
Abstract
First Nations families continue to endure profound trauma stemming from the disproportionately high rates of infant (<1 year old) removal, exacerbated by culturally unsafe practices and inadequate support from midwives. This scoping review examines existing literature on the experiences of First Nations families who experience removal of an infant, as well as the perspectives of midwives involved in these removals. A scoping review of online databases identified primary qualitative, or mix-method studies published between 2002 and 2025. Seven publications from Australia, Canada and the United States met the inclusion criteria. Five key themes emerged from the review: (1) The colonial legacy; (2) “It is because I am Aboriginal you know”; (3) The intense emotional toll; (4) No control and (5) The power of honesty. The findings highlight the pervasive absence of culturally safe practices during infant removals and reveal significant challenges midwives face in delivering culturally safe, women-centred care to First Nations families.
Introduction
Globally, rates of infant (<1 year of age) removals from families have risen sharply. In Aotearoa (New Zealand), there was a 33% increase in the number of infants entering out-of-home care within 3 months of birth between 2015 and 2018 (Keddell, 2019). In the United States, infants represented the largest population of new foster care entries, accounting for 21% in 2021 (U.S. Department of Health & Human Services, 2021). In Australia, the Australian Institute of Health and Welfare (Australian Institute of Health and Welfare, 2026) reported that as of June 2024, approximately 20,000 Aboriginal and Torres Strait Islander children were living in out-of-home care. Among these, 21 per 1,000 were infants, a rate more than four times higher than the national average of 4 per 1,000 for infants across Australia. Nationally, out-of-home care is defined as ‘overnight care for children aged under 18 who are unable to live with their families due to child safety concerns, and where the carer receives a financial payment’ (Australian Institute of Health and Welfare, 2026). Importantly, elevated rates of out-of-home care for First Nations infants are not unique to Australia. Similar patterns are evident among other First Nations populations globally, reflecting broader systemic issues rooted in colonial histories and ongoing institutional inequities (Hyslop, 2021; Kenny et al., 2021).
Decisions and policies regarding the care of Aboriginal and Torres Strait Islander peoples in Australia were introduced by Commonwealth, state and territory governments to break culture and ‘westernize’ those who wanted to survive (Short, 2003; Turnbull-Roberts et al., 2022). Between 1910 and 1970 Aboriginal and Torres Strait Islander children were forcibly removed from their families and taught to forget their culture to blend in with Western society, and this became what is now referred to as the “stolen generations” (Funston & Herring, 2016). It is estimated that between three in ten and one in ten Aboriginal and Torres Strait Islander children were forcibly removed from their families under past government policies. These removals had enduring consequences, and it is said that every Aboriginal and Torres Strait Islander family has been impacted by these practices (Turnbull-Roberts et al., 2022).
It is well established within the literature that the impact of child removal can be extremely traumatic which not only affects the person directly affected, but can ripple throughout the family (Sankaran et al., 2018). Adverse outcomes include attachment issues, increased stress and disconnection from family and cultural identity. Intergenerational trauma and its long-lasting effects on First Nations peoples internationally are becoming increasingly recognised within academic literature (Isobel et al., 2021; Menzies, 2019). The outcomes of intergenerational trauma include, but are not limited to, mistrust of self and others, fear and anticipation of betrayal, experiences of shame and humiliation, loss of traditional values, desecrating land and institutions, violence including self-directed, risky behaviour and suicide (Gee et al., 2020; Menzies, 2019).
Despite the impact of discriminatory policies that led to the removal of Aboriginal and Torres Strait Islander children in the past, child removal persists in high numbers (Newton, 2020). Children are removed from family care when it is suspected or confirmed that the child is suffering from emotional, physical abuse and/or neglect (Australian Institute of Family Studies, 2025; Australian Nursing and Midwifery Federation, 2025). These reports of concern can be made by many professionals including midwives and nurses; however, these requirements do vary from different jurisdictions (O’Donnell et al., 2019). Due to the complexities of these issues, changes are needed within organisations, government, non-government bodies and local Aboriginal and Torres Strait Islander communities (Fisher et al., 2021). Supporting families through empowerment, early intervention, healing support and prevention tools need to be made a priority to prevent a repeat of history and further trauma (Fisher et al., 2021).
Cultural safety is a concept developed by Māori midwives and nurses in Aotearoa to foster partnership with Māori communities and address the racist attitudes and behaviours exhibited by health professionals. It aims to create a health care environment where Māori people feel respected, empowered and safe to access services without fear of harm (Best & Fredericks, 2021; Denison et al., 2014). There is currently no known literature that addresses culturally safe practices implemented during the removal of an infant (<1 year old) from First Nations families. However, several studies have addressed the absence of culturally safe approaches in such an intervention (Everitt et al., 2015; Newton, 2020; Wilson et al., 2015). Providing culturally safe care to Aboriginal and Torres Strait Islander Peoples plays an important role in closing the gap in many aspects of life (Fisher et al., 2021; Laverty et al., 2017), including the national target to reduce the overrepresentation of Aboriginal and Torres Strait Islander children in the child protection system (Australian Government., 2021). The National Framework for Protecting Australian Children (2021–2031) emphasises that achieving this goal requires transforming government organisations to identify and eliminate institutional racism and embed meaningful cultural safety in practice (Commonwealth of Australia & Department of Social Services, 2021).
The perspectives of midwives during the removal of an infant are also addressed in this scoping review as midwives play a unique role in maternal and newborn care. Globally, they are recognised as specialists in supporting pregnant individuals and promoting early life health outcomes (El-Ardat et al., 2025). An underpinning philosophy to midwifery internationally is women-centred care (Brady et al., 2024). A widely cited definition of women-centred care is provided by Leap (2009). This definition highlights the importance of addressing each woman’s unique needs, aspirations and expectations; ensuring choice, control and continuity of caregiver; and recognising the interconnected needs of the woman, baby, family and anyone else deemed significant to the woman. It also encompasses social, emotional, physical, psychological, spiritual and cultural needs and expectations and acknowledges the woman as the expert in decision-making (Leap, 2009). Understanding how midwives uphold the principles of women-centred care during the process of infant removal is a key area of interest and holds significance for the findings of this paper.
Midwives involved with a mother who had an infant removed at birth described the event as distressing and traumatic and spoke of the grief seen, similar to mothers who experienced perinatal loss (Everitt et al., 2015). The theme of grief is further reinforced by findings that show most parents who have experienced infant removal have histories of personal trauma, including being in out-of-home care during their own childhoods (Ross, 2017). Evidence shows that health professionals felt ill-equipped to work with Aboriginal and Torres Strait Islander patients, including managing the removal of Aboriginal and Torres Strait Islander infants (Wilson et al., 2015). Key challenges identified included a lack of helpful strategies, fear of being deemed racist or getting things wrong, and the challenges of navigating complex social and cultural realities faced by Aboriginal and Torres Strait Islander peoples.
This scoping review adopts an international lens to examine the experiences of First Nations peoples in countries with shared histories of colonisation, including Australia, Aotearoa, Canada, and the United States. Colonisation in these regions has resulted in the loss of land, language, and culture, alongside enduring systemic challenges such as racism, poverty, and discrimination (Maple-Brown & Hampton, 2020). In Australia, the colonisation of unceded land beginning in 1788 marked the onset of intergenerational disruption to Aboriginal and Torres Strait Islander kinship systems, a deeply sophisticated cultural structure that shapes identity, social organisation, and responsibilities across generations, and differs significantly from Western notions of family (Best & Fredericks, 2021; Morphy, 2006). Disruption to these kinship roles can have devastating effects on families and communities. This review focuses on the global experiences of First Nations families in relation to infant (<1 year old) removal, with particular emphasis on Aboriginal and Torres Strait Islander peoples in Australia. It is not the intention of this review to investigate child protection services including protocols of child removal. It explores qualitative and mixed-method research capturing the perspectives of families who have experienced infant removal, as well as midwives involved in the process. While literature in this area is expected to be limited, the insights gained will be invaluable for informing culturally safe, trauma-informed practices among health care professionals.
Note
This paper uses the terms Aboriginal, Aboriginal and Torres Strait Islander, First Nations, and Indigenous interchangeably. We acknowledge that preferences vary across geographies, communities, and individuals, and that these terms may not fully reflect the diversity of identities they aim to describe.
We also recognise that these terms are colonial constructs, shaped by imposed systems of classification. Their use here reflects common language in policy and research contexts, while affirming the importance of self-identification and Indigenous sovereignty.
Methods
A scoping review was selected as the most appropriate form of literature review as it has the capacity to systematically map existing literature, identify key concepts, enhance understanding of current knowledge and highlight potential gaps in the research (Peters et al., 2015). This was deemed more appropriate than a systematic review due to the diversity and complexity of the research topic, “First Nations families and midwives’ perspectives on infant removal in mainstream maternity settings”, which includes varied viewpoints and interdisciplinary evidence. A scoping review is particularly relevant for informing evidence-based health care as it helps integrate existing knowledge, systematically map available research and identify gaps (Aromataris et al., 2024).
This review was guided by the methodological framework developed by Arksey and O’Malley (2005), which included five key stages: (1) identifying the research question, identifying relevant studies, (2) study selection, (3) charting the data, and (4) collating, summarising, and (5) reporting the results. The authors acknowledged that conventional evidence-based practice is rooted in Western epistemologies, which may not align with Indigenous ways of knowing, being and doing. In response, the research team incorporated the critical perspectives presented by Luke et al. (2022), who question the ethical foundations of evidence-based practice within Indigenous health and social contexts in Australia. Upholding Indigenous methodologies, even within a scoping review is essential for producing knowledge through an anti-colonial, decolonising, and self-determining lens. This approach honours Indigenous ways of being, knowing, and doing, and actively challenges dominant discourses, traditions, and assumptions. The research team carefully considered the limitations identified by Luke et al. (2022) in constructing the review, ensuring that Indigenous perspectives were central to the process.
The authors acknowledge their ongoing work with decolonising research methods and recognise the importance of striving to use a decolonising lens. As stated by Durie (2004) this is fundamental when obtaining information from First Nations peoples as it engages authentic knowledge and stories. As this paper took form of a scoping review and no data were collected, the team discussed the importance of upholding Indigenous ways of knowing, being and doing which challenge the dominant Western paradigms. Hence, storytelling was adopted for this scoping review with the decision to not use quantitative data as this does not align with a decolonising lens and capture experiences in the same way. It was also important that only First Nations voices were interpreted in our results, as some of the included data were from both First Nations and non-Indigenous participants. No grey literature was identified in our search. The review was developed, registered and published with PROSPERO (National Institute for Health and Care Research [NIHR], 2024). By submitting the proposed research questions to a portal such as PROSPERO it minimises potential for bias and avoids unintended duplication of reviews (Stewart et al., 2012).
Study Population
The studies included in this review prioritise the experiences of First Nations families globally who have had an infant removed from their care and midwives who have been involved in infant removal from a First Nations family. The First Nations peoples included in the study were from Australia, Canada, the United States and Aotearoa. These groups were selected due to their shared experience of colonisation and comparable approaches to health systems and services (Maple-Brown & Hampton, 2020). It is also important to note the diverse, multicultural populations within these countries.
Defining the Research Question
The research question guiding this review was: “What are the experiences of First Nations families and midwives in relation to the removal of an infant from family care?” The experiences of First Nations peoples were explored in an international context, including countries with shared histories of colonisation, both historical and ongoing, as previously outlined. Midwives’ perspectives were included only if they had direct experience supporting First Nations families during the removal of an infant. This criterion was essential due to the disproportionate representation of First Nations families in infant removals and the profound historical and intergenerational trauma linked to these practices.
Study Selection
Two separate searches were conducted as part of the scoping review process. The initial search, completed in 2022, focused on identifying qualitative or mixed-method studies published in English between 2002 and 2022. Databases searched included PubMed, Scopus, EBSCO/CINAHL, ScienceDirect, Informit, and ProQuest.
In October 2025, an updated and more comprehensive search was undertaken to strengthen the review. This included searches across Medline, ProQuest, ScienceDirect, Scopus, PubMed, and PsycINFO. To ensure thorough coverage, Google Scholar and manual reference list checks were also used to identify additional relevant literature. Key concepts and the full search string are provided in the supplementary materials. A further two studies were found, and one was removed from the original search as it did not address the removal of a First Nations infant.
The scoping review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to minimise bias and ensure replicable findings (Moher et al., 2015). The study titles and abstracts were screened for relevance – Figure 1 shows the search and screening process. Full-text articles were then evaluated against the following inclusion criteria: (1) included the perspectives of First Nations peoples who had experienced the removal of an infant from family care, (2) the study was conducted in the following locations: Australia, Aotearoa (New Zealand), Canada, Kalaallit Nunaat (Greenland), United States and Sámi regions to reflect the transnational nature of Indigenous experiences and to capture diverse Indigenous perspectives across settler-colonial contexts, each with distinct but similar histories, policies, and cultural frameworks, (3) the health professionals featured in the study were midwives. It is important to note that the perspectives of extended family were included, as many First Nations families have diverse and strong kinship structures. Therefore, the experiences of relatives such as aunties and grandmothers are considered equally significant and appropriate to capture alongside those of mothers and fathers. Studies were excluded if they were: (1) an opinion article, (2) quantitative data only, (3) not a primary study, (4) not in the English language, (5) not identified as First Nations women, (6) not family or midwives’ perspectives and (6) not about the removal of an infant (under 1 year old).
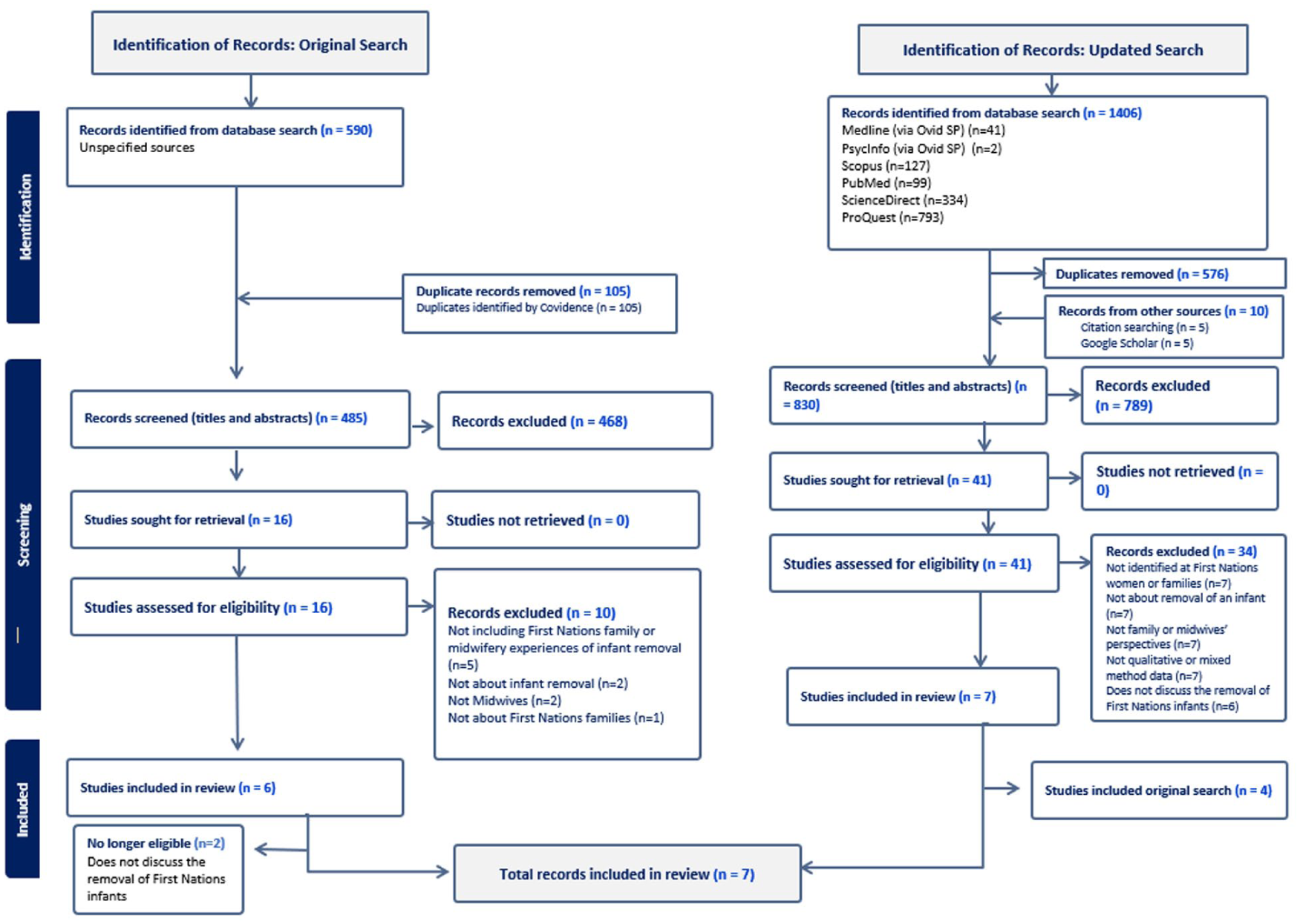
PRISMA flow chart.
Charting the Data
The research team comprised two Indigenous – Aboriginal and Sámi – and two non-Indigenous members. The team incorporated two Registered Nurses, one Registered Midwife and one Registered Nurse midwife researcher. Throughout this project, but especially during the analysis phase, researcher reflexivity and positionality were discussed within the team on an ongoing basis.
Prior to screening titles and abstracts, the inclusion and exclusion criteria were discussed at length by the team. Following the search, a total of 1406 studies were imported for screening into Covidence, with 576 removed as duplicates. Subsequently, 830 studies were screened at the abstract level by two reviewers (TJ and SS), with 41 full-text studies screened for eligibility. A further 34 articles were excluded due to not meeting the study criteria. Any conflicts were resolved by a collective meeting with a third reviewer (NS). The final number of articles included was seven.
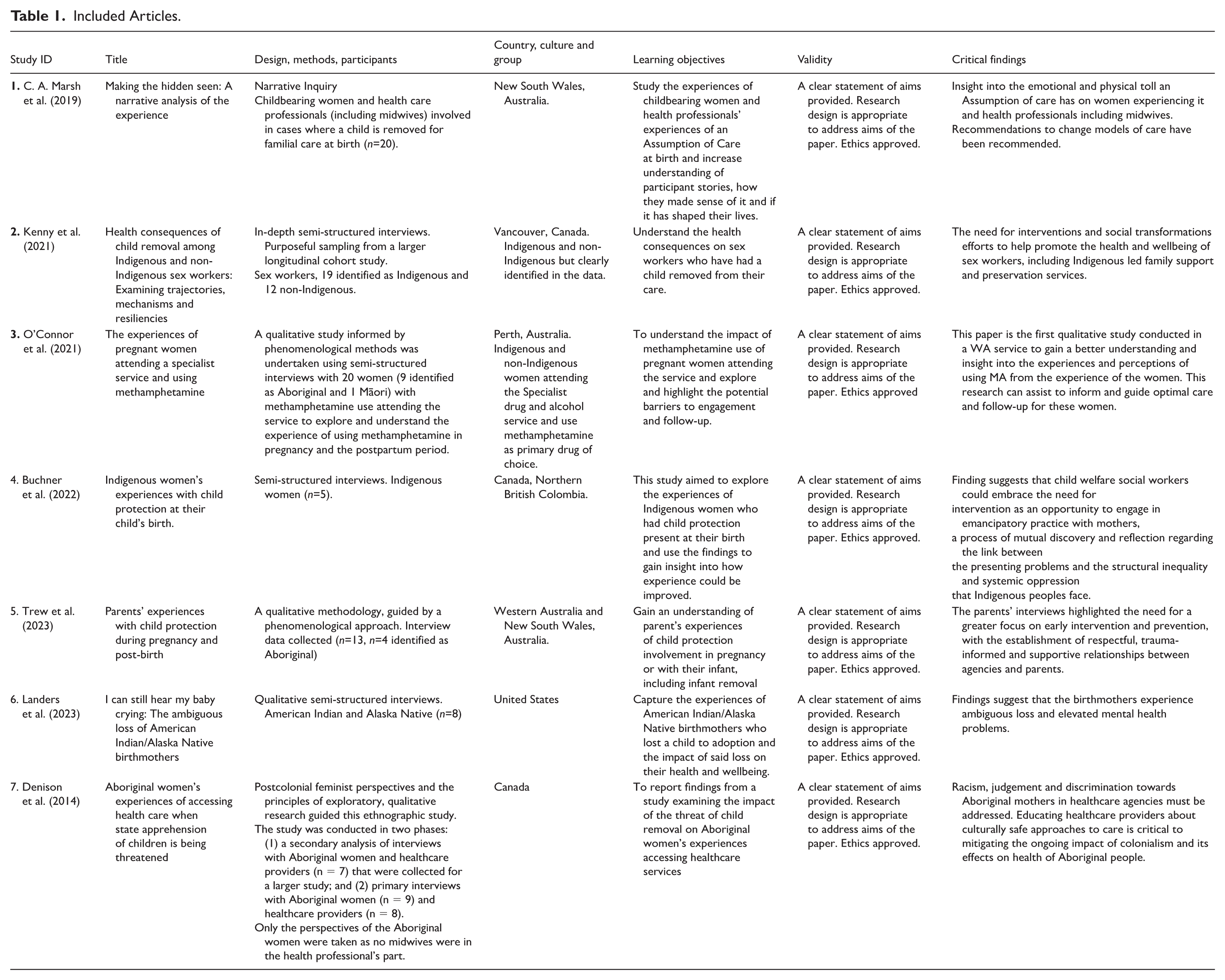
All studies (7) were identified for review using the PRISMA process (Page et al., 2021) – as outlined in Figure 1. Within the seven final articles there were a diverse range of families as described in Table 1. Families interviewed included families who had their infant returned to their care, families who did not have their infant in their care, families linked with agencies and families who lived in smaller rural communities. The midwives interviewed were from a metropolitan hospital in New South Wales, Australia.
Included Articles.
Setting
The studies that met inclusion criteria for the review included First Nations families from Australia (n = 3), Canada (n = 3) and the United States (n = 1). In addition, midwives from Australia who had been involved in cases of First Nations infant removal were also included to provide clinical perspectives on systemic practices (n = 1).
Key characteristics can be found in Table 1, with the study number, methodology, location where the research was conducted, learning objectives, validity and key findings.
Results (Collating and Summarising)
Seven papers were included in this scoping review with data obtained from four countries including Australia, the United States, Canada and New Zealand. Data were obtained from five cultural groups including: Aboriginal and/or Torres Strait Islander (n = 30), American First Nations – including the United States and Alaska (n = 8), Canadian First Nations (n = 19) and Māori (n = 1). Data were also obtained from 15 health care professionals including seven midwives (Buchner et al., 2022; Denison et al., 2014; Kenny et al., 2021; Landers et al., 2023; C. A. Marsh et al., 2019; O’Connor et al., 2021; Trew et al., 2023).
The reviewed studies collectively explore the complex and often traumatic experiences of First Nations women and families facing infant removal with one study also capturing midwives’ perspectives on such removals. Using qualitative methodologies such as narrative inquiry, phenomenology and ethnography, these studies span diverse contexts including Australia, Canada and the United States. Three of the final studies had First Nations and non-Indigenous participants, and they were selected for this review because they clearly distinguished and addressed First Nations experiences within their findings (Kenny et al., 2021; Newton, 2020; Trew et al., 2023). Similarly, the study involving health professionals included various roles, but for the purpose of this review, only the perspectives of midwives were considered (C. A. Marsh et al., 2019).
The final articles (n = 7) were thematically analysed by the research team (TJ, NS, SS) using the six steps of thematic analysis by Braun and Clarke (2006) which identified the main themes: (1) Colonial Legacy; (2) “It is because I am Aboriginal you know” (3) The intense emotional toll; (4) No control and (5) The power of honesty.
Reporting the Results
Theme 1: Colonial Legacy
A recurring theme across five studies involving both First Nations families and midwives was the deep resonance between contemporary infant removals and historical practices (Kenny et al., 2021; C. A. Marsh et al., 2019; Newton, 2020). Women described the removal of their infant as a continuation of the traumatic legacy experienced by First Nations families throughout history. Many expressed feelings of history repeating itself, and that professionals involved in their care lacked understanding of the historical and cultural significance of these removals. Several women felt discriminated against simply for being First Nations (Buchner et al., 2022; Denison et al., 2014).
Many families spoke about their experiences of being removed from their own parents, leaving them with no guidance when it came to parenting their own children (Denison et al., 2014; Kenny et al., 2021; Newton, 2020; Trew et al., 2023). This intergenerational trauma was seen as a contributing factor to the ongoing cycle of infant removals. Multiple articles highlighted the lack of support available for reconnecting families with their infants (Denison et al., 2014; Landers et al., 2023; C. A. Marsh et al., 2019; Newton, 2020; Trew et al., 2023). Barriers identified included systemic challenges, physical and emotional distance, ongoing trauma, burdensome requirements, feelings of shame and guilt and a lack of resources available throughout pregnancy. In several cases, child protection agencies were aware in advance that the infant would be removed at birth. However, in these cases, no support was provided for the mothers during pregnancy to discuss ways they could keep their baby or access rehabilitation services if needed.
All included articles addressed the socio-political context surrounding infant removal. Factors such as poverty, homelessness, trauma, being a young parent, domestic violence, mental illness and substance abuse were frequently cited. Many families were living in poverty at the time their infants were removed and struggled to secure housing or employment. Mothers who believed that they were doing everything they could to care for their infants still felt judged based on their appearance or living conditions, long before they had the opportunity to demonstrate their parenting capacity.
Theme 2: “It is because I am Aboriginal you know”
All included articles highlight the pervasive challenges First Nations families face within the child protection system (CPS), particularly around surveillance and discrimination. Families described feeling constantly watched and judged for their parenting, with some women even choosing to go ‘off grid’ to escape the pressure. The sense of being targeted was deeply felt, with many women expressing that First Nations infants were disproportionately removed from their communities. Participants emphasised that CPS workers often lacked understanding of First Nations culture and community dynamics, reinforcing the belief that First Nations women are unfairly singled out.
Women spoke of the intense anxiety experienced in pregnancy, fearing any misstep could be used against them (Buchner et al., 2022; Denison et al., 2014; Kenny et al., 2021; Landers et al., 2023; Newton, 2020; Trew et al., 2023). This constant scrutiny contributed to feelings of racial profiling and institutional racism, both within CPS and in hospital settings. The legacy of systemic racism which is rooted in historical abuses of First Nations families dates to the 1900s and was described as very much alive today. Both families and midwives acknowledge that these patterns continue to shape the experience of First Nations mothers.
Families also expressed that the systems they were forced to navigate felt inherently Westernised and incompatible with First Nations ways of parenting (Buchner et al., 2022; Landers et al., 2023; C. A. Marsh et al., 2019). Many felt that these structures were not designed to support their success but rather perpetuate cycles of removal and disempowerment. The lack of access to culturally safe health care further compounded these challenges, leaving families feeling isolated and unsupported.
Theme 3: Intense Emotional Toll
All included articles powerfully illustrated the profound emotional toll that infant removal has on both First Nations families and midwives. The grief experiences of mothers were described as enduring and life-altering. For example, one woman stated, “You’re never going to imagine how many years you’re going to live grieving; nobody tells you that part, that you never forget” (Woman) (Landers et al., 2023).
Women reported feeling a complex mix of emotions including grief, fear, anger, powerlessness, shame, numbness, and hopefulness. The trauma was so severe that some described the loss of basic life skills and sense of spiritual identity (Kenny et al., 2021). The hours’ following birth was especially intense. Mothers spoke of the disrespect they felt and the impossibility of expressing their emotions freely, fearing that any reaction could be used against them. For some, the trauma led to high-risk behaviours, driven by a sense of despair and detachment from their own wellbeing.
Midwives also reported extreme emotional strain (C. A. Marsh et al., 2019). They noted that when mothers were informed in advance about the removal, reactions were more measured. However, unexpected removals were described as deeply traumatic. All midwives agreed that their training did not prepare them for the emotional complexity of supporting families through infant removals. They spoke of the contradiction between their professional commitment to woman-centred care and the reality of witnessing removals, a conflict that created personal and ethical distress. One midwife stated that “Funerals are never easy, but going can provide a healing experience for closure. With ‘infant removal’ there’s a void, an empty space” (Midwife) (C. A. Marsh et al., 2019).
Midwives who witnessed the removals described feeling traumatised by the process and the lack of respect shown to the families. Unlike stillbirths, where they were offered time off and opportunities for closure, removals left them emotionally stranded. This lack of institutional support contributed to burnout and emotional exhaustion.
Theme 4: No Control
The overwhelming sense of powerlessness experienced by First Nations families during the process of infant removal was highlighted in all seven articles. Families described feeling confused about who they could trust within the system, including midwives and emphasised the importance of a trusting client-patient relationship. Yet many felt betrayed by those involved in their care, especially when removals occurred despite efforts to cooperate with authorities and subsequently families said they felt betrayed again. Many families felt immense disrespect from the people involved in their care when their infant was removed. They felt like they were being spoken down to and not deserving of respect. There were several examples of families working with the department to increase their chances of keeping their infants, but still ended up with their infants removed with no explanation. This led families to feel powerless in the decision-making process. Some reported that no matter how much they tried to work with authorities, they were never in with a ‘chance’. One woman stated, “They were filling paperwork to get him taken away when I was pregnant . . . all I did was worry about if they were going to take him away . . .” (Woman) (Denison et al., 2014).
Families reported feeling disrespected, spoken down to, and treated as undeserving of dignity. Even when they actively worked with CPS in hopes of keeping their infants, many still experienced removals without clear justification. This led to a deep sense of futility that no matter how hard they tried, they were never truly given a chance (Buchner et al., 2022; Denison et al., 2014; Trew et al., 2023). Women also described being left “out of the loop” regarding removal plans which intensified feelings of isolation and helplessness, especially when the removal was unexpected (C. A. Marsh et al., 2019). One woman stated, “You have to do what they want; they control everything . . . What they say goes or they take your kids.” (Woman) (Trew et al., 2023).
Midwives echoed these concerns, describing the emotional and ethical challenges of working with families under such conditions (C. A. Marsh et al., 2019). In some cases, midwives were legally required to withhold information about the impending removals, placing them in direct conflict with the philosophy of women-centred care. They expressed distress over situations they felt were unjust and questioned the rationale behind certain removals.
Poor communication from CPS was a recurring issue in all studies. Midwives reported feeling anxious and unprepared, especially when removals occurred suddenly without warning. In some instances, multiple CPS workers entered a woman’s hospital room within hours of birth with between one and seven social workers present within the first 12–24 hr post birth (C. A. Marsh et al., 2019). These abrupt and overwhelming interventions further eroded trust and compounded trauma for both families and midwives providing care.
Theme 5: The Power of Honesty
Across all articles both women and midwives emphasised that honesty in their interactions led to better outcomes. When transparency was absent, women felt deeply betrayed by the midwives they had come to trust, and midwives experienced significant professional guilt about withholding information which was often under legal or institutional pressure. One participant stated, ‘Look, we’re not taking your baby, she’s coming home with you’ . . . They led us to believe we’re keeping her . . . two Department workers . . . they handed me a piece of paper and said, ‘we’re taking your baby’. I was in shock . . . I felt like I was ambushed. (Woman). (Trew et al., 2023)
This lack of honesty created a climate of fear and mistrust. Women described feeling unsafe within the system, which discouraged them from seeking help even when they wanted it. The fear of consequences such as losing their infant led many to withhold critical information which impacted their care (Newton, 2020). Similarly, midwives found themselves in professionally inappropriate and emotionally distressing situations, often unaware of the impending removal (C. A. Marsh et al., 2019). When CPS withheld information, midwives felt their practice was compromised and their ability to provide woman-centred care undermined. This lack of communication created traumatic experiences not only for families but for the midwives themselves. Midwives agreed that early intervention and open communication between departments, health professionals and families could significantly alter outcomes. They believed that honesty and transparency could foster trust, enable bonding and motivate positive change and potentially prevent removals altogether (C. A. Marsh et al., 2019).
Discussion
This scoping review identified five interrelated themes across seven studies exploring First Nations families’ experiences of infant removals as well as midwives’ perspectives while caring for a First Nations family who experienced infant removal. In addition, this review also revealed systemic issues within child protection systems across Australia and internationally which disproportionately affect First Nations families. However, it was the express intention of this review to focus on the effects of child removal on families and midwives rather than address the shortcomings within CPS.
A key finding across the literature is the persistent lack of knowledge and cultural competency regarding First Nations history and kinship structures within health care and CPS. Historical disruptions to Aboriginal and Torres Strait Islander communities including forced removals, disconnection from kin and government policy aimed at assimilation continue to shape contemporary experiences of infant removal (Payne, 2024; Venables et al., 2025). Despite efforts to improve practice, the legacy of colonialism remains deeply embedded in institutional responses to First Nations families. The literature (Jones et al., 2019; Redvers et al., 2020; Venables et al., 2025) emphasises the importance of culturally informed care and historical awareness when working with Aboriginal and Torres Strait Islander peoples. The findings of this review support this, highlighting how the absence of culturally safe practices contributes to mistrust, trauma and disengagement from services. Families who are descendants of the Stolen Generations in Australia are particularly vulnerable, with evidence suggesting they experience significantly poorer health outcomes and are at higher risk of having their own children removed from their care which was addressed in the findings from this review (Menzies, 2019).
This review highlights the complex and often conflicted role midwives play in cases of infant removal when working with First Nations families. While there is existing literature on midwives’ experiences with infant removals (Everitt et al., 2015; W. Marsh et al., 2014; Mason et al., 2023; Wood, 2008), it is not specific to a First Nations context. This gap is significant, as the colonial legacy surrounding First Nations infant removals introduces unique cultural, historical and systemic dimensions that deeply shape both families and midwives’ experiences (Payne, 2024; Venables et al., 2025). The emotional toll is compounded by intergenerational trauma, institutional racism and culturally unsafe practices which are factors that are rarely addressed in mainstream midwifery research.
It is essential to recognise and build upon the work that is being done internationally to reduce removals of First Nations infants. In Australia, research has emphasised the importance of the five key elements of the Aboriginal and Torres Strait Islander Child Placement Principles; prevention, partnership, placement, participation and connection (SNAICC – National Voice for our Children, 2020). One example of action aligned with these principles is the redesign of maternity and neonatal services to ensure all parents have access to culturally responsive, trauma-integrated support during pregnancy, birth and early postnatal period (Chamberlain et al., 2022). Community-led continuity models are also showing promising outcomes in reducing infant removals in Aboriginal and Torres Strait Islander families (O’Dea et al., 2024).
Even though we did not have articles from Aotearoa that met the inclusion criteria, it is important to acknowledge the similar efforts underway to reduce First Nations infant removals. These include providing holistic care at organisational levels, developing culturally relevant services, particularly for Māori families and encouraging self-determination in service provision (Keddell et al., 2021). These international examples highlight the potential for systemic change when First Nations communities are empowered to lead and shape the care they receive.
In Australia, systemic reform is urgently needed in maternity settings to ensure culturally safe care for Aboriginal and Torres Strait Islander women and families. A key priority identified by the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM, 2024a) is the critical need to increase the number of Aboriginal and Torres Strait Islander midwives. The most recent workforce report recorded only 460 midwives identifying as Aboriginal or Torres Strait Islander, while an estimated 1,300 are required to reach workforce parity (CATSINaM, 2024b). Barriers to this goal include both interpersonal and institutional racism, a lack of cultural safety, and challenges related to balancing responsibility and financial pressures (Hartz et al., 2025; Springall et al., 2025).
A notable gap identified in this review is the absence of literature exploring the experiences of First Nations midwives involved in the removal of First Nations infants. Springall et al. (2025) documented the account of a First Nations midwifery student who was involved in such removal, highlighting the emotional and ethical complexities faced. This reinforces the need for culturally responsive support and debriefing processes. Addressing this gap is critical, as these experiences may act as a barrier to recruiting and retaining First Nations midwives, and risks contributing to further intergenerational trauma and moral injury within the current and future First Nations workforce.
Limitations
This review is believed to be the first to systematically synthesise existing evidence on First Nations families’ experiences of child removal. This is also thought to be the first study to evaluate midwives’ perspectives in these contexts. A key strength of this review lies in its unique contribution which integrates First Nations insights across international settings, drawing on primary research studies from Australia, Canada and the United States. While efforts were made to include data from other First Nations populations, few studies in this field were located, highlighting a significant gap in the literature.
A limitation of this scoping review was that it included English-language publications only, which may have excluded relevant studies published in other languages. As a result, the generalisability of findings to non-English-speaking contexts remains uncertain. This limitation is particularly important when considering the potential underrepresentation of perspectives from smaller or more isolated First Nations communities. Although the voices included in this review offer valuable insights, they may not fully capture the diversity of lived experiences across different First Nations populations. A further limitation is the small number of participants included in individual studies; however, this may be less significant given the small number of infants removed from family care overall.
Future research must prioritise the inclusion of multiple, diverse First Nations voices to develop a more holistic and representative understanding of infant removal practices and their impacts. This includes expanding the scope to incorporate non-English studies and engaging with communities whose experiences may be less visible in mainstream academic discourse. Addressing this limitation is essential to avoid overgeneralisation and to ensure that future research remains culturally respectful, community-led, and reflective of the full breadth of First Nations diversity, particularly in relation to infant removals and family preservation.
Conclusion
This scoping review is the first to systematically synthesise evidence on First Nations families’ experiences of infant removal alongside midwives’ perspectives in these contexts. The five themes identified reveal the deeply embedded systemic, cultural, and emotional complexities surrounding infant removal practices in Australia, Canada and the United States. The findings also highlight the lasting influence of colonial policies, systemic racism, and culturally unsafe practices that continue to marginalise First Nations families within child protection and health care systems. Midwives, whose practice is grounded in the principles of woman-centred care, often find themselves in ethically complex situations during infant removals, leading to significant moral distress and professional tension. These findings suggest that midwives and health care professionals are often ill-equipped to navigate these complex circumstances.
Ultimately, this review calls for urgent systemic reform. Policies and practices must be co-designed with First Nations communities, grounded in cultural safety, and committed to healing rather than surveillance. Only through such transformative efforts can we begin to address the harms of infant removal and support the wellbeing of First Nations families and the midwives who care for them.
Supplemental Material
sj-docx-1-aln-10.1177_11771801261445645 – Supplemental material for First Nations Families and Midwives’ Perspectives on Infant Removal in Mainstream Maternity Settings: A Scoping Review
Supplemental material, sj-docx-1-aln-10.1177_11771801261445645 for First Nations Families and Midwives’ Perspectives on Infant Removal in Mainstream Maternity Settings: A Scoping Review by Tahlia Johnson, Julian Grant, Susan Smith and Nina Sivertsen in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Acknowledgements
The authors are thankful to the First Nations families for sharing their time and views.
Glossary
Indigenous word English definition
Aotearoa New Zealand
Kalaallit Nunaat Greenland
Kaurna Land The traditional Country of the Kaurna people in South Australia, spanning the Adelaide Plains, stretching from Cape Jervis in the south to Port Wakefield in the north and including the Mount Lofty Ranges.
Māori Indigenous people of Aotearoa
Ngarrindjeri Land The traditional country of the Ngarrindjeri Nation in South Australia, spanning the lower Murray River, Lakes Alexandrina and Albert, the Coorong, and the Fleurieu Peninsula coast.
Peramangk Land The traditional Country of the Peramangk people in South Australia, spanning from the foothills above the Adelaide Plains, north from Mount Barker through Harrogate, Gumeracha, Mount Pleasant, and Springton to the Angaston and Gawler districts in the Barossa, and south to Strathalbyn and Myponga on the Fleurieu Peninsula.
Sámi The Indigenous people of Norway, Sweden, Finland and the Russian Kola Peninsula.
Warramunga Traditional name of the Aboriginal community in Tennant Creek area of the Northern Territory.
Authors’ Note
Ethical Considerations
This study was conducted by Tahlia Johnson in partial fulfilment of the requirements for the Bachelor of Health Science (Honours). Systematic reviews do not require ethical approval as it does not collect confidential information from participants and the data collected has already undergone ethical approval. However, it is important when working in research that ethical approval is noted in each study and by the appropriate committee. This review includes literature involving Aboriginal and/or Torres Strait Islander peoples, making it essential that cultural ethical considerations are clearly articulated. The Ethical conduct in research with Aboriginal and Torres Strait Islander Peoples and communities: Guidelines for researchers and stakeholders (National Health and Medical Research Council, 2018) outlines the principles required to ensure that research involving Aboriginal and/or Torres Strait Islander peoples is culturally safe, respectful, and of clear benefit to communities.
Author Contributions
Conception and design of the study by Tahlia Johnson, Julian Grant and Nina Sivertsen. Data analysis and drafting by Tahlia Johnson, Julian Grant and Nina Sivertsen. Critical revision of the manuscript was conducted by Susan Smith and Nina Sivertsen and final approval of the version to be submitted by all authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: The primary author (TJ) received a Research Preparation Scholarship from Flinders University for Indigenous Students scholarship from Flinders University to assist in the completion of this review. This scholarship was used to support the author financially and had no direct input into the research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Article Description
This systematic review explores the experiences of First Nations families and Midwives involved in the removal of an infant from family care.
Terminology
In Australia, care must be taken to ensure appropriate terminology when referring to Aboriginal and Torres Strait Islander people and communities. This study has followed Aboriginal and Torres Strait Islander guide to terminology endorsed by the Public Health Association of Australia (Public Health Association Australia, 2023). The term First Nations is used when speaking about First Nations peoples as a whole but specific communities names may be used as identified in the selected article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.