
Abstract
Introduction:
Arteriovenous fistula (AVF) dysfunction causes significant morbidity in maintenance hemodialysis (MHD) patients. This study investigated the association between the gut-derived uremic toxin Trimethylamine-N-oxide (TMAO) and AVF failure risk.
Methods:
Baseline serum TMAO was measured in 164 MHD patients with functional AVFs. The primary endpoint over a 24-month follow-up was the first AVF dysfunction event. We utilized optimal cut-point determination, Kaplan-Meier survival analysis, and Cox proportional hazards models.
Results:
Over 24 months, 43 patients (26.2%) experienced AVF dysfunction. The optimal TMAO cut-point was 278.74 μmol/L. High TMAO (>278.74 μmol/L) correlated with significantly earlier AVF dysfunction (log-rank p = 0.030) and remained an independent predictor of AVF failure after multivariable adjustment (HR, 2.07; 95% CI, 1.04–4.13; p = 0.035).
Discussion:
Elevated baseline TMAO is an independent risk factor for AVF dysfunction. Serum TMAO >278.74 μmol/L serves as a novel prognostic risk stratifier identifying MHD patients at high risk for vascular access failure.
Keywords
Introduction
Chronic kidney disease (CKD) has emerged as a major public health concern worldwide. For patients progressing to end-stage renal disease (ESRD), renal replacement therapy (RRT) becomes essential for survival. 1 Data from the Chinese National Renal Data System (CNRDS) between 2012 and 2022 reveal a significant annual increase in the incidence of RRT in China, of which hemodialysis (HD) was the predominant modality, comprising 82.4% of cases in 2022. 2 The efficacy of hemodialysis and, consequently, patient survival are intrinsically linked to the reliability of the vascular access system. Therefore, establishing and maintaining functional vascular access and preventing its dysfunction are critical determinants of long-term patient outcomes. 3
The autogenous arteriovenous fistula (AVF) is the most common type of vascular access for hemodialysis and is widely recommended as the first-line choice by clinical guidelines.3,4 Complications related to vascular access are a major contributor to increased morbidity, hospitalization rates, and healthcare costs among HD patients, and they also represent a leading cause of cardiovascular events and mortality.5,6 Flow-limiting stenosis and thrombosis represent the principal complications that ultimately lead to AVF failure. 7 Recognizing this, routine surveillance of vascular access is widely recommended by clinical guidelines as a crucial strategy for the early detection and intervention of malfunction, aiming to prevent thrombosis and ensure dialysis adequacy.3,4,8 Recent observational studies have explored potential associations between AVF dysfunction in HD patients and several emerging variables, including mean platelet volume (MPV), p-Cresyl sulfate (PCS), retinol-binding protein 4 (RBP4), and hemodynamic parameters.9–12 However, these associations remain largely circumstantial, and these variables have not yet been definitively established as clinical biomarkers for stenosis progression. Nevertheless, they highlight the complex, multifactorial nature of alterations in vascular structure and intimal hyperplasia, which are primary pathological mechanisms underlying AVF failure. 13
Trimethylamine-N-oxide (TMAO), a prominent gut-derived uremic toxin, is generated when gut bacteria metabolize dietary choline, carnitine, and betaine into trimethylamine (TMA), which is then oxidized to TMAO by hepatic flavin-containing monooxygenases (FMOs). Studies have demonstrated that TMAO accumulates in patients with CKD, and elevated TMAO levels are closely associated with both CKD progression and the incidence of cardiovascular events. 14 This accumulation is exacerbated in ESRD, where compromised renal clearance leads to circulating TMAO concentrations far exceeding those of healthy individuals. This pathological elevation of TMAO is considered a potential risk factor for adverse clinical outcomes in the ESRD population. 15 Supporting this, high circulating TMAO has been shown to be an independent predictor of hospitalization, as well as cardiovascular and all-cause mortality, among patients on maintenance hemodialysis (MHD).16,17
Multiple studies have indicated that TMAO promotes vascular endothelial dysfunction and promotes vascular calcification through the activation of the nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) signaling pathway and the NLR family pyrin domain containing 3 (NLRP3) inflammasome.14,18 Given these potential pathogenic effects of TMAO on vascular endothelium, we hypothesized that aberrant TMAO levels might also impact the function of vascular access in patients undergoing MHD. However, to date, few large-scale cohort studies have directly investigated the association between serum TMAO levels and AVF dysfunction in the MHD population. Therefore, this study aims to explore the association between serum TMAO levels and the time to the first AVF dysfunction event in MHD patients, and to evaluate its value in predicting access failure.
Materials and methods
Study design and participants
A total of 164 patients with ESRD undergoing maintenance hemodialysis at the Blood Purification Center of the Baoshan Branch of Huashan Hospital, Fudan University, were enrolled between March 2023 and September 2023. These patients were subsequently followed up from October 1, 2023 to September 30, 2025. During the study period, all participants received hemodialysis using polysulfone dialyzers and bicarbonate-based dialysate. This study protocol was in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Ethics Review Board of Huashan Hospital, Fudan University (No. KY2024-1355), and written informed consent was obtained from all participants prior to their inclusion in the study.
Eligible participants were adults (age ⩾18 years) who had been receiving a stable hemodialysis regimen for at least 6 months, consisting of two weekly hemodialysis (HD) sessions and one weekly hemodiafiltration (HDF) session (4 h each), utilized an AVF for vascular access, were anuric or nearly anuric (urine output < 100 mL/day), and had complete medical records. Furthermore, all included patients were required to have normal AVF function confirmed by duplex ultrasound within 3 months prior to enrollment. Patients were excluded if they used other access types such as an arteriovenous graft (AVG) or a central venous catheter (CVC), had potential for renal function recovery, or suffered from other organ failures. Additional exclusion criteria included uncorrected or incorrigible congestive heart failure, a recent history of major cardiovascular or cerebrovascular events (myocardial infarction, cerebral infarction, or cerebral hemorrhage within 3 months), active gastrointestinal bleeding within the past month, or an untreated malignancy within the past 5 years. Patients with incomplete medical records or those who were unable to cooperate or refused consent were also excluded.
Data collection
Baseline demographic and clinical data, including age, gender, dialysis vintage, and cause of ESRD, were extracted from the electronic medical records. Anthropometric measurements, including height, pre- and post-dialysis weight, and blood pressure, were recorded. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in meters (kg/m2). The mean pre-dialysis systolic (SBP) and diastolic (DBP) blood pressure over the 3 months prior to enrollment served as baseline values. In the last week of September 2023, pre-dialysis venous blood samples were collected after a minimum 6-h fast. A comprehensive panel of laboratory parameters was analyzed, which included complete blood count, electrolytes, markers of liver and renal function, lipid profiles, iron metabolism, N-terminal pro-B-type natriuretic peptide (NT-proBNP), C-reactive protein (CRP), intact parathyroid hormone (iPTH), etc. Dialysis adequacy was assessed using single-pool Kt/V. 19
Pre-dialysis blood samples were collected from fasting (⩾6 h) patients in the last week of September 2023. Serum TMAO concentrations were subsequently measured using an enzyme-linked immunosorbent assay (MIBio, Shanghai, China) following the manufacturer’s protocol. 20
Clinical outcomes
In this cohort study, 164 MHD patients were followed from October 1, 2023 to September 30, 2025. The primary endpoint of this study focused strictly on secondary AVF failure (late dysfunction) in previously mature and functional fistulas. Primary failures (early maturation failures) were inherently excluded, given the inclusion criteria requiring an established dialysis vintage of at least 6 months. In the present analysis, AVF dysfunction was defined as the first occurrence during the follow-up period of thrombosis or clinically significant stenosis (defined as >50% luminal narrowing accompanied by clinical indicators of dysfunction) requiring endovascular or surgical intervention, such as percutaneous transluminal angioplasty (PTA), catheter-directed thrombectomy, or surgical access revision, or the inability to complete a full dialysis session.12,21 Secondary endpoints, specifically all-cause mortality and transfers to other facilities or treatment modalities, were systematically documented using data from official medical records.
Statistical analysis
Data management was performed using Microsoft Excel (Version 16.80; 2023 Microsoft Corporation). All statistical analyses and graphical representations were conducted using RStudio (Version 2025.05.0+496).
Continuous variables were tested for normality using the Shapiro-Wilk test. Normally distributed variables are presented as mean ± standard deviation (SD), while non-normally distributed variables are presented as median [interquartile range, IQR]. Categorical variables are described as frequencies and percentages. For comparisons between two groups, the independent samples t-test was used for normally distributed continuous variables, and the Mann-Whitney U test was used for non-normally distributed variables.
The relationship between serum TMAO levels and the AVF dysfunction event was visualized using Kaplan-Meier survival curves, generated with the survival package in R. The optimal cut-point for baseline serum TMAO to stratify patients was determined using the maximally selected rank statistic method via the surv_cutpoint function in the survminer package.22,23 To internally cross-validate the robustness of this identified threshold, a Survival Classification and Regression Tree (CART) analysis was additionally performed as an unbiased machine-learning approach for risk stratification.24,25 The value that maximized the survival difference between groups was 278.74 μmol/L (Supplemental Figure S1), closely matching the CART-derived root-node split (279.69 μmol/L) to confirm its mathematical robustness (Supplemental Figure S2). Based on this cut-point, the cohort was divided into a high TMAO group (>278.74 μmol/L) and a low TMAO group (⩽278.74 μmol/L). The log-rank test was used to assess the significance of the difference in event-free survival between the two groups.
To evaluate the impact of TMAO levels on the risk of AVF dysfunction, univariable and multivariable Cox proportional hazards models were employed. First, all clinically relevant factors were included in univariable analyses. Multicollinearity among variables was assessed using the tolerance and variance inflation factor (VIF), with tolerance > 0.1 and VIF < 5 indicating no significant multicollinearity. Subsequently, variables from the univariable analysis with a p-value < 0.1 were entered into a multivariable Cox regression model. A stepwise regression approach was used for final variable selection to construct the final model. Additionally, a 1:1 propensity score matching (PSM) sensitivity analysis was performed using a nearest-neighbor algorithm to control for potential confounding from baseline nutritional and inflammatory statuses (including age, BMI, serum albumin, and CRP).
All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant.
Results
Baseline characteristics of the patients
A total of 164 patients on maintenance hemodialysis were included in this study. The baseline characteristics of the cohort are summarized in Table 1. The median age of the participants was 65.00 [57.00, 69.00] years, and the median dialysis vintage was 54.50 [24.75, 94.50] months. The cohort comprised 108 (65.9%) male and 56 (34.1%) female patients. The causes of ESRD were diabetic kidney disease (n = 46, 28.0%), primary glomerulonephritis (n = 36, 22.0%), hypertensive nephropathy (n = 34, 20.7%), and other causes (n = 48, 29.3%).
Baseline characteristics of the study population stratified by serum TMAO levels.
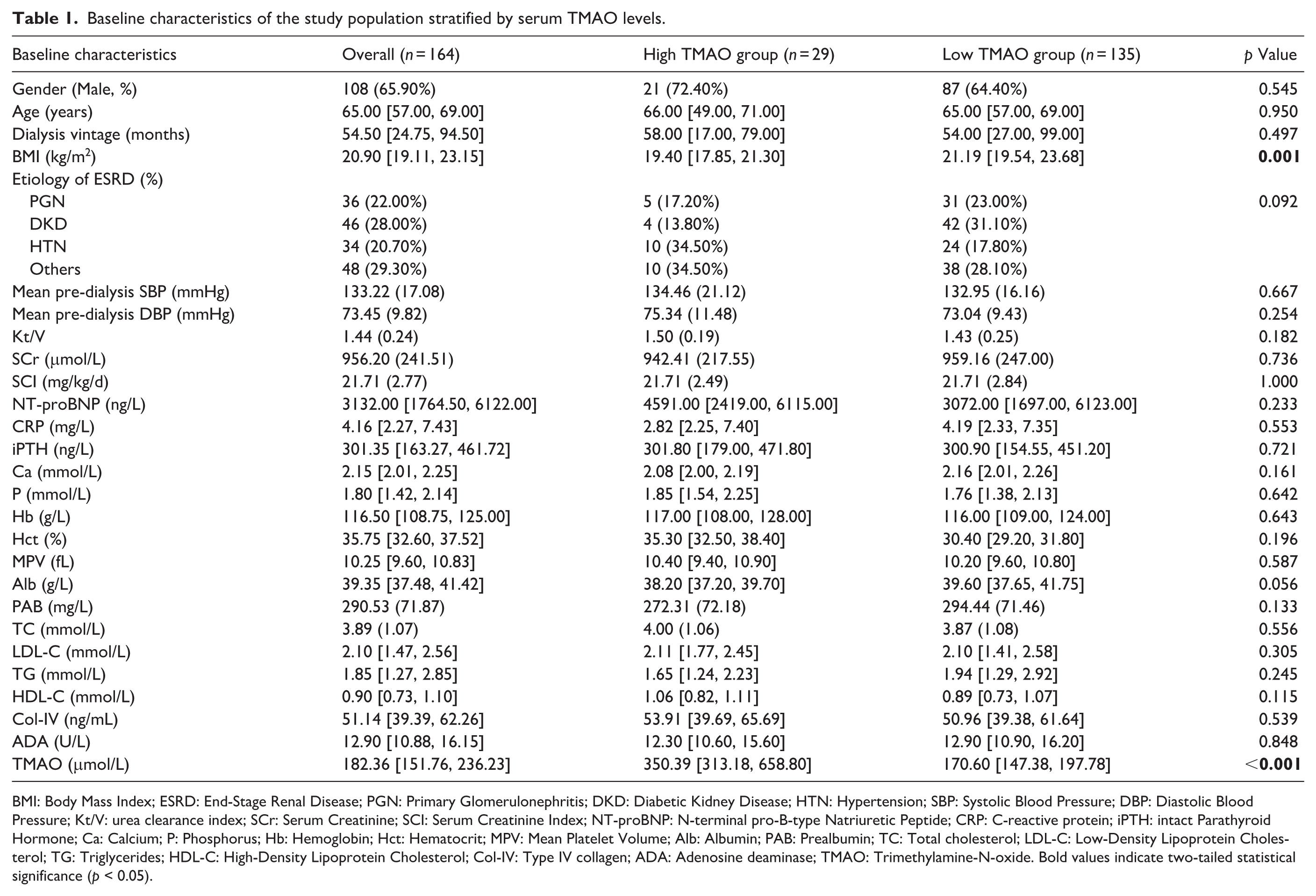
BMI: Body Mass Index; ESRD: End-Stage Renal Disease; PGN: Primary Glomerulonephritis; DKD: Diabetic Kidney Disease; HTN: Hypertension; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; Kt/V: urea clearance index; SCr: Serum Creatinine; SCI: Serum Creatinine Index; NT-proBNP: N-terminal pro-B-type Natriuretic Peptide; CRP: C-reactive protein; iPTH: intact Parathyroid Hormone; Ca: Calcium; P: Phosphorus; Hb: Hemoglobin; Hct: Hematocrit; MPV: Mean Platelet Volume; Alb: Albumin; PAB: Prealbumin; TC: Total cholesterol; LDL-C: Low-Density Lipoprotein Cholesterol; TG: Triglycerides; HDL-C: High-Density Lipoprotein Cholesterol; Col-IV: Type IV collagen; ADA: Adenosine deaminase; TMAO: Trimethylamine-N-oxide. Bold values indicate two-tailed statistical significance (p < 0.05).
The median TMAO level of the study cohort was 182.36 [151.76, 236.23] μmol/L. Based on the optimal cut-point value of 278.74 μmol/L, patients were stratified into a high TMAO group (n = 29) and a low TMAO group (n = 135). A comparison of their baseline characteristics is presented in Table 1. Patients in the high TMAO group had a significantly lower BMI (19.40 [17.85, 21.30] vs 21.19 [19.54, 23.68] kg/m2, p = 0.001) compared to the low TMAO group. Additionally, there was a trend toward lower serum albumin levels in the high TMAO group compared to the low TMAO group (38.20 [37.20, 39.70] vs 39.60 [37.65, 41.75], although this difference did not reach statistical significance (p = 0.056). No other significant differences in baseline characteristics were observed between the two groups (p > 0.05).
Clinical outcomes
During the 24-month follow-up period, among the 164 MHD patients enrolled, 18 (10.9%) deaths occurred, and 11 (6.7%) patients were censored due to transfer to other medical facilities or treatment modalities. Of the 18 mortalities, 10 were attributed to cardiovascular causes. The remaining eight non-cardiovascular deaths resulted from malignancy (n = 4, 22.2%), infection (n = 2, 11.1%), trauma (n = 1, 5.6%), and suicide due to depression (n = 1, 5.6%). Among the 11 patients who were censored, 8 continued hemodialysis at other centers, and 3 successfully underwent kidney transplantation and discontinued dialysis.
Over the 24-month follow-up period, 43 of the 164 patients (26.2%) experienced an AVF dysfunction event (Supplemental Table S1). The Kaplan-Meier survival analysis demonstrated that patients in the high TMAO group (>278.74 μmol/L) had a significantly higher risk of developing AVF dysfunction compared to those in the low TMAO group (log-rank p = 0.030; Figure 1).
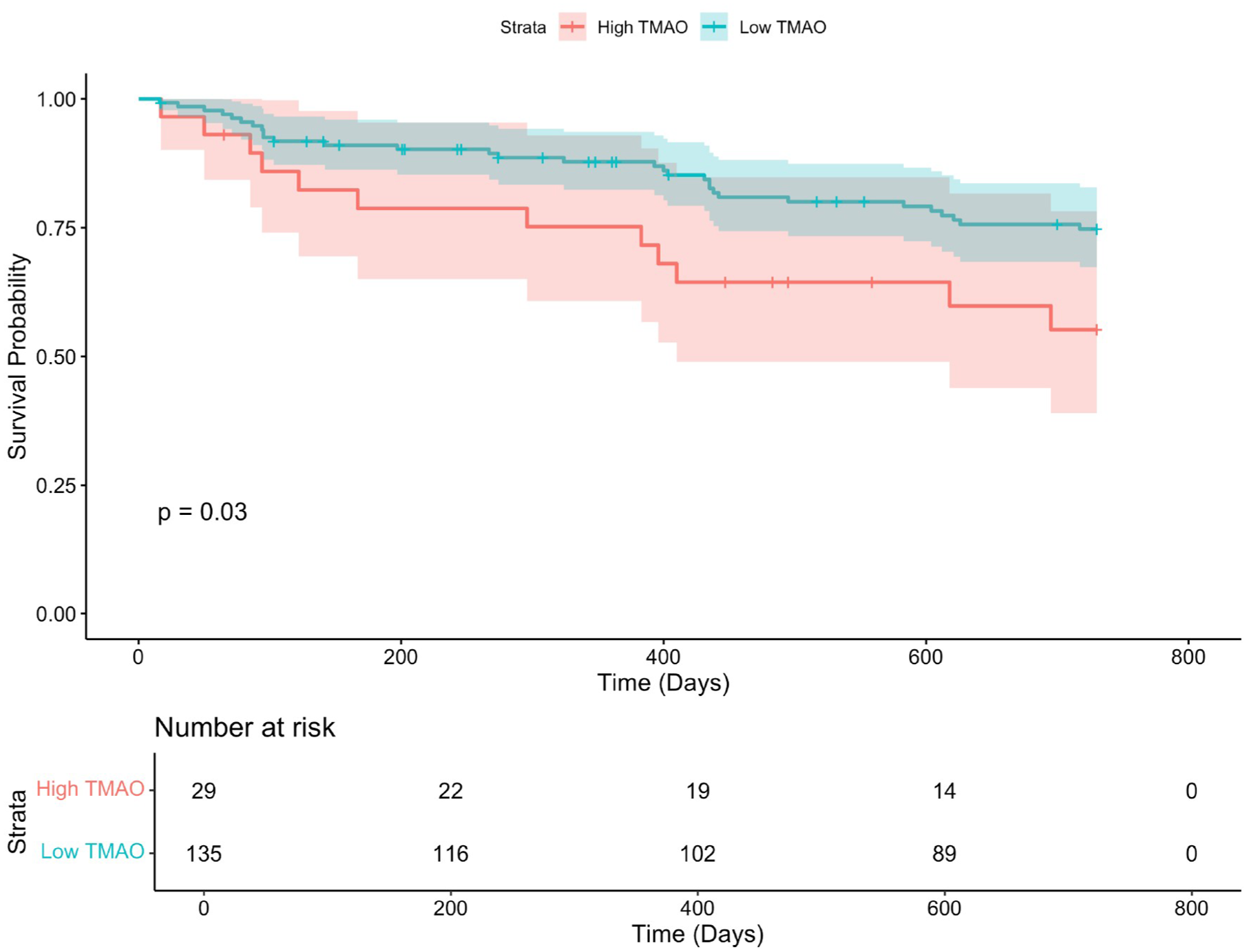
Kaplan-Meier survival curves for AVF dysfunction events.
Univariable and multivariable analysis
Univariable analysis revealed that serum TMAO >278.74 μmol/L was significantly associated with an increased risk of vascular access events (HR, 2.06; 95% CI, 1.06–4.02; p = 0.033). Additionally, prealbumin, adenosine deaminase, type IV collagen, and mean pre-dialysis systolic blood pressure showed potential associations with the outcome (p < 0.1).
After accounting for multicollinearity (VIF < 5), the final multivariate Cox proportional hazards analysis identified both a high TMAO level (>278.74 μmol/L; HR = 2.07, 95% CI 1.04–4.13, p = 0.035) and type IV collagen (HR = 1.02, 95% CI 1.00–1.04, p = 0.016) as independent predictors of AVF dysfunction in MHD patients (Table 2, Supplemental Figure S3).
Univariable and multivariable Cox regression analysis for AVF dysfunction.
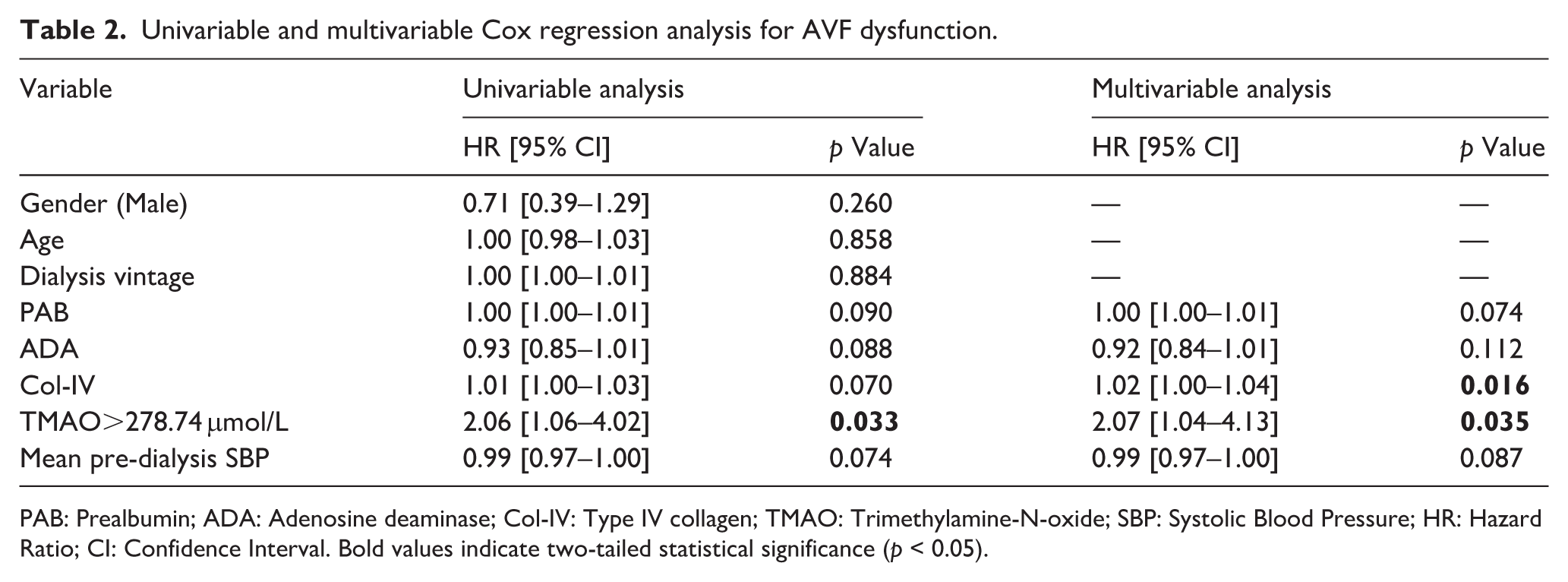
PAB: Prealbumin; ADA: Adenosine deaminase; Col-IV: Type IV collagen; TMAO: Trimethylamine-N-oxide; SBP: Systolic Blood Pressure; HR: Hazard Ratio; CI: Confidence Interval. Bold values indicate two-tailed statistical significance (p < 0.05).
Importantly, in the PSM sensitivity cohort (n = 58; 29 pairs) where baseline nutritional and inflammatory disparities were eliminated (Supplemental Table S2), elevated TMAO (>278.74 μmol/L) remained a robust predictor of accelerated AVF failure (log-rank p = 0.025; Cox HR, 3.37; 95% CI, 1.08–10.45, p = 0.036; Supplemental Figure S4).
Discussion
This cohort study, involving 164 MHD patients, provides novel evidence establishing a direct link between serum TMAO levels and AVF dysfunction. Our findings demonstrate that elevated TMAO is an independent predictor of AVF failure. After adjusting for potential confounders, patients with baseline serum TMAO concentrations exceeding 278.74 μmol/L exhibited a more than two-fold increased risk of AVF dysfunction (HR, 2.07; 95% CI, 1.04–4.13; p = 0.035).
The primary pathological basis of AVF dysfunction involves a complex process of stochastic maladaptive vascular remodeling. While intimal hyperplasia characterized by the accumulation of smooth muscle cells and extracellular matrix does occur, recent clinical and histological studies demonstrate that intimal hyperplasia alone is not the primary determinant of AVF failure. Instead, failing AVFs are increasingly defined by a state of fibro-inflammatory remodeling and impaired outward venous adaptation where medial fibrosis, chronic inflammation, and biomechanical dysregulation synergistically restrict the venous outflow tract. 26 This maladaptive response is driven by both local and systemic factors.13,27 Locally, surgical trauma and regional hemodynamics trigger an inflammatory infiltrate of macrophages and lymphocytes that orchestrates a pro-fibrotic environment. Macrophage migration inhibitory factor activating signaling pathways such as p38 MAPK upregulates inflammatory cytokines including VEGF-A, IL-8, IL-1β, and MCP-1.28,29 Systemically, the accumulation of uremic toxins in ESRD patients fosters oxidative stress and chronic inflammation characterized by elevated levels of pro-inflammatory cytokines such as IL-6, TGF-β1, and TNF-α. 30 Concurrently, ESRD-related mineral and bone disorders can influence the vessel wall by modulating osteoclast activity and promoting adverse vascular stiffness and remodeling.31,32 These local and systemic mechanisms synergize through complex cytokine cascades to drive excessive extracellular matrix deposition and smooth muscle cell phenotypic switching, ultimately inducing negative venous remodeling and access dysfunction. 33
Notably, our study reveals a significant association between high serum TMAO levels and an increased risk of AVF dysfunction. The established pathogenic mechanisms of TMAO share considerable overlap with the core fibro-inflammatory processes of AVF failure described above. Previous research indicates that TMAO promotes vascular injury and thrombosis through multiple mechanisms that are highly relevant to vascular remodeling.34,35 First, TMAO triggers systemic oxidative stress and activates the NLRP3 inflammasome, leading to the release of pro-inflammatory cytokines such as IL-1β and IL-18, which exacerbate endothelial injury and perpetuate the inflammatory state of the venous wall.35–37 Furthermore, elevated TMAO levels activate the NF-κB pathway, inducing the overexpression of pro-inflammatory genes like cyclooxygenase-2, E-selectin, IL-6, and intercellular adhesion molecule-1, thus fueling the fibro-inflammatory cascade.38,39 Crucially, TMAO has been shown to drive profibrotic responses and excessive extracellular matrix deposition that lead to vascular stiffening,40,41 thereby impairing the vessel’s ability to undergo adaptive outward remodeling. Additionally, TMAO enhances platelet hyperreactivity and in vivo thrombosis potential by altering stimulus-dependent calcium signaling thereby increasing the risk of acute thrombotic events. 34 Therefore, we postulate that TMAO contributes to accelerated AVF failure by synergistically amplifying the pathological cascade of adverse vascular remodeling, stenosis, and thrombosis. It likely achieves this by intensifying inflammation, promoting oxidative stress, exacerbating medial fibrosis, and enhancing a prothrombotic milieu. Importantly, because baseline TMAO levels are ubiquitously elevated in the ESRD population due to impaired renal clearance, 14 our identified threshold (>278.74 μmol/L) likely represents a critical pathological inflection point. Beyond this level, TMAO-driven cascades transition into an overwhelmingly aggressive state, accelerating access failure even against the severe background of uremic toxicity. This multifaceted pathogenic role provides a compelling molecular basis to explain the heightened risk of access dysfunction observed in patients with extreme TMAO elevation.
In the present study, we also identified elevated serum type IV collagen as an independent risk factor for vascular access events (HR, 1.02; 95% CI, 1.00–1.04; p = 0.016). Type IV collagen is a major constituent of the basement membrane, typically existing as a stable triple-helix trimer composed of two α1 chains and one α2 chain. 42 As a critical component of the perivascular basement membrane, type IV collagen is not only involved in early vasculogenesis but also plays a vital role in maintaining the structural integrity of mature blood vessels. 43 Previous studies have reported substantial deposition of type IV collagen in advanced atherosclerotic plaques, suggesting its potential pro-atherogenic role. 44 Building upon these observations and our findings, we speculate that type IV collagen may also contribute to the pathogenesis of AVF dysfunction in MHD patients, although the specific underlying mechanisms require further investigation.
Additionally, from our baseline analysis, we found that compared to the low TMAO group, patients in the high TMAO group had a significantly lower BMI (19.40 [17.85, 21.30] vs 21.19 [19.54, 23.68] kg/m2, p = 0.001) and tended to have lower serum albumin levels, a trend that approached but did not reach statistical significance (38.20 [37.20, 39.70] vs 39.60 [37.65, 41.75] g/L, p = 0.056). This observation suggests that patients with elevated TMAO may be in a state of heightened catabolism or have a poorer nutritional status. This hypothesis is supported by previous research that has identified elevated serum TMAO as an independent risk factor for protein-energy wasting (PEW) in hemodialysis patients. Notably, a significant negative correlation between plasma TMAO and serum albumin levels has been reported in HD patients with PEW,15,45 a finding that aligns with the trend observed in our study. Crucially, our propensity score-matched sensitivity analysis demonstrated that the prognostic significance of elevated TMAO on AVF failure remained highly robust even after completely neutralizing these nutritional and inflammatory disparities. This epidemiological evidence strongly confirms that TMAO exerts an independent pathological risk contribution to access dysfunction, rather than merely acting as a passive bystander reflecting a baseline “sicker” patient phenotype.
The high incidence of vascular access failure remains a major clinical challenge in the MHD population. Our investigation provides a novel insight into the association between the gut microbiota metabolite TMAO and subsequent onset of AVF dysfunction. These findings have important clinical implications, highlighting a potential avenue for intervention. By identifying TMAO as a modifiable risk factor, our work paves the way for future studies to investigate TMAO-lowering strategies, such as dietary and microbiome-targeted therapies, for the potential prevention of vascular access events and provides a crucial basis for elucidating the possible underlying molecular mechanisms. 46
This study has several limitations. First, as a single-center study, the generalizability of our findings may be limited due to potential selection bias. Consequently, the specific prognostic threshold identified in our dataset requires further validation in external populations before broad clinical application. Furthermore, the small high-risk subgroup (n = 29) generated a wide confidence interval, necessitating larger cohorts to precisely estimate the risk magnitude. Second, this study is limited by its single baseline TMAO measurement and observational design, precluding the assessment of longitudinal dynamic changes and direct causality. Although current literature provides strong biological plausibility, future research incorporating repeated measurements and targeted in vivo/in vitro mechanistic models is required to definitively validate these findings. Third, the lack of histopathological specimens from the stenotic vascular access sites prevented us from directly elucidating the specific local mechanisms of TMAO in the pathogenesis of vascular lesions. Future studies should aim to validate our findings in better-designed, large-scale, multicenter cohorts, further elucidate the underlying pathogenic mechanisms, and ultimately evaluate TMAO-targeted therapies for the prevention of vascular access events.
Conclusion
In this single-center cohort of MHD patients, elevated baseline serum TMAO was identified as a robust, independent predictor of AVF dysfunction. Specifically, a TMAO level exceeding 278.74 μmol/L was associated with a significantly increased risk of accelerated vascular access failure, highlighting its potential as a novel associated risk factor for risk stratification.
Supplemental Material
sj-docx-1-jva-10.1177_11297298261461927 – Supplemental material for Elevated serum Trimethylamine-N-oxide predicts the risk of arteriovenous fistula dysfunction in patients on maintenance hemodialysis
Supplemental material, sj-docx-1-jva-10.1177_11297298261461927 for Elevated serum Trimethylamine-N-oxide predicts the risk of arteriovenous fistula dysfunction in patients on maintenance hemodialysis by Qiaozhi Gu, Yuan Ren, Xiaoye Zhu, Xiaowan Liang, Yuelin Zhang, Li You and Yuanhao Wu in The Journal of Vascular Access
Footnotes
Author contributions
YH.W. and L.Y. conceptualized and designed the study, provided supervision, and critically revised the manuscript. XY.Z., XW.L., and YL.Z. were responsible for patient enrollment, data acquisition, and sample collection. QZ.G. and Y.R. performed the statistical analysis, interpreted the data, and drafted the original manuscript. All authors have read and approved the final manuscript for submission.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.*
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study protocol was in accordance with the ethical principles of the Declaration of Helsinki and was approved by the Institutional Ethics Review Board of Huashan Hospital, Fudan University (No. KY2024-1355).
Consent to participate
Written informed consent was obtained from all participants prior to their inclusion in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.