
Abstract
Background:
Juxta-anastomotic stenosis is a major cause of arteriovenous fistula (AVF) dysfunction. Although drug-coated balloons (DCB) have demonstrated clinical benefit, the associated morphological changes compared with plain old balloon angioplasty (POBA) remain poorly defined. This study aimed to characterize vascular remodeling patterns after DCB and POBA using ultrasonographic cross-sectional area (CSA) analysis.
Methods:
In 41 patients with juxta-anastomotic AVF stenosis, all initially underwent POBA and subsequently DCB for recurrent stenosis. Luminal cross-sectional area (L‑CSA), external vessel cross-sectional area (E‑CSA), and vessel wall area (VWA) were assessed pre-treatment, post-treatment, and at 3 months. Longitudinal mixed-effects and baseline-adjusted models evaluated remodeling patterns and independent treatment effects. Exploratory intima–media thickness (IMT) analysis was performed.
Results:
Median target lesion primary patency (TLPP) was longer after DCB than POBA (10.8 vs 3.3 months). At 3 months, L‑CSA and E‑CSA were significantly larger after DCB, whereas VWA did not differ between treatments. Longitudinal mixed-effects models showed significant treatment-by-time interactions for L‑CSA and E‑CSA, with progressive luminal narrowing and external vessel shrinkage after POBA that were attenuated after DCB, while VWA increased similarly in both groups. Baseline-adjusted models confirmed that DCB was independently associated with larger 3-month L‑CSA and E‑CSA suggesting that the patency benefit observed after DCB was associated with preservation of external vessel dimensions rather than suppression of wall thickening. Exploratory analyses further showed that, despite similar changes in IMT area, IMT thickness increased more slowly after DCB, suggesting a possible contribution to sustained E‑CSA preservation.
Conclusion:
DCB provided improved clinical outcomes in juxta-anastomotic stenosis. These findings suggest that improved outcomes after DCB may be associated with preservation of external vessel architecture and mitigation of constrictive remodeling, potentially supported by IMT suppression, rather than a predominant inhibitory effect on wall thickening. This suggests a site-specific mechanism of DCB action in the hemodynamically stressed juxta-anastomotic segment.
Keywords
Introduction
Stenosis of arteriovenous fistulas (AVFs) is a leading cause of vascular access dysfunction in hemodialysis patients, and percutaneous transluminal angioplasty (PTA) is widely used as the standard treatment. Nevertheless, restenosis after PTA remains common, with some studies reporting target lesion primary patency (TLPP) rates at 6 months of approximately 50%–60%.1,2
Although PTA temporarily restores luminal patency through mechanical dilation, vascular smooth muscle cell proliferation and adventitial remodeling frequently occur soon after the procedure, leading to recurrent stenosis. To address this limitation, drug-coated balloons have recently been introduced, delivering antiproliferative agents—primarily paclitaxel—locally to the vessel wall. Several clinical trials have demonstrated that DCBs significantly improve TLPP compared with conventional PTA, thereby supporting their clinical efficacy.3,4
Previous work has shown that repeated DCB treatment is associated with sustained long-term patency. In addition, ultrasonographic analyses have demonstrated preservation of external vessel diameter, suggesting that DCB may attenuate constrictive remodeling in addition to suppressing luminal narrowing. 5 Building on these observations, the present study sought to explore longitudinal changes in vascular morphology following POBA and DCB treatment using serial ultrasonography, focusing on both luminal and external vessel dimensions. Furthermore, another investigation from our group showed that DCB treatment achieved particularly favorable patency outcomes when applied to juxta-anastomotic stenosis compared with more distal venous lesions. 6 The juxta-anastomotic region is characterized by a unique hemodynamic environment involving complex flow interaction and turbulence, suggesting that the interaction between drug effects and local hemodynamic stress may contribute to vascular remodeling stability. 7
However, few studies have quantitatively evaluated how DCBs influence vascular wall structure and cross-sectional morphology—specifically the lumen, intima–media, and adventitia—in juxta-anastomotic stenosis. In particular, direct morphological comparisons between DCB and plain old balloon angioplasty (POBA) remain limited. In this study, POBA was defined as angioplasty using non-drug-coated balloons, including standard, cutting, and scoring balloons.
Therefore, the present study aimed to compare vascular cross-sectional morphology following POBA and DCB within the same patients using ultrasonographic cross-sectional area (CSA) analysis, to elucidate how DCB contributes to vascular structural preservation in juxta-anastomotic stenosis.
Methods
Study population
This study was a retrospective paired analysis comparing data obtained after POBA and subsequent DCB treatment, which were performed sequentially for the same juxta-anastomotic lesion within the same patient. A juxta-anastomotic lesion was defined as a stenotic segment in which of maximum stenosis (the narrowest point identified by ultrasonography) was located within 4 cm of the arteriovenous anastomosis. All DCB procedures were performed using the IN.PACT AV Drug-Coated Balloon (Medtronic, Dublin, Ireland). The study period spanned from April 2021 to June 2025 and included patients who underwent endovascular treatment for AVF stenosis at our institution. The interval between the index POBA and the subsequent DCB procedure was defined as the period from the date of POBA to the date of DCB intervention for recurrent stenosis. This interval effectively represented as the TLPP of the initial POBA treatment.
The study was conducted using fully anonymized retrospective data. The institutional ethics committee approved the study protocol (approval No. 25102) and determined that formal written informed consent could be waived due to the retrospective and non-interventional nature of the study. The study complied with the principles of the Declaration of Helsinki, and informed consent was obtained via an opt-out procedure.
Patient selection
All AVF stenoses were evaluated using ultrasonography. Among cases with stenosis, DCB treatment was performed in patients who met our institutional criteria for DCB therapy: those undergoing maintenance hemodialysis, aged 18 years or older, without planned kidney transplantation within 2 years, and without central venous lesions. Cases with central venous lesions, artificial vascular graft (AVGs) thrombotic occlusion, and those with associated access infections were excluded based on clinical indications.
A total of 274 initial DCB procedures performed at our institution were screened. Of these, 186 procedures were excluded due to non–juxta-anastomotic stenosis, leaving 88 procedures with confirmed juxta-anastomotic lesions.
Further exclusions were applied to ensure the availability of paired ultrasonographic evaluations at 90 ± 15 days after both POBA and DCB. Specifically, procedures were excluded if (1) DCB was performed before the scheduled ultrasonographic follow-up after POBA, thereby precluding paired evaluation (n = 13); (2) ultrasonographic data within 90 ± 15 days after DCB were unavailable (n = 18); or (3) ultrasonographic data within 90 ± 15 days after POBA were unavailable (n = 16). Consequently, a final total of 41 patients (providing 41 paired datasets of POBA and DCB) met all inclusion criteria and were included in the final analysis (Figure 1).
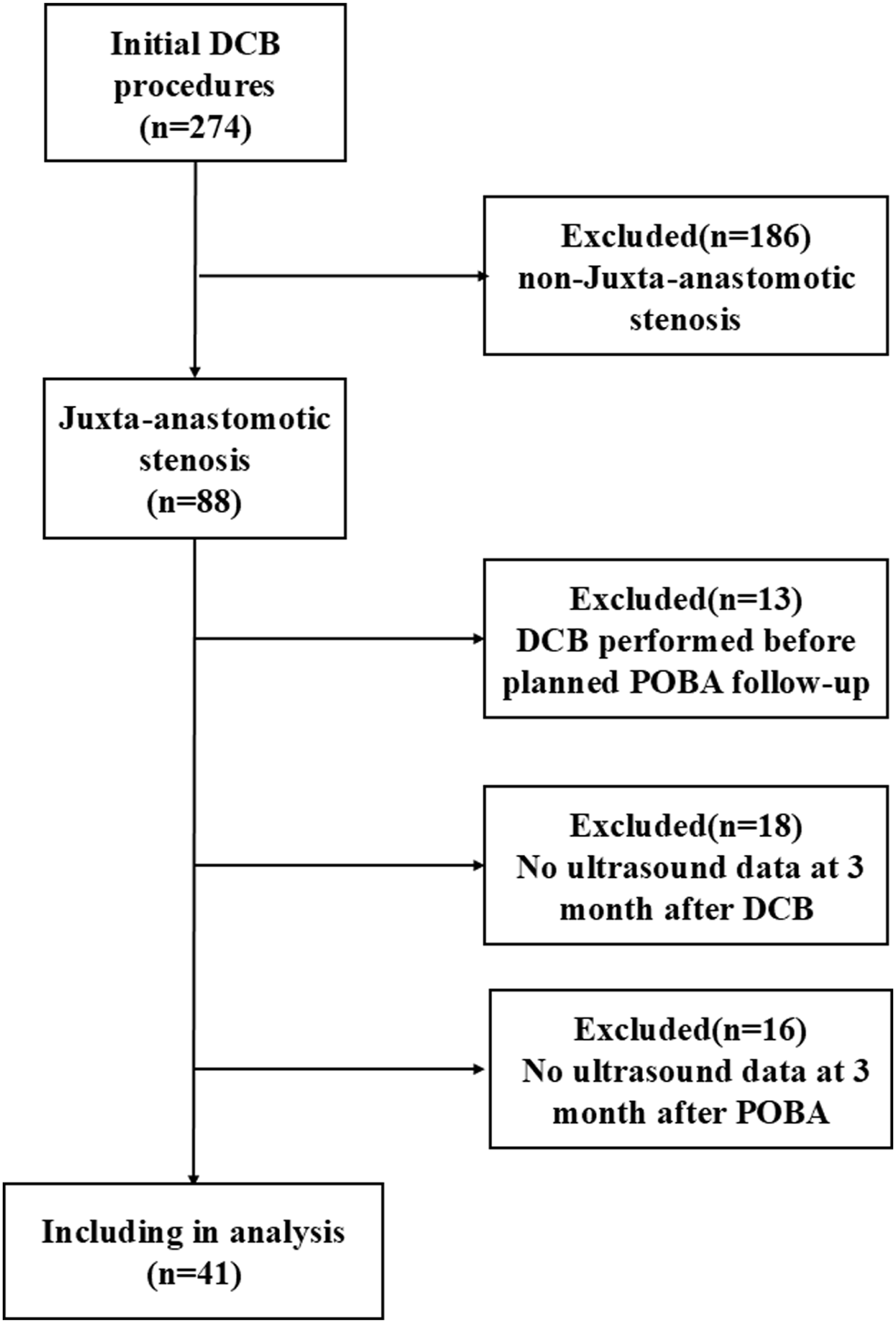
Flowchart of patient selection and study design.
Clinical data and endpoints
Clinical and procedural data were extracted from electronic medical records, including sex, age, dialysis vintage, diabetes mellitus status, use of antiplatelet agents, number of prior POBA procedures, balloon diameter, and dates of ultrasonographic follow-up (90 ± 15 days after POBA and DCB). Flow volume in the brachial artery was measured at 3 months after the intervention using duplex ultrasound in the resting state on a non-dialysis day and expressed in mL/min. Both POBA and DCB procedures were performed under ultrasound guidance following a standardized protocol.
The primary objective of this study was to assess vascular remodeling at 3 months using vascular cross-sectional area (CSA) as the outcome measure. To account for the sequential study design, we primarily focused on the independent effect of each treatment (POBA vs DCB) on these structural parameters. Secondary outcomes included brachial artery flow volume and the clinical TLPP for each treatment session.
Ultrasound evaluation and measurement
Vascular measurements were performed using an Aplio i700 and Aplio 300 ultrasound system (Canon Medical Systems Corporation, Tochigi, Japan) equipped with linear high-frequency probes (21–24 MHz or 14–18 MHz).
All examinations were conducted under standardized conditions immediately before, immediately after, and 3 months (90 ± 15 days) after each procedure using a high-resolution vascular access ultrasound protocol.
All examinations were performed by two experienced sonographers and three certified dialysis access nurses. After confirming that the vessel was nearly circular in the short-axis view, high-resolution long-axis images were captured and stored for subsequent offline analysis. All measurements were performed with patients in the supine position, and no tourniquet was applied during image acquisition to maintain consistent vascular filling conditions.
To ensure objectivity, all stored images were retrospectively analyzed by the authors using POP Net Viewer (Image ONE Co., Ltd., Tokyo). This approach allowed for precise measurement of the luminal and external vessel diameters on static images, independent of the initial real-time assessment. Each vascular parameter was measured three times at the same anatomical site using images acquired from the same cross-sectional plane. The measurements were performed at different time points during offline analysis, and the mean value was used for statistical analysis to improve measurement reproducibility.
For each stenotic segment, CSAs were calculated using the following formulas (Figure 2):
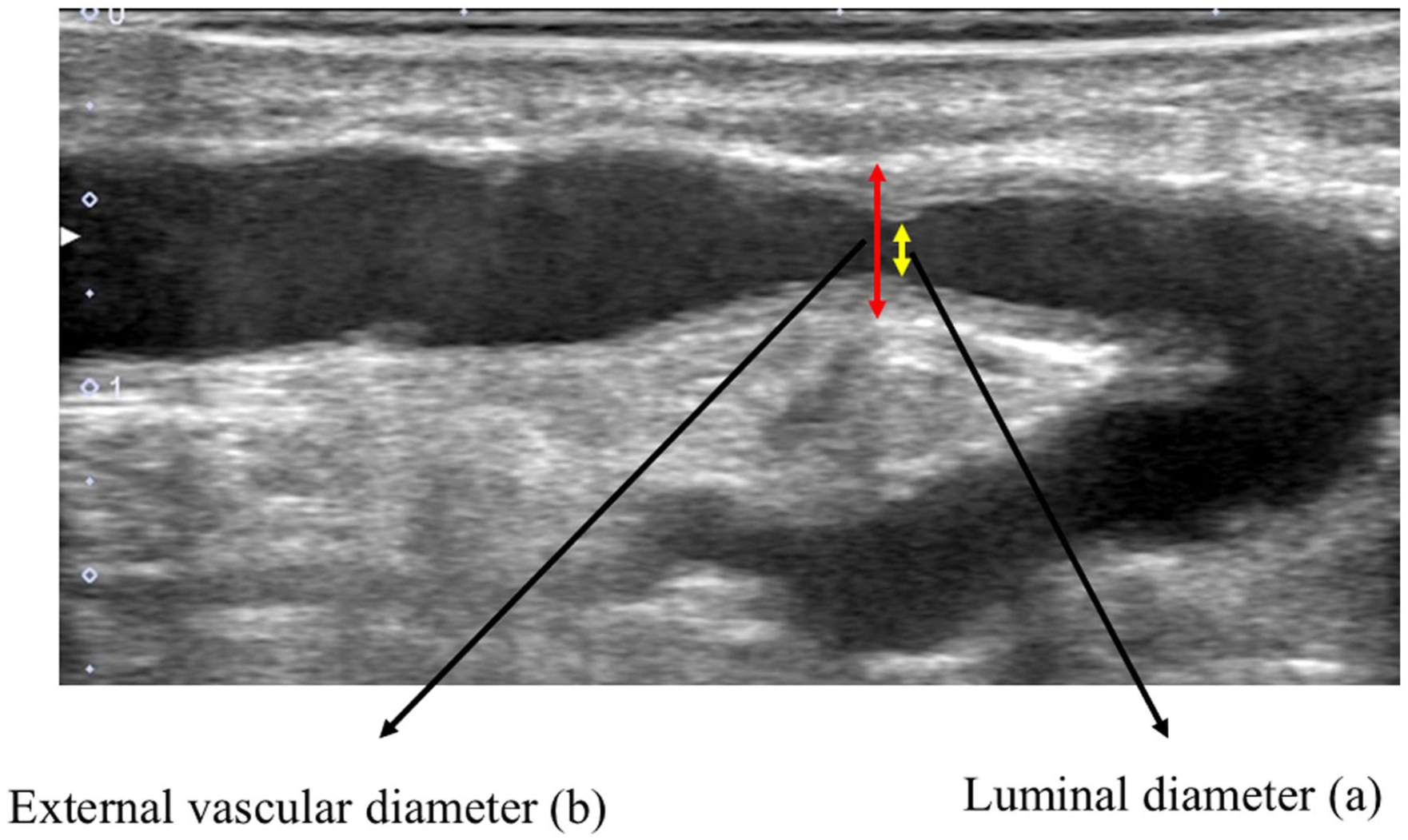
Ultrasound-based cross-sectional area measurements of vessel segments.
Due to the limitations of ultrasonic resolution, the interface between the media and adventitia is identified as the outermost edge of the adventitia. Consequently, in cases where the intima-media complex could not be clearly distinguished as a separate entity, we defined the entire area within this boundary as External CSA (E‑CSA). Based on this, the vessel wall area (VWA) was calculated to represent the total area of the vascular wall structure.



Intima–media thickness (IMT) was measured on the same longitudinal images used for CSA analysis and calculated as the difference between the external and luminal vessel diameters. In this study, IMT included as an exploratory parameter in the linear mixed-effects model (LMM) analysis.
For lesions involving long segment or multiple stenoses within the juxta anastomotic region, a predefined target lesion was selected for analysis. The target lesion was defined as the segment with the smallest luminal diameter identified on longitudinal ultrasound imaging. In cases with multiple stenotic segments, measurements were consistently performed at the most severely narrowed site.
A juxta-anastomotic lesion was defined as a stenotic segment in which the point of maximum narrowing was located within 4 cm of the arteriovenous anastomosis. This boundary was selected because hemodynamic disturbances, including elevated shear stress and flow turbulence, are most prominent within this region based on prior computational fluid dynamics assessments.
During subsequent DCB sessions, the same predefined strategy was applied, selecting the segment with the smallest luminal diameter within the juxta anastomotic region at each time point. Although the exact anatomical location may not have been identical between POBA and DCB sessions, this standardized approach ensured consistent evaluation of the most hemodynamically significant lesion.
E‑CSA was calculated from the outer vessel boundary, VWA as the difference between E‑CSA and L‑CSA, and IMT as the mean thickness of the intima media complex measured at the target lesion. All measurements were performed by two independent sonographers blinded to treatment assignment, and inter-observer reproducibility was assessed using intraclass correlation coefficients.
Balloon angioplasty procedure
All lesions were treated according to a standardized angioplasty protocol. Lesion preparation was performed using high pressure balloons before DCB delivery. Balloon type (high-pressure, scoring, or ultrahigh-pressure) was selected at the operator’s discretion based on lesion morphology.
During initial POBA, balloon size was determined according to the reference vessel diameter, and inflation pressure and duration were adjusted to achieve adequate luminal expansion. Before DCB delivery, additional lesion preparation (pre-DCB dilation) was routinely performed using high pressure or ultra-high-pressure balloons to optimize luminal gain and drug uptake.
Inflation pressures typically ranged from 18 to 26 atm, and inflation duration from 75 to 180 s. Residual stenosis was assessed by ultrasound immediately after dilation, and procedural success was defined as residual stenosis <30%.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate. Paired comparisons between POBA and DCB were conducted using the paired t-test or Wilcoxon signed-rank test, depending on data distribution. Categorical variables were reported as counts and percentages.
TLPP after POBA and DCB was estimated using the Kaplan–Meier method. For the POBA group, the interval was defined as the time from the index POBA to the subsequent DCB procedure for restenosis. To evaluate potential bias related to the sequential design, baseline vascular parameters (L‑CSA, E‑CSA, and VWA) were compared between the POBA and DCB sessions to confirm comparable pre-treatment conditions.
Longitudinal morphological changes were analyzed using LMMs fitted separately for L‑CSA, E‑CSA, VWA, and IMT. Patient-specific random intercepts were included to account for within-subject correlation. Fixed effects consisted of time, treatment type (POBA vs DCB), and their interaction to assess differences in temporal trajectories between treatments.
To evaluate treatment effects on 3-month remodeling while adjusting for acute procedural gain, post-procedural baseline-adjusted linear models were additionally fitted using the 3-month value of each parameter as the dependent variable and the corresponding immediate post-procedural value as a covariate. This approach is equivalent to an analysis of covariance (ANCOVA) and provides an estimate of treatment effect while accounting for baseline imbalance.
Time-invariant patient characteristics (e.g. age, diabetes) were not included as fixed effects because they were inherently controlled for by the within-patient design. Because this study employed a sequential treatment design, inter-patient variability was eliminated, to evaluate treatment-associated differences of POBA and DCB on vascular structural parameters.
Regression coefficients (β) are presented with 95% confidence intervals. A two-sided p value < 0.05 was considered statistically significant. All statistical analyses were performed using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
To maintain consistency in cross-sectional comparisons, IMT was not included in the analyses of L-CSA, E-CSA, VWA, or in the baseline-adjusted models for 3-month outcomes, all of which were evaluated using area-based parameters. However, IMT was incorporated exclusively into the longitudinal mixed-effects models because the thickness of the intima–media layer, rather than its cross-sectional area, was considered a physiologically relevant determinant of temporal changes in E-CSA.
To comprehensively evaluate vascular remodeling, two complementary analytical approaches were applied: longitudinal mixed-effects models to characterize treatment-by-time trajectories, and baseline-adjusted linear models to estimate treatment effects on 3‑month outcomes.
Results
Baseline patient and procedural characteristics
Because comparisons between POBA and DCB were based on paired within-patient analyses (n = 41), clinical characteristics—including diabetes mellitus status, use of antiplatelet agents, sex, age, dialysis vintage, and the number of previous POBA procedures—were identical between groups owing to the paired within-patient design owing to the paired within-patient design. There were no missing data for any of the baseline or follow-up variables.
Diabetes mellitus was present in 20 patients (48.8%), 14 patients (34.1%) were receiving antiplatelet therapy, and 10 patients (24.4%) were female. The mean age was 73.7 ± 9.9 years, the median duration of dialysis was 6.6 years (interquartile range (IQR), 2.4–9.7 years), and the median number of prior POBA sessions was 6 (IQR, 2–10). Antiplatelet therapy status was recorded for all patients, and no changes were made immediately following the intervention; patients continued their pre-existing regimen without initiation or discontinuation of therapy.
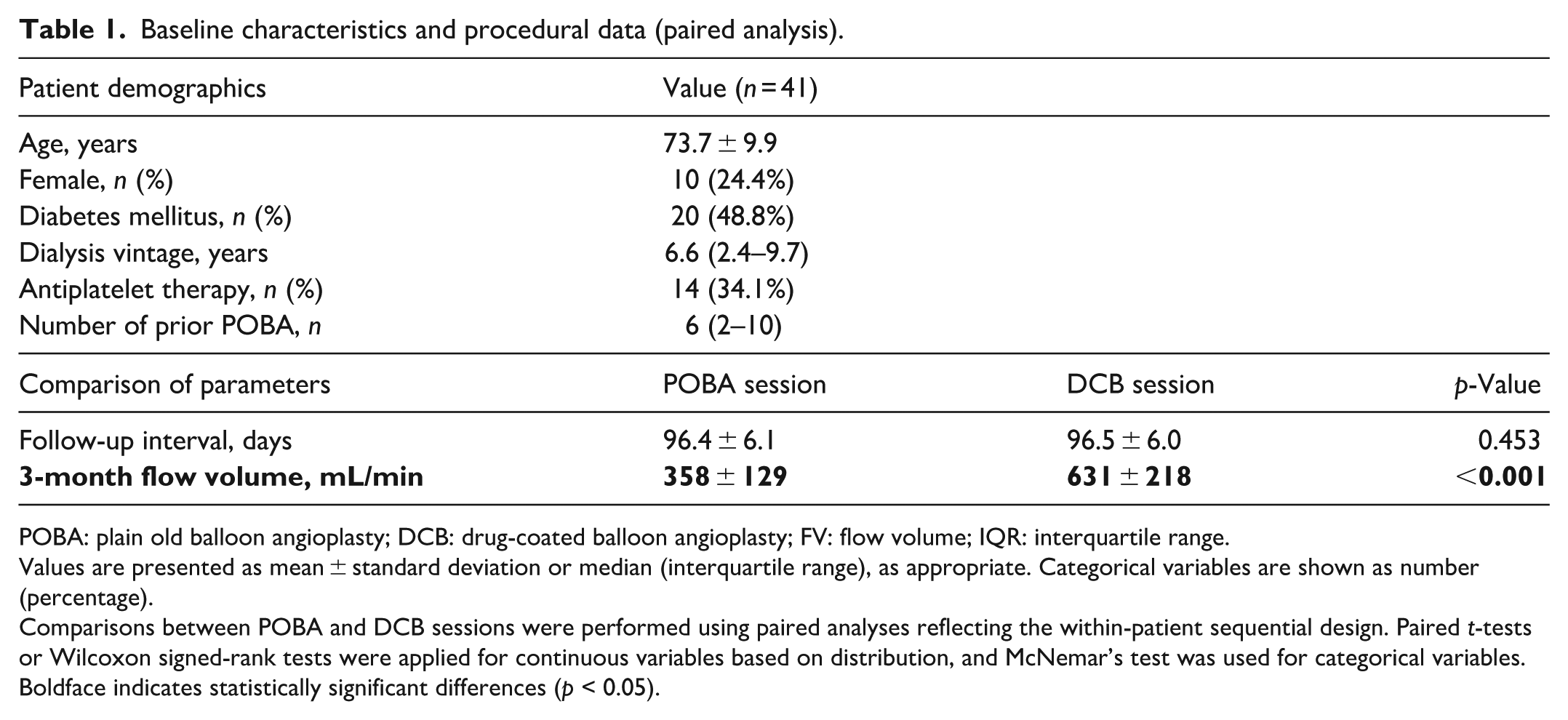
The interval between the intervention (POBA or DCB) and the 3-month follow-up measurement was also comparable (POBA: 96.4 ± 6.1 days; DCB: 96.5 ± 6.0 days; p = 0.453; Table 1).
Baseline characteristics and procedural data (paired analysis).
POBA: plain old balloon angioplasty; DCB: drug-coated balloon angioplasty; FV: flow volume; IQR: interquartile range.
Values are presented as mean ± standard deviation or median (interquartile range), as appropriate. Categorical variables are shown as number (percentage).
Comparisons between POBA and DCB sessions were performed using paired analyses reflecting the within-patient sequential design. Paired t-tests or Wilcoxon signed-rank tests were applied for continuous variables based on distribution, and McNemar’s test was used for categorical variables.
Boldface indicates statistically significant differences (p < 0.05).
Balloon procedural characteristics
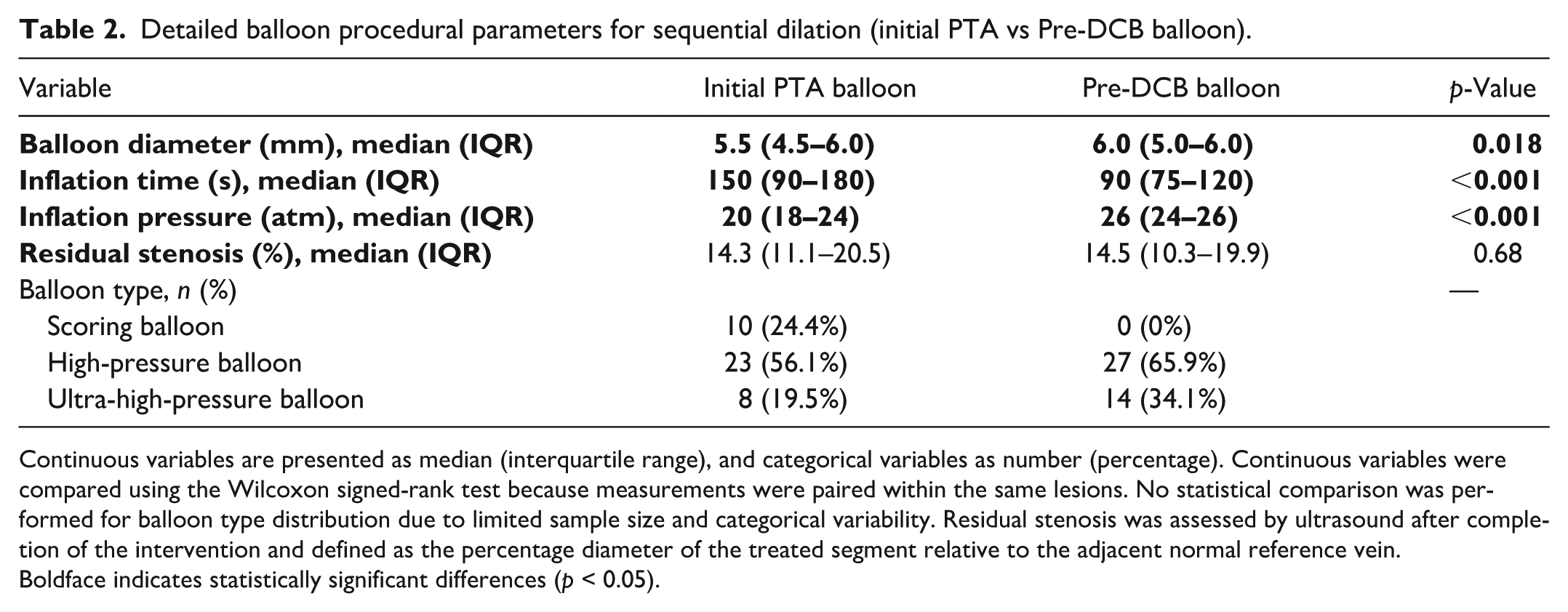
Among the 41 lesions treated with sequential dilation, the pre-DCB balloon diameter was significantly larger than the initial PTA balloon (6.0 (5.0–6.0) mm vs 5.5 (4.5–6.0) mm, p = 0.018). Pre-DCB inflation time was shorter (90 (75–120) sec vs 150 (90–180) sec, p < 0.001), whereas inflation pressure was higher (26 (24–26) atm vs 20 (18–24) atm, p < 0.001).
Residual stenosis after the procedure did not differ between POBA and DCB sessions (14.3 (11.1–20.5) % vs 14.5 (10.3–19.9) %, p = 0.68). Scoring balloons were used in 24.4% of initial POBA procedures but not during pre-DCB dilation, whereas high- pressure and ultra-high-pressure balloons were more frequently used before DCB delivery (Table 2).
Detailed balloon procedural parameters for sequential dilation (initial PTA vs Pre-DCB balloon).
Continuous variables are presented as median (interquartile range), and categorical variables as number (percentage). Continuous variables were compared using the Wilcoxon signed-rank test because measurements were paired within the same lesions. No statistical comparison was performed for balloon type distribution due to limited sample size and categorical variability. Residual stenosis was assessed by ultrasound after completion of the intervention and defined as the percentage diameter of the treated segment relative to the adjacent normal reference vein.
Boldface indicates statistically significant differences (p < 0.05).
Clinical outcomes
The clinical TLPP after POBA—representing the interval until the subsequent DCB intervention—was a median of 3.27 months (95% CI: 3.21–3.33). Following the subsequent DCB treatment, the median TLPP was markedly prolonged at 10.80 months (95% CI: 8.17–13.43). Due to the sequential and non-independent nature of the study design, these data are presented descriptively. Nonetheless, this substantial clinical improvement after switching to DCB provided the rationale for exploring the underlying vascular remodeling changes.
Comparison of cross-sectional areas and vessel wall area
Comparisons of vascular cross-sectional parameters (L-CSA, E-CSA, and VWA) between POBA and DCB are summarized in Table 3.
Comparison of vascular cross-sectional areas between POBA and DCB at each time point (paired analysis).
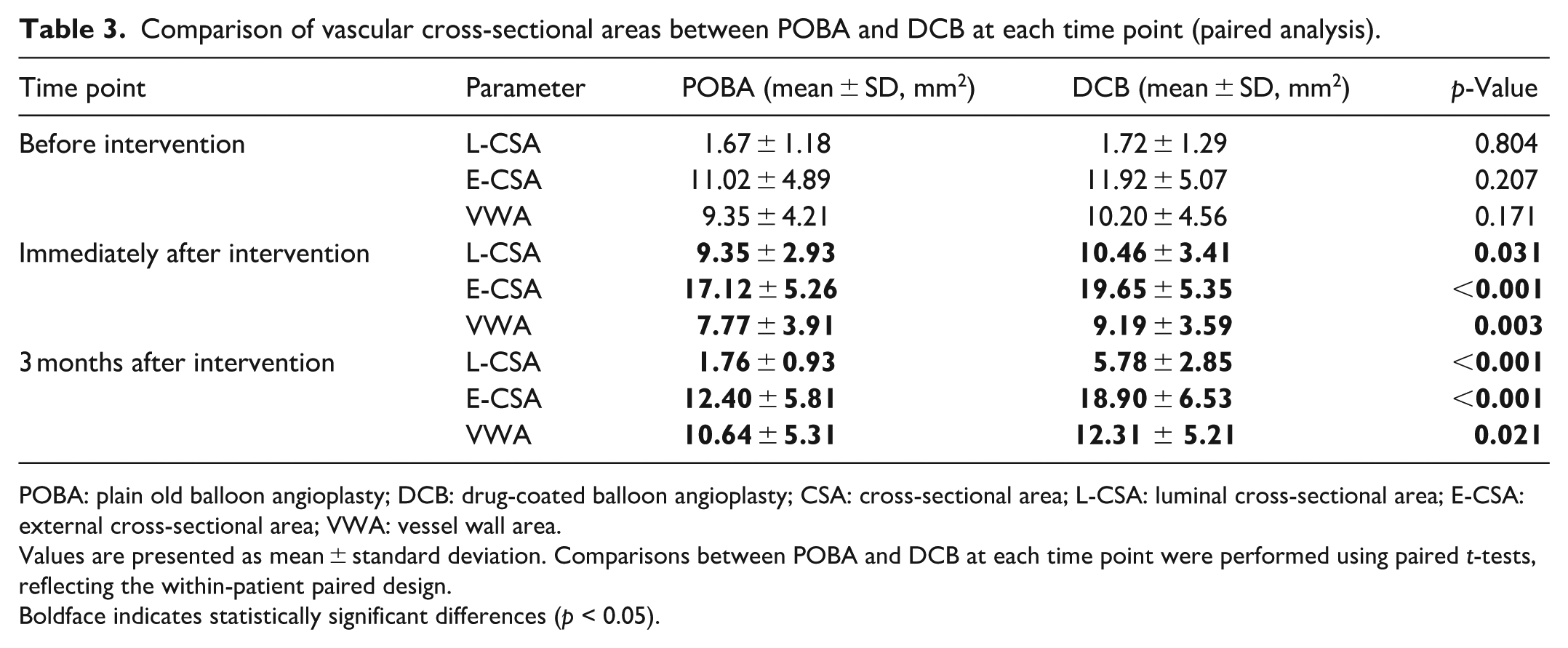
POBA: plain old balloon angioplasty; DCB: drug-coated balloon angioplasty; CSA: cross-sectional area; L-CSA: luminal cross-sectional area; E-CSA: external cross-sectional area; VWA: vessel wall area.
Values are presented as mean ± standard deviation. Comparisons between POBA and DCB at each time point were performed using paired t-tests, reflecting the within-patient paired design.
Boldface indicates statistically significant differences (p < 0.05).
At baseline (pre-treatment), no significant differences were observed between groups in L-CSA, E-CSA, or VWA (all p > 0.05). Immediately post-treatment, the DCB group demonstrated significantly larger L-CSA and E-CSA compared with POBA (p = 0.031 and p < 0.001, respectively), and VWA was also significantly greater (p = 0.003). These differences persisted at 3 months, with the DCB group maintaining significantly larger L-CSA and E-CSA (both p < 0.001) and a higher VWA (p = 0.021).
In addition, brachial artery flow volume at 3 months was significantly higher in the DCB group than in the POBA group (631 ± 218 vs 358 ± 129 mL/min, p < 0.001).
Morphological comparisons at 3‑month follow-up
Individual paired comparisons of vascular morphology at 3 months are presented in Figure 3.
(a)
(b)
(c)
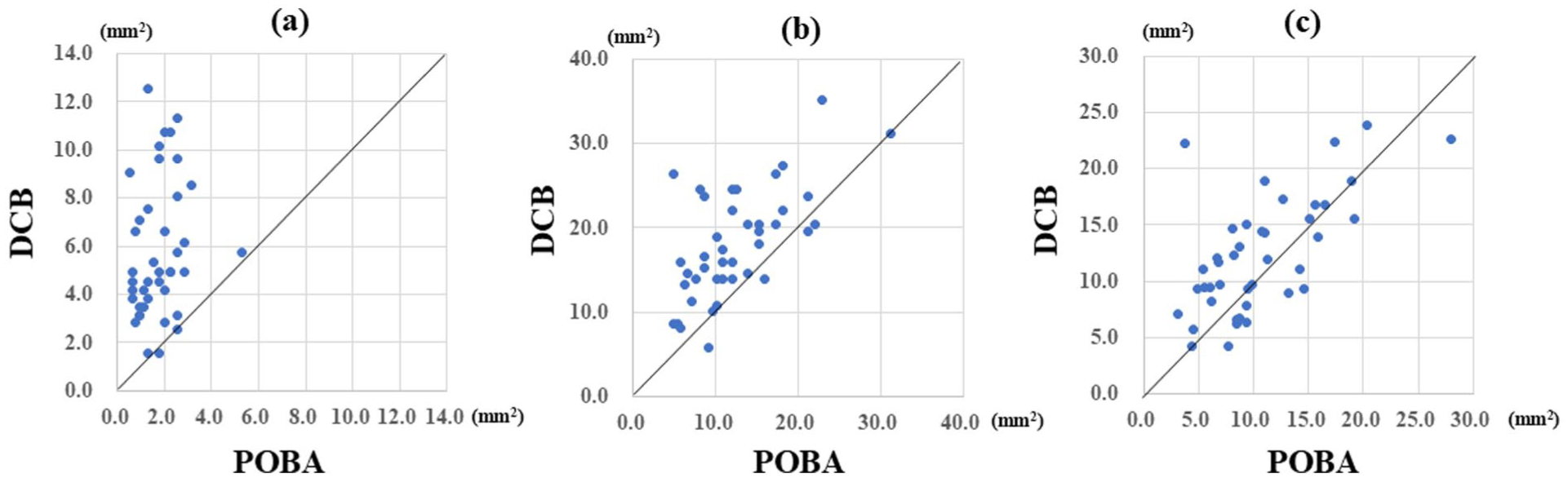
Individual comparisons of vascular morphology at 3 months: POBA versus DCB (n = 41). Individual paired comparisons are shown for (a) luminal cross-sectional area (L-CSA), (b) external crosssectional area (E-CSA), (c) vessel wall area (VWA), between the POBA session and the subsequent DCB session at the 3-month follow-up.
Together, these paired comparisons highlight distinct geometric patterns between treatments at 3 months.
Longitudinal analysis using linear mixed-effects models
To evaluate temporal changes in vascular morphology, linear mixed-effects models with patient-specific random intercepts were fitted for L-CSA, E-CSA, VWA, and IMT across all measurement points.
Luminal‑CSA (L-CSA)
A significant treatment-by-time interaction was observed (β = 0.032, p < 0.001). L-CSA declined progressively after POBA (β = −0.084, p < 0.001), whereas this reduction was markedly attenuated after DCB, indicating sustained luminal preservation.
External‑CSA (E-CSA)
E-CSA also showed a significant interaction (β = 0.035, p = 0.007). POBA produced a significant decrease over time (β = −0.053, p < 0.001), while the decline was mitigated after DCB, consistent with persistent outward remodeling.
Vessel wall area (VWA)
VWA showed no significant interaction (β = 0.003, p = 0.786), indicating similar thickening rates between groups. Overall, VWA increased over time (β = 0.032, p < 0.001), independent of treatment type.
Intima–media thickness (IMT)
IMT demonstrated a significant treatment-by-time interaction (β = 0.0050 mm/day, p = 0.00052), with faster thickening after POBA and attenuation after DCB.
Figure 4 illustrates individual patient data and LMM-derived regression lines, highlighting divergent remodeling in L-CSA and E-CSA, comparable VWA progression, and treatment-dependent IMT behavior. LMMs characterized temporal remodeling, whereas baseline-adjusted models assessed independent treatment effects at 3 months.
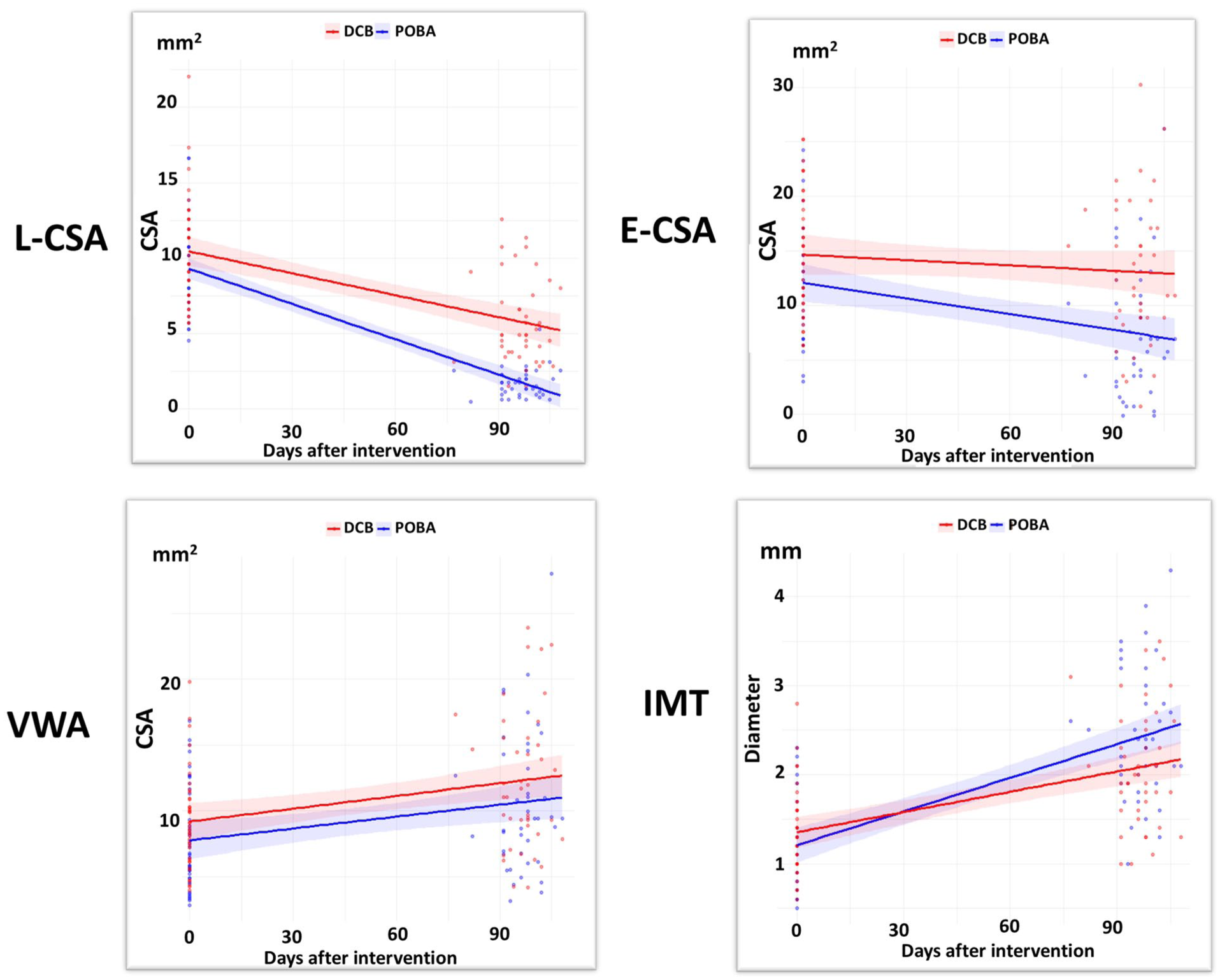
Longitudinal changes in luminal CSA (L CSA), external CSA (E CSA), vessel wall area (VWA), and intima–media thickness (IMT) by treatment group.
Baseline-adjusted linear models for 3‑month outcomes
Baseline-adjusted linear models were fitted using the 3-month value of each vascular parameter as the dependent variable and the corresponding immediate post-treatment value as a covariate (Table 4).
Baseline-adjusted treatment effects on vascular morphology at 3 months.
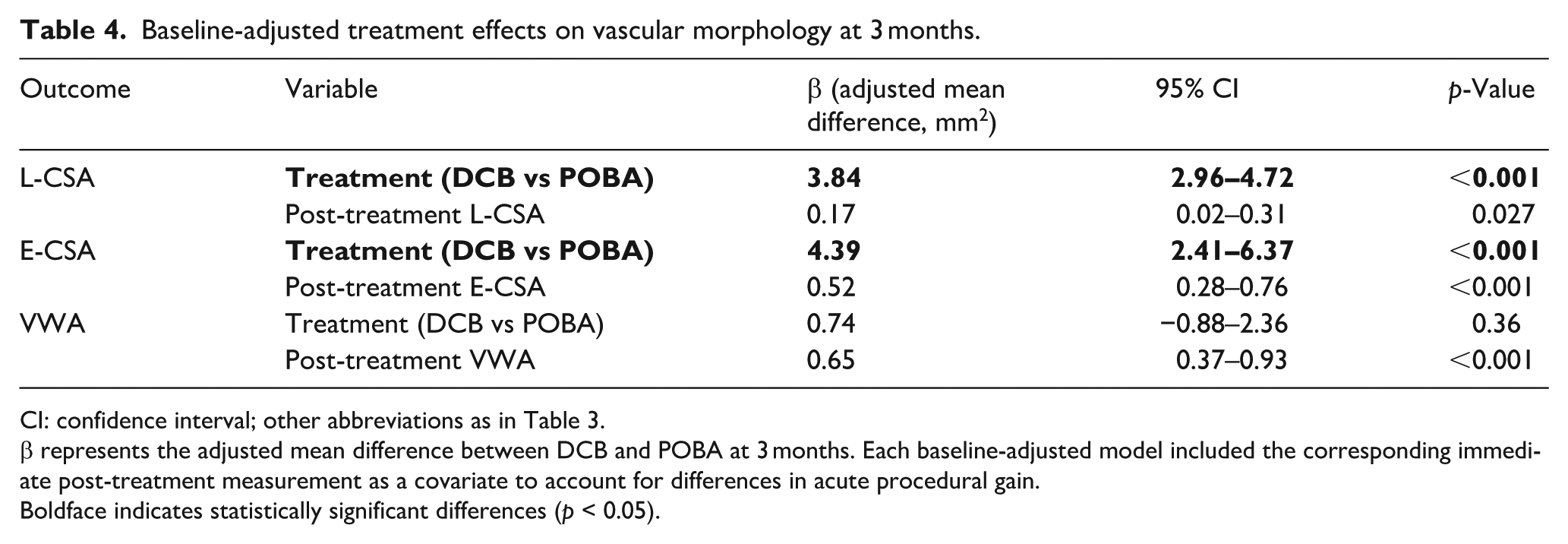
CI: confidence interval; other abbreviations as in Table 3.
β represents the adjusted mean difference between DCB and POBA at 3 months. Each baseline-adjusted model included the corresponding immediate post-treatment measurement as a covariate to account for differences in acute procedural gain.
Boldface indicates statistically significant differences (p < 0.05).
Luminal‑CSA (L-CSA)
DCB treatment was independently associated with a larger L-CSA at 3 months (β = 3.84 mm2, 95% CI 2.96–4.72, p < 0.001). Immediate post-treatment L-CSA also predicted the 3-month value (β = 0.17, p = 0.027).
External‑CSA (E-CSA)
DCB treatment similarly resulted in a larger 3-month E-CSA (β = 4.39 mm2, 95% CI 2.41–6.37, p < 0.001), and post-treatment E-CSA remained strongly associated with the 3-month measurement (β = 0.52, p < 0.001).
Vessel wall area (VWA)
The adjusted treatment effect on VWA was not significant (β = 0.74 mm2, p = 0.36), although post-treatment VWA was a significant predictor of the 3-month value (β = 0.65, p < 0.001).
Overall, these findings indicate that the superior luminal preservation after DCB treatment is driven mainly by preservation of external vessel expansion rather than reduced wall thickening.
Discussion
This study is the first to directly compare post-interventional morphological changes after POBA and DCB treatment in juxta-anastomotic AVF lesions within the same patients using ultrasonographic cross sectional area analysis. By employing a paired sequential design, we were able to isolate the treatment-specific contribution of paclitaxel-coated balloon therapy to vascular remodeling and provide morphological insights that complement previously reported clinical patency outcomes.
Our findings suggest that DCB may exert broader vascular remodeling effects beyond simple suppression of neointimal proliferation, potentially contributing to sustained outward remodeling and preservation of vessel geometry.
DCB promotes sustained outward remodeling
DCB-treated lesions demonstrated greater initial expansion and sustained enlargement over time, suggesting attenuation of post-procedural constrictive remodeling that persists beyond the acute procedural effect. Lesions treated with DCB demonstrated significantly greater and more durable enlargement of both luminal‑CSA (L‑CSA) and external‑CSA (E‑CSA) at 3 months, consistent with the prolonged TLPP observed clinically. The accompanying increase in brachial artery flow volume suggests that this morphological expansion translated into meaningful functional improvement. Importantly, differences in CSA remained significant even after adjustment for immediate post-procedural vessel size using baseline-adjusted linear models, indicating that the long-term morphological differences cannot be explained solely by greater acute expansion, and may reflect attenuation of post-procedural constrictive remodeling.
Hemodynamic characteristics of the juxta anastomotic region
The juxta-anastomotic segment is exposed to a mechanically hostile hemodynamic environment characterized by turbulent flow, complex secondary flow patterns, and oscillatory shear stress. Recent ultrasound vector flow imaging studies have demonstrated pronounced flow recirculation and elevated oscillatory shear index in this region, conditions closely associated with adverse vascular remodeling—particularly inward (constrictive) remodeling that contributes to progressive luminal narrowing. 8 In this context, the significant enlargement of E‑CSA observed after DCB treatment suggests that the vessel wall underwent outward redistribution despite these unfavorable mechanical forces.
Interpretation of VWA: Acute procedural effects and structural stability
Unadjusted 3-month measurements showed a larger vessel wall area (VWA) in the DCB group; however, adjusted analyses accounting for immediate post-procedural values revealed no independent effect of DCB on VWA. Paclitaxel is known to inhibit abnormal smooth muscle cell contraction and proliferation. In addition, it modulates inflammatory responses and remodeling processes across multiple vascular layers.8,9 The absence of long-term VWA enlargement in the present study is consistent with these pharmacological effects.
Conversely, the observation that E-CSA increased significantly without a corresponding change in VWA suggests that DCB may preserve the expanded vessel caliber without evidence of structural destabilization of the vessel wall. From the perspective of Laplace’s law, this geometric configuration would be expected to reduce wall stress and thereby facilitate outward remodeling in the high-flow AVF environment. However, this mechanistic interpretation remains speculative and requires further dedicated biomechanical investigation.10,11
However, VWA alone does not fully capture potential changes in the structural configuration of the vessel wall. Additional structural insights were obtained from the supplementary analysis of IMT. To further contextualize this finding of unchanged VWA, we performed an additional analysis focusing on IMT.
IMT increased more prominently in the POBA group, whereas this progression was attenuated after DCB treatment. In the juxta-anastomotic region—where high flow and complex shear patterns impose substantial outward mechanical forces—a thinner intima–media layer may allow potentially more effective transmission of these forces to the vessel wall. This configuration could help maintain an enlarged E-CSA and L-CSA after DCB treatment, thereby supporting sustained outward remodeling. Although exploratory, this hemodynamically coherent mechanism provides a plausible link between IMT suppression and the preserved vessel caliber.
The E‑CSA-based findings are visually summarized in Figure 5. As illustrated in Figure 5, POBA was associated with progressive reduction of both luminal and external vessel diameters accompanied by vessel wall thickening. In contrast, after DCB treatment the external vessel diameter was largely preserved, resulting in maintenance of luminal caliber despite ongoing vessel wall remodeling. This geometric pattern is consistent with the‑CSA-based analyses and supports the concept that DCB promotes sustained outward remodeling rather than merely suppressing neointimal proliferation.
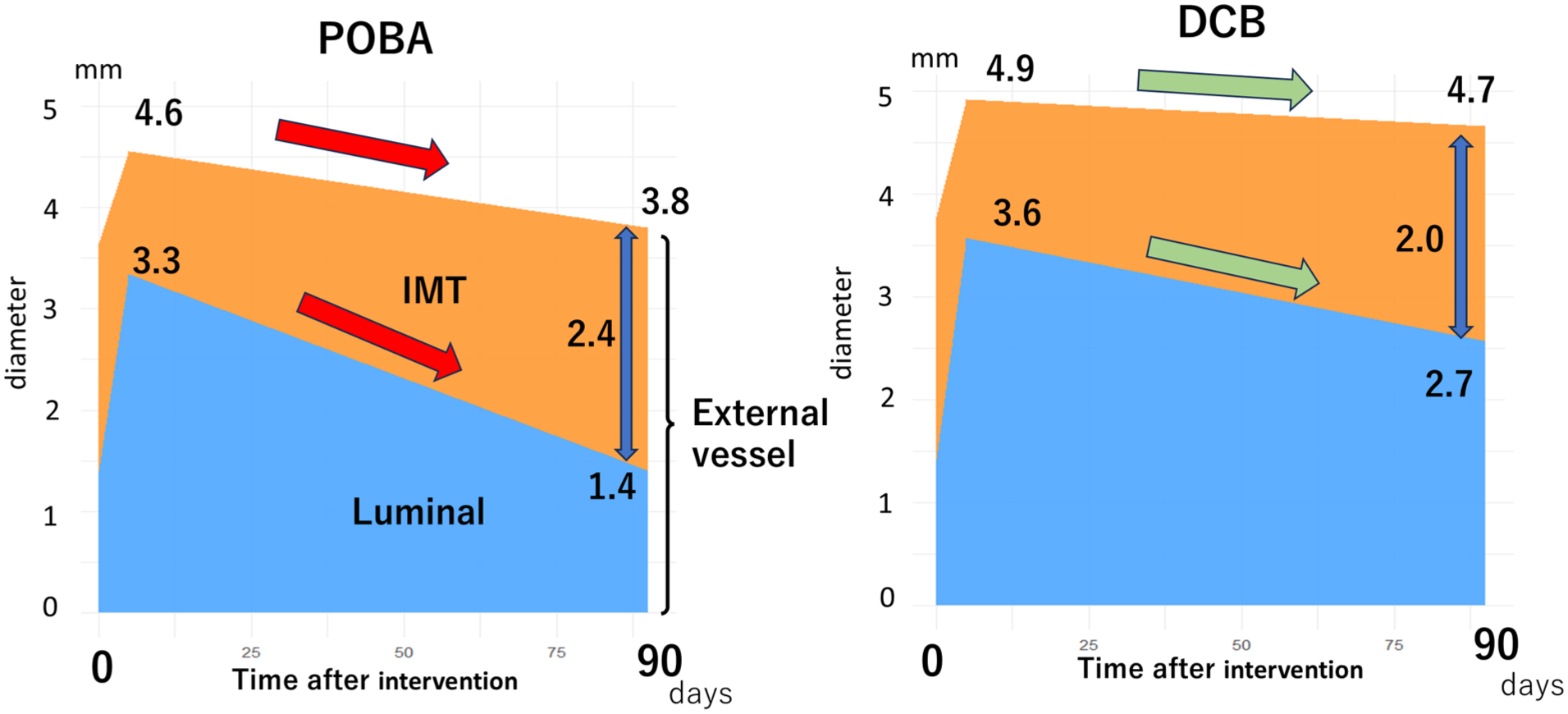
Conceptual illustration of temporal changes in vessel diameter after POBA and DCB.
The larger immediate post procedural L‑CSA observed in the DCB group warrants careful interpretation. Because paclitaxel does not produce instantaneous mechanical effects, procedural factors—such as higher inflation pressures and the use of slightly larger pre- DCB balloons—likely contributed to the greater acute expansion observed before drug delivery. To mitigate the influence of these acute differences, baseline-adjusted models incorporating immediate post-treatment CSA were applied. Even after such adjustment, DCB treatment remained independently associated with larger CSA at 3 months, indicating that the sustained differences reflect true remodeling rather than purely procedural effects. Although baseline-adjusted models mitigate the influence of acute procedural differences, residual confounding cannot be completely excluded.
Reframing the mechanism of DCB efficacy
Taken together, these findings refine the conventional “intima-centric” paradigm of DCB efficacy, which has traditionally attributed restenosis prevention primarily to suppression of neointimal proliferation.12,13
In the specific context of juxta-anastomotic AVF lesions, our results suggest that constrictive remodeling may also contribute to restenosis. A further point is that restenosis mechanisms may vary by lesion location. While our study focused on juxta anastomotic lesions, DCB efficacy is often lower in non–juxta anastomotic sites such as cephalic arch stenosis, suggesting additional contributors beyond flow related remodeling. These location specific differences may require alternative therapeutic approaches and help contextualize our findings within the broader spectrum of access stenosis.
This interpretation should be considered hypothesis-generating and may provide a broader framework for understanding lesion-specific vascular remodeling. Such multilayer effects may influence cellular behavior without necessarily manifesting as measurable changes in VWA.
This multilayered structural interpretation should be considered hypothesis-generating, providing a possible morphological framework for understanding the favorable clinical performance of DCB in juxta-anastomotic stenosis.
One possible explanation for the observed differences between POBA and DCB may involve cellular migration and matrix remodeling processes induced by angioplasty. Mechanical injury from POBA induces migration of vascular smooth muscle cells contributing not only to intimal thickening but also to progressive constrictive remodeling of the vessel wall. This concept is supported by prior work demonstrating the central role of vascular smooth muscle cell phenotypic switching and migration in arterial remodeling. 14
In contrast, paclitaxel delivered by DCB may suppress cellular proliferation and migration within both the intima and deeper vessel wall layers. Paclitaxel has been shown to inhibit smooth muscle cell proliferation and migration in vitro and to reduce neointimal formation in vivo, providing a mechanistic basis for attenuated inward remodeling after DCB treatment. 15
Although these mechanisms were not directly evaluated in the present study, this cellular‑level interpretation provides a plausible biological framework linking the observed morphological differences to known pharmacological effects of DCB.
Future directions
Future studies should address three key issues. First, comparative analyses of juxta-anastomotic and distal outflow venous stenosis are needed to clarify temporal changes in L‑CSA, E‑CSA, and VWA following POBA and DCB. Second, integration of morphological assessment with hemodynamic analysis, including computational fluid dynamics, may help elucidate the interplay between mechanical stress and the multilayered vascular response, including adventitial stabilization. Third, long-term follow-up focusing on patency and restenosis rates is required to determine whether the durability of DCB efficacy differs by lesion location. Collectively, these investigations may enable site-specific optimization of DCB therapy tailored to local hemodynamic environments.
Future studies should investigate the potential influence of cumulative prior POBA procedures on vascular structural remodeling and treatment response, as repeated interventions may alter vessel wall characteristics and remodeling capacity.
An important next step would be prospective comparative studies evaluating POBA and DCB as initial treatment strategies for juxta-anastomotic lesions.
Because the present study focused on sequential treatments in recurrent lesions, the observed differences may partially reflect lesion progression or prior treatment effects. Future randomized or prospective studies in treatment-naïve lesions would be valuable to clarify the independent role of DCB in early-stage vascular remodeling.
Limitations
This study has several limitations.
First, the sample size was relatively small (41 matched pairs), which may have limited statistical power, particularly for parameters with small effect sizes such as VWA, and may have affected the stability of the LMMs. As no a priori power analysis was performed, the results should be considered exploratory. In addition, unmeasured procedural variability—such as differences in lesion preparation—may have influenced the observed outcomes.
Second, the sequential nature of the interventions (POBA followed by DCB in the same lesion) may have introduced carry-over effects. Although this design allowed within-patient comparison, the potential influence of treatment sequence cannot be completely excluded.
Third, this study focused exclusively on juxta-anastomotic stenosis, and the findings may not be generalizable to other venous segments with different hemodynamic environments.
Fourth, the observation period was limited to 3 months, and longer-term follow-up is required to assess sustained vascular remodeling and patency.
Fifth, cases requiring reintervention before the scheduled 3-month ultrasonographic follow-up after POBA were excluded from the paired analysis.
In particular, 13 lesions underwent DCB before the planned follow-up assessment and were therefore not included. These early failure cases may have represented lesions with more aggressive biological activity or unfavorable vascular geometry, and their exclusion may have introduced selection bias toward relatively stable lesions.
In addition, vascular remodeling occurring during the early post-procedural phase was not captured in the present study. Future studies incorporating earlier ultrasonographic evaluations at shorter intervals may help clarify the mechanisms underlying early restenosis and treatment failure.
Sixth, selection bias should be considered. In this study, the median TLPP after POBA was notably short at 3.27 months, reflecting a patient population with rapid recurrence. While this specific cohort may limit the generalizability of our findings to all stenotic lesions, the superior outcomes achieved with DCB in such challenging cases further underscore its clinical efficacy over conventional POBA.
Seventh, the IMT analysis was exploratory in nature and not specifically powered to determine mechanistic relationships; therefore, these findings should be interpreted as hypothesis-generating.
Finally, hemodynamic factors such as shear stress were not directly evaluated, and future studies integrating morphological and hemodynamic analyses are needed to clarify the mechanisms underlying site-specific DCB effects.
Conclusion
This study demonstrated that DCB angioplasty provides superior TLPP compared with POBA in juxta-anastomotic AVF stenosis. This clinical benefit was supported morphologically by sustained enlargement of both luminal and externaL‑CSAs, which translated into significantly improved flow volume. Our findings suggest that DCB may help maintain vessel architecture through a combination of modest intimal thickening suppression and attenuation of constrictive remodeling. This suggests a possible site-specific, multilayered mechanism of action, offering a novel strategy for optimizing vascular access management in challenging lesions.
Footnotes
Author contributions
Study group/Acknowledgements
We would like to acknowledge the following individuals for their essential contributions to the clinical execution of this study:
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.*