
Abstract
Background:
Long peripheral catheters are increasingly used as an alternative to short peripheral catheters for short-term intravenous therapy, particularly in patients with difficult intravenous access. However, evidence on their short-term functional performance and the impact of insertion techniques remains limited.
Methods:
This retrospective observational study included adult patients who received 4 Fr, 11 cm catheters inserted in the mid-upper arm at a tertiary academic hospital between January and August 2024. Clinical and procedural data were collected from routine records. Outcomes at 7 days included catheter function, ultrasound findings and complications. Associations between insertion technique, tip location and outcomes were explored using Spearman’s correlation analysis.
Results:
A total of 106 patients were included (mean age 77 ± 12 years), of whom 55 (51.9%) had catheter s in place at day 7. Dysfunction in withdrawal was common (54.5%), whereas infusion dysfunction was infrequent (5.4%). Ultrasound findings included non-compressible veins (23.6%) and hyperechoic material at the catheter tip (40%). The pseudo-tunnel technique was adopted in 40% of insertions. No significant associations were found between procedural variables and clinical outcomes (all p > 0.05).
Conclusions:
Long peripheral catheters represent a useful option for short-term vascular access in patients with difficult venous access. However, their limited reliability for blood withdrawal and the frequency of functional alterations after 7 days highlight the importance of careful device selection and close clinical monitoring.
Introduction
Vascular access is a fundamental component of inpatient care, as most hospitalised patients require intravenous therapy during their admission. Each year, hundreds of millions of vascular access devices (VADs), both central and peripheral, are inserted worldwide, highlighting their central role in contemporary clinical practice. 1 Among these, peripheral venous catheters are the most used, owing to their ease of insertion and wide applicability across different clinical settings.2,3
Peripheral venous access devices are generally classified according to catheter length and tip location into three main categories: short peripheral catheters (SPCs), long peripheral catheters (LPCs) and midline catheters. SPCs, typically 2–6 cm in length, are inserted into superficial veins and are widely used in acute care. LPCs, ranging from 6 to 15 cm, are placed under ultrasound guidance into superficial or deep veins, with the tip located in the proximal upper limb venous system. Midline catheters (15–25 cm) are similarly inserted under ultrasound guidance, with the tip positioned in deeper veins such as the axillary or subclavian vein.4,5
While SPCs remain the first-line device in many settings, their high early failure rates, reported between 43% and 59%, have raised concerns regarding their reliability. These failures are mainly related to complications such as occlusion, thrombosis, phlebitis, infiltration, dislodgement and infection, often leading to repeated insertions and increased resource utilisation.6,7
In this context, LPCs have emerged as a potentially valuable alternative, particularly for patients requiring short- to intermediate-term intravenous therapy or presenting with difficult venous access (DIVA).8,9 Their greater length and deeper tip location may improve device stability and reduce the risk of premature failure, while still maintaining a peripheral approach. However, despite their increasing use in clinical practice, evidence on their functional performance, complication profile and optimal insertion strategies remains limited.
In particular, the role of insertion technique and tip location in influencing short-term outcomes has not been clearly defined. The present study was therefore designed to evaluate the clinical performance of LPCs over a standardised 7-day dwell period, focussing on insertion technique and clinically relevant outcomes, including catheter function, complications and safety.
Methods
Study design and setting
This retrospective observational study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 10 guidelines at an Italian academic hospital (IRCCS San Gerardo dei Tintori Foundation, Monza, Italy) between January and August 2024. The study focussed on LPCs placed in hospitalised adult patients as part of routine clinical care.
In the study centre, LPCs are preferentially used for short-term therapy in patients with unavailable or unsuitable superficial veins at the forearm level, whereas SPCs are used when superficial venous access is feasible. As a result, LPCs are typically inserted in the mid-upper arm.
Study population
Patients aged ⩾18 years who received a 4 Fr, 11 cm LPC inserted in the mid-upper arm during the study period were eligible for inclusion. Patients younger than 18 years and those who received a 3 Fr LPC were excluded. Consecutive eligible patients were retrospectively identified and included in the analysis.
Catheter type
All devices were 4 Fr × 11 cm power-injectable long peripheral catheters (Microcath, Deltamed S.p.A., Viadana, Italy).
Insertion procedure
All LPCs were inserted by trained nurses of the local Vascular Access Team (VAT), following current evidence-based practice and the SIP protocol, with strict adherence to a catheter-to-vein ratio of <33%. 11
Procedures were performed under ultrasound guidance and included pre-procedural assessment of upper limb, supraclavicular and infraclavicular veins. Full aseptic technique was adopted using 2% chlorhexidine gluconate in 70% isopropyl alcohol and maximal sterile barrier precautions. Vein selection was based on vessel diameter and anatomical location according to Dawson’s ‘green zone’ approach.11,12
Prior to venipuncture, the median nerve and brachial artery were identified by ultrasound. Venipuncture was performed under real-time ultrasound guidance, with intra-procedural confirmation of catheter tip position.
When a vein of adequate calibre was available within Dawson’s ‘green zone’, direct puncture was performed. Conversely, when the most suitable vein was located within the ‘yellow zone’, the pseudo-tunnel technique was adopted in order to maintain an appropriate catheter exit site position within the green zone.13,14 The devices available to the Vascular Access Team allowed the use of either the direct or the indirect Seldinger technique. In the study centre, this aspect of the procedure was not rigidly standardised, and the choice of insertion technique was left to the operator’s discretion, according to individual preference and technical expertise.
Data collection and outcomes
Data were retrospectively collected from routine clinical records. Baseline variables included demographic and clinical characteristics (age, sex, hospital ward and DIVA condition, assessed using the A-DIVA score),9,15 as well as procedural data, including direct venipuncture versus pseudo-tunnel technique, Seldinger technique and ultrasound-assessed catheter tip position classified relative to the axillary line as distal or at/proximal.
Clinical outcomes were assessed at 7 days after insertion by the local VAT nurses, trained in vascular ultrasound for the identification of potential catheter-related complications. The following variables were recorded: Visual Exit Site (VES) score, 16 presence of haematoma, total occlusion, sub-occlusion, persistent withdrawal occlusion (PWO), vein compressibility, presence of hyperechoic material at the tip or along the catheter, leakage and exit site infection. 17 In cases of early catheter removal (before day 7), the reason for removal was documented, including accidental self-removal, hospital discharge, death or completion of therapy. All data were collected as part of routine follow-up performed by VAT nurses, according to local institutional protocols. The retrospective nature of the study did not allow discrimination between thrombosis and fibroblastic sheath formation; therefore, these findings were collectively reported under the term ‘hyperechoic material’. Routine ultrasound follow-up was primarily aimed at functional and morphological catheter assessment rather than formal diagnostic evaluation for catheter-related thrombosis. A more detailed diagnostic assessment was performed only in the presence of clinical signs or symptoms suggestive of thrombosis.
The study was approved by the local Ethics Committee (Comitato Etico Territoriale Lombardia 3; approval date: March 11, 2026). All clinical and ultrasound data had been routinely collected during standard VAT follow-up activities. Ethical approval for retrospective scientific analysis of the anonymised dataset was obtained before data extraction and formal analysis for research purposes.
Statistical analysis
Data were recorded in Microsoft Excel and analysed using JMP 16 (SAS Institute, Cary, NC, USA). Continuous variables were expressed as mean ± standard deviation or median (interquartile range), as appropriate, while categorical variables were presented as counts and percentages.
Bivariate analysis was performed using Spearman’s rank correlation coefficient (ρ) to assess associations between procedural variables and clinical outcomes. Correlation analysis was conducted on the subgroup of patients with catheters in place at day 7 (n = 55). A two-sided p < 0.05 was considered statistically significant.
Given the exploratory design of this retrospective observational study and the limited number of patients with catheters still in place at day 7, statistical analyses were performed with a descriptive and exploratory purpose. The study was not originally planned to test predefined hypotheses or detect specific effect sizes; therefore, no a priori sample size calculation was performed. The primary aim was to provide a real-world description of short-term functional and ultrasound findings associated with LPC use in clinical practice.
Results
A total of 106 patients were observed, with a mean age of 77 ± 12 years; 52 (49%) were male. Patients were admitted to medical (44%), surgical (34%) and intensive or sub-intensive care units (23%).
Of these, 51 (48.1%) patients underwent early catheter removal before day 7, while 55 (51.9%) retained the catheter for the full observation period of 7 days and were included in the outcome analysis. Most early catheter removals were related to completion of therapy or hospital discharge rather than device-related complications. Patients whose catheters were removed before day 7 were retained in the descriptive analysis to better reflect the real-world use of LPCs in an acute-care setting. Functional and ultrasound outcomes, however, were evaluated only in patients who still had the catheter in place at day 7. Among the A-DIVA components, 77% of patients had a history of difficult cannulation, and approximately 65% had no visible or palpable veins. The median A-DIVA score was 3 (IQR 1–3).
Regarding procedural characteristics, the brachial vein was the most frequently cannulated vessel (53%), followed by the basilic (39%), cephalic (6%) and axillary veins (2%). The right arm was used in 80% of cases. Direct puncture was performed in 60% of procedures, while the pseudo-tunnel technique was used in 40%. Direct Seldinger technique was adopted in 90% of cases. The catheter tip was located distal to the axillary line in 72% of patients and at or proximal to the axillary line in 28%.
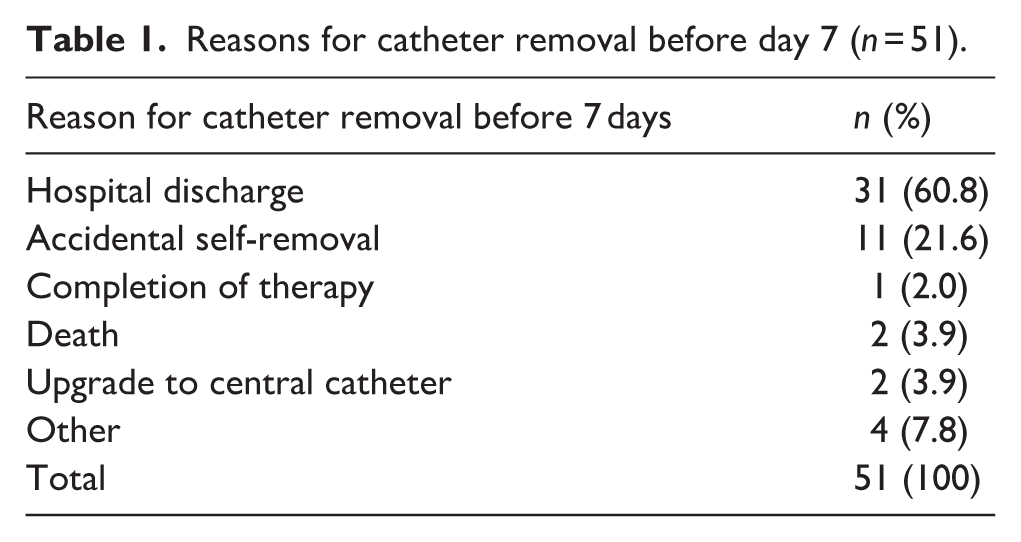
Among patients with early catheter removal (n = 51), the causes are reported in Table 1. The mean dwell time in this subgroup was 4.48 days.
Reasons for catheter removal before day 7 (n = 51).
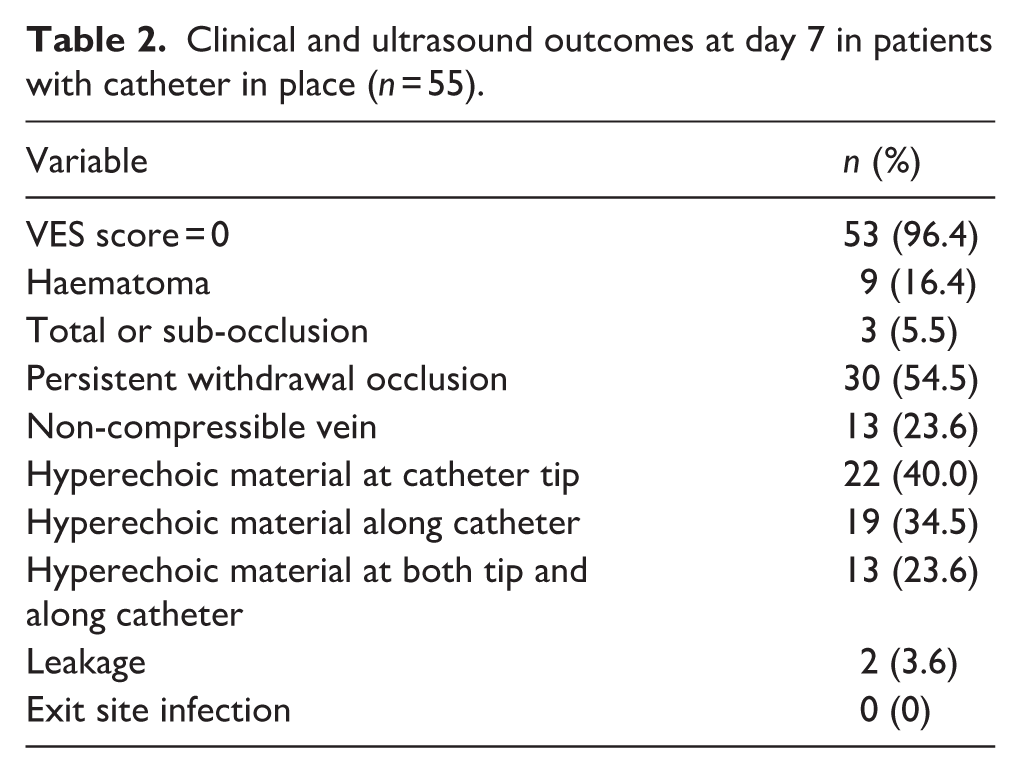
In the subgroup of patients with catheters still in place at day 7 (n = 55), PWO was the most frequent finding (54.5%), whereas total occlusion and sub-occlusion were uncommon (5.4%). Hyperechoic material at the catheter tip was observed in 40% of cases, while non-compressible veins were found in 23.6% of patients, as detailed in Table 2. Among the 30 catheters with PWO, total occlusion or sub-occlusion, 26 (86.7%) showed hyperechoic material either at the catheter tip or along the catheter body. Hyperechoic material was observed both at the tip and along the catheter body in 13 cases (50.0%), only at the tip in 8 (30.8%) and only along the catheter body in 5 (19.2%).
Clinical and ultrasound outcomes at day 7 in patients with catheter in place (n = 55).
Spearman correlation analysis between insertion technique (including pseudo-tunnel technique), tip location and post-insertion outcomes is presented in Table 3. No statistically significant associations were observed between procedural variables and ultrasound or functional outcomes (all p > 0.05).
Spearman correlation analysis between procedural variables and clinical outcomes in patients with catheter in place at day 7 (n = 55).
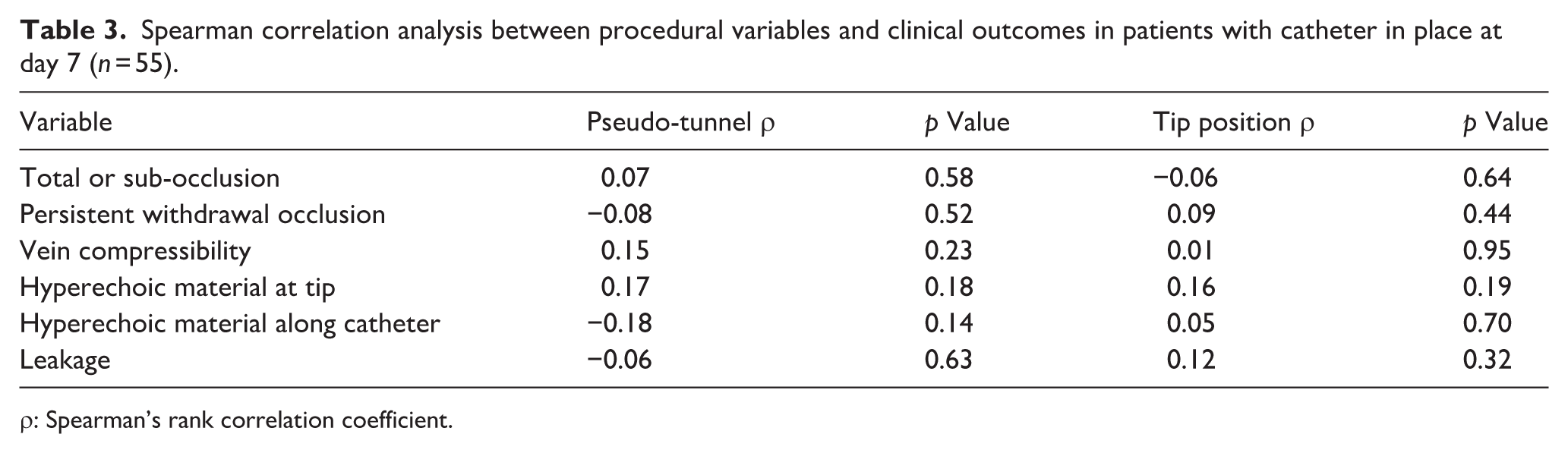
ρ: Spearman’s rank correlation coefficient.
Discussion
This observational study examined short-term clinical outcomes of LPCs, focussing on functional complications and their association with insertion techniques and tip location. Notably, more than half of the evaluated catheters (54.5%) exhibited dysfunction in withdrawal, limiting their utility for venous blood sampling. These findings are consistent with existing consensus recommendations, such as ERPIUP, which emphasise the contraindication and limited suitability of LPCs for blood sampling. 8
The presence of non-compressible veins (23.6%) and hyperechoic material at the catheter tip (40%) may reflect thrombotic phenomena or fibroblastic sheath formation, although a definitive distinction was not possible within the study design.18,19 These ultrasound findings were frequently observed in association with functional alterations including PWO or occlusion; however, no statistically significant correlations were demonstrated, and no cases required additional pharmacological treatment (such as anticoagulant therapy) during indwelling time or following catheter removal.
Different insertion and Seldinger techniques were adopted according to venous anatomy, without evidence of increased complication rates at 7 days.
No statistically significant associations were observed between procedural variables and short-term outcomes; however, the limited sample size and the exploratory nature of the analysis preclude definitive conclusions regarding potential predictors of LPC dysfunction. The pseudo-tunnel technique was adopted in 40% of insertions, mainly in patients with limited superficial venous availability, and was not associated with a higher rate of short-term functional or ultrasound abnormalities.13,20,21 However, the study was not designed to specifically evaluate the efficacy or safety of this technique, and dedicated prospective studies are warranted.
Overall, LPCs may represent a useful less invasive alternative to midline catheters in selected patients requiring short-term therapy and presenting with difficult venous access. However, the limited functional longevity and suboptimal performance for blood withdrawal warrant careful patient selection and close follow-up. These findings contribute to the ongoing refinement of peripheral vascular access strategies within a vessel health and preservation framework. Although no data on cost-effectiveness or nursing workload were collected in the present study, LPC use in DIVA patients may potentially reduce repeated SPC insertion attempts and the associated procedural burden related to peripheral venous access failure.
This study presents several limitations, foremost among them the small sample size and the retrospective nature of the analysis. The relatively small sample size limited the statistical power of the analyses and the possibility of identifying clinically relevant associations. Because functional and ultrasound assessments were only feasible in catheters still in place at day 7, the outcome analysis may have been influenced by survivorship bias. The study design did not allow for monitoring beyond 7 days, nor did it permit distinction between thrombosis and fibroblastic sheath formation in cases of venous hyperechogenicity and non-compressibility. Although LPCs were intended for therapies compatible with peripheral administration, 22 inadvertent infusion of drugs requiring central venous access cannot be completely excluded. This may have contributed, albeit marginally, to the findings of non-compressible veins or hyperechoic material at the catheter tip. Because of the retrospective design, data regarding rescue manoeuvers, additional venipunctures or catheter replacement following withdrawal dysfunction were not systematically available. Further studies are needed to better clarify the clinical performance of LPCs. Because these devices are frequently positioned in relatively small-calibre veins, they may be more exposed to complications related to lower blood flow and higher catheter-to-vein ratios at the tip level. Recent comparative studies suggest that, although LPCs remain a useful option for short-term vascular access, midline catheters may provide better functional performance and lower catheter-failure rates when dwell times exceed approximately 7–10 days, especially in patients requiring prolonged or intensive intravenous therapy.23,24 At the same time, LPCs may retain practical advantages related to their easier and faster insertion. 25 Future studies should also explore the organisational and cost implications of LPCs compared with MCs in different clinical settings.
Conclusion
LPCs represent a valuable option for peripheral venous access in patients requiring short-term therapy, particularly in the presence of difficult intravenous access. The pseudo-tunnel technique may be a feasible option in selected anatomical conditions, although this aspect requires dedicated investigation. However, after approximately 1 week of use, LPCs are associated with a high rate of functional limitations, particularly affecting blood withdrawal. These findings highlight the importance of appropriate device selection and careful clinical monitoring to optimise outcomes and minimise device-related complications.
Footnotes
Author contributions
Stefano Elli: conceptualisation, methodology, formal analysis and original draft – writing. Dario D’Amata: conceptualisation, methodology, formal analysis and original draft – writing. Noemy Francesca Lenti, Chiara Brunello, Lisa Invernizzi and Angelo Ascione: data collect and statistical analyses. Inga Berliba and Lin Jingyi: data collect, review and editing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the local Ethics Committee (Comitato Etico Territoriale Lombardia 3; approval date: March 11, 2026).