
Abstract
Attention-deficit hyperactivity disorder is a neurodevelopmental disorder characterised by persistent inattention, hyperactivity, impulsivity, and executive dysfunction. While commonly associated with childhood, attention-deficit hyperactivity disorder often persists into adulthood and poses significant challenges in various aspects of life, leading to negative self-perceptions, decreased quality of life, and increased risk of comorbid mental health conditions. There is a desperate need for more research about attention-deficit hyperactivity disorder from a Māori (Indigenous peoples of New Zealand) perspective. Considering the limited research, this article introduces the metaphor of the pīwakawaka (New Zealand Fantail) as a culturally grounded way of conceptualising attention-deficit hyperactivity disorder from a Māori perspective. The pīwakawaka’s characteristics, including its quick movements, curiosity, and ability to adapt to changing environments, mirror certain aspects of attention-deficit hyperactivity disorder.
Keywords
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterised by inattention, hyperactivity, and impulsivity. While ADHD was believed to affect children primarily, recent research has shown that a significant proportion of cases persist into adulthood, affecting 2.5% (Simon et al., 2009; Song et al., 2021) or 2% to 3% of adults (Williams et al., 2023).
However, in Aotearoa (New Zealand), the public health system does not adequately support adult ADHD diagnosis, except in some exceptional cases; as a result, many adults with undiagnosed ADHD turn to private psychiatrists for diagnosis (Rangiwai, 2023). This article explores the definition and diagnosis of ADHD, its characteristics in adults, and the need for a Māori (Indigenous peoples of New Zealand) perspective on ADHD. Furthermore, this article introduces the metaphor of the pīwakawaka (New Zealand Fantail) to conceptualise ADHD from a Māori perspective.
Ko wai au: who am I?
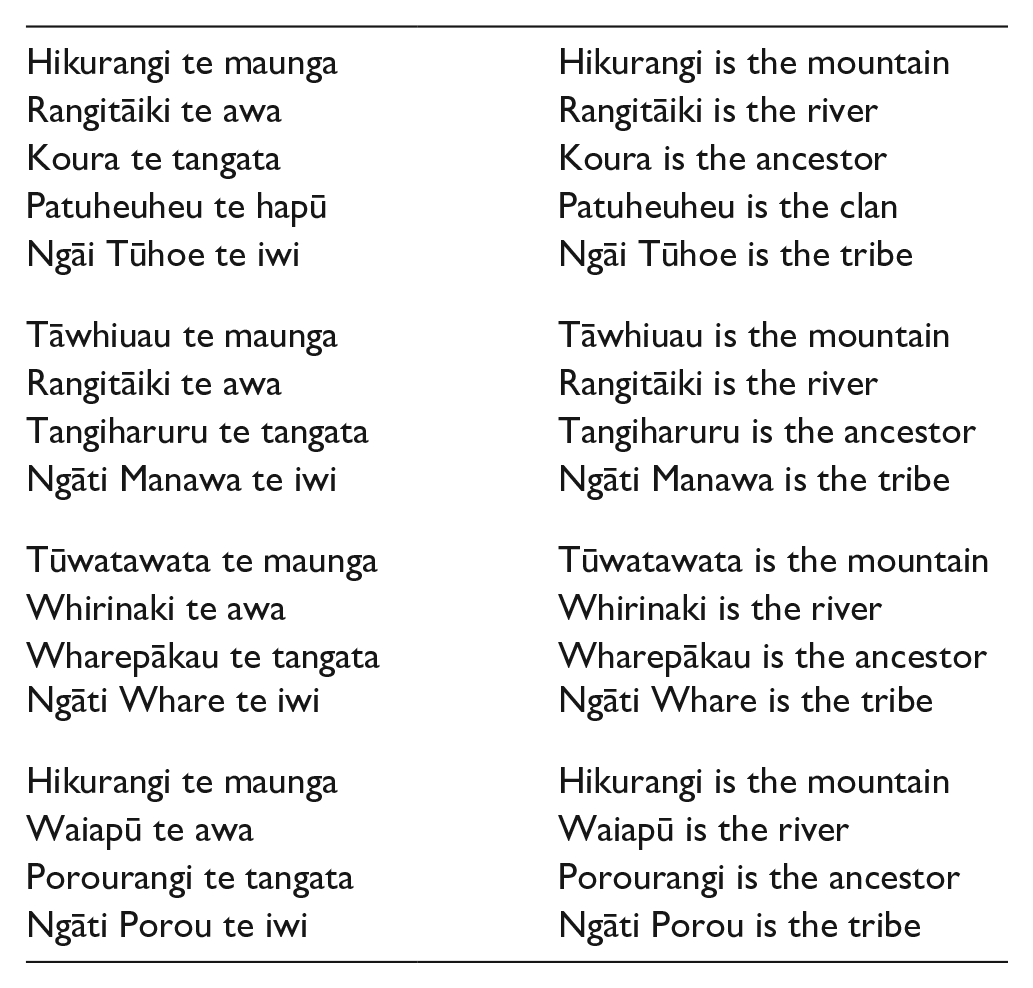
In the Māori world, it is customary to introduce oneself using pepeha or tribal aphorism (Rangiwai, 2015). The four pepeha above are cultural expressions—declaring landscapes, bodies of water, and ancestries—that vocalise the whakapapa (genealogy) or genealogical parameters within which my identity is located: “These mountains and rivers are, to me, living beings, and my tīpuna (ancestors) are alive in my veins” (Rangiwai, 2019, p. xx).
I was born in Gisborne and raised in Murupara and Waiōahau. My school reports featured low grades and myriad comments from teachers such as “Byron is a bright child but needs to focus” or “Byron is a delight to have in the classroom but needs to follow instructions more carefully” (Rangiwai, 2023, p. 1). I now realise that one of the key factors contributing to my struggles was undiagnosed ADHD.
Undiagnosed ADHD profoundly affected my ability to concentrate and stay focused in the classroom; I remember many instances of being easily distracted by the slightest noise or visual stimuli, making it extremely difficult to understand and absorb learning material (Rangiwai, 2023). In addition, my impulsivity often led me to act without thinking, causing me to rush through assignments, blurt out answers, or make careless mistakes (Rangiwai, 2023).
As a result of my struggles at school, my self-esteem suffered greatly; I began to doubt my intelligence and capabilities, internalising the belief that I was not good enough (Rangiwai, 2023). Seeing my grades declining despite my best efforts to improve was disheartening; this downward spiral created a cycle of negativity, further exacerbating my ADHD symptoms and making it even more challenging to break free from the pattern of underachievement (Rangiwai, 2023).
Despite the potential others saw in me, I left high school with just a School Certificate, Year 11, in English, and a Sixth Form Certificate, Year 12, in English, with the very bare minimum requirements met for each qualification (Rangiwai, 2023). I had dreamed about attending university but lacked the qualifications to enter, so I worked instead following high school (Rangiwai, 2023).
I attended university as a mature student once I turned 20; I started and failed many courses and papers and have a substantial student loan debt to prove it (Rangiwai, 2023). I fantasised about becoming a lawyer or some highly paid corporate, but I needed to possess sufficient ability to focus to succeed in exams (Rangiwai, 2023). I eventually graduated with a Bachelor of Arts—majoring in education studies, which, as it happens, was an entirely internally assessed major, meaning that I would not need to sit exams—from the University of Waikato in the early 2000s, but my grades were very erratic (Rangiwai, 2023).
Following my undergraduate degree, I tried and failed to study several other qualifications; however, once I lost interest or confidence in my abilities, I would withdraw from a course or stop attending altogether (Rangiwai, 2023). However, a family tragedy took me home to Waiōhau, and it was in Whakatāne, 45 km away, at Te Whare Wānanga o Awanuiārangi (tribal university), in the Master of Indigenous Studies programme, that I found my academic voice (Rangiwai, 2010, 2015, 2023). Here, I was exposed to Kaupapa Māori (by Māori, for Māori) theory and had access to the academics who developed it initially. I had never seen so many Māori academics in one place, and it was both validating and encouraging as I could see myself, as Māori and Indigenous, in the faces of the faculty (Rangiwai, 2023).
I quickly discovered that postgraduate study suited me because I could choose the topic and focus on the arguments I wanted to advance (Rangiwai, 2023). Success in the master’s programme eventually led to successful doctoral study; while my late success will hopefully encourage others, I often think about what could have been if I had been diagnosed with ADHD earlier in life (Rangiwai, 2023). Of course, ruminating about this—a typical feature of ADHD, by the way!— is pointless, except if it helps someone else realise that early intervention may benefit academic success (Henning et al., 2022).
Since 2017, I have worked in academia. I have taught at both undergraduate and postgraduate levels. Being an academic is already challenging, requiring high levels of focus, organisation, and attention to detail; however, when coupled with undiagnosed ADHD, the difficulties can be overwhelming and often misunderstood (Rangiwai, 2023). One of the primary difficulties of being an academic with undiagnosed ADHD is struggling with sustained attention; ADHD can make it incredibly challenging to focus on tasks requiring extended periods of concentration, such as reading dense academic texts or conducting research (Rangiwai, 2023). I was frequently and easily distracted and struggled to start and complete boring tasks, and because of undiagnosed ADHD, I had to push myself even harder to succeed (Rangiwai, 2023).
I was diagnosed with ADHD in May 2023. In Aotearoa, assessment of adult ADHD is not sufficiently supported by the public health system, except in some instances (Rangiwai, 2023). Adults living with undiagnosed ADHD often need to seek diagnosis through a private psychiatrist at a high cost. My experience of the ADHD assessment and diagnosis process aligns with the advice provided by Beehyve (2022)—an Aotearoa-based online support hub for those living with ADHD—which asserts that the public health system will essentially only support the assessment and diagnosis of adults whose ADHD symptoms are incredibly debilitating. As my ADHD symptoms were not severe enough to warrant public health system support, I sought a referral from my general practitioner (GP) to seek assessment and diagnosis from a private psychiatrist.
ADHD definition and diagnosis
Attention-deficit hyperactivity disorder is a neurodevelopmental disorder characterised by varying clinical manifestations, encompassing inappropriate levels of inattention, hyperactivity, and impulsivity (Rosso et al., 2023; Scholz et al., 2023). Attention-deficit hyperactivity disorder is linked to a higher risk of coexisting psychiatric disorders and significant cognitive and executive function difficulties (Biederman et al., 2006; Boonstra et al., 2010; Fuermaier et al., 2015, 2022; Gjervan et al., 2012; Kooij et al., 2012; Onandia-Hinchado et al., 2021; Torgalsbøen et al., 2021; Tucha et al., 2017). Although it was previously believed to affect children principally, recent studies indicate that a substantial proportion of cases persist into adulthood, affecting approximately 2.5% (Simon et al., 2009; Song et al., 2021) or 2% to 3% of the population (Williams et al., 2023).
The number of adults seeking assessment for ADHD has increased significantly due to an improved understanding of the disorder and the advantages—such as medication and specialised therapy—of receiving a diagnosis (Paris et al., 2015; Song et al., 2021). Given that childhood diagnosis may prevent the development of other comorbidities, early diagnosis may be an advantage (Tal & Goodman, 2023). Therefore, it is imperative to give thorough attention to the assessment phase to ensure accurate identification of individuals with this neurodevelopmental disorder (Rosso et al., 2023). From a neuropsychological standpoint, greater emphasis should be placed on standardised tools that enhance the diagnostic precision of adult ADHD assessments, mainly when there is suspicion of overlapping symptoms or comorbid psychiatric conditions (Rosso et al., 2023). More than 80% of adult ADHD patients have concurrent psychiatric disorders such as major depression, anxiety disorders, bipolar disorder, personality disorder, and substance or alcohol abuse (Grazioli et al., 2019; Katzman et al., 2017; Mucci et al., 2019; Xenaki & Pehlivanidis, 2015). Consequently, distinguishing ADHD from other clinical disorders represents the most challenging aspect of diagnosing ADHD in adults (Luo et al., 2019; McGough et al., 2005; Whlstedt et al., 2009).
I was diagnosed with depression more than 10 years ago, a diagnosis which, at first, was attributed to an earlier diagnosis of type 2 diabetes, as those with diabetes experience depression at twice the rate of those without (Sartorius, 2018). However, ADHD and depression are also closely connected (Skymba et al., 2023), so it could be the case that my depression stems from diabetes, ADHD, and possibly other factors, too. To further complicate things, recent studies show that those living with ADHD are at increased risk of developing type 2 diabetes (Garcia-Argibay et al., 2023). There is a need for more research in this area, particularly about Māori experiences of ADHD (Rangiwai, 2023) and its associated and complex comorbidities (Vitiello et al., 2024). Furthermore, a clinical psychologist first thought I may have had bipolar disorder rather than ADHD. Whereas a psychiatrist—with a specialisation in ADHD—diagnosed me with ADHD during the first session, highlighting, as Ryan (2023) argues, the need for more psychiatric training and expertise in ADHD, specifically adult ADHD.
The clinical assessment for diagnosing ADHD, as outlined in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013), relies on behavioural criteria and does not necessitate psychometric testing. Nonetheless, objective measures are frequently employed in the routine evaluation of individuals during ADHD diagnostic assessments (Rosso et al., 2023). Specific neuropsychological tests have been recommended as suitable measures for ADHD assessment (Fuermaier et al., 2019; Marshall et al., 2021), although the inclusion of cognitive assessment in the diagnostic process is still subject to debate (Barkley, 2019; Lange et al., 2014; Mapou, 2019).
As part of the ADHD assessment process, I was first asked to complete an ADHD Self Report Scale (ASRS) self-reported questionnaire designed to help the person being assessed describe experiences of potential signs and symptoms of ADHD (McManus et al., 2024). The ASRS results indicated a need for further objective testing, so I was also asked to complete a 40-min online test from Creyos (https://www.creyos.com), which consisted of 13 gamified assessments targeting working memory, reasoning, verbal skills, and focus (Hennessy et al., 2024). The Creyos assessments included Spatial Span, Grammatical Reasoning, Double Trouble, Odd One Out, Monkey Ladder, Rotations, Feature Match, Digit Span, Spatial Planning, Paired Associates, Polygons, Token Search, and the Sustained Attention to Response Task (Hennessy et al., 2024). The Creyos platform caters to a wide age range and holds a substantial database of 4.5 million scores from about 400,000 users (Hennessy et al., 2024). The results of my Creyos screening assessment indicated to the psychiatrist that my brain worked in ways that did not align with some of my achievements in later life, such as completing two PhDs and publishing journal articles—of which this article is another! What seemed to surprise the psychiatrist the most was how impaired my cognitive abilities appeared in the Creyos assessments, as my scores were overwhelmingly below average.
Attention-deficit hyperactivity disorder’s epidemiology and potential causes are complex, involving genetic, prenatal, and environmental factors (Kosaka et al., 2019; Leong & Graichen, 2024). Attention-deficit hyperactivity disorder symptoms arise from various factors, which include genetics, neurodevelopmental disorders, abnormal development of brain cells, brain injury, and exposure to the environment (Williams et al., 2023). Recent research conducted by Posner et al. (2020) discovered that environmental risks play a role in ADHD symptoms during different stages: before birth, around the time of delivery, and after birth. Factors such as prematurity, low birth weight, maternal smoking history, stress, trauma, and obesity during the prenatal and perinatal periods are strongly linked to ADHD (Williams et al., 2023). In addition, postnatal factors such as trauma, parenting style, artificial colours and fragrances, pollutants, and pesticides can worsen ADHD symptoms (Yadav et al., 2021).
Diagnosing ADHD is challenging due to hidden coping strategies—commonly referred to as “masking” and which involves suppressing one’s neurodivergent behaviours to appear “normal” (Kosaka et al., 2019; Leong & Graichen, 2024)—and symptom similarities with other frequently diagnosed disorders (Williams et al., 2023). I would have masked my ADHD most of my life. However, as I have aged, and following my ADHD diagnosis and consequent openness about my experience of living with the condition, my tendency to mask—a coping mechanism which causes significant stress and exhaustion for those with ADHD (Eagle & Ringland, 2023; Kosaka et al., 2019)—has diminished. I tell others, including potential employers, about my ADHD, and I include it on my curriculum vitae. I am now at a stage in life where I embrace the condition, and I expect that employers, in line with legislation—the Human Rights Act 1993 provides specific provisions to protect individuals from discrimination, including those with disabilities, while the Employment Relations Act 2000 allows for variations to working arrangements—will make the appropriate accommodations for me. In addition, I also include a note on my email signature which declares that I live with ADHD and may check emails less frequently to focus or that I may need reminders occasionally.
Treatment strategies involving medication have proven effective and affordable in the short term, with numerous available and widely recommended compounds (Williams et al., 2023). However, the long-term effectiveness of these treatments in terms of clinical, occupational, and social outcomes remains uncertain (Williams et al., 2023). There is an urgent need for improved long-term treatments for ADHD (Salvi et al., 2021). Concerning medication, I trialled several methylphenidate formulations and was eventually prescribed dexamphetamine. Of course, medication is only one part of the ADHD treatment puzzle, with other treatments, including psychoeducation, psychotherapy, and behavioural and environmental changes (Dobrosavljevic et al., 2023).
ADHD characteristics
Adults with ADHD often exhibit distinct characteristics that differentiate them from their neurotypical counterparts (Williams et al., 2023). Inattention is a common struggle for adults with ADHD (Ahlberg et al., 2023), as they find it challenging to sustain attention, stay organised, and complete tasks (Scholz et al., 2023; Worden & Tolin, 2023). Difficulties in following through on instructions, poor time management skills (Mette, 2023), frequent loss or misplacement of items (Worden & Tolin, 2023), forgetfulness, fidgeting, and impulsivity (Rivas-Vazquez et al., 2023) are also common manifestations of this characteristic. I have experienced all of the abovementioned struggles living with ADHD. However, I have developed—and continue researching and developing other strategies—to cope with these impacts. Some of the methods I have used include writing things down, making lists, using diaries, whiteboards, and timers, to name a few.
While hyperactivity tends to decrease in adults compared to children, some individuals with adult ADHD may still experience restlessness, fidgeting, and a constant need for movement (Rivas-Vazquez et al., 2023; Worden & Tolin, 2023). Sitting still for extended periods and engaging in activities requiring sustained mental effort can be particularly challenging for them (Rivas-Vazquez et al., 2023; Worden & Tolin, 2023). I struggle daily to sit still. My hands and feet seem to have a life of their own, and I tend to want to stand up and move even when doing so is inappropriate. It takes tremendous mental energy to keep my body still when required.
Impulsivity is another prominent characteristic of adult ADHD (Vizgaitis et al., 2023). This impulsivity can manifest through impulsive decision-making (Chen et al., 2023), blurting, interrupting others during conversations (Majarwitz & Perumareddi, 2023), and speaking before thinking (Dohrmann & Schneider, 2023). The drive to be impulsive is difficult, but not impossible, to manage. For me, impulsivity, like the other aspects of ADHD symptomatology, can be managed with strategies, self-care, therapy, mindfulness, and many different ways. I often want to speak too much or interrupt others when they are speaking; the urge to do so seems to come from a sense that if I do not say what is on my mind, then I will completely forget what I want to say. To mitigate this impulse, I try to note down what I want to say on a notepad so I can return to it. I have also been described as a person who speaks without a filter. This facet of ADHD can be embarrassing and causes stress and worry about the things that have been said yesterday, last week, or even years ago.
Individuals with adult ADHD may face relationship conflicts, engage in risky behaviours (Halbe et al., 2023), and struggle with managing their emotions effectively (El Archi et al., 2023; Gillioz et al., 2023; Tan et al., 2023). Frustration, irritability, and impatience are common, posing challenges in interpersonal relationships (Modesto-Lowe et al., 2023). My impatience and emotional reactions can often seem disproportionate or “over the top”. However, with the help of cognitive behavioural therapy and other treatments, I can manage the facets of ADHD more effectively.
Executive dysfunction is a prevalent challenge for many adults with ADHD (Skymba et al., 2023). Planning, organising, and prioritising tasks may be complex, making it hard to start and complete projects, manage time effectively, and set and achieve goals (Ogrodnik et al., 2023). While I certainly do have issues with executive function at times, I can manage these, for the most part, with medication, strategies, and therapy. I have found that it is much easier to complete a task when I am passionate about it. In contrast, I find it incredibly difficult when I perceive a task as tedious. So, I use strategies, such as using interesting tasks as a reward for completing uninteresting tasks, or switching rapidly between tasks, using a timer to measure chunks of time for each.
Adults with ADHD face many challenges that impact various aspects of their lives (Kenter et al., 2023). Maintaining stable relationships can be problematic due to poor impulse control, forgetfulness, and communication difficulties (Ginapp et al., 2023). Occupational problems may arise as the symptoms of adult ADHD interfere with work performance, affecting meeting deadlines, staying organised, and maintaining focus (Martin et al., 2023). Similarly, those pursuing further education may encounter challenges related to studying, organisation, and time management, which can impact academic performance and completion of coursework (Oram et al., 2023). In addition, adults with ADHD are more susceptible to co-occurring mental health conditions (El Archi et al., 2023; Hartman et al., 2023), and the challenges associated with ADHD can contribute to low self-esteem, frustration, and difficulty coping with daily stressors (Bodalski et al., 2023). My experience of ADHD reflects the many facets of this complex and multilayered condition, and I hope that sharing my lived experience will help others, particularly Māori and other Indigenous peoples.
Māori perspective
There is an immense chasm in the literature about ADHD from a Māori perspective and only two articles which attempted to describe ADHD from a Māori perspective were found, which indicates a dire need for more research. This reflective article, I hope, will be a stepping stone for others to use as they traverse these complex, misunderstood, and all-too-often stigmatising waters.
In the context of the Mahi a Atua (work of the gods; a Māori approach to mental health) approach (Kopua et al., 2020) to Māori mental health, Rangihuna et al. (2018) attribute ADHD behaviours to a Māori deity (Rangiwai, 2019, 2022a, 2022b) named Uepoto (one of the youngest children of the Māori deities, Papatūānuku [the earth] and Ranginui [the sky]): Imagine the distress felt by a defiant and hyperactive 8-year-old boy who was falling out with his parents, failing at school, forbidden from the skating rink and the Time Out studio for troublesome behaviour, and then diagnosed with attention deficit hyperactivity disorder (ADHD) and told by the paediatrician that “we are giving you medicine to control your unacceptable behaviour.” In contrast, what if he had been compared, during a multidisciplinary team consult, to a curious and impish Māori Atua (deity) called Uepoto, who had himself veered out of control but had found his pathway forward with solid support from his own family of gods? This somewhat less distressed boy is then told by the therapeutic team working with him and his whānau (family group) that “we will all band together to help you make it on this journey.” (Rangihuna et al., 2018, p. 16)
In another article, Cherrington and Rangihuna (2000) associate the fluctuating symptomatology of ADHD, conduct disorders, and anger issues to the Māori deity, Tāwhirimātea (one of the older sons of Ranginui and Papatūānuku, and personal name of the deity of the wind): Every story contains key messages, storylines, and atua (deity), which the listener can identify with. For example, the creation story of Ranginui (the sky) and Papatūānuku (the earth) presents a story of whānau separation. We see examples of whānau conflict, differing opinions, and separation issues in the story. Characteristics of atua can also be used as role models of human behaviour. The atua of the wind, Tāwhirimātea, is often used as an external example to discuss anger problems, conduct disorder, and ADHD. This is because, on some days, Tāwhirimātea is fine, clear, and calm. However, on other days, Tāwhirimātea sends tornadoes, hurricanes, and cyclones as revenge on the descendants of those who betrayed him. (Cherrington & Rangihuna, 2000, p. 3)
There exists a significant gap in the literature about Māori perspectives on ADHD as well as ADHD strategies and treatments that align with a Māori worldview. While there is a tremendous amount of work that needs to be done in this field, Māori approaches such as pūrākau or Māori stories (Clifford, 2023), for example, may be beneficial for Māori who live with ADHD. By combining mātauranga Māori and Western psychology, pūrākau may be used as a healing modality in the context of mental health to assist in managing emotional pain and sorrow, nurturing the cultural, psychological, and interpersonal dimensions of wellness, and actively enhancing the comprehensive healing journey, pūrākau embodies a holistic and impactful approach to therapy (Clifford, 2023).
Pīwakawaka behaviour as a metaphor for ADHD from a Māori perspective
The literature has a vast gap concerning how ADHD is understood from a Māori perspective. As Western literature on ADHD seems to describe the condition—and the words deficit and disorder prove this—in deficit terms. However, Kaupapa Māori theory can be used to reclaim, reframe, and realise Māori ways of knowing and being (Rameka, 2021; Rangiwai et al., 2023; L. T. Smith, 2021; H. Smith et al., 2023). The metaphor of the pīwakawaka is intended to create a space for conceptualising ADHD from a Māori perspective and is a beginning point for reclaiming, reframing, and realising a Māori way of thinking about the condition. I have used the word pīwakawaka in this article because, as Wehi et al. (2019) note, it is one of the most used Māori terms for the bird.
Manu or birds played a critical role in traditional Māori life, providing sustenance (Rangiwai, 2021) and adorning chiefly individuals with their feathers; they were also seen as predictors of weather and future events (Keane-Tuala, 2015). Certain manu symbolised status and were associated with chiefs, and bird behaviour was believed to foretell fortune or death (Hemopo, 2021; Keane-Tuala, 2015). Aphorisms comparing people to manu were used to acknowledge and honour people, and birds were often named for their distinctive traits, sounds, and behaviours (Keane-Tuala, 2015). As birds and humans descend from the Māori deity Tāne (one of the older sons of Papatūānuku and Ranginui, and personal name of the deity of the forest), they are connected through whakapapa or genealogy, indicating an indissoluble bond from a Māori perspective (Funaki, 2023).
The pīwakawaka is a small-medium bird species native to Aotearoa (Heaphy & Cain, 2021), and variations are also found in Australia, Solomon Islands, Vanuatu, and New Caledonia (Amiot et al., 2014). The pīwakawaka has an average length of 15.5 cm (Parris & Schneider, 2009) and appears in two primary colour variations: black and pied (Atkinson & Briskie, 2007). Its tail feathers extend in an expanded, fan-like configuration (Mackinven & Briskie, 2014). Renowned for its distinctive physical attributes and idiosyncratic behaviours, the pīwakawaka is known by at least 19 different Māori names (Appendix 1) (Wehi et al., 2019).
Described as “flighty” (Metge, 1998, p. 4), pīwakawaka are known for their agility, constant movement, and dynamic flying skills. They dart through the air with great speed and agility, changing direction quickly (Troup, 2015). As aerial insectivores, pīwakawaka can catch and consume insects mid-flight (Miskelly & Sagar, 2008). Pīwakawaka typically breed from August to February (Powlesland, 1982), and breeding may begin as late as October (McLean, 1984). Pīwakawaka fearlessly defend their territories and nests, particularly during the breeding season (Heather & Robertson, 2015; Innes et al., 2022).
Any metaphor concerning the pīwakawaka must include the pūrākau (story) of Māui (a tipua [demigod] who believed that humans should live forever), Hinenuitepō (personal name of the deity of death and the underworld), and the pīwakawaka. Hinenuitepō, whose name means “the great woman of the place of the departed spirits” is both a child and wife of Tāne (Higgins, 2004, p. 61). Māui’s attempt to kill Hinenuitepō, as a means of cheating death was thwarted by the characteristically erratic behaviour of the pīwakawaka (Metge, 1998; Pouwhare, 2016).
Māui attempted to enter Hinenuitepō through her vulva and emerge victorious from her mouth (Higgins, 2004; Jahnke, 2013; Melbourne, 2000; Mika, 2021; Pouwhare, 2016). The pīwakawaka found Māui’s efforts so amusing that it “could not refrain from laughing, twittering and frolicking about,” disturbing the slumbering deity who promptly crushed Māui with her thighs (Melbourne, 2000, p. 32). Thus, creating a pathway of inevitable death for all humankind to follow (Higgins, 2004; Melbourne, 2000).
Ngāi Tūhoe (tribal group of the Bay of Plenty, North Island, New Zealand) more commonly refers to the fantail as tīrairaka. Recalling his memories of wānanga (a meeting where ancient Māori knowledge is discussed) held at Waiōhau marae in the late 1960s and early 1970s—which related the behaviours and sounds of the tīrairaka with the mastery associated with the wielding of Māori weaponry—Pouwhare (2016) describes the characteristics of the tīrairaka in the following ways: “cheeky, mischievous and disobedient”, “a bird that made peculiar sounds and squeaks”, “prowess at flight and quick movement”, and “prowess at aerodynamics as it appeared to change direction in mid flight” (p. 2).
Metaphorically relating pīwakawaka behaviour to ADHD from a Māori perspective, we can draw parallels between the two. Attention-deficit hyperactivity disorder, like the pīwakawaka, is characterised by alertness, liveliness, and vibrancy. Just as the pīwakawaka dart through the air with speed and agility, individuals with ADHD often exhibit a high level of energy and impulsivity, constantly changing direction in their thoughts and actions.
The pīwakawaka’s ability to catch insects mid-flight reflects the quick processing and apparent multitasking skills often seen in individuals with ADHD. They possess a unique way of engaging with the world, much like the pīwakawaka’s distinctive physical attributes and behaviours that set it apart from other birds.
Moreover, the pīwakawaka’s fearlessness in defending their territories and nests during the breeding season can be likened to the resilience and determination individuals with ADHD may display when faced with challenges. They may exhibit a strong sense of protectiveness over their personal space and strive to overcome obstacles, just as the pīwakawaka diligently guards its nest.
There are strengths associated with both the pīwakawaka and ADHD. The agility and dynamic flying skills of the pīwakawaka enable it to adapt swiftly to its surroundings. Similarly, individuals with ADHD often possess heightened creativity and the ability to think outside the box, making them excellent problem solvers and innovators.
The pīwakawaka’s constant movement and quick thinking allow it to thrive in its environment, exploring new territories and adapting to changing circumstances. Similarly, individuals with ADHD can harness their energy and adaptability to excel in dynamic and fast-paced settings, making them valuable assets in fields that require spontaneity, excitement, and flexibility.
The pīwakawaka’s mischievous and cheeky nature can be seen as a positive trait associated with ADHD. Individuals with ADHD often exhibit an imaginative and innovative spirit, bringing enthusiasm, humour, and novel perspectives to their interactions and endeavours.
Conclusion
The characteristics of adult ADHD, including inattention, hyperactivity, impulsivity, and executive dysfunction, significantly impact various aspects of an individual’s life. Relationships, work performance, and academic pursuits are often affected by the challenges associated with ADHD. Moreover, individuals with adult ADHD are more susceptible to co-occurring mental health conditions, further exacerbating their difficulties.
Due to a significant gap in the literature regarding ADHD from a Māori perspective, there is a desperate need for further research about ADHD diagnosis and treatment as it relates to Māori. The metaphor of the pīwakawaka provides a starting point for conceptualising ADHD from a Māori perspective, highlighting the unique traits and behaviours associated with this energetic and iconic manu (bird).
Footnotes
Appendix 1
Some alternate names for the pīwakawaka (New Zealand Fantail) (Wehi et al., 2019, p. 4).
hīrairaka; hītakataka; hīwai; hīwaiwaka; hīwakawaka; kōtiutiu; kōtiutiu; pīrairaka; pīrakaraka; pīrangirangi; pītakataka; pīwaiwaka; pīwakawaka; tīaiaka; tīaka; tīakaaka; tieaka; tīrairaka; tīrakaraka; tītaiwaka; tītakataka; tītakataka; tītīrairaka; tīwaiwaka; tīwakawaka.
Author’s note
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The author received no financial support for the research, authorship, and publication of this article.
Glossary
Aotearoa New Zealand
atua deity
Hinenuitepō personal name of the deity of death and the underworld; the great woman of the place of the departed spirits
Kaupapa Māori by Māori, for Māori
kōtiutiu New Zealand Fantail
Mahi a Atua literally, work of the gods; a Māori approach to mental health
manu birds, bird
Māori Indigenous peoples of New Zealand
mātauranga Māori Māori knowledge
Māui a tipua (demigod) who believed that humans should live forever
Ngāi Tūhoe tribal group of the Bay of Plenty, North Island, New Zealand
Ngāti Manawa tribal group of the Bay of Plenty, Murupara, Galatea and Kaingaroa areas, North Island, New Zealand
Ngāti Porou tribal group of the East Coast of the North Island, New Zealand
Ngāti Whare tribal group of the Bay of Plenty, Te Whāiti and Minginui areas, North Island, New Zealand
Papatūānuku the earth; wife of Ranginui and personal name for the deity represented by
pepeha tribal aphorism
pīwakawaka New Zealand Fantail
pūrākau Māori stories, story
Ranginui husband of Papatūānuku and personal name for the deity represented by the sky
Tāne one of the older sons of Papatūānuku and Ranginui, and personal name of the deity of the forest
Tāwhirimātea one of the older sons of Ranginui and Papatūānuku, and personal name of the deity of the wind
Te Whare Wānanga o Awanuiārangi
tipua a demigod
tīpuna ancestors
Uepoto one of the younger sons of Papatūānuku and Ranginui, and personal name for the deity associated with seeking light
wānanga a meeting where ancient Māori knowledge is discussed
whakapapa genealogy
whānau family group