
Abstract
Central vein stenosis or occlusion is a significant cause of vascular access dysfunction in patients with chronic kidney disease (CKD). Typically related to intraluminal factors such as long-term cuffed hemodialysis catheters or thrombus formation, central venous stenosis may also result from extrinsic compression by adjacent musculoskeletal or vascular structures. Here we report a case of central vein stenosis secondary to extrinsic compression caused by pericardial effusion. A 68-year-old woman with CKD secondary to immunoglobulin A nephropathy underwent left forearm arteriovenous fistula (AVF) creation before dialysis initiation and developed severe edema of the left upper limb. Computed tomography revealed stenosis of the left brachiocephalic vein for which percutaneous transluminal angioplasty was performed; recanalization was achieved. However, the thrombus in the brachiocephalic vein persisted; therefore, anticoagulation therapy and a pericardiocentesis were performed, resulting in the draining of more than 2 L of fluid. Thereafter, the thrombus disappeared, stenotic lesion improved, and upper-limb edema improved. Throughout this case, clinicians should be aware of this potential complication caused by a massive pericardial effusion, and additionally, prompt combination therapy, that is, endovascular therapy, anticoagulation therapy, or pericardiocentesis, could maintain a patent AVF.
Keywords
Introduction
Central vein stenosis or occlusion is a common cause of vascular access dysfunction. 1 In patients receiving hemodialysis (HD) with arteriovenous fistula (AVF) creation, central veins including the cephalic arch, subclavian vein, brachiocephalic vein, and iliac vein are commonly affected by stenosis. 2 Additionally, stenosis often causes various clinical symptoms such as swelling; significant venous dilatation; and worsening upper-extremity edema with pain, discomfort, skin ulceration, and recurrent infections of the upper limb. 3 Therefore, patients with central vein stenosis must be treated as intentionally as possible.
The primary risk factors for central vein stenosis or occlusion include the use of HD catheters 4 or extrinsic compression of the vein such as due to large lung cancer, open chest surgery, or unusual musculoskeletal structures, 3 in which cases the vein can be easily compressed structurally versus the artery. Percutaneous transluminal angioplasty (PTA) is often recommended for central vein stenosis or occlusion due to its high initial success rate, technical feasibility, and low complication rate. 3
Here we report a rare case of brachiocephalic vein stenosis caused by compression due to a massive pericardial effusion.
Case description
A 68-year-old Japanese woman presented with chronic kidney disease (CKD) due to immunoglobulin A nephropathy. An AVF was created in the left forearm more than 1 year earlier; however, she had not yet been initiated HD. A pericardial effusion was also previously identified. Although she had hypertrophic obstructive cardiomyopathy, the cause of the pericardial effusion was unclear, and it had recently shown progressive worsening (Figure 1(a)); pericardiocentesis was considered. Two days prior to the admission, she rapidly developed edema in the left upper limb with an AVF. Ultrasonography revealed no abnormalities, including vascular stenosis within the arm with the AVF; therefore, she was referred to our hospital for further examination and treatment.
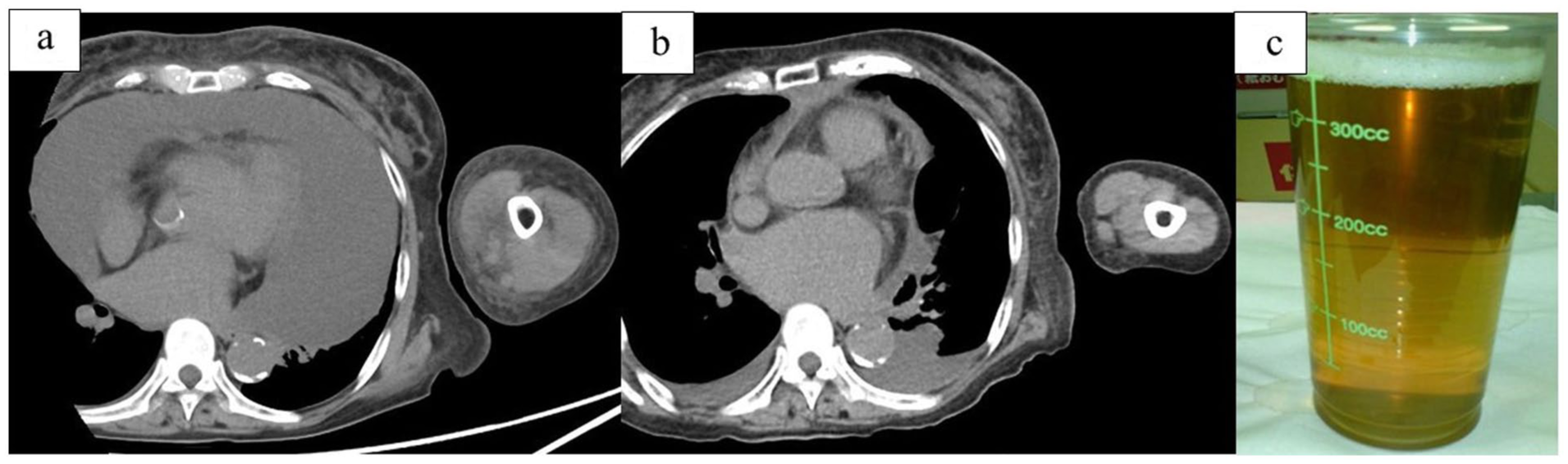
Computed tomography images of the pericardial effusion and arteriovenous fistula limb before and after pericardiocentesis. (a) Before the pericardiocentesis. (b) After the pericardiocentesis. (c) Extracted pale-yellow pericardial effusion fluid.
On admission, the patient’s systolic/diastolic blood pressure was 163/89 mmHg, heart rate was 72 beats/min, respiratory rate was 18 breaths/min, and oxygen saturation was 97% on room air. A physical examination revealed severe edema of the left upper limb. However, thrill and bruit were present over the AVF. Blood tests showed elevated levels of blood urea nitrogen (96 mg/dL), serum creatinine (7.18 mg/dL), fibrinogen (416 µg/mL), and serum D-dimer (3.9 µg/mL). The prothrombin time–international normalized ratio (PT-INR; 1.13), activated partial thromboplastin time (APTT; 29.4 s), and antithrombin III level (56%) were within the normal ranges. Chest radiography revealed marked cardiomegaly, while electrocardiography revealed inverted T waves in leads I, II, and V3–V6. Unenhanced computed tomography (CT) revealed no external factors such as a mass lesion except for a massive pericardial effusion, although the left brachiocephalic vein was compressed.
Angiography performed after the hospitalization revealed a vascular occlusion in the left brachiocephalic vein (Figure 2(a)). Therefore, the patient was diagnosed with secondary venous hypertension due to the central venous occlusion. Following angiography, thrombus removal was performed as possible, but passing the guidewire proved very difficult. Therefore, we prioritized dilation of the stenotic lesion to circulate blood within the brachiocephalic vein and prevent thrombus formation. First, PTA was performed using a 0.035-inch guidewire and 6-mm balloon dilation catheter (Mustang™; Boston Scientific Japan, Tokyo, Japan) and mainly dilated the brachiocephalic vein up to the rated burst pressure (24 atm; Figure 2(b)). Thereafter, to enable additional dilation with matching brachiocephalic venous diameters, the balloon catheter was exchanged for an 8-mm balloon dilation catheter (Mustang™; Boston Scientific Japan). Although a large residual thrombus was observed, recanalization using PTA was successful (Figure 2(c)). Consequently, a continuous intravenous heparin sodium infusion of 20,000 U/day was initiated immediately after PTA. In the clinical course (Figure 3), because the APTT was excessively prolonged (148 s) on hospital day 2, the heparin dose was reduced to 15,000 U/day.
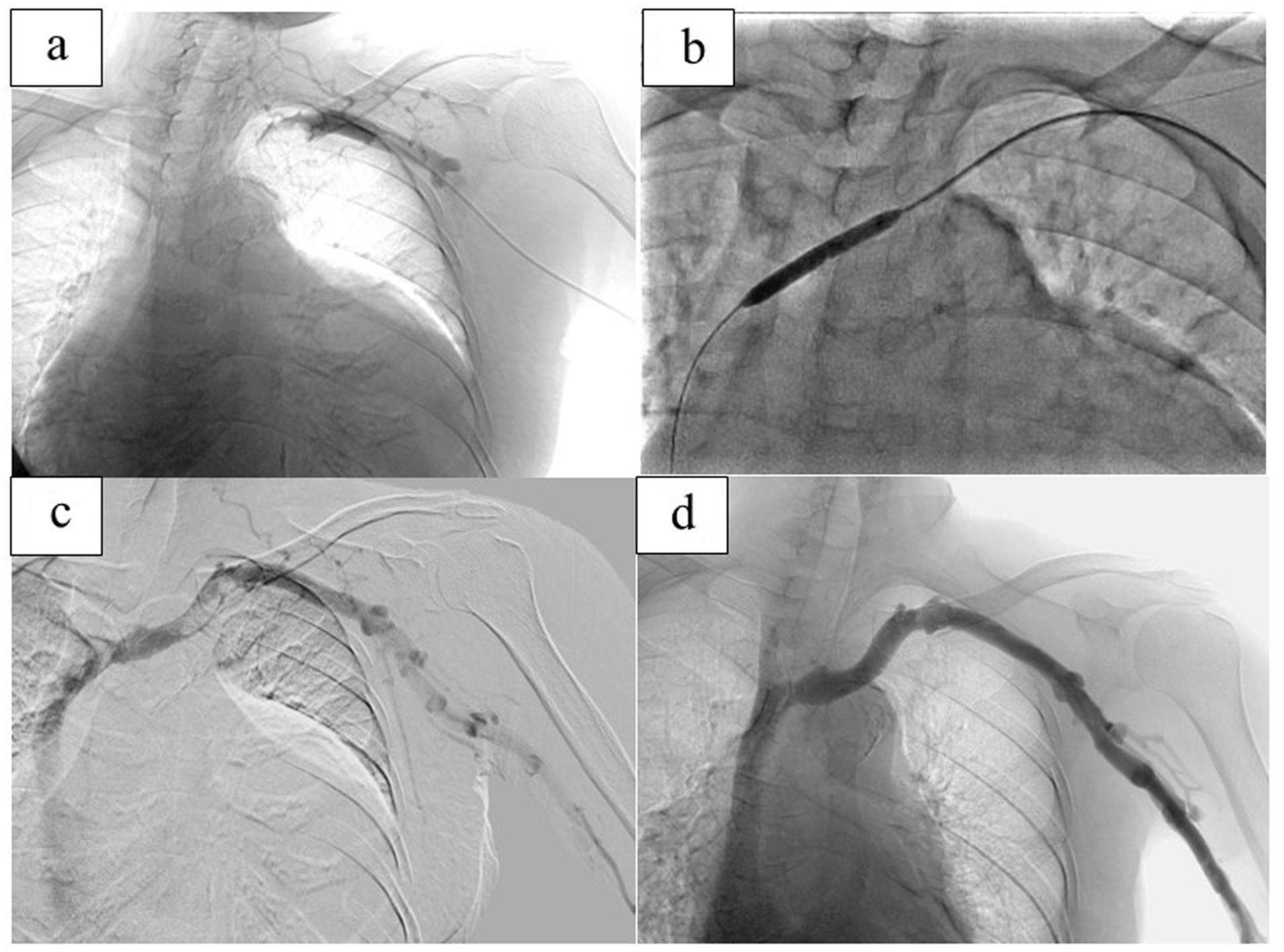
Angiograms taken before versus after PTA. (a) Initial angiogram showing stenosis of the left brachiocephalic vein. (b) Angiogram taken during PTA using a 6-mm balloon catheter at 24 atm. (c) Angiogram taken post-PTA showing successful recanalization with residual stenosis and thrombus. (d) Final angiogram demonstrating recanalization of the stenosis and the thrombus in the left brachiocephalic vein.
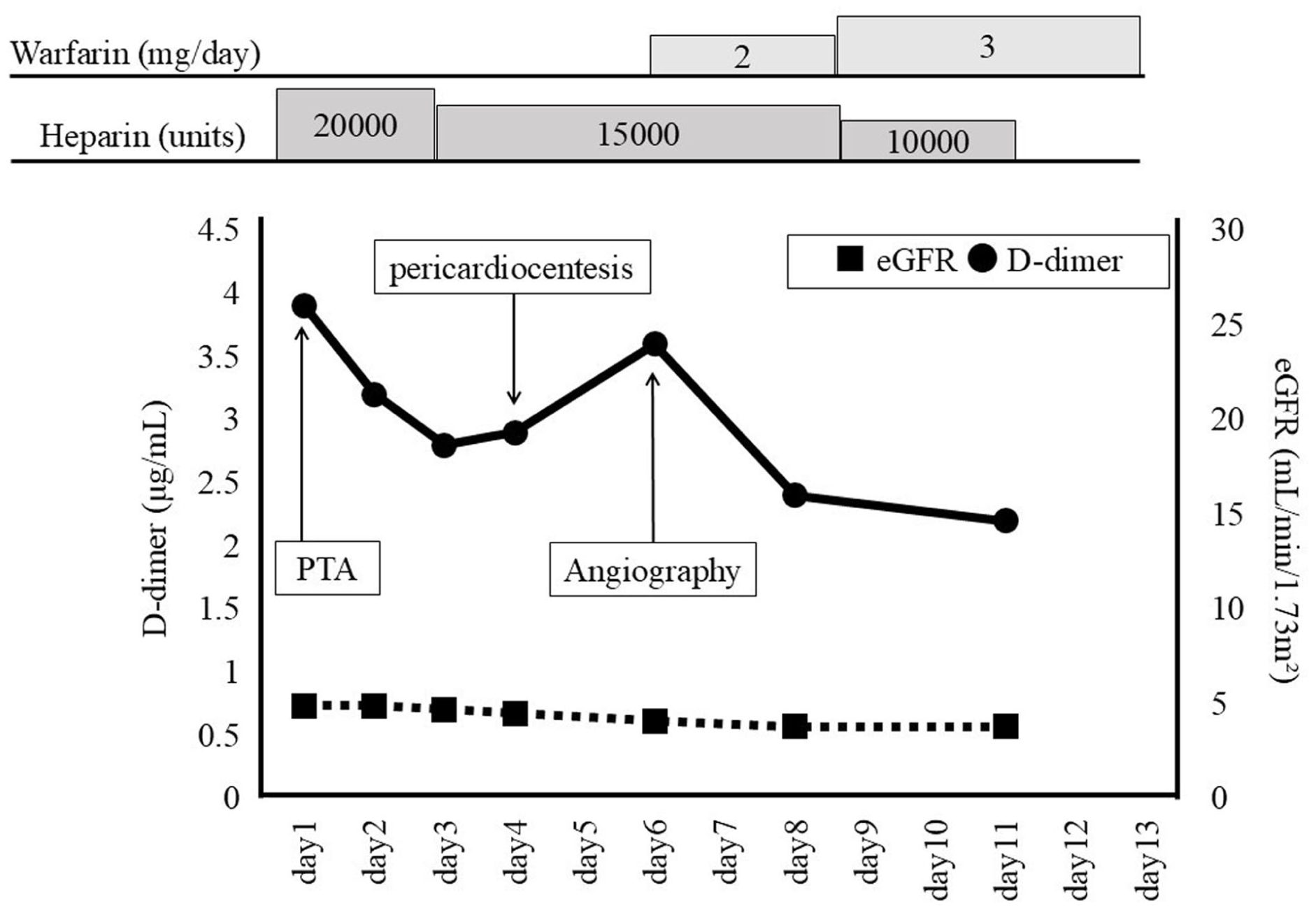
Patient’s clinical course.
Considering the possibility that the massive pericardial effusion was compressing the left brachiocephalic vein and causing the stenosis, a pericardiocentesis was performed by a cardiologist on hospital day 4 (Figure 1(b)), during which 2270 mL of non-bloody, pale-yellow fluid was drained (Figure 1(c)). A pericardial fluid analysis revealed a cell count of 60, total protein level of 4.9 g/dL, albumin level of 2.6 g/dL, lactate dehydrogenase level of 42 U/L, adenosine deaminase level of 9.3 IU/L, and hyaluronic acid level of 11,700 ng/mL. A cytological examination revealed no malignant cells, and bacterial cultures were negative.
On hospital day 6, an angiography was performed to confirm the venous condition, and we confirmed disappearance of the thrombus and improvement of the brachiocephalic vein deviation by the massive pericardial effusion (Figure 2(d)). Two days after the re-angiography, the left upper-limb edema disappeared. Thrombophilia workup results were negative (antinuclear antibody, anti-double-stranded DNA antibody, anticardiolipin antibody, lupus anticoagulant, anti-SS-A antibody, anti-SS-B antibody, protein C, and protein S); therefore, the cause of the venous stenosis was identified as the massive pericardial effusion. Warfarin 2 mg/day was started to replace the heparin infusion and increased to 3 mg/day at discharge. As of 6 months after discharge, no recurrence of the left upper-limb edema was noted.
Discussion
Central vein stenosis or occlusion is a clinically significant complication of HD-related vascular access, as it can cause vascular access problems such as ipsilateral swelling, marked venous dilatation, worsening upper-extremity edema with associated pain and discomfort, skin ulceration, and recurrent infections. 3 Previous reports demonstrated an approximately 10% prevalence of central vein stenosis in patients with CKD, including those who have not yet started HD. 4 Thus, it is not necessarily a rare complication, and clinicians should be well informed about appropriate management strategies.
The major risk factors for central vein stenosis include the use of long-term cuffed HD catheters, the placement of cardiac rhythm devices, and a previous history of dialysis access or transplantation. 4 The mechanism of vein stenosis involves venous wall thickening resulting from microthrombus formation and smooth muscle proliferation caused by endothelial injury. 5 An intravascular obstruction due to long-term cuffed HD catheter use may be affected by other factors contributing to thrombus formation, such as intimal vessel injury, turbulent blood flow, and coagulation cascade activation, that lead to fibrin sheath formation. 6 In contrast, extrinsic compression of the central veins might cause turbulent blood flow or thrombus formation resulting from a tumor mass effect, post-surgical scarring, musculoskeletal or vascular compression, or fibrosis. 3 Furthermore, it was previously reported that extrinsic anatomical compression of the central veins was frequently observed in the subclavian vein, which passes between the clavicle and the first rib. 7
Our patient had no history of HD catheter insertion or cardiac rhythm device implantation, and the thrombophilia workup in this case was unremarkable. CT did not demonstrate mass lesions or other potential causes of extrinsic compression except the massive pericardial effusion. As the stenotic lesion caused by extrinsic compression improved after the pericardiocentesis, we concluded that the left brachiocephalic vein stenosis was caused by the massive pericardial effusion. Only a few reports have described superior vena cava stenosis caused by a pericardial effusion. 8 However, to our knowledge, no previous report has described brachiocephalic vein compression or stenosis in a patient with an AVF secondary to a pericardial effusion.
PTA is widely recommended as the first-line therapy for managing symptomatic central vein stenosis or occlusion associated with HD access owing to its favorable initial success rate, high technical feasibility, and relatively low complication rate. 3 However, a major limitation of PTA is its high restenosis rate because its use in the central versus peripheral veins tends to cause recoiling. 9 When PTA alone fails to achieve adequate dilation or the stenosis is recurrent, stenting of the central vein is sometimes advised. 9 Nevertheless, current evidence remains inconclusive, as several studies reported no significant difference in primary patency rates between PTA alone and PTA plus stenting. 3 Therefore, additional stenting therapy is typically individualized according to a patient’s clinical situation. In our case, PTA did not fully dilate the veins without thrombus formation. The underlying cause was suspected as extrinsic compression by the massive pericardial effusion, and the pericardiocentesis might have improved blood stagnation and flow in the brachiocephalic vein. However, the treatment sequence, in which PTA preceded the pericardiocentesis, may have led to the favorable outcome. If a pericardial effusion can be removed all at once and the extrinsic pressure dramatically released by the pericardiocentesis, the brachiocephalic vein can rapidly dilate after the drainage occurs. Thus, in this case, a large thrombus in the brachiocephalic vein might have flowed into the pulmonary artery in the large state. Therefore, it would have been preferable to first partially relieve the stenosis using PTA, followed by pericardiocentesis under concomitant anticoagulation therapy.
Inevitably, although the thrombus mobilizes and partly embolizes the pulmonary artery after any treatment, the best decision should be made by combining the available therapeutic options. Moreover, a pericardial effusion is relatively common in patients receiving HD and can result from cardiac disease or uremia. Therefore, in patients with both central venous stenosis and a pericardial effusion who are undergoing HD, a pericardiocentesis should be considered in addition to PTA.
Conclusions
In summary, here we reported a case of brachiocephalic vein stenosis caused by compression by a massive pericardial effusion. Clinicians should be aware of the potential risk of central venous stenosis due to extrinsic compression in patients with CKD, AVF, and a pericardial effusion.
Footnotes
Author contributions
Y. W. collected the data and wrote the original manuscript. K.I. and Y. M. diagnosed and collected the data and edited the manuscript. J.M., S.I., H.M., and Y.K. collected the data and reviewed and edited the manuscript. S.O. critically revised and supervised the manuscript. All authors approved the final manuscript.
Data availability
The data supporting the findings of this case report are available upon request from the corresponding author.*
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Institutional review board approval was not required for this single case report.
Consent for publication
Informed consent was obtained from the patient for the publication of this case report.