other compared CVC-plus to AVF/AVG. Greedy matching was utilized due to the large size of the data set, with a caliper of 0.25 for the logit of the propensity score. Matching was assessed by calculation of standardized mean differences using Cohen’s d. Models for patient outcomes were performed on each of the matched subsets. Four models were reported for each outcome: Model 1 was an unadjusted model for effect of vascular access over the entire population. Model 2 was a multivariable adjusted model over the entire population. Models 3 and 4 were propensity score models comparing matched subjects with AVF/AVG (Model 3) and matched subjects CVC-only (Model 4). Patients with CVC-plus were the reference group for all models.
The primary outcome was patient mortality after day 90, evaluated using Cox proportional hazards models for time to death. For this analysis, patients were followed until death, or December 31, 2021. Patients were censored at the time of first kidney transplant, change in modality to peritoneal dialysis, recovery of kidney function, or loss to follow up, if the subsequent event period persisted for ⩾30 days. Mortality was assessed over the entire population, and also over both propensity-matched subsets. The secondary outcome was time to kidney transplantation. Multivariable models were adjusted for age, sex, race (Black, Hispanic, White, and other), BMI, pre-ESKD nephrology care, pre-ESKD dietician care, and primary kidney failure diagnosis (diabetes, hypertension, others), as well as baseline serum albumin, hemoglobin, and eGFR. In addition, adjustment was made for the following co-morbid conditions: cancer, cardiac disease, COPD, diabetes, disabled status, hypertension, tobacco use, stroke, and drug and alcohol use disorders. These covariates were also used to perform propensity-matching.
Sensitivity analyses with the insertion of two-way interaction variables were performed to establish whether patient age or serum albumin exerted effect modification on the impact of vascular access type.
All analyses were conducted using SAS, version 9.4 (SAS Institute Inc., Cary, NC).
Results
There were 214,673 subjects who met inclusion criteria, of whom 141,204 (66%) initiated HD with CVC-only, 32,282 (15%) with CVC-plus, and 41,187 (19%) with AVF/AVG. Among patients with CVC-plus, 91% (n = 29,293) had non-functional AVF and 9% (2989) had an non-functional AVG. The flow diagram for study inclusion is illustrated in Figure 1. Median follow-up for the cohort was 30 months, with an interquartile range (IQR) of 18–38 months. Baseline characteristics are shown in Table 1. Mean age was 63.6 ± 14.5 years, and 42% were female. Compared to patients initiating with AVF/AVG, those starting with CVC-only were more likely to be female and to have comorbid conditions (aside from hypertension and a history of cancer) and less likely to have pre-ESKD nephrology and dietician care. Patients with CVC-plus demonstrated an increased prevalence of diabetes (67% vs 61% for AVF/AVG and 62% for CVC-only). The propensity-matched subset for CVC-only versus CVC-plus retained 64,564 patients (30.1%); the propensity-matched subset for with CVC-plus versus AVF/AVG retained 59,984 patients (27.9%). Standardized mean differences for the matched subsets are shown in Tables S2 and S3, indicating excellent matching across all covariates.
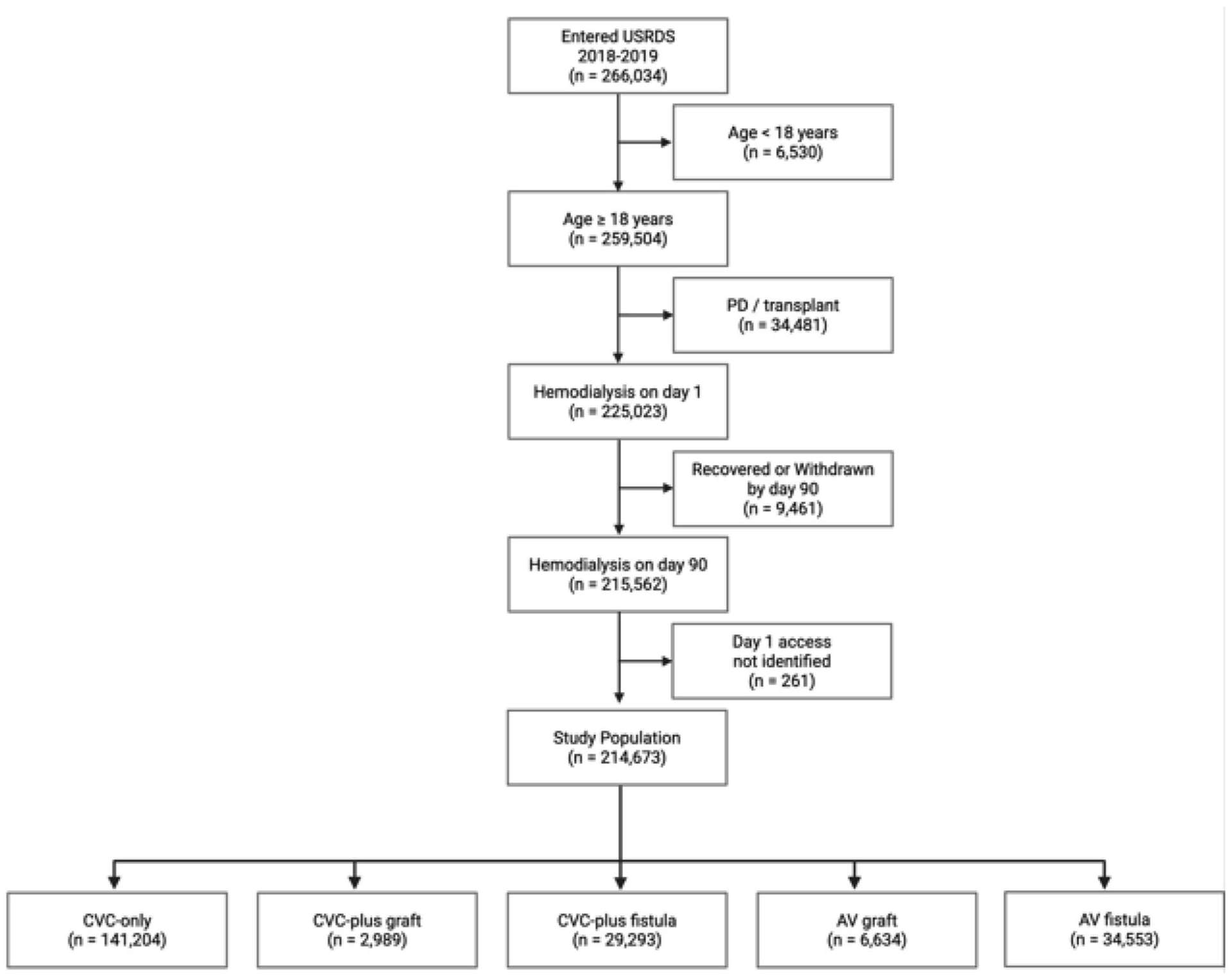
Flow diagram for inclusion into the analysis.
Baseline characteristics of patients initiating hemodialysis from 2018 to 2019.
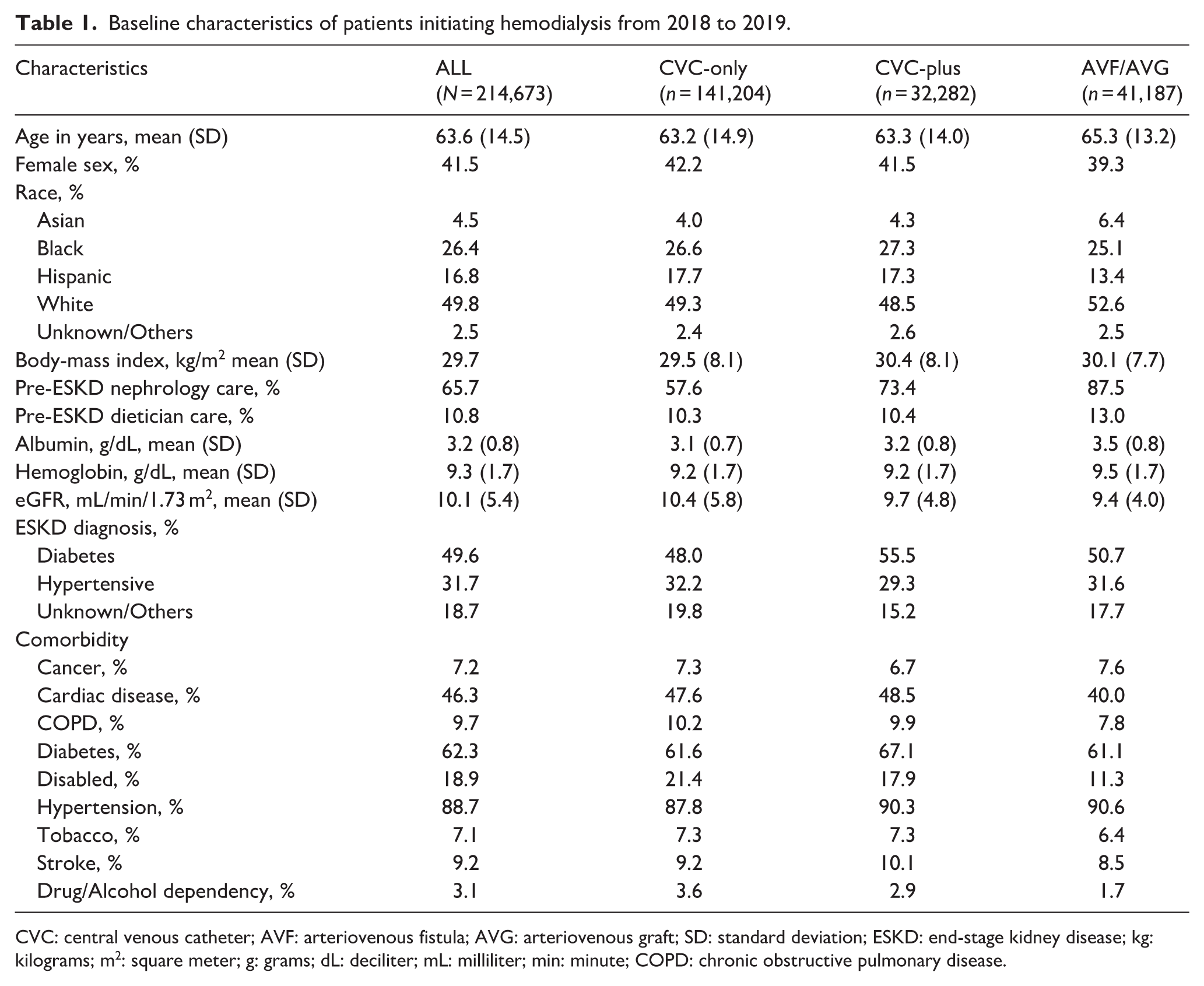
CVC: central venous catheter; AVF: arteriovenous fistula; AVG: arteriovenous graft; SD: standard deviation; ESKD: end-stage kidney disease; kg: kilograms; m2: square meter; g: grams; dL: deciliter; mL: milliliter; min: minute; COPD: chronic obstructive pulmonary disease.
Patient survival
Over the course of the study, 108,469 patients (51%) died. Death occurred in 76,366/141,204 (54%) of patients with CVC-only, 15,560/32,282 (48%) of patients with CVC-plus, and 16,543/41,187 (40%) of patients with AVF/AVG. Cox models for patient survival are shown in Table 2. Over the whole population, the unadjusted hazard ratio (HR) for death was 0.78 (95% confidence interval (CI) = 0.76–0.80) for patients with AVF/AVG, and 1.31 (95% CI = 1.29–1.34) for patients with CVC-only, p < 0.001 for both. These effects were moderated but not extinguished by adjustment. Full unadjusted and adjusted models for patient death in the unmatched population (N = 214,673) are shown in Table S1.
Cox proportional hazard models for 90-day mortality by initial vascular access type.
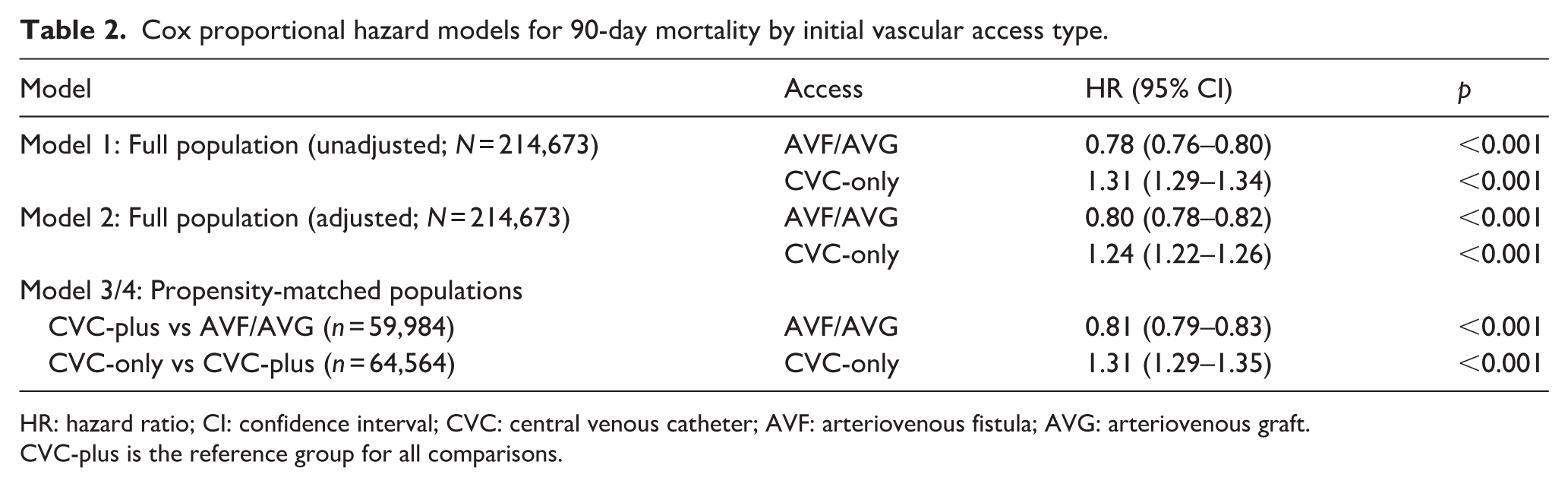
HR: hazard ratio; CI: confidence interval; CVC: central venous catheter; AVF: arteriovenous fistula; AVG: arteriovenous graft.
CVC-plus is the reference group for all comparisons.
Within the matched subsets, CVC-only patients were associated with an increased hazard of death (aHR = 1.31 (95% CI = 1.29–1.35), p < 0.001) compared to CVC-plus patients. Patients in the matched subset with AVF/AVG had reduced risk of death (HR = 0.81 (95% CI = 0.79–0.83), p < 0.001), compared to CVC-plus patients.
Kidney transplantation and waitlisting
During the study period, 29,450 (13.7%) patients were waitlisted and 10,957 (5.1%) of patients received kidney transplants. Results for listing and transplantation are shown in Table 3. While patients with CVC-plus were more likely to be listed than patients with CVC-only (14% vs 12%, p < 0.001), the rate of transplantation did not differ (4.7% vs 4.6%, p = 0.30). Patients with AVF/AVG were substantially more likely to be transplanted than patients with CVC (7.3% vs 4.6%, p < 0.001).
Waitlisting and transplantation by incident vascular access type.
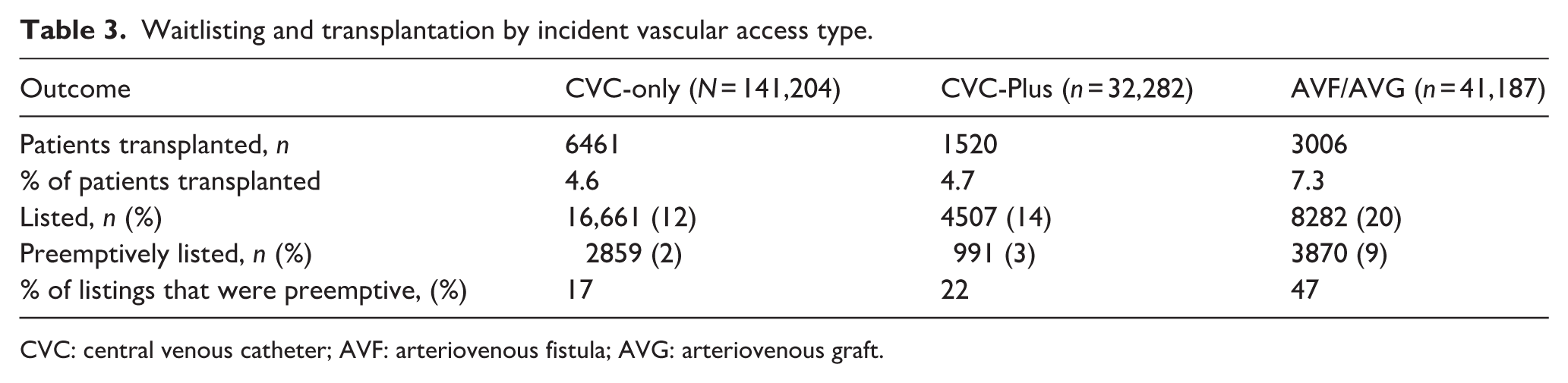
CVC: central venous catheter; AVF: arteriovenous fistula; AVG: arteriovenous graft.
Model results for transplantation are shown in Table 4. In the full population, compared to CVC-plus, the unadjusted hazard ratio (HR) for transplantation was 1.01 (95% CI = 0.95–1.07, p = 0.72) for patients starting with CVC-only, and 1.54 (95% CI = 1.44–1.64) for patients starting with AVF/AVG, p < 0.001. The association of AVF/AVG with increased transplant persisted after multivariable adjustment (HR = 1.31 (95% CI = 1.23–1.40, p < 0.001). In the propensity matched populations, having AVF/AVG at initiation of dialysis was associated with increased transplantation (HR = 1.39, 95% CI = 1.30–1.50, p < 0.001); while the rate of kidney transplant did not differ between patients initiating with CVC-only, compared to patients starting with CVC-plus (HR = 1.05, 95% CI = 0.97–1.14, p = 0.20). Unadjusted and adjusted models for transplant over the unmatched full population are shown in Table S4.
Cox models for kidney transplant by initial vascular access type.
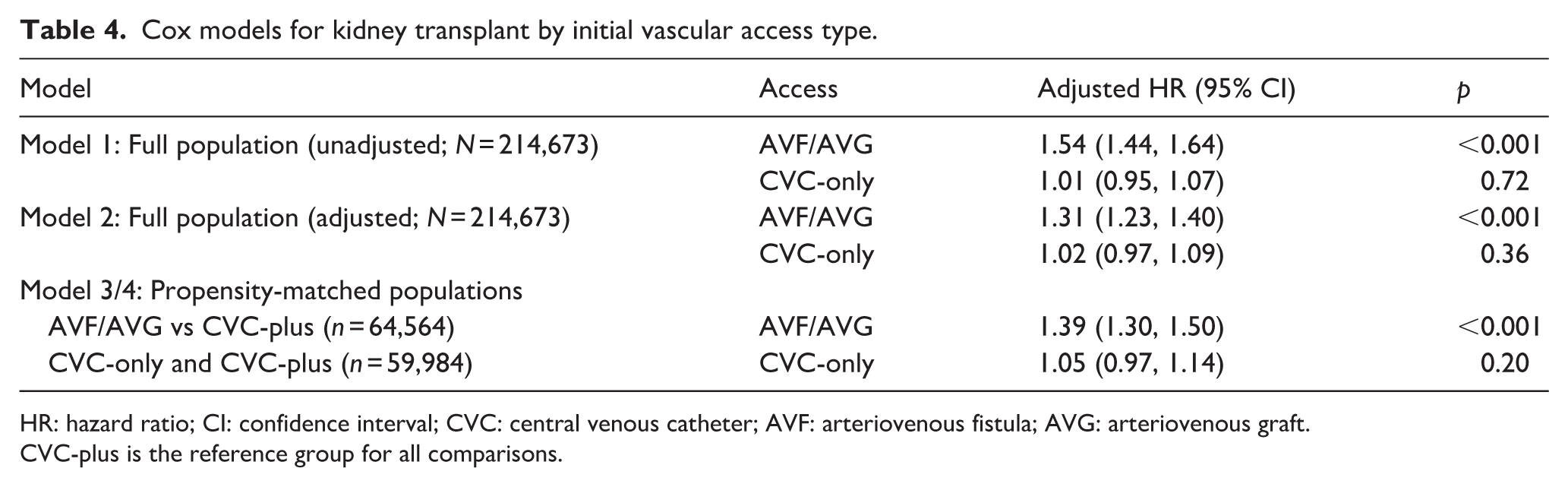
HR: hazard ratio; CI: confidence interval; CVC: central venous catheter; AVF: arteriovenous fistula; AVG: arteriovenous graft.
CVC-plus is the reference group for all comparisons.
In the sensitivity analyses, inclusion of two-way interaction variables in the model did not result in significant effect modification by patient age or serum albumin. Subgroup hazard ratios are shown in Tables S5 and S6.
Discussion
Among patients initiating HD with a CVC, those who had a non-functional AVF or AVG had better survival, compared to patients with a CVC as their sole vascular access. Nonetheless, initiating dialysis with a functional AVF/AVG was associated with better survival. The rates of kidney transplantation did not differ between patients with CVC-only and CVC-plus, but were significantly increased among patients initiating dialysis with AVF/AVG.
Much has been written about the comparison of AVF/AVG with CVC-only,9,10 with the hemodialysis and vascular access communities retreating from an inflexible dedication to AVF toward a more nuanced goal of “the right access at the right time for the right patient.” 11 The successful production of a mature AVF/AVG is a complicated and time-consuming process involving many different stakeholders, as illustrated in Figure 2. The time and skills of many different professionals are needed, and substantial patient involvement, motivation and resolve are required to bring the process to a successful conclusion. For many patients, it is deeply counterintuitive to undergo a surgical procedure in order to enable ongoing sharp cannulation, and to do this prior to the onset of illness bespeaks a dedication to self-care. 12 A functional AVF represents successful navigation of the entire pathway; arriving at ESKD in a state of CVC-plus indicates a process that was underway, but did not reach completion. For some CVC-plus patients, only time is required for completion; in others, access maturation will not occur, and these patients face repeated cycles of referral and invasive procedures.1,6,7
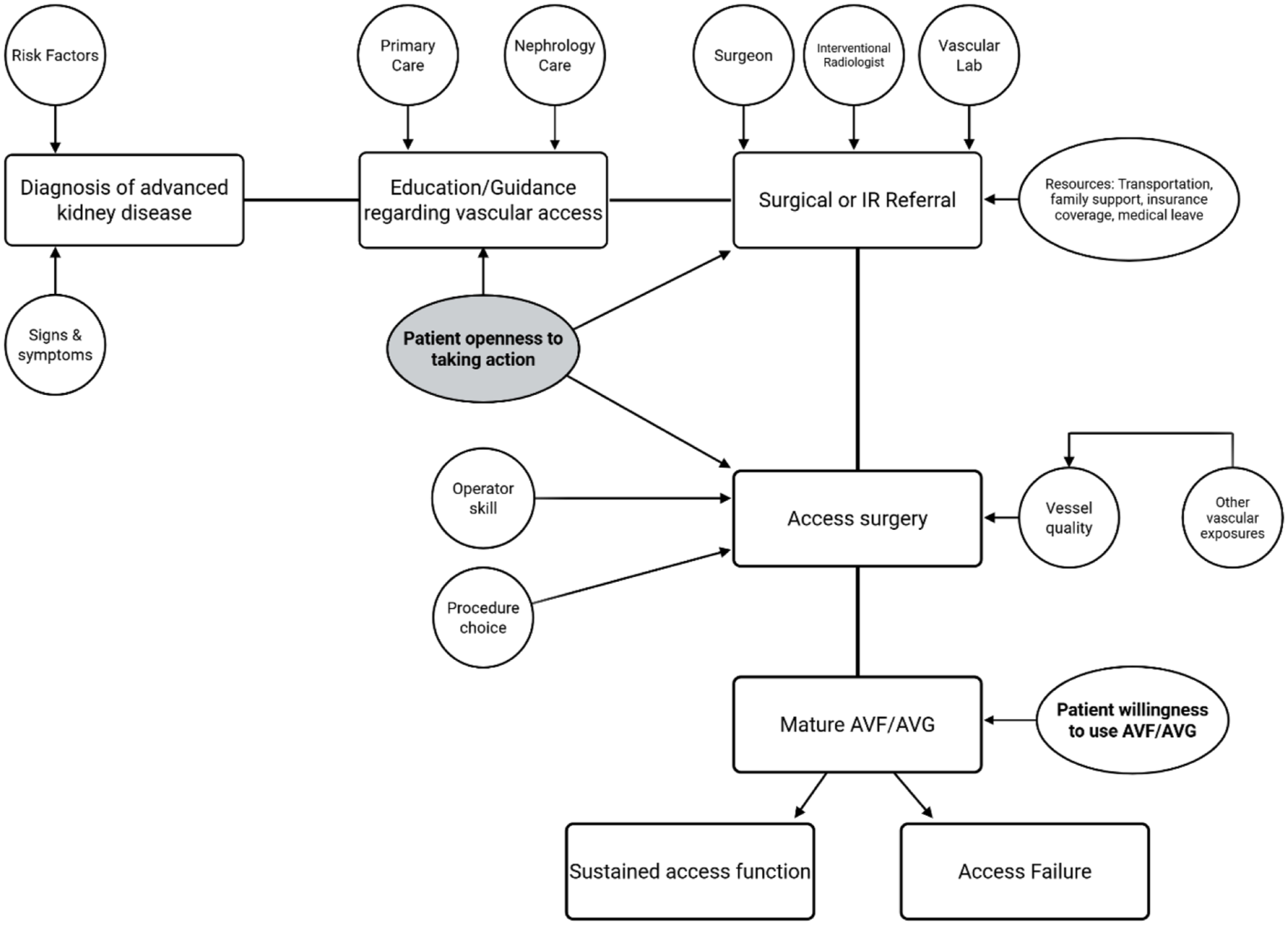
Flow diagram outlining the tasks and resources required for the process of creating an arteriovenous fistula or graft.
An unsuccessful CVC-plus attempt leaves patients in a similar state as CVC-only, as some patients initiating HD with CVC-only are also at intermediate stages of the process. Some are contending with kidney failure that occurred with little or no foreknowledge, and some have made an autonomous decision to delay or decline AVF/AVG, even when fully informed of risks and benefits. 13 CVC-plus patients have demonstrated their willingness to proceed, even if this willingness is not entirely limitless, and the importance of patient activation cannot be overstated. 12
The underlying question addressed here is whether early attempts at permanent access creation produce benefits for patients, even when maturation failures are common. There are important physical factors that affect vessel maturation, which can in turn be influenced by preceding medical exposures. Diseases that are associated with ESKD are also often associated with excess hospitalization and intravascular devices, including peripherally-inserted central catheters, implantable cardioverter-defibrillators, chemotherapy ports, and subclavian venous catheters and pulmonary artery catheters.6,14,15 Vessel depletion is not uncommon amongst patients with ESKD, and can occur at any point during their natural history of kidney disease, including prior to ESKD and even after reinitiation of dialysis after a failed kidney allograft. 16 Proceeding earlier may result in more and better quality vessels being available for access construction. However, earlier failures expend the physical and emotional resources of patients, and require assiduous support and continued patient motivation.
The same internal and extrinsic forces that propel patients toward vascular access would also be expected to promote candidacy for kidney transplant. We did not demonstrate a difference in the rate of transplantation between CVC patients with and without unready AVF/AVG, possibly reflecting the complexity of the transplantation evaluation process. Episodes of CVC-related septicemia would be expected to reduce opportunities for transplant, but so could sequelae of failed vascular access attempts, such as thrombosis or vascular steal. Furthermore, failure of AVF or AVG, and continued dependence on CVC may be a result of severe peripheral artery disease, which may also complicate a patient’s candidacy for kidney transplantation. 17 Less obvious is whether the patient activation involved in moving toward AVF or AVG signals a perception of a more cooperative potential candidate for transplantation. 12 Our observational data were not designed to evaluate these interesting questions.
Our data did show that on balance, patients acting on vascular access prior to the onset of ESKD was associated with reduced mortality. These findings were robust to adjustment for clinical and demographic factors and persisted when the population was balanced in terms of propensity to have surgery. These findings should provide motivation for clinicians who are working with patients at advanced stages of chronic kidney disease and reduce patient and provider temptation to wait for ESKD before acting on vascular access.
The strengths of this study are the large population, with substantial follow-up time and the use of a propensity-score model to adjust for multiple factors. Limitations include reliance upon retrospective registry data, with few covariates that reflect patient resources and patient activation. Additional confounding due to unmeasured covariates remains possible. Nonetheless, our data adds further understanding to the literature regarding vascular access and population-based outcomes.
In conclusion, early attempts to secure vascular access in patients with advanced kidney disease may be advantageous to patients, even when remaining time to ESKD is not sufficient to complete a working AVF or AVG.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261461909 – Supplemental material for Clinical significance of maturing vascular access for incident hemodialysis patients
Supplemental material, sj-docx-1-jva-10.1177_11297298261461909 for Clinical significance of maturing vascular access for incident hemodialysis patients by Andrea Liu, Ryan M Song, Jacob Ryno, Mary Hammes, Peter Angelos, Ted A Skolarus and Rita L McGill in The Journal of Vascular Access
Footnotes
Acknowledgements
The data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation of the U.S. government.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.L.M. is a member of the editorial board of the Journal of Vascular Access. The authors declared no other potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) awards U2CDK129917 and TL1DK132769.
Data sharing statement
The datasets used and/or analyzed during the current study are available from the United States Renal Data System (USRDS) upon Data Use Agreement (DUA) approval. Per the DUA between the authors and NIDDK, the rerelease of the data or the deposition of data into publicly available repositories or to individuals is not allowed.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.