
Abstract
Objective:
This study aimed to determine the effects of virtual reality on procedural pain, distress, and comfort levels during cannulation in hemodialysis patients.
Methods:
This randomized controlled study included 52 patients who were randomly assigned to either the intervention group or the control group. The intervention group received virtual reality glasses during the procedure in addition to standard routine care, while the control group received standard routine care only. Data were collected using a Descriptive Information Form, the Visual Analog Scale, the Distress Thermometer, and the Hemodialysis Comfort Scale. Statistical analysis was performed with the level of significance set at p < 0.05
Results:
Following arteriovenous fistula cannulation, the median pain and distress scores in the intervention group were found to be statistically significantly lower than those in the control group (p < 0.001). However, there was no statistically significant difference between the groups regarding patients’ comfort levels after the procedure (p = 0.75).
Conclusion:
Based on these findings, nurses can recommend virtual reality during arteriovenous fistula cannulation as a simple, cost-effective, and evidence-based non-pharmacological method for managing procedural pain.
Introduction
A critical requirement for the successful and long-term survival of patients undergoing hemodialysis is ensuring safe and permanent vascular access.1,2 This procedure is necessary for every hemodialysis treatment, and studies indicate that patients undergo an average of more than 300 cannulation procedures annually.3,4
Pain, distress, and discomfort related to arteriovenous fistula (AVF) cannulation are significant issues, with reported occurrence rates ranging widely from 12% to 80%.5,6 This persistent procedural discomfort during every hemodialysis session often leads to serious psychological and behavioral outcomes, including irritability, depression, and insomnia. Collectively, these problems contribute to non-adherence to treatment, increased healthcare costs, and a significantly reduced quality of life for patients.7 –9
Controlling pain and anxiety during cannulation is a key priority for nurses to enhance patient comfort and ensure compliance with long-term hemodialysis treatment. 7 A range of pharmacological and non-pharmacological methods are used to manage this invasive pain and distress. However, non-pharmacological approaches are now frequently preferred because they are more accessible, have minimal side effects, and are more cost-effective, thus mitigating the risks of drug dependence and side effects associated with pharmacological methods.10 –12
Virtual reality (VR) applications are a key distraction technique used to manage the pain and anxiety associated with needle-related medical procedures. VR works by using specialized hardware (headsets) and software to create a real or fictional environment, which immerses individuals and generates a powerful sensation of physical presence.13 –15 By directing a patient’s attention toward this immersive space, VR effectively slows the brain’s processing speed of pain and anxiety signals. Studies confirm the efficacy of VR in managing pain and distress during various invasive procedures, including but not limited to intravenous catheterization, insulin injections, coronary angiography, oncological treatments, and gynecological and dental procedures.8,13,16
Virtual Reality is favored in clinical practice by nurses due to its accessibility, affordability, and non-invasive nature. 10 However, research specifically investigating VR’s effect on invasive pain and distress during AVF cannulation is limited.13,17 Critically, there are no currently known studies in the literature concerning the effects of VR on the procedural pain, distress, and comfort levels associated with cannulation in hemodialysis patients. Therefore, the findings of this study are anticipated to provide valuable insights and serve as a foundational resource for future academic research in this specific area (Figure 1).

Virtual reality glasses used in the study.
Study hypotheses
H1: The use of virtual reality in hemodialysis patients is effective in reducing cannulation-related procedural pain.
H2: The use of virtual reality in hemodialysis patients is effective in reducing cannulation-related distress.
H3: The use of virtual reality in hemodialysis patients is effective in reducing cannulation-related comfort.
Methods
Study design
This study is a randomized controlled trial with control and intervention groups, pre-test and post-test. The results were reported based on the CONSORT guidelines (Figure 2).
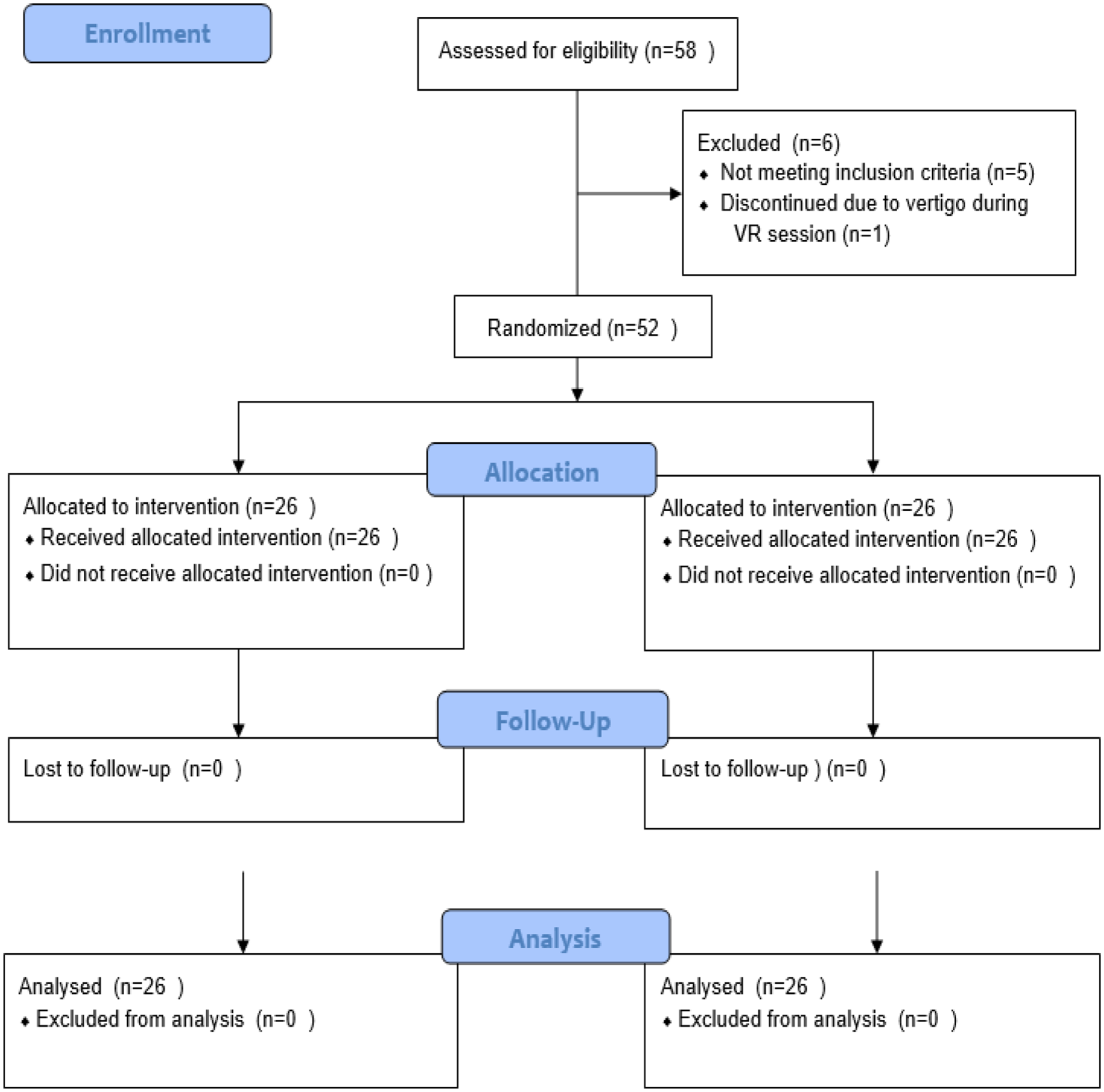
CONSORT study follow diagram.
Participants and setting
This study included patients undergoing hemodialysis (n = 52) in a dialysis unit a state hospital in Turkey between November 2024 and November 2025.
Inclusion and exclusion criteria
Participants were included if they were aged 18 or older, had been receiving hemodialysis via native arteriovenous fistulas (AVF; 4-h sessions, three times per week) for at least 6 months, had a baseline VAS pain score of 0, were not taking psychiatric medication, and provided voluntary consent. The mean duration of hemodialysis treatment for the participants was 6.43 ± 4.43 years. Exclusion criteria involved having a diagnosed mental health disability, language barriers, using analgesic drugs within 8 h before the session, or having a history of epilepsy, vertigo, anxiety, active nausea/vomiting, or headaches. Furthermore, patients with a history of vascular access complications (e.g. thrombosis or stenosis), recent access interventions, chronic pain disorders, regular painkiller use, or previous virtual reality experience were excluded from the study.
Sample size
A power analysis using G*Power 3.1.9.4 software 16 determined the minimum sample size. Based on similar literature,18 –21 an estimated effect size of 0.70 was used. Targeting a 95% confidence interval (alpha = 0.05) and 80% power, and assuming an independent-samples t-test for pain intensity differences, the required sample size was calculated to be 26 participants. The study ultimately included a total sample of 52 patients. Six patients were excluded: five did not meet the inclusion criteria, and one discontinued the virtual reality intervention due to dizziness.
Randomization and blinding
Simple randomization was performed using the website www.randomize.org. Participants with an even number were assigned to the experimental group, and those with an odd number were assigned to the control group, ensuring equal distribution. The intervention was administered by the specialist nurse researcher within the department. To maintain study objectivity (blinding), pre- and post-procedure tests were administered by a clinical nurse independent of the study. Finally, data entry and statistical analyses were conducted by two separate, independent researchers.
Measurements
The data were collected by the researcher by using “Descriptive Information Form,” “Visual Analog Scale (VAS),” Distress Thermometer (DT), and the Hemodialysis Comfort Scale (HDCS).
Descriptive Information Form
This form prepared by the researchers after reviewing relevant literature,18,21 this semi-structured form includes 12 questions focusing on the socio-demographic and medical information of the participants. The researchers administered the questionnaire through face to face interviews, taking approximately 10 min during the second hour of hemodialysis treatment.
Visual Analog Scale
This scale, originally developed by Price et al. 22 and validated in Turkish for postoperative pain assessment by Eti Aslan, 23 was used to quantify pain intensity. The scale consists of a 10-cm horizontal line anchored by the descriptors “no pain” and “worst imaginable pain.” Participants marked their perceived pain level on the line, and the score was recorded in centimeters. Written permission for the Turkish version was secured from Eti Aslan. All VAS measurements were recorded by an independent nurse who was not involved in the intervention.
Distress Thermometer
Developed by Roth et al. to define non-pathological distress, the DT is a single-item scale rated from 0 to 10. 24 The accompanying problem list was established by the National Comprehensive Cancer Network and the scale’s Turkish validity was established by Ozalp et al. 25 The scores are grouped into clinical zones to guide intervention: the Yellow Zone indicates a need for intervention, and the Red Zone necessitates urgent and comprehensive intervention. The DT is frequently used as a screening tool in various studies, including those assessing distress in hemodialysis patients.26 –28
Hemodialysis Comfort Scale
This scale developed by Orak et al., 29 is a reliable, nine-item, five-point Likert-type instrument used to assess comfort in patients receiving hemodialysis for at least 6 months. It consists of two subscales: “Relaxation” and “Coping.” Items are scored from 1 to 5 with Item 4 being reverse-scored. Total scores range from 9.00 to 45.00, where higher scores indicate greater comfort. Subscale ranges are 3.00–15.00 for Relaxation and 7.00–30.00 for Coping. The scale demonstrated strong reliability, with a Cronbach’s alpha of 0.87 in the original Turkish validation study, and 0.80 in the present study.
Data collection
Dialysis sessions occurred 3 days a week (Monday–Wednesday–Friday or Tuesday–Thursday–Saturday) between 08:00 and 16:00 h. All consenting patients meeting the study criteria were included. Data collection began after obtaining written consent. The descriptive information form was completed in the patient’s room 15–20 min before the cannulation procedure. This process did not interfere with routine treatment, care, personnel schedules, or the cannulation procedure itself. Subsequently, the DT was administered via face-to-face interview both before and after the cannulation (first measurements) and recorded by a nurse independent of the study.
Intervention and procedure
The intervention utilized a VR Shinecon head-mounted display (HMD) integrated with a compatible smartphone to provide a stereoscopic, 3D viewing experience. The system employed adjustable lenses for depth perception and delivered fully immersive 360° nature-based relaxation scenes (e.g. forests, seascapes) with accompanying stereo audio. By simultaneously stimulating visual and auditory channels, the intervention aimed to occupy cognitive resources, thereby diverting attention from nociceptive stimuli and modulating pain perception. While the VR media were commercially available rather than developed through a user-centered co-design process, the content was specifically selected for its clinical suitability, ease of use, and potential to provide a calming experience for adult hemodialysis patients. For infection control, the HMD was disinfected with alcohol-based wipes between uses.
The procedure was executed in three distinct phases:
Pre-procedure: Approximately 3 min before the AVF cannulation, patients selected their preferred VR environment, and the intervention commenced to allow for adequate immersion.
During the procedure: While the patient engaged with the passive VR content, their pain was evaluated and recorded by an independent nurse (first measurement).
Post-procedure: Immediately following the completion of the procedure and removal of the HMD, the independent nurse assessed and recorded the VAS, DT, and HDCS scores (second measurement).
To ensure participant safety, the intervention was conducted in a seated or semi-recumbent position under the joint supervision of the researcher and a dialysis nurse. Patients were monitored for cybersickness (e.g. dizziness, nausea); in this study, one participant reported dizziness and subsequently withdrew, with no other significant adverse events observed.
Because the primary objective was to evaluate clinical outcomes, no formal immersion questionnaires were administered. However, continuous observation confirmed high usability with no reported technical malfunctions, latency, or connectivity issues. To maintain study rigor, all sessions were managed by a single trained researcher using a standardized protocol to ensure consistent hardware, content, and timing across the intervention group.
Control group
Patients in the control group received the routine cannulation procedure with no additional intervention. During the procedure, the patient’s pain was assessed and recorded by an independent nurse using the VAS (first measurement). After the procedure (second measurement), both VAS and DT were again evaluated and recorded by the independent nurse. Additionally, the HDCS score was evaluated and recorded immediately after the procedure was completed.
Ethical approval
The research obtained ethical approval (2024/106) from the University’s non-interventional ethics committee and institutional permission (date: February 1, 2025; number: 4) from the relevant hospital. In line with the Declaration of Helsinki’s Privacy and Confidentiality Principle, all steps were taken to ensure the confidentiality of participating volunteers and their personal information. The study’s purpose and its voluntary nature were explained to each patient, who was informed that the collected data would be used strictly for scientific purposes.
Data analysis
Data analysis was conducted using SPSS for Windows Version 24.0 (Statistical Package for Social Sciences, Inc., Chicago, IL, USA). Frequency and percentage analyses were used for employee descriptive characteristics, while mean and standard deviation summarized the scale data. Kurtosis and Skewness assessed variable normality. The paired-sample t-test and Wilcoxon signed-rank test determined score changes within a single group over time. The independent sample t-test compared mean scores between groups. For non-parametric comparisons, the Wilcoxon signed-rank and Mann–Whitney U test were employed. Categorical variables were analyzed using the chi-squared test. Statistical significance was accepted at p < 0.05.
Results
The results of the group comparisons indicated that the study groups were homogeneous regarding their socio-demographic and disease-related characteristics. This homogeneity confirms that the groups were comparable at baseline, ensuring the results were not confounded by variables that might otherwise influence the severity of pain and distress experienced by the patients. 30
Participants in the intervention group had a mean age of 52.15 ± 17.69 years. The majority were male (61.5%) and had completed primary education (69.2%). More than half of the participants (61.5%) had been receiving hemodialysis treatment for 5 years or longer. The most common primary cause of renal failure was glomerulonephritis (69.2%; Table 1).
Sociodemographic and clinical characteristics of the participants by group.
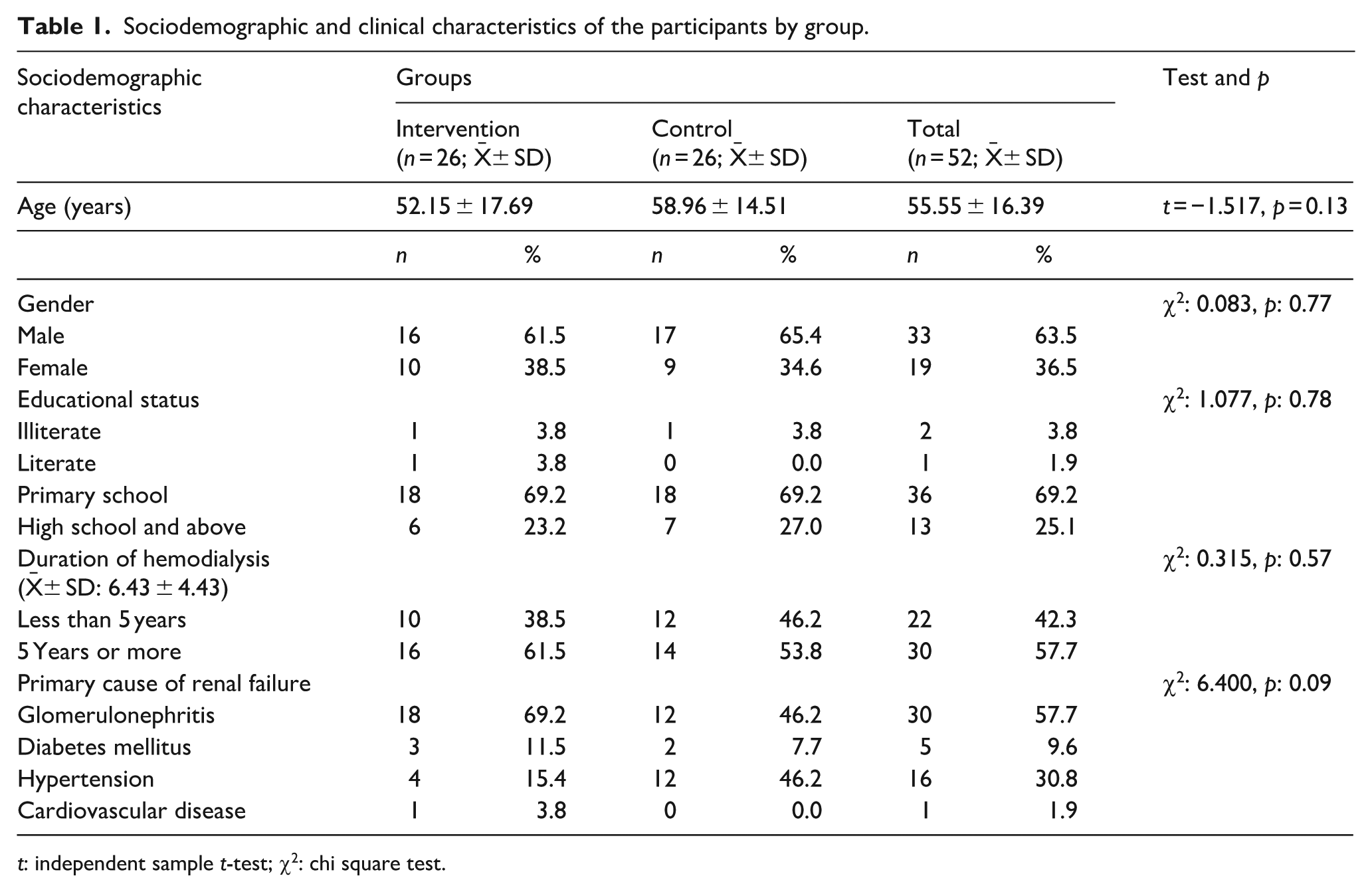
t: independent sample t-test; χ2: chi square test.
The VAS scores of the intervention group were found to be statistically significantly lower than the control group after (p < 0.001, Z = −3.857) the procedure. After the procedure, the DT scores of the patients in the control group were found to be statistically significantly higher than those in the intervention group (p < 0.001, Z = −2.269). No statistically significant within-group change in distress scores was observed in either group. Additionally, the magnitude of change between the groups did not reach statistical significance (p > 0.05; Table 2). There weren’t any statistically significant differences between the groups after the procedure regarding the HDCS of the patients (t = 0.318, p = 0.75).
Comparison of pain, distress, and comfort level scores between groups.
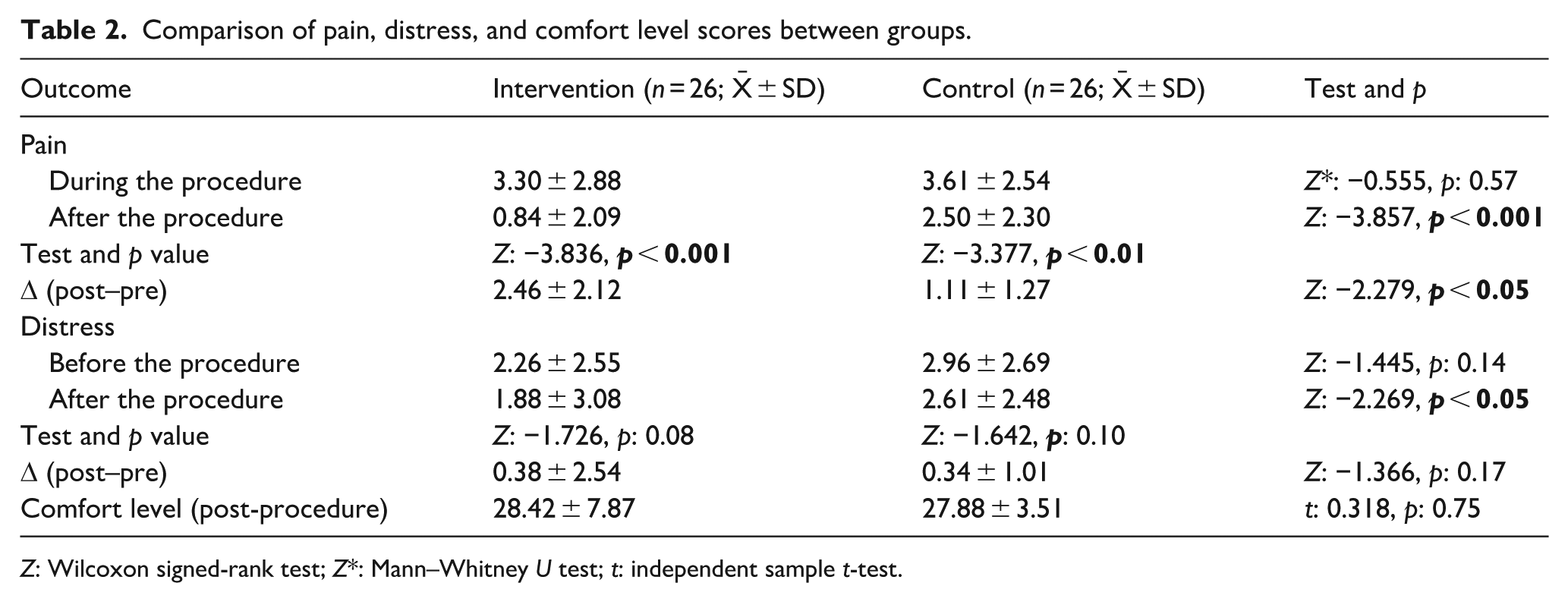
Z: Wilcoxon signed-rank test; Z*: Mann–Whitney U test; t: independent sample t-test.
Discussion
Inadequate pain and distress management during medical procedures can lead to therapy avoidance, poor recovery, and psychological trauma.9,13,31 Given that hemodialysis is a long-term, repetitive treatment, the unnerving nature of regular cannulation often reduces patient compliance.3,4,8
While distraction is a long-established intervention for pain and distress, VR has emerged as a novel technique.17,32 Despite its potential, existing literature has limited studies examining VR’s effectiveness specifically for managing pain, distress, and comfort during AVF cannulation.7,33 The findings of this study partially support the effectiveness of VR distraction during AVF cannulation. While our results clearly demonstrate a statistically significant reduction in procedural pain in the intervention group compared to the control group, the impact on distress and comfort levels was more nuanced. Our findings align with established research, including a systematic review of 42 trials recommending VR for clinical pain reduction and other reviews validating its efficacy in managing acute procedural pain. 34 The literature confirms that VR decreases pain and improves distress management across various needle-related and invasive procedures, ranging from vascular access and biopsies to burn debridement and endoscopic interventions.15,35 –40 However, while we observed a clinical decrease in distress in the intervention group contrasting with the increase in the control group this trend did not reach statistical significance. Similarly, no significant difference was found in patient comfort levels. 41
This suggests that while VR is a highly effective tool for acute pain modulation, its influence on broader psychological constructs like “overall comfort” and “procedural distress” may be limited by the short duration of the VR experience relative to the patients’ long-term, chronic exposure to hemodialysis.
Unlike traditional methods like topical anesthetics or verbal distraction, VR offers a uniquely immersive multisensory experience that decouples attention from the stimulus by creating a sense of “presence.” 42 Nonetheless, as a pilot study, these results highlight VR’s potential while underscoring the need for larger-scale trials to compare VR directly with other techniques and evaluate its cumulative impact on holistic patient comfort.
Limitations
The primary limitations of this study include the lack of participant blinding, an inherent challenge in non-pharmacological VR distraction research. Additionally, the reliance on self-reported measures for pain, distress, and comfort may introduce individual perceptual biases. The use of a single VR session precludes evaluating long-term efficacy or potential habituation effects. Furthermore, as a single-center pilot study with a small sample size, the generalizability of these findings to the broader Turkish hemodialysis population is limited. Finally, although vascular access characteristics were recorded, confounding variables such as overall comorbidity status and concurrent pharmacological treatments were not fully controlled.
Conclusion and clinical implications
This study confirms that VR is a viable non-pharmacological tool for significantly reducing cannulation-related pain in hemodialysis patients. While its effect on distress warrants further large-scale validation, its success in pain modulation empowers nurses to champion this technology. Integrating VR training into nursing curricula and in-service programs is recommended to enhance patient experience and strengthen the nurse’s role in proactive pain management.
Footnotes
Acknowledgements
We thank the participants for investing their time and attention in this research. There is no external funding for this study.
Author contributions
Ezgi Mutluay Yayla and Mehmet Ağaslan was involved in the entire study process. All authors contributed to the literature review, design, data collection, analysis and interpretation, critical review and writing up of the study. All authors read and approved the final version of the paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author.