
Abstract
Background
Breast cancer is a heterogeneous disease in which hormone receptor and HER2/neu expression patterns are closely associated with tumor histologic grade, prognosis, and treatment response.
Objective
To investigate the correlation of hormone receptors and HER-2/Neu status with histologic grades of invasive ductal carcinoma of the breast.
Design
A facility-based retrospective cross-sectional study.
Methods
A facility-based retrospective cross-sectional study was conducted. Clinical and socio-demographic data were retrieved from medical records. Histopathological and immunohistochemical analysis were done according to standard procedures. Statistical analyses were performed using IBM SPSS version 25. Spearman’s rank correlation coefficient was determined to assess the association between the histological grades, the receptors and the HER-2/Neu status. p-values less than 0.05 are considered as statistically significant.
Result
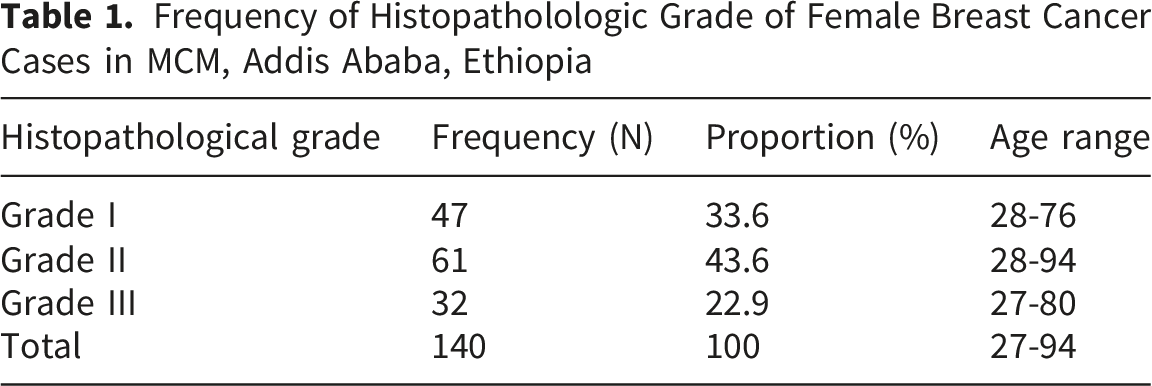
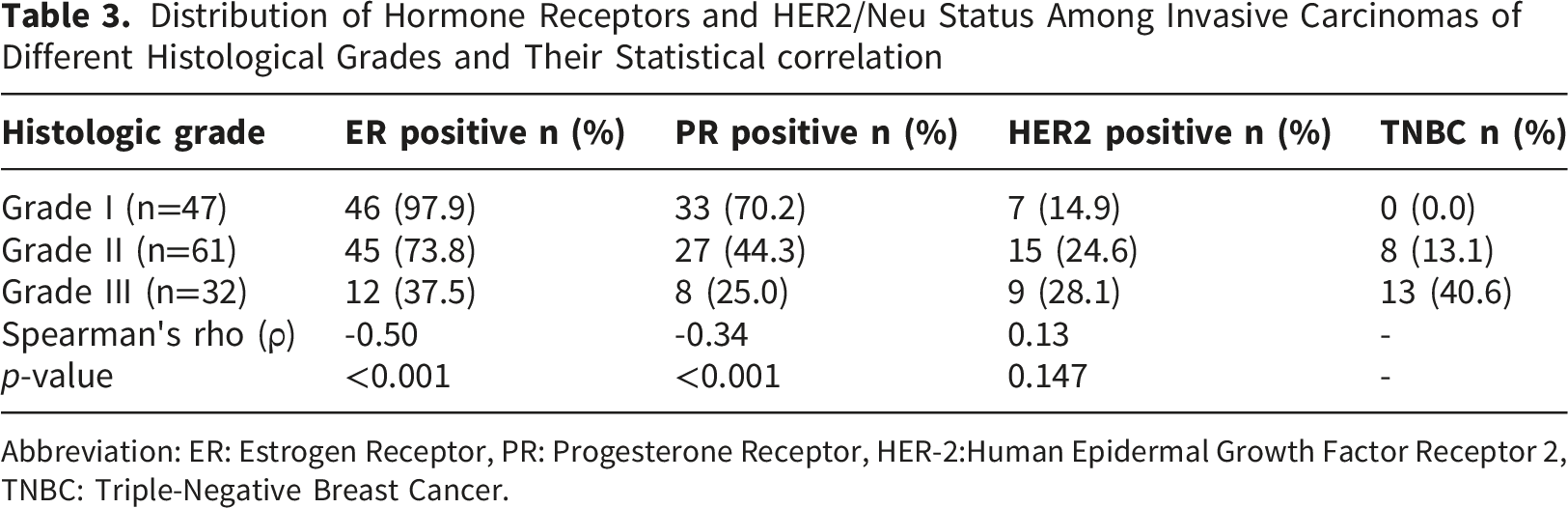
One hundred forty BC cases were included in this study. The mean age of study subjects was 47. The most frequent age group was distributed within 36 to 45 years, with 49 cases (35%). Most (N=61, 43.6%) cases were identified to be grade II, followed by grade I (N=47, (33.6%) and grade III (22.9%, N=32). Majority of the BC tissues showed high expression of ER (N=103, 73.6%) and PR (N=68, 48.6%) and HER2 (N=31, 22.1%). Some of ER+ cases (N=43, 41.2%) were observed to be histological grade 1 whereas 43.7% (N=45) ER+ cases were identified to be histological grade II. The remaining 15% (N=12) were histological grade III. There were 21 cases which were categorized as triple negative breast cancer (TNBC), representing 15% of all the cases studied. Spearman’s rank correlation analysis demonstrated a significant inverse association between histologic grade and ER and PR positivity (p<0.001), indicating that higher-grade tumors were less likely to express the receptors.
Conclusion
The status of hormone receptors and HER-2/Neu in BC is similar to previous reports. An inverse correlation between histological grade and hormone receptor status is reported. Thus, more attention is needed from the health care authorities to improve the diagnostic capacity of pathology laboratories by widely availing access to immunohistochemistry services.
Introduction
Breast cancer (BC) is a growing public health concern and represents one of the leading causes of cancer-related morbidity and mortality among women in Ethiopia. Recent epidemiological reports indicate a steady increase in the incidence of the disease over the past few decades, reflecting both demographic changes and improved recognition of the disease.1,2 Despite this increasing burden, the majority of Ethiopian BC patients are diagnosed at advanced stages of the disease, which significantly impairs treatment success and survival rates. Delayed presentation is common and is frequently associated with prolonged referral pathways, inadequate awareness of BC symptoms, socioeconomic limitations, and restricted access to specialized healthcare services. 3 Moreover, access to advanced diagnostic techniques, including immunohistochemistry (IHC) testing, molecular profiling, and comprehensive oncology care, remains limited outside major urban centers such as Addis Ababa. 4 As a result, treatment decisions in many Ethiopian healthcare settings are often based primarily on conventional histopathologic evaluation rather than detailed molecular characterization of the tumors. This limitation may compromise the selection of appropriate therapies, particularly targeted and endocrine treatments that depend on receptor-status determination in the breast cancer tissue.
BC is a biologically heterogeneous disease composed of multiple molecular subtypes with distinct clinical, pathological, and prognostic characteristics. The assessment of estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor-2 (HER2/neu) status has become a cornerstone in the diagnosis and management of BC worldwide.5,6 These biomarkers play a key role in predicting tumor behavior, determining prognosis, and guiding therapeutic decision-making. For example, tumors that express ER and PR are generally associated with better prognosis and responsiveness to endocrine therapies such as tamoxifen or aromatase inhibitors. In contrast, HER2-positive tumors are often associated with more aggressive disease behavior but may benefit significantly from HER2-targeted therapies such as trastuzumab. Triple-negative breast cancers (which lack ER, PR, and HER2 expression) are commonly associated with poor prognosis, higher histologic grade, and limited treatment options. Consequently, accurate determination of receptor status is essential for optimizing individualized treatment strategies and improving patient outcomes.6,7
Histologic grading is another well-established prognostic factor in BC and reflects the degree of tumor differentiation and aggressiveness. The Nottingham histologic grading system evaluates tubule formation, nuclear pleomorphism, and mitotic activity to classify tumors into low-grades, intermediate-grades, or high-grade categories. High-grade tumors are generally associated with increased proliferative activity, more aggressive clinical behavior, and poorer prognosis compared with low-grade tumors. Previous studies conducted in different populations have demonstrated significant associations between histologic grade and the expression patterns of ER, PR, and HER2/neu receptors.7-9 For example, hormone receptor-negative tumors are frequently associated with higher histologic grades, whereas hormone receptor-positive tumors tend to exhibit lower grades and better differentiation. Similarly, HER2 overexpression has often been linked to increased tumor aggressiveness and unfavorable prognostic features. However, these relationships have shown variability across populations and geographic regions, suggesting that genetic, ethnic, environmental, and healthcare-related factors may influence the biology and receptor distribution patterns of BC.10,11
Despite the increasing burden of BC in Ethiopia, data regarding the clinicopathologic characteristics and molecular profiles remain limited and inconsistent. This knowledge gap is important because understanding local tumour characteristics may help clinicians improve diagnostic accuracy, predict disease behaviour and optimize treatment approaches in resource-constrained settings. In environments where advanced molecular testing is not routinely available, histologic grades may serve as a useful surrogate indicator for tumour aggressiveness and potential receptor-status patterns. Furthermore, identifying correlations between tumour grades and receptors expression may support more efficient utilization of limited pathology resources and contribute to evidence-based clinical decision-making.
Therefore, this study was intended to investigate the correlation between histologic grade and ER, PR, and HER2/neu status among Ethiopian women diagnosed with invasive ductal carcinoma of the breast. By characterizing the relationship between tumour differentiation and receptors expression patterns in a resource-limited setting, the study aimed to generate locally relevant evidence that may contribute to improved diagnostic, prognostic, and therapeutic strategies for BC management in Ethiopia. Additionally, the findings of this study may provide valuable information for clinicians, pathologists, and policymakers working to strengthen BC care services and enhance outcomes for Ethiopian BC patients.
Materials and methods
Study Design, Population and Inclusion Criteria
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (Supplementary 1) Statement. 12 A facility-based cross-sectional study was conducted on female breast cancer (BC) patients at Myungsung Comprehensive Specialized Hospital (MCSH) in Addis Ababa, Ethiopia, from January 2021 to September 2023. MCSH is one of the largest private comprehensive hospitals located in Addis Ababa. The study population were female BC patients who attended pathology department at this MCSH during the study period. All histologically confirmed invasive ductal carcinoma (IDC), non-special type cases diagnosed during the study period and fulfilling the eligibility criteria were included consecutively based on the availability of complete socio-demographic, histopathology and immunohistochemistry records. BC patients with known molecular signature, age less than 18 and not willing to participate in the study are excluded from the study. As the study relied on archived pathology materials and retrospective medical records, cases with incomplete histopathologic or immunohistochemical records, inadequate tissue samples, equivocal HER2 (+2) results, or missing key demographic information were intentionally excluded from the analysis. However, this may have introduced selection bias if excluded patients differed systematically from included patients.
Socio-Demographic Data and Sampling Techniques
A retrospective consecutive sampling technique was used to include all eligible histologically confirmed IDC cases diagnosed during the study period with available complete histopathologic and immunohistochemical data. To minimize information bias, data were extracted by trained personnel using standardized data abstraction procedures and cross-checked for completeness and consistency. Socio-demographic data were retrieved from medical records by experienced data collector. A total of 140 histologically-proven cases of invasive ductal carcinoma, non-special type, diagnosed from mastectomy and core needle biopsy specimens were included. The collection of tumor tissue was done by attending surgeons in MCSH hospital. Portions of the solid tumours, free of fat, connective tissue, debris, and blood were cut into pieces of approximately 3x3x3 mm and transported to the pathology laboratory using icebox. Then, histopathological and immunohistochemical analysis were done by following standard procedures. Inter-observer variability was minimized through independent evaluation by experienced pathologists and consensus review of discordant cases. Standardized immunohistochemistry protocols, internal controls, and independent pathologist review were employed to reduce measurement variability. Although age was adjusted for in multivariable analysis, residual confounding from unmeasured factors such as menopausal status, tumor stage, lymph node involvement, and reproductive characteristics cannot be excluded.
Tissue Sectioning and Haematoxylin and Eosin Staining
The tissue sectioning and haematoxylin and eosin staining was carried out by following the standard histopathological procedures. Briefly, the collected breast cancer (BC) tissue was washed with PBS, fixed in Roti® Histofixn (Carl Roth, Germany) for 24 hours. Then it was dehydrated using ASP300 Tissue Processor (Leica country, Germany) and embedded in paraffin. A series of 4 µm thick sections were cut for staining. Wax was removed from paraffin embedded tissue sections with the aid of 2x Roti® Histol (Carl Roth, Germany) for 5 minutes. Then, the tissue was rehydrated with the decreasing alcohol series (2x 100%, 2x 96% and 2x 80% EtOH), each for 3 minutes. Sections were then stained in haematoxylin for 5 sec, gently washed in tap water for 10 min and then stained in eosin for approximately 20 sec. Tissue was dehydrated with an increasing alcohol series (2x 80%, 2x 96% and 2x 100% ethanol). After immersing 2x for 5 min in Roti® Histol (Carl Roth, Germany) slides were mounted in PERTEX for microscopic observation. All cases under study were histopathologically classified using Chapter 11 Neoplasm, International Statistical Classification of Diseases and Related Health Problems 10 Revision (ICD-10)-WHO Version for; 2016) by experienced pathologist. The samples were graded according to the Nottingham histologic grading system, which takes into account glandular formation, nuclear grading and mitotic activity. Glandular formation was assigned a total of 3 points based on the degree of formation. Accordingly, it was interpreted as well-formed=1, moderately formed=2 and poorly formed=3. Nuclear atypia was graded on a scale of 3 points according to severity, considering pleomorphism and the presence of nucleoli. Mitotic activity was given a total of 3 points based on the number of mitotic figures observed per 10 high-power fields (HPF). It was inferred as mitotic activity <7 per 10 HPF=1, mitotic activity between 7 and 14 per 10 HPF=2, mitotic activity >14 per 10 HPF=3). Adding up all the scores, we get a total score out of nine. Therefore, a total score of 3 to 5 points is considered grade I, a score of 6 to 7 points is considered grade II, and a score above 7 points is considered grade III.
Immunohistochemistry Protocol and Analysis
The immunohistochemistry was performed manually using the EnVision™ FLEX+ (DAKO, Denmark). Formalin-fixed paraffin sections were cut at 4 μm and rehydrated with water. Subsequently, the samples were heated in the oven for 1 hour for further de-waxing. After preparing the retrieval solution, the slide was placed in a water bath for 20 minutes. Then, the specimens were treated with EnVision™ FLEX Peroxidase-Blocking Reagent (DAKO, Denmark) for 20 minutes. Subsequently, they were treated with monoclonal primary antibody (FLEX RTU and EnVision FLEX LINKER mouse, DAKO, Denmark) for 20 and 15 minutes, respectively. Then, EnVision™ FLEX/HRP (DAKO, Denmark) substrate working solution was applied for 10 and 20 minutes, respectively. Finally, counterstaining was performed with EnVision™ FLEX Hematoxylin (RTU) for 5 minutes. Rinsing with wash buffer and water was done in between each step. Positive and negative controls were included with each staining batch to ensure staining quality and reproducibility. All stained slides were independently evaluated by experienced pathologists, and discordant findings were reviewed jointly to achieve consensus interpretation.
Interpretation was performed according to the Allred scoring system. 13 The primary outcomes were ER, PR, and HER2 receptor status determined by immunohistochemistry. Tumors with an Allred score of ≥3 were considered positive for ER and PR expression. HER2/neu expression was evaluated according to standard scoring criteria based on the intensity and completeness of membranous staining and categorized as 0, 1+, 2+, or 3+. Cases scored as 0 and 1+ were considered negative, while cases scored as 3+ were considered positive for HER2 overexpression. HER2 equivocal cases (2+) were excluded from the analysis because fluorescence in situ hybridization (FISH) confirmation was not available in our setting. Potential residual confounding by menopausal status, lymph node involvement, reproductive factors, treatment history, and comorbidities could not be assessed because these data were unavailable. No effect-modifier analyses were also performed.
Statistical Analysis
All statistical analyses were performed using IBM SPSS version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistics including mean, median, frequencies, and percentages were used to summarize study variables. Associations between histologic grade and ER, PR, and HER2/neu status were assessed using Spearman’s rank correlation coefficient (Spearman’s rho). Correlation coefficients and corresponding p-values were calculated. p<0.05 are considered as statistical significant. Only representative pictures of histopathology and immunohistochemistry were demonstrated.
Ethical Clearance
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the College Ethics and Research Committee of Myungsung Comprehensive Specialized Hospital College, Addis Ababa, Ethiopia. The study was retrospective and conducted using archived tissue slides and anonymized clinical data retrieved from medical records. Since no direct patient contact or intervention was involved, the requirement for written informed consent was waived by the Ethics and Research Committee (Protocol No. Pro-230224). All data were handled anonymously, and strict confidentiality of patient information was maintained throughout the study.
Results
A total of 140 female breast cancer (BC) cases were included in this study. The mean age of study subjects was 47 (ranging from 27 to 94 years). The most frequent age group was 36 to 45 years, with 49 cases (35%). The least frequent age group was above 86, accounting for only 1 case (0.7 %) (Figure 1). Age-distribution amoung the breast cancer patients included in this study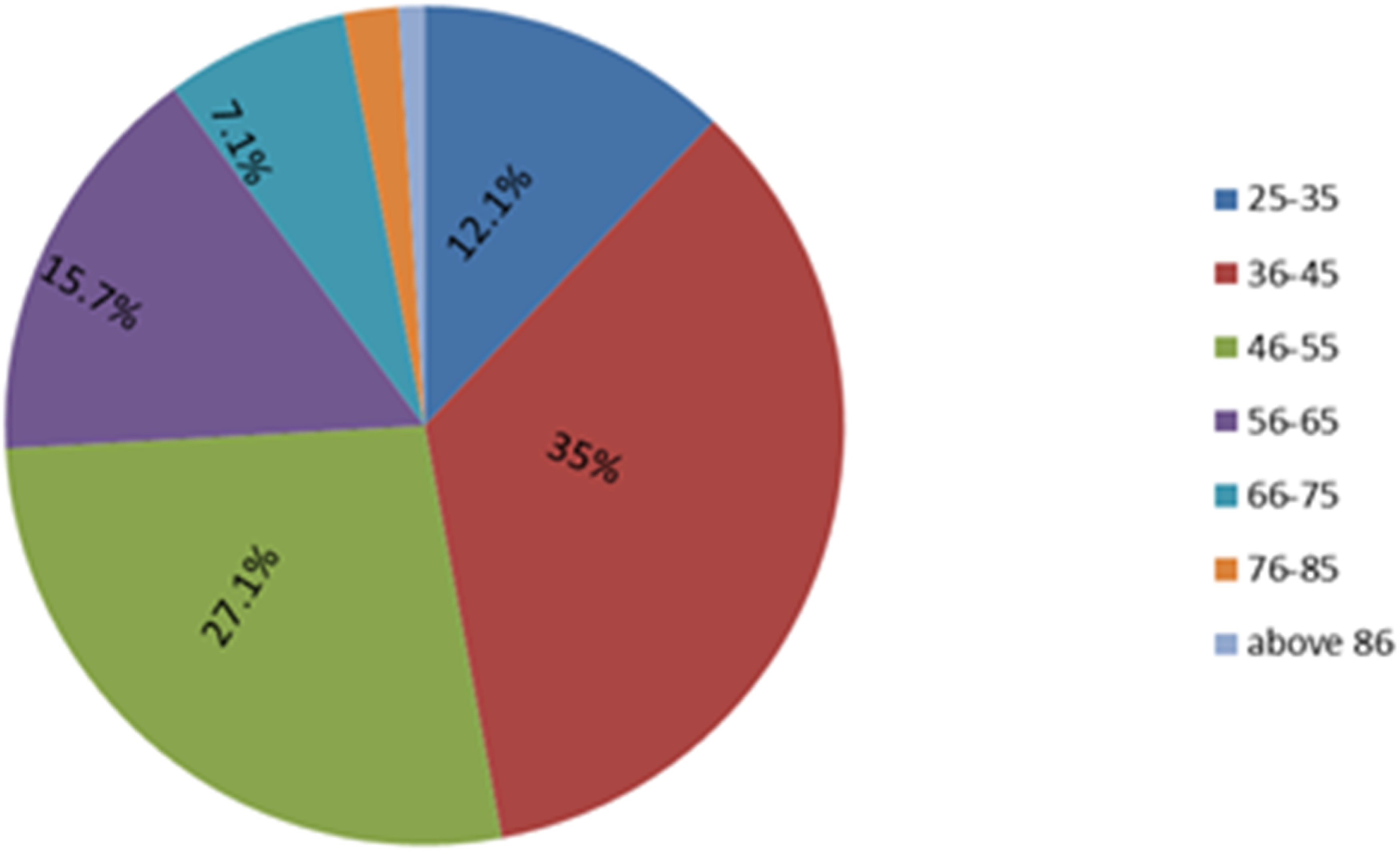
Frequency of Histopatholologic Grade of Female Breast Cancer Cases in MCM, Addis Ababa, Ethiopia
Furthermore, the histopathological features of the female breast cancer cases were explored microscopically. However, it was not statistically significant. The microscopic appearance of the Hematoxyline and Eiosin (H & E) stained tissue of invasive ductal carcinoma of the breast indicated occasional entrapped normal ducts with secretory changes adjacent to invasive tumour (Figure 2). Representative picture of photo-micrograph after H &E staining invasive ductal carcinoma of the breast adjacent to normal duct under 40X magnification using LEICA ICC50HD Microscope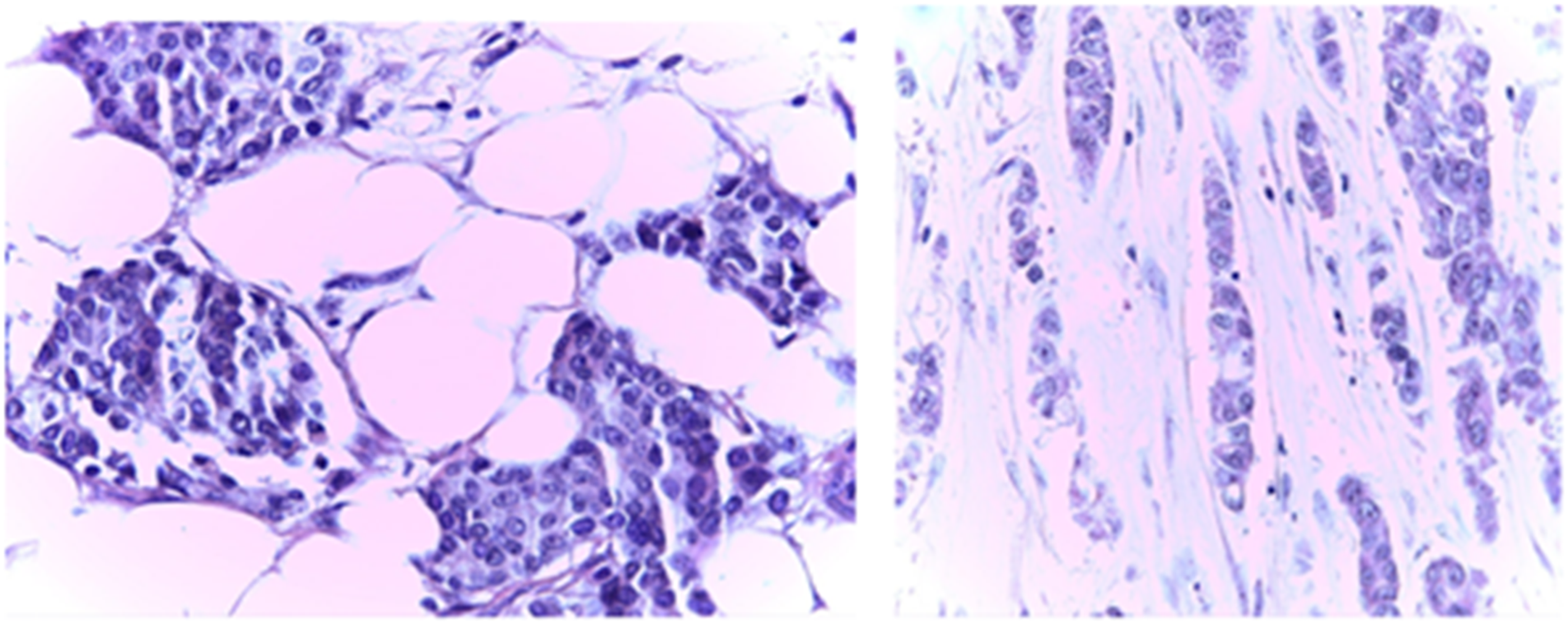
Distribution Pattern of Hormone Receptors and HER-2 status

Abbreviation: ER:Estrogen Receptor, PR: Progesterone Receptor, HER-2:Human Epidermal Growth Factor Receptor 2, TNBC: Triple-Negative Breast Cancer.
The Spearman’s rank correlation analysis demonstrated a significant inverse association between histologic grade and ER positivity (ρ=-0.496, p< 0.001), indicating that higher-grade tumors were less likely to express estrogen receptors. A weaker but statistically significant inverse correlation was also observed between histologic grade and PR positivity (ρ=−0.342, p<0.001). In contrast, HER2 positivity showed a weak positive correlation with histologic grade that did not reach statistical significance (ρ=0.125, p=0.142). Furthermore, there was no significant correlation between age and Nottingham grade, ER status, PR status and HER-2 receptor positivity (Figure 3 and Table 3). Immunohistochemistry photograph showing diffuse strong positive nuclear stain for ER (A) and PR (B). and showing diffuse +3 cytoplasmic membrane positivity for HER 2 under 40X magnification using LEICA ICC50HD Microscope Distribution of Hormone Receptors and HER2/Neu Status Among Invasive Carcinomas of Different Histological Grades and Their Statistical correlation Abbreviation: ER: Estrogen Receptor, PR: Progesterone Receptor, HER-2:Human Epidermal Growth Factor Receptor 2, TNBC: Triple-Negative Breast Cancer.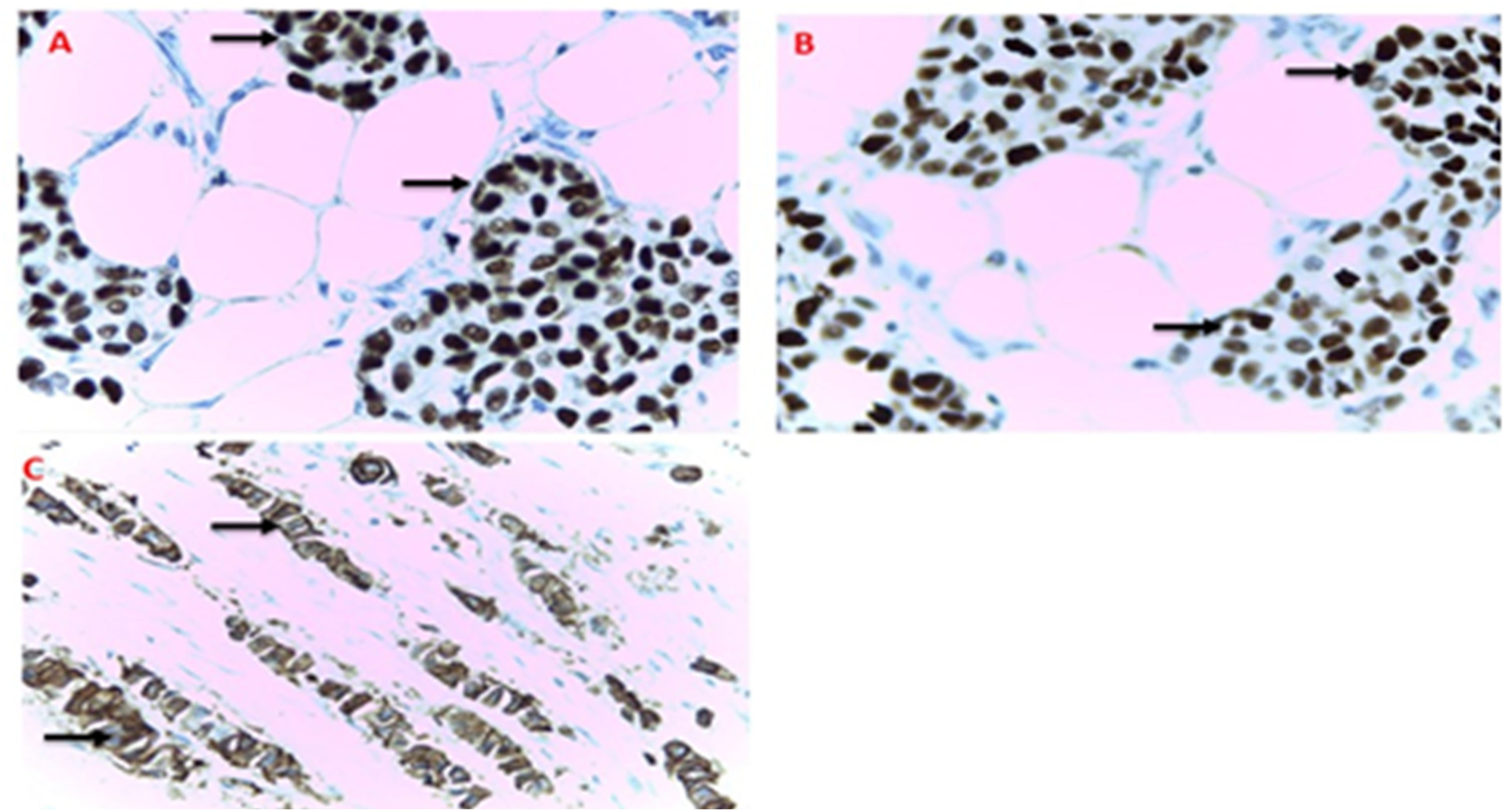
Discussion
Breast cancer (BC) is an important healthcare challenge both in high income and low income countries. Due to the advanced diagnostic and treatment modalities and increased awareness of the people, mortality from BC is significantly decreased in Western world.14-16 In contrary, the incidence and mortality from BC is sginificantly increasing in low income countries like Ethiopia.1,2,17 This is mainly due to the poor awareness of people about the disease, unavailability and inaccessibility to the advanced health care facility and the biological heterogeneity of the BC itself.3,8 In addition to revisiting the strategies of awareness education, it is useful to study the intrinsic molecular signature and pathobiological characteristics of BC in low income countries. These will enable the clinicians to apply the right treatment modalities and improve the disease outcomes. Thus, the objective of the current study was to explore the correlation between the hormone receptors, HER-2 status and histopathologic grades of invasive ductal carcinoma (IDC) of the breast among women attending the Myungsung Comprehensive Specialized Hospital (MCSH), Addis Ababa, Ethiopia.
This study revealed relatively a higher proportion of younger patients, with a median age of 47. The prevalence of BC in younger female population is commonly reported from both LICs and HICs.18-20 This is in contrast to the previous assumption that breast cancers commonly occur at higher age groups. The usual trends of BC in people of European origins show that the disease occurs in women over 50 years of age. This shift in age distribution may be attributed to demographic changes and genetic factors. Further investigations, particularly molecular epidemiological studies involving broader populations and wider geographic coverage, are required to validate these findings and draw definitive conclusions.21,22
The ER and PR play crucial roles in several physiological activities of the breast tissue. 23 They are important in the breast tissue development, growth and differentiation. Pathologically, the ER and PR play fundamental roles in tumorigenesis, tumour diagnosis, prognosis and prediction of the diseases. 24 Similarly, HER-2 oncogene codes for a transmembrane glycoprotein with tyrosine kinase activity. 25 The expression status of ER, PR, and HER-2 is a major determinant of prognosis and treatment outcomes in patients with breast cancer. Moreover, the distribution and expression patterns of these important molecular biomarkers vary significantly among different populations.23-25 The expression pattern of these molecules differs in intratumour and intertumour tissues of the breast. Thus, we determined the status of these molecular players in the invasive ductal carcinoma of the breast. The overall high expression of ER and PR in our study groups aligns with similar findings conducted in Ethiopia and some East African countries.26-29 Our findings also show the highest ER positivity and lowest triple negative breast cancer (TNBC) types among sub-Saharan countries (Table 2). These findings further suggest that the distribution of receptor-defined breast cancer subtypes in Ethiopia is broadly comparable to that observed in Western populations. 30 However, this is in contrast to the molecular characteristics of breast cancer in Western Africa where the ER and PR are expressed at lower rate and the TNBC are more prevalent than the in the Eastern Africa.31,32 It was also shown that the molecular features of breast cancer in African-Americans and Western African are characterized by aggressive TNBC forms that appears more frequently in younger populations. 33 The observed comparability in BC subtype distributions between East African populations and Western world may be attributable to the considerable heterogeneity in lifestyle factors and the complex patterns of genetic admixture that characterize Sub-Saharan African populations. 26 Nevertheless, further investigations at the molecular and genomic levels are urgently required to elucidate the underlying mechanisms driving this clinically significant variation.
Hormone-Receptor and HER-2 Status Identified in Various Studies in Africa
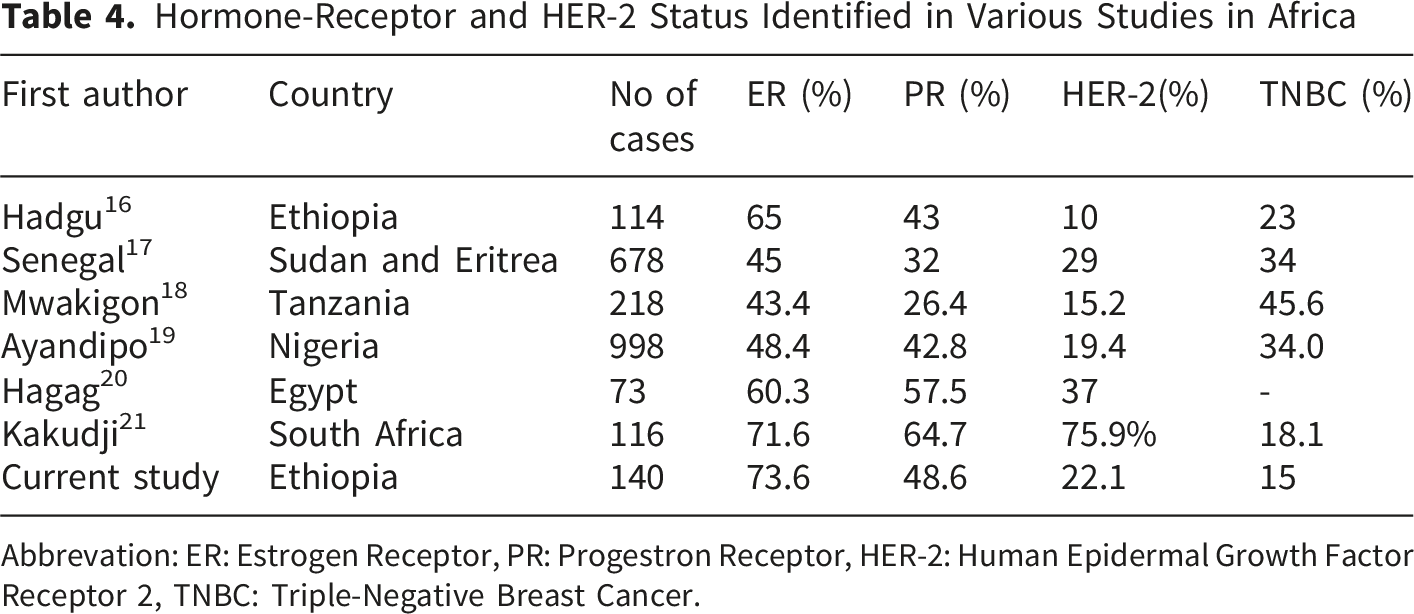
Abbrevation: ER: Estrogen Receptor, PR: Progestron Receptor, HER-2: Human Epidermal Growth Factor Receptor 2, TNBC: Triple-Negative Breast Cancer.
Although immunohistochemistry is a mandatory requirement for every breast cancer patient, majority of cases in low income countries, like Ethiopia, are unable to access the service due to poor infrastructure and financial constraints. The existing system also has various limitations, including quality issues and incompleteness. Our research, along with similar studies, will provisionally address this issue by predicting the immunohistochemistry profile of compromised patients through the correlation of histologic grade. In spite of the presence of several limitations, the study population reflects a real-world cohort of consecutively diagnosed invasive ductal carcinoma cases and therefore provides clinically relevant evidence for breast cancer management in Ethiopia. The observed inverse association between histologic grade and hormone receptor expression is consistent with findings from other regions, supporting the biological plausibility and potential applicability of these results beyond the study setting. Nevertheless, multicenter studies incorporating more diverse patient populations and comprehensive molecular characterization are warranted to confirm the external validity of these findings.
Conclusion
This study reinforces existing evidence on hormone receptor expression patterns among Ethiopian breast cancer patients. We found that ER and PR positivity rates are comparable to those reported in Western populations but differ from those observed in West Africa. Notably, our cohort exhibited a high rate of ER positivity and a low prevalence of triple-negative breast cancer (TNBC). Hormone receptor positivity was significantly associated with lower histological grade, whereas HER2 status showed no significant association with grade. Additionally, neither hormone receptor status nor Nottingham grade was significantly associated with patient age. These findings provide important insights into the clinicopathological characteristics of breast cancer in Ethiopia and highlight the need to improve access to immunohistochemistry services to support optimal treatment decisions.
Limitations
First, the retrospective cross-sectional design precludes establishing causal relationships between histologic grade and hormone receptor/HER2 status. Selection bias cannot be excluded, as only cases with complete histopathologic and immunohistochemical data were included. Key clinicopathologic variables, including tumor stage, menopausal status, treatment history, and comorbidities, were unavailable or incomplete and could not be assessed as potential confounders. Additionally, HER2-equivocal (2+) cases were excluded due to the lack of FISH confirmation, potentially underestimating HER2 positivity and affecting the observed association with histologic grade. Although standardized immunohistochemical protocols and quality control measures were used, inter-observer variability in receptor interpretation was not formally evaluated.
Supplemental Material
Supplemental Material - Correlation of Hormone Receptors and HER-2/Neu Status With Histologic Grades of Invasive Ductal Carcinoma of Breast Among Women at Myungsung Comprehensive Specialized Hospital, Addis Ababa, Ethiopia
Supplemental Material for Correlation of Hormone Receptors and HER-2/Neu Status With Histologic Grades of Invasive Ductal Carcinoma of Breast Among Women at Myungsung Comprehensive Specialized Hospital, Addis Ababa, Ethiopia by Taye Jemberu Robele, Abirham Ayine Minayehu, Yonas Mulugeta Balcha, Henock Seyoum Tsegaye, Dagmawit Mesfin Tassew, Wajana Lako Labisso in Breast Cancer: Basic and Clinical Research
Footnotes
Ethical Considerations
Ethics approval is not required. But IRB Clearance was obtained with protocol number (Protocol No. Pro-230224).
Author contributions
All authors contributed to study conception and design and drafting. Material preparation, laboratory work and data collection were performed by Taye Jemberu Robele, Wajana lako and Abirham Ayine Minayehu. Data analysis was completed by Wajana Lako Labisso, Taye Jemberu Robele, Abirham Ayine Minayehu. The draft was written by Wajana Lako Labisso, Taye Jemberu Robele, Abirham Ayine Minayehu, Yonas Mulugeta Balcha, Henock Seyoum Tsegaye, Dagmawit Mesfin Tassew; and all authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data may be made available to bona fide researchers only, on reasonable request to the corresponding author.
AI Disclosure
No scientific data were generated or modified using AI.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.