
Abstract
Background:
Medical error reporting serves as a crucial indicator of healthcare professionals’ commitment, accountability, and reliability, which ensures patient rights, and also functions as a mirror of organizational culture, reflecting staff attitudes and practices regarding patient safety. This study was conducted to predict factors affecting nurses’ medical error reporting behavior using the theory of planned behavior (TPB) at Shiraz University of Medical Sciences, Iran, in 2024.
Methods:
This applied, cross-sectional study examined 280 nurses working in teaching hospitals. The required samples were selected using stratified random sampling proportional to size and simple random sampling methods. Data were collected using the Persian version of the medical error reporting questionnaire developed by Seyedin et al based on the theory of planned behavior and were analyzed and modeled through structural equation modeling (SEM) using Smart PLS 3.0.
Results:
The results showed that the model demonstrated a relatively strong overall fit (GOF = 0.342, SRMR <0.08, RSM Theta <0.12), and all its constructs were associated with and demonstrated predictive power for behavior, so that both direct and indirect paths on behavior were statistically significant (P < .001). However, perceived behavioral control (β = .385; f2 = 0.161) and behavioral intention (β = .378; f2 = 0.155) showed the strongest direct associations, and control beliefs (β = .175; f2 = 0.730) exhibited the greatest indirect association on behavior.
Conclusion:
The findings indicated that improving medical error reporting requires comprehensive attention to both behavioral and cognitive characteristics of nursing staff and providing a supportive environment that reinforces positive beliefs and attitudes toward error reporting. Practical recommendations include facilitating access to reporting systems, giving continuous feedback about reported errors to nurses and providing them with positive consequences, considering various rewards for timely and accurate reporting of medical errors, and creating continuous supportive mechanisms.
Introduction
Medical errors present a significant challenge to healthcare systems globally, encompassing all mistakes occurring during diagnosis, treatment, test result interpretation, and use of medical equipment or medications by healthcare providers, including physicians, nurses, laboratory technicians, and radiologists. 1 In other words, a medical error is defined as “an event that, due to a defect or mistake in the planning or execution, results in or could result in an unintended outcome.” 2 The results of various studies show that some factors, including personal, managerial, and organizational factors; the complexity of the work method; environmental conditions; the design of equipment and devices; the method of training personnel; the method of supervision; the absence of work instructions, 3 high workload, large number of patients, unstable patient conditions, lack of awareness, inappropriate work space, lack of support and cooperation with experienced personnel, 4 lack of attention to taking a complete history, poor communication with the patient, lack of motivation, and resource shortages 5 can play an effective role in causing medical errors by medical staff, especially nurses.
According to the World Health Organization (WHO) Global Patient Safety Report 2024, more than 1 in 10 patients in healthcare settings suffer harm due to unsafe care, and half of these harms are preventable. This instability causes millions of deaths and high economic costs annually. Additionally, nearly two-thirds of patient harm due to unsafe care occurs in low- and middle-income countries, which bear the highest mortality burden. 6 Studies in Iran show that a significant percentage of medical errors goes unreported, which creates a serious gap in patient safety; based on one of the conducted investigations, the estimated rate of underreporting of medical errors in Iran ranges from 40% to 70%, indicating the necessity for improving the medical error reporting system. 7
Since many medical errors are difficult to detect electronically, and manual review is time-consuming and challenging, error reporting remains one of the most reliable methods for collecting data about medical errors. 2 Generally, error reporting is an important and influential component in the quality of healthcare services and patient safety. 8 It helps reduce the adverse effects of errors, lowers financial costs for organizations and patients, shortens hospital stays, prevents similar errors, and demonstrates healthcare professionals’ commitment, accountability, and reliability, thereby protecting patient rights.9,10 As a behavior, error reporting reflects organizational culture and safety attitudes. 11 In general, reporting medical errors improves and corrects healthcare providers’ performance, particularly nurses, by enabling organizations to learn from harmful events, enhancing competition, job skills, and staff efficiency, and narrowing gaps between research, treatment, and decision-making processes. 10 However, barriers such as perceived futility of reporting, lack of awareness, disbelief in safety improvement, unfamiliarity with procedures, fear of negative consequences, time constraints, lack of support, and fear of litigation reduce error reporting.6,12
On the other hand, understanding the factors that influence human behavior is crucial for predicting how individuals will respond in various situations. In this regard, there are various theories, one of the most widely used of which is the theory of planned behavior (TPB), which is widely applied in nursing management behaviors, such as reporting medical errors. 13 This theory is a cognitive-social framework that provides a valuable structure for predicting and comprehending health-related behaviors, and represents an advanced version of the Theory of Reasoned Action, 14 which was originally developed by Ajzen and Fishbein to explain and predict human behavior. 15 According to the TPB, individuals make decisions through rational analysis, carefully evaluating available information and considering the potential consequences of their actions before making a decision. At the core of this theoretical approach lies the concept that our beliefs shape our attitudes toward specific subjects. Human behavior is guided by 3 fundamental belief systems: behavioral beliefs, normative beliefs, and control beliefs. Behavioral beliefs form the foundation for developing either positive or negative attitudes toward particular actions. Normative beliefs contribute to the perception of social pressure, known as subjective norms. Control beliefs, relating to one’s sense of control, lead to perceived behavioral control-reflecting an individual’s confidence in their ability to voluntarily perform or refrain from a specific behavior. These 3 components-attitudes toward behavior, subjective norms, and perceived behavioral control-collectively shape behavioral intention, which serves as the primary determinant of actual behavior. Consequently, the theory of planned behavior examines 8 key constructs: behavior, behavioral intention, attitude toward behavior, behavioral beliefs, subjective norms, normative beliefs, perceived behavioral control, and control beliefs. 16 The interrelationships among these constructs within the theory of planned behavior are visually represented in Figure 1.
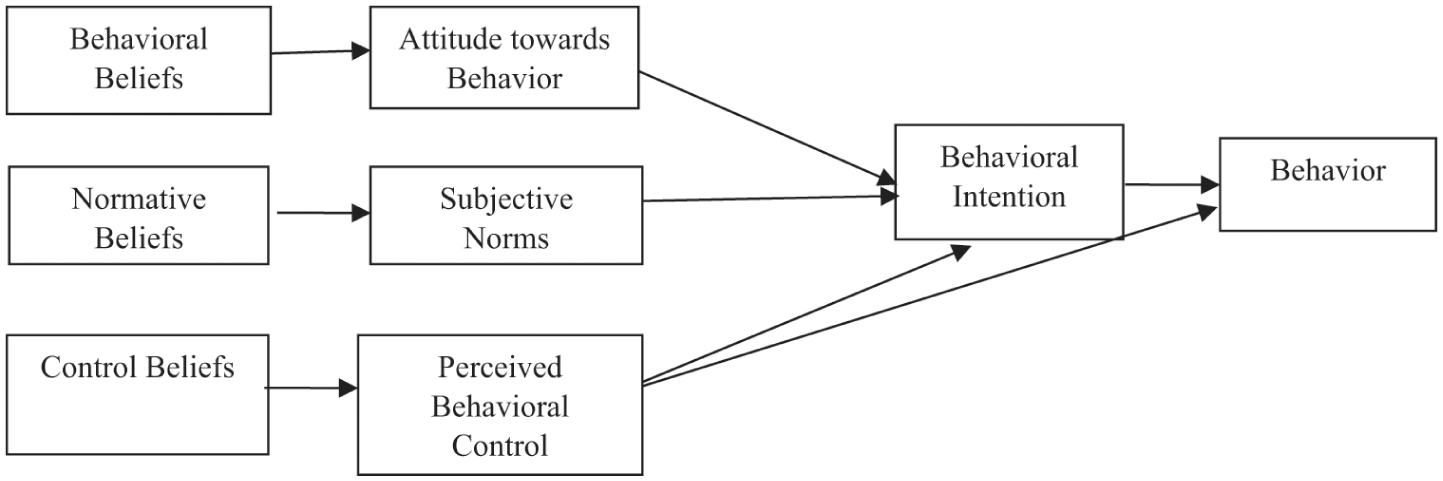
Theory of planned behavior. 17
Given the critical importance of medical error reporting by nurses in improving healthcare services and enhancing patient safety, determining the psychological and social factors associated with their reporting behavior is essential for developing effective interventions. While the theory of planned behavior (TPB) has demonstrated utility in predicting various health-related behaviors, its application to nurses’ medical error reporting remains underexplored, particularly in Middle Eastern healthcare contexts where organizational culture, hierarchical structures, and fear of blame may distinctly shape reporting intentions and behavior.18,19 To address this gap, the present study aimed to test the TPB framework in the Iranian healthcare setting and identify which TPB strongly predict nurses’ reporting behavior in teaching hospitals affiliated with Shiraz University of Medical Sciences, Iran, in 2024. The outcome of interest was operationalized as nurses’ self-reported frequency of medical error reporting over the past 6 months, measured using a validated scale. Consistent with TPB’s theoretical framework, the researchers hypothesized that nurses’ reporting behavior would be directly predicted by behavioral intention and perceived behavioral control, and that these proximal predictors would themselves be influenced by attitude, subjective norms, and the underlying belief structures that shape these constructs.
Methods
This applied, and cross-sectional study was conducted in 2024 at 11 teaching hospitals affiliated with Shiraz University of Medical Sciences, Iran. The study population included all nurses working in these hospitals.
The sample size was determined using the results from a similar study 20 and the following formula, yielding a final sample of 308 participants (assuming P = .761, α = .05, d = 0.05, and the probability of 10% nurses’ dropout):

Where n = sample size, Z = level of confidence according to the standard normal distribution (Z = 1.96 for the level of 95% confidence),
Stratified random sampling proportional to size was employed to select the samples. Initially, the required sample size for each hospital was calculated based on the number of working nurses. Participants were then selected through the simple random sampling method using personnel identification numbers.
Inclusion criteria comprised having a minimum of 1 year of hospital work experience and willingness to participate in the study. Exclusion criteria also consisted of incomplete questionnaires and nurses’ withdrawal before study completion.
The study utilized the Persian version of the reliable and validated medical error reporting questionnaire developed by Seyedin et al, 21 which was designed based on the theory of planned behavior in Persian and was used within the Iranian nursing context. The instrument comprised 37 items in 8 constructs, including behavior (4 items), behavioral intention (4 items), attitude toward behavior (5 items), behavioral beliefs (5 items), subjective norms (2 items), normative beliefs (8 items), perceived behavioral control (5 items), and control beliefs (4 items), all rated on a 7-point Likert scale. Each construct was operationalized to capture distinct TPB dimensions: behavior items assessed actual reporting frequency and observational learning (eg, “How many errors have you reported in the past 6 months using the standard reporting form?”); behavioral intention items measured prospective commitment to reporting errors, including intention to increase reporting frequency and intention to report despite potential legal or punitive concerns (eg, “I intend to increase the percentage of errors I report in the next 3 months”); attitude toward behavior items employed semantic differential scales and evaluative beliefs about reporting outcomes (eg, “Reporting errors can be a good tool for learning from adverse events”); subjective norms items captured perceived social pressure from key referents (eg, “I feel that I am under (social) pressure to reduce the rate of reporting errors to my superiors”); normative beliefs items assessed expectations of specific referent groups such as colleagues, managers, and patients’ families, and motivation to comply (eg, “Reporting errors according to the wishes and opinions of my supervisors is important to me”); perceived behavioral control items measured self-efficacy and perceived autonomy over reporting decisions (eg, “The decision about whether I report an error in the next 3 months is entirely up to me”); behavioral beliefs items assessed beliefs about possible consequences of error reporting (eg, “If I report my medical error, I increase the chances of diagnosing and treating the patient at an early stage”); and control beliefs items assessed perceived barriers, including knowledge deficits and fear of punitive supervisory responses (eg, “Lack of necessary knowledge and skills causes me to report a lower percentage of errors”). Data collection was conducted by the researchers across all 3 hospital shifts.
The collected data were analyzed and modeled through structural equation modeling (SEM) using Smart PLS 3.0. Factor loadings, R2 values, and effect sizes (f2) were obtained from the PLS algorithm output (Figure 2); direct and indirect (mediated) effects were evaluated using non-parametric bootstrapping with 5000 resamples; path coefficients and their corresponding P values (Figure 3) were derived from this bootstrapping procedure, where P values reported as 0.000 indicated P < .001. Statistical significance was determined using t-values, P values, and 95% bootstrap confidence intervals. Descriptive statistics and graphical checks indicated no problematic outliers and only mild non-normality typical of Likert-type data. PLS–SEM was therefore chosen because it is robust to departures from multivariate normality and suitable for complex models with multiple latent constructs and indicators.
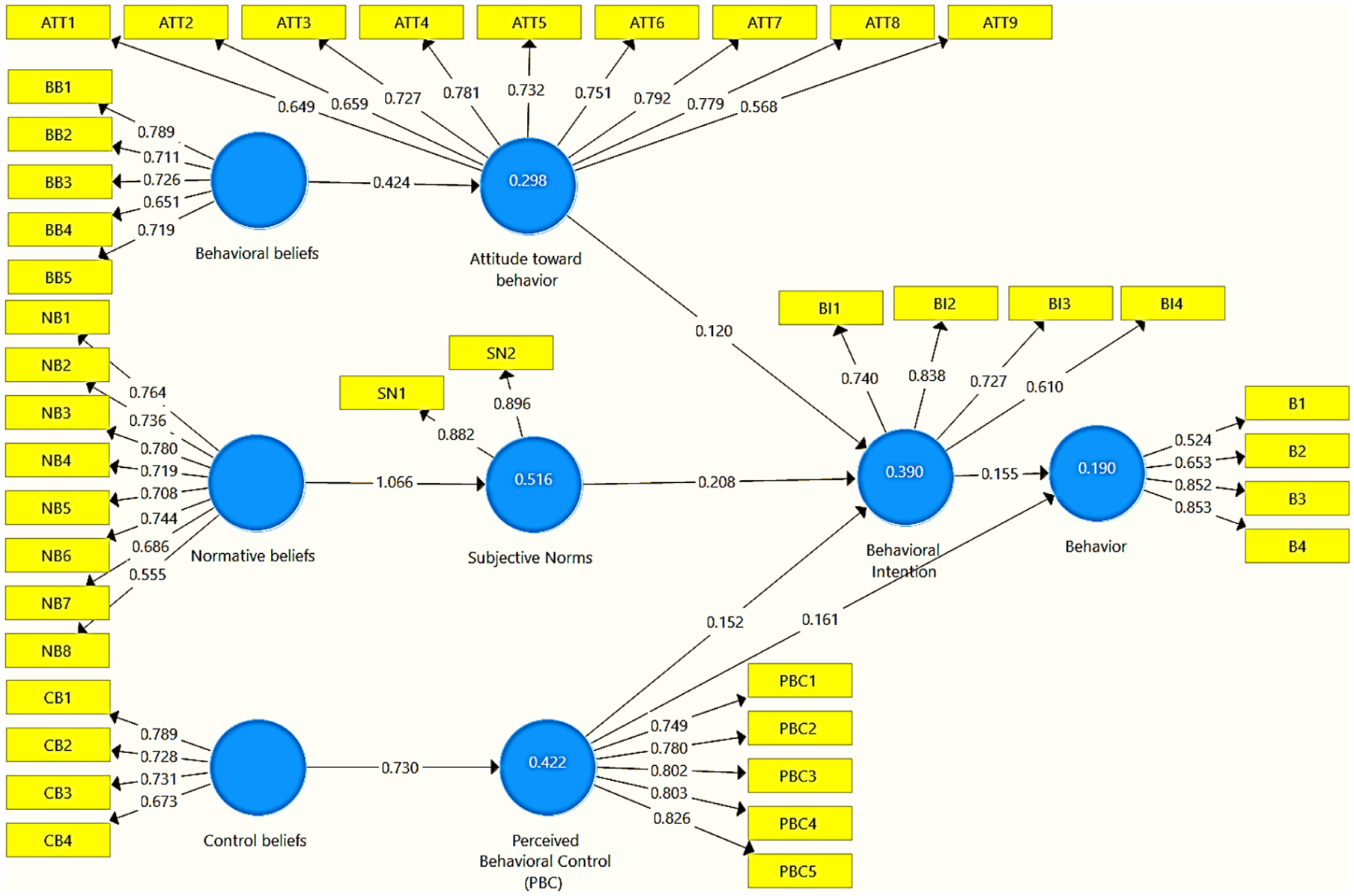
PLS algorithm results showing factor loadings for measurement model indicators, coefficients of determination (R2), and effect sizes (f2) for endogenous constructs in the TPB model.
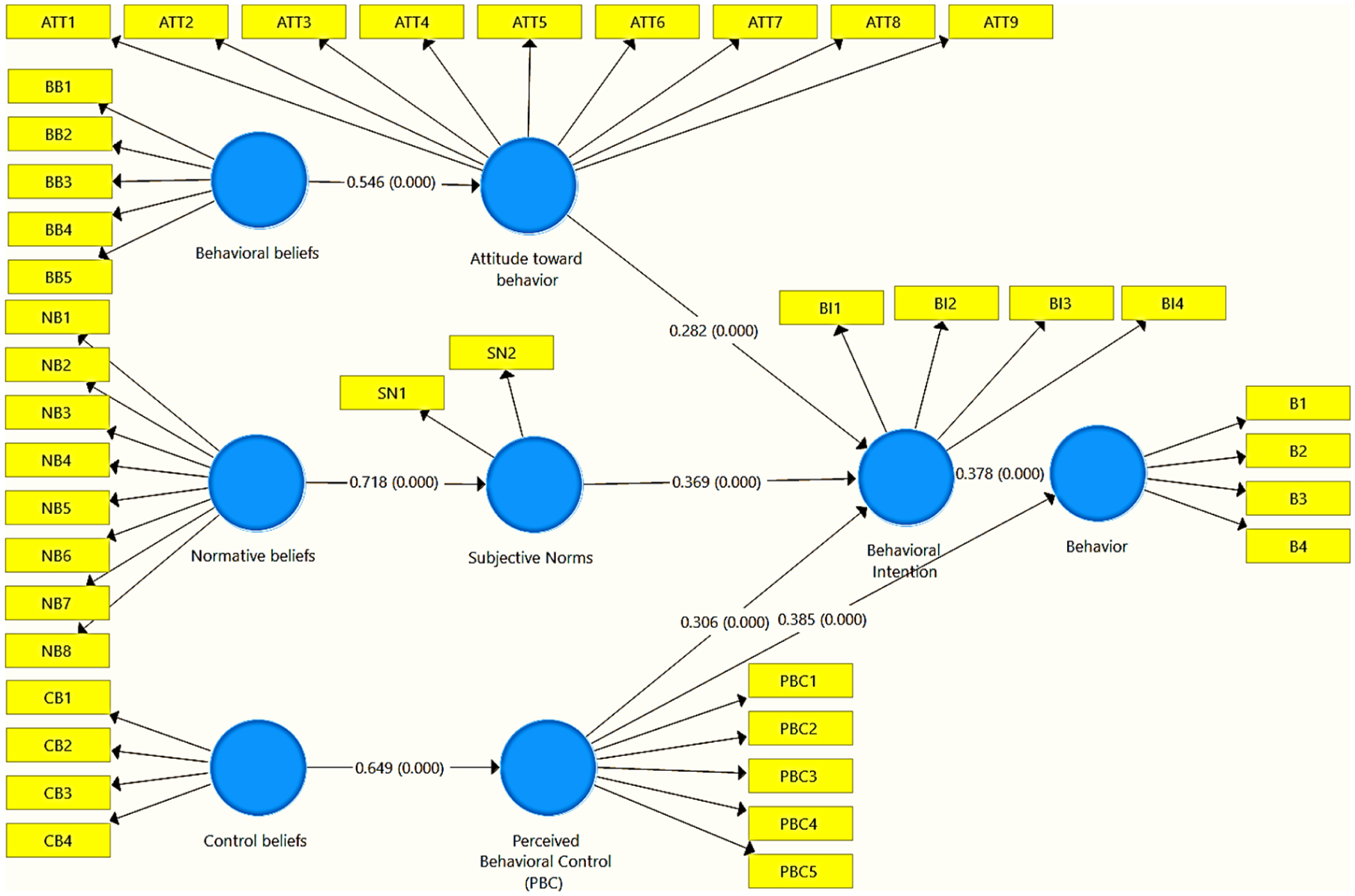
Bootstrapping results showing standardized path coefficients (β) and corresponding P values for structural relationships in the theory of planned behavior model.
The research model was rigorously examined through measurement model fit, structural model fit, overall model fit, and model fit assessment. In other words, first, using reliability and validity criteria, the accuracy of the relationships in the measurement model was ensured, and then the relationships in the structural model were examined and interpreted. Finally, the overall model fit and model fit assessment were examined.
To assess the reliability of the model, Cronbach’s alpha, composite reliability (CR), and outer loadings were assessed. According to Cronbach’s alpha results, items with values below .4 should be removed, values between .4 and .6 require further inspection, and values of .7 or higher indicate acceptable reliability. According to Hair et al, the acceptable threshold for composite reliability and outer loadings is above 0.7. Additionally, items with outer loadings between 0.4 and 0.7 are considered acceptable only if their removal does not improve composite reliability and average variance extracted (AVE), or if such removal results in minimal changes. 22
In the assessment of the measurement model validity, convergent validity was evaluated using the average variance extracted (AVE) criterion, where values >0.5 indicate adequate convergent validity of the model. Moreover, divergent validity was assessed using the Fornell-Larcker criterion and the Heterotrait-Monotrait (HTMT) ratio. According to the Fornell-Larcker criterion, the average variance extracted for each construct, found on the diagonal of the matrix, should be greater than the shared variance between that construct and other constructs (ie, the correlations reported in the off-diagonal elements of the matrix). HTMT values should also be <0.9 to indicate good discriminant validity of the model. 23
In the assessment of model fit, the fit of the measurement model was evaluated using the construct cross-validated communality (CV Com), where positive values indicate acceptable quality and values closer to +1 represent a better fit. Structural model fit was assessed by examining relationships between variables through standardized path coefficients and their t-values, coefficients of determination (R2), effect sizes (f2), and construct cross-validated redundancy (Q2). 24 t-values were used to determine the statistical significance of relationships. R2 was interpreted as the proportion of variance in each endogenous (dependent) construct explained by its predictors, with values around 0.19, 0.33, and 0.67 typically considered weak, moderate, and strong, respectively. 22 Effect sizes (f2) quantified the strength of individual paths, with 0.02, 0.15, and 0.35 indicating small, medium, and large effects. Q2 was used to assess the predictive relevance of the model for the endogenous constructs. 24
The overall model fit was assessed through goodness-of-fit (GOF). Wetzels et al proposed 3 thresholds for GOF values, including 0.01, 0.25, and 0.36, representing weak, moderate, and strong fit, respectively. 25
Model fit assessment was conducted using the standardized root mean square residual (SRMR) and RMS Theta indices. For the SRMR criterion, a value below 0.08 indicates a very good model fit, values between 0.08 and 0.1 indicate an acceptable fit, and values above 0.1 indicate a poor model fit. For the RMS Theta index, values <0.12 are considered appropriate. 26
Ethical Approval and Study Implementation
The study received ethical approval from the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.NUMIMG.REC.1403.057 in 2024.9.7) and commenced after obtaining official authorization letters. Participating nurses were fully informed about the study objectives, voluntary participation, and data confidentiality protocols before enrollment. Written informed consent was obtained from all participants who agreed to participate in the research.
Results
Questionnaires were checked for completeness and, finally, 280 fully completed questionnaires were retained for analysis, corresponding to an effective response rate of 91%.
All studied nurses completed the questionnaire. The results showed that the majority of the nurses were female (82.14%), single (52.14%), with a bachelor’s degree (94.64%), employed unofficially (52.14%), and had no managerial experience (81.79%; Table 1).
Sociodemographic Characteristics of the Nurses (n = 280).
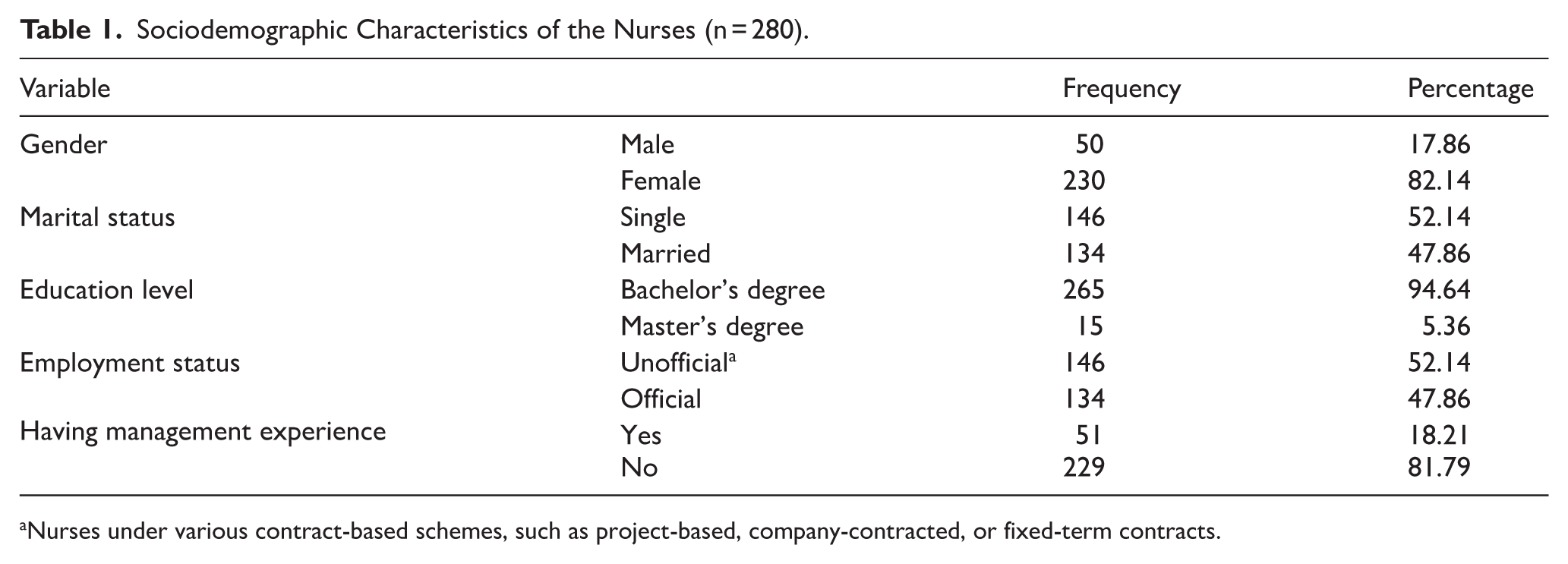
Nurses under various contract-based schemes, such as project-based, company-contracted, or fixed-term contracts.
Also, the results showed that the highest and lowest means were related to attitude toward the behavior (5.05 ± 1.36) and behavior (2.12 ± 0.73), respectively (Table 2).
Descriptive Statistics, Internal Consistency Reliability, and Convergent Validity of the TPB Constructs.
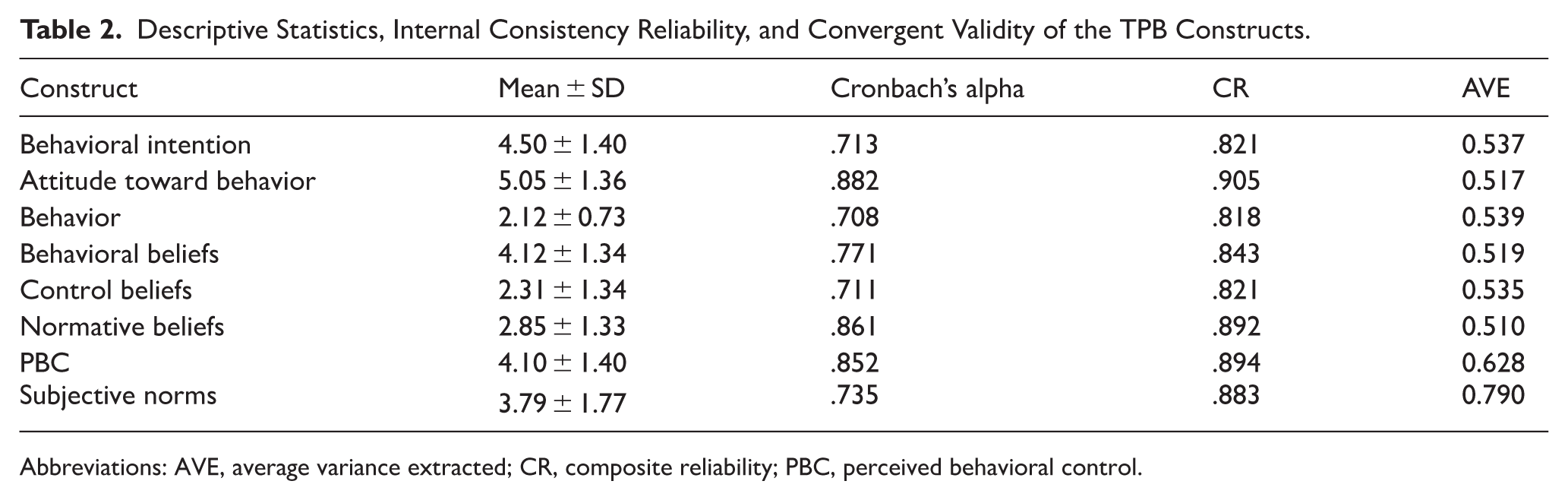
Abbreviations: AVE, average variance extracted; CR, composite reliability; PBC, perceived behavioral control.
As shown in Table 2, for all constructs, the Cronbach’s alpha was above .7, and the composite reliability (CR) was above 0.8, indicating acceptable reliability for the model. Furthermore, the average variance extracted (AVE) values were >0.5, demonstrating that the model had convergent validity.
It should be noted that the values of factor loadings were above 0.7, and in cases where they were between 0.5 and 0.7, removing those items did not change the composite reliability (Figure 2).
The discriminant validity of the model was assessed using the Fornell-Larcker criterion and the HTMT ratio. According to the Fornell-Larcker criterion, the square root of AVE on the diagonal should exceed the correlations of that construct with other constructs; this condition was met for all construct pairs (see Table A1). The strongest correlation was observed between normative beliefs and subjective norms, which is expected given that normative beliefs theoretically underpin subjective norms within the TPB framework. Additionally, all HTMT values fell below the recommended threshold of 0.90, with the maximum value observed for the normative beliefs-subjective Norms pair (HTMT = 0.894), consistent with their theoretical proximity. Taken together, these results indicate acceptable discriminant validity (Table 3 and see also Table A1).
HTMT Ratios of Correlations Between Latent Constructs.
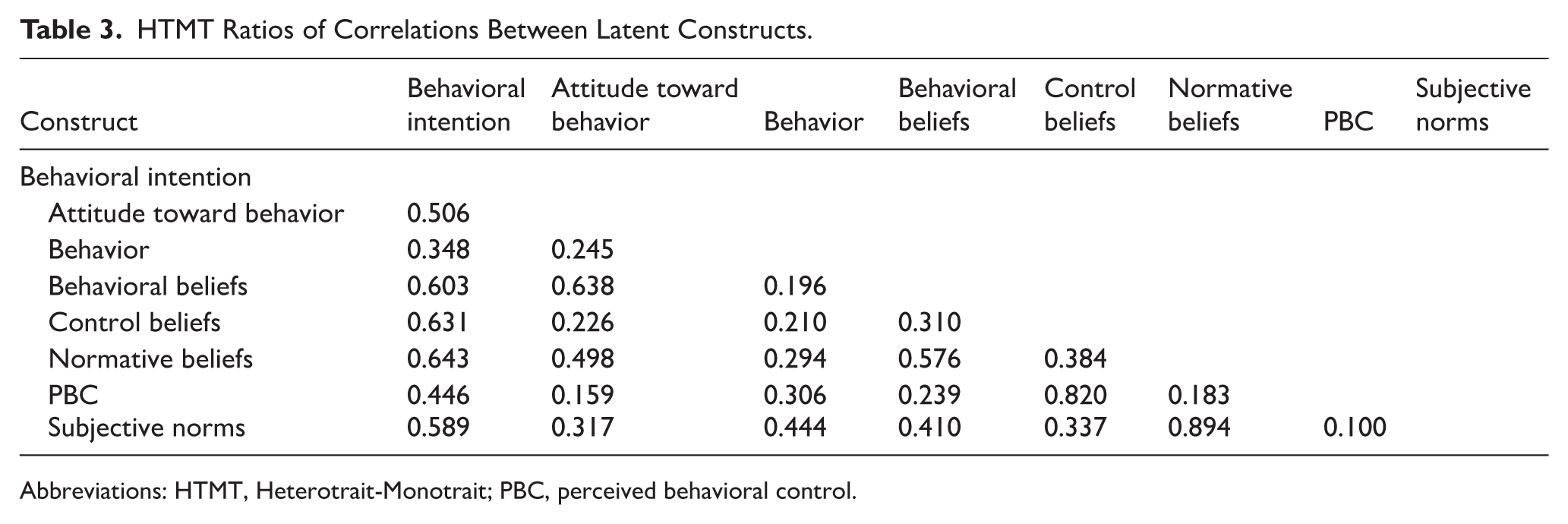
Abbreviations: HTMT, Heterotrait-Monotrait; PBC, perceived behavioral control.
Furthermore, construct cross-validated communality (CV Com) values were computed as a supplementary assessment of measurement model quality. All CV Com values were positive (mean = 0.322), indicating satisfactory predictive relevance and acceptable cross-validation performance of the measurement model (see Table A2).
The t-values and P values indicated that all the direct and indirect paths in the model were significant (t > 1.96, P < .001), and therefore, all constructs of the theory of planned behavior were associated with and demonstrated predictive power for nurses’ behavior in reporting medical errors (Tables 4 and 5). The path coefficients in the study model (Figure 3) showed that subjective norms (β = .369), perceived behavioral control (β = .306), and attitude toward behavior (β = .282) significantly predicted behavioral intention. Perceived behavioral control (β = .385) and behavioral intention (β = .378) also significantly predicted nurses’ behavior in reporting medical errors and showed a significant association with it. Taken together, these results suggest that, among the TPB constructs included in the model, perceived behavioral control and behavioral intention were the strongest predictors of nurses’ reporting behavior, whereas subjective norms and attitude primarily acted as important antecedents of behavioral intention, with subjective norms showing the largest coefficient among predictors of behavioral intention (β = .369), suggesting that social normative pressures from colleagues and supervisors played a particularly important role in shaping nurses’ intentions to report errors. Notably, the relatively comparable magnitudes of perceived behavioral control (β = .385) and behavioral intention (β = .378) on behavior suggested that both volitional control and motivational readiness were equally critical determinants of nurses’ error reporting, with neither dominating the other in this clinical context.
Direct Effects in the Structural Model: Standardized Path Coefficients (β), t-Statistics, and P Values.
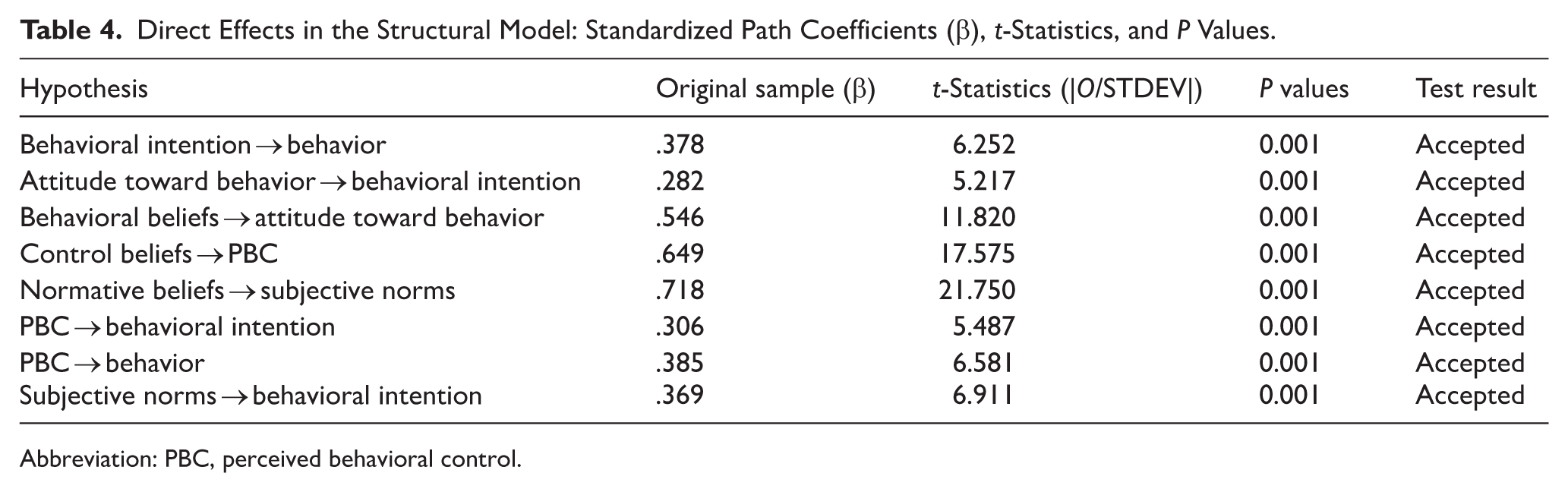
Abbreviation: PBC, perceived behavioral control.
Indirect (Mediated) Effects in the Structural Model Based on Bootstrapped Standardized Coefficients (β).
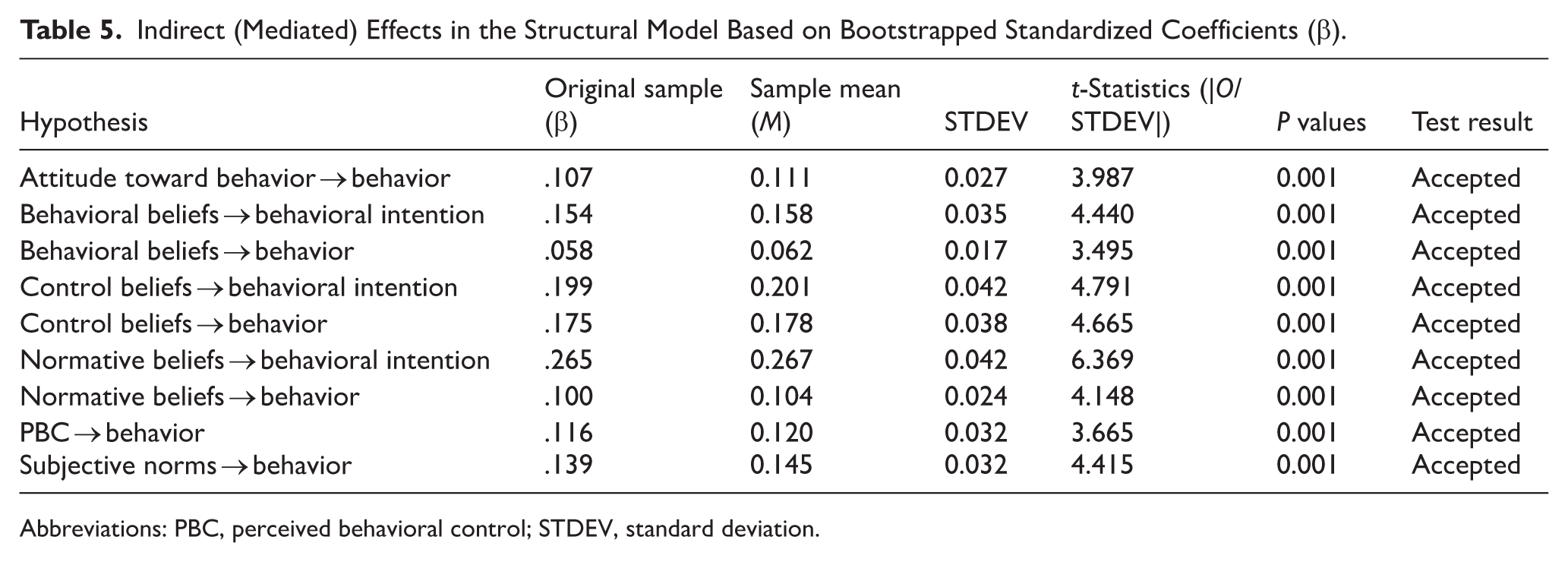
Abbreviations: PBC, perceived behavioral control; STDEV, standard deviation.
The R2 values (Table 6) and the effect size (f2) values (Table 7) indicated that the model had a moderate to strong structural fit.
Coefficients of Determination (R2) for Endogenous TPB Constructs.

Abbreviation: PBC, perceived behavioral control.
Effect Sizes (f2) for Structural Paths in the TPB Model.
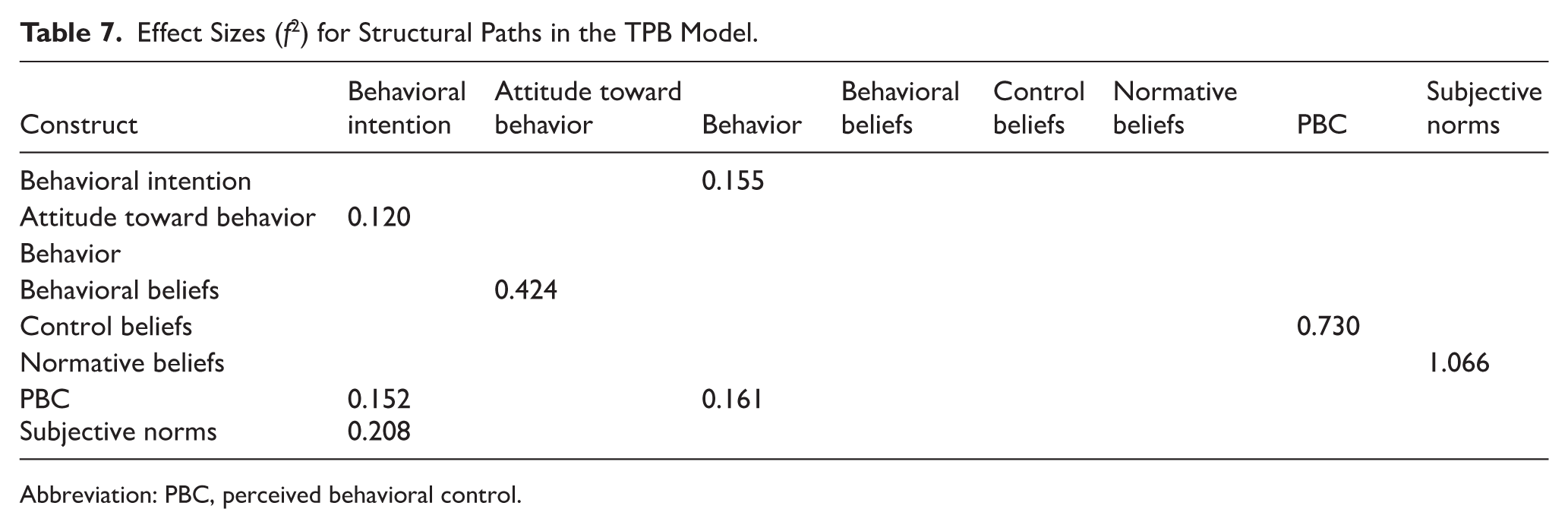
Abbreviation: PBC, perceived behavioral control.
According to the results, the mean of R2 was 0.363, which reflects a relatively good predictive power of the model in the studied sample (Table 6 and Figure 2). These findings suggest that the predictor variables in the theory of planned behavior play an effective role in explaining the variations of behavioral constructs and in accounting for nurses’ behavioral intention to report errors.
As mentioned, the effect sizes (f2) of the paths indicated the strength of the impact each predictor construct had on the dependent variables and highlighted the key role of some paths. Accordingly, control beliefs had the largest effect on perceived behavioral control (f2 = 0.730), and behavioral beliefs significantly influenced attitude toward behavior (f2 = 0.424). Based on the f2 benchmarks described in the “Methods” section, these f2 values indicated very large effects for control beliefs and normative beliefs, and medium-to-large effects for behavioral beliefs, perceived behavioral control, and behavioral intention, suggesting that these relationships are not only statistically significant but also of practical importance for nurses’ error reporting behavior. Other paths exhibited small to moderate effects (Table 7 and Figure 2). In other words, paths with higher effect sizes contribute more to explaining the variations in constructs and align with the R2 values, meaning that paths with high f2 values play an important role in increasing R2 for each construct.
Based on the results, perceived behavioral control (β = .385; f2 = 0.161) and behavioral intention (β = .378; f2 = 0.155) showed the strongest direct associations with nurses’ behavior in reporting errors (Tables 4 and 7). At the underlying construct level, control beliefs (β = .649; f2 = 0.730) and normative beliefs (β = .718; f2 = 1.066) had very strong associations with the intermediate variables of perceived behavioral control and subjective norms, which themselves were strongly associated with behavioral intention and ultimately with behavior (Tables 4 and 7, and Figure 2). Therefore, although “behavioral beliefs” played a significant role in shaping attitude toward behavior (β = .546; f2 = 0.424), its direct contribution to accounting for behavior was very limited and mostly acted indirectly (β = .058; Table 5). For all reported indirect paths, the 95% bootstrap confidence intervals did not include zero, confirming the statistical significance of these mediation effects. Overall, the pattern of significant direct and indirect paths (Tables 4 and 5) suggested a statistical mediation structure consistent with the TPB, whereby attitude toward behavior, subjective norms, and perceived behavioral control were associated with behavior partly through behavioral intention, and control beliefs and normative beliefs influenced behavior indirectly via perceived behavioral control and subjective norms, underscoring that underlying belief structures serve as critical foundations for the more proximal TPB constructs.
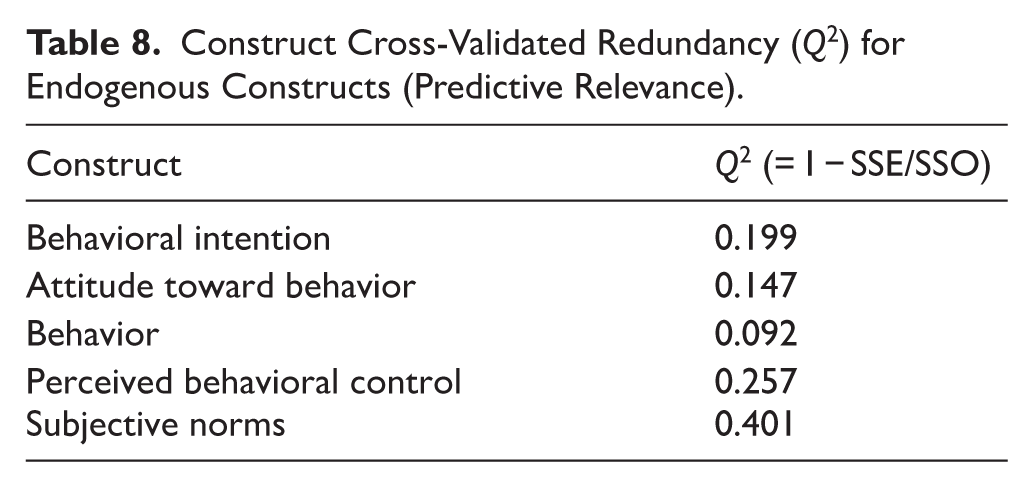
The construct cross-validated redundancy (Q2), which evaluates out-of-sample predictive capability, provided complementary results to R2 and f2, indicating that the model not only explained variations within the sample but also possessed the ability to predict the constructs. According to the results in Table 8, the model exhibited weak predictive power for attitude toward behavior (Q2 = 0.147) and behavior (Q2 = 0.092); moderate predictive power for behavioral intention (Q2 = 0.199) and perceived behavioral control (Q2 = 0.257); and strong predictive power for subjective norms (Q2 = 0.401). These findings demonstrate that paths with strong effects (high f2) and appropriate R2 offer better out-of-sample prediction, confirming the alignment between the predictive relevance (Q2) and explanatory power (R2) of the model (Table 8).
Construct Cross-Validated Redundancy (Q2) for Endogenous Constructs (Predictive Relevance).
In line with the current PLS–SEM practice, model fit was mainly evaluated using SRMR, R2, and Q2. The saturated model’s SRMR was below 0.08, the estimated model’s SRMR was between 0.08 and 0.10, and RMS Theta was 0.119, indicating an acceptable fit. In addition, the traditional GOF index was computed for comparability with earlier PLS-SEM studies and had a value of 0.342 (based on the mean CV Com = 0.322 and the mean R2 = 0.363), but it was not used as a primary criterion for model evaluation.
Discussion
Reporting of medical errors by nurses is a key factor in increasing patient safety and improving the quality of healthcare services, as this process enables the identification and analysis of the causes of errors and prevents their recurrence. 8 Therefore, it is necessary to determine the factors affecting the reporting of medical errors by nursing staff. The need to find these factors is because awareness of these factors helps health managers and policymakers to identify and remove existing barriers and create a safe and supportive environment for reporting, which ultimately leads to a reduction in errors and an increase in the quality of healthcare. 27 There are various theories to identify factors affecting the occurrence of individual behavior, one of which is the theory of planned behavior. Since, according to studies, a wide range of individual, motivational, organizational, etc, factors can have an effective role in the behavior and performance of nurses in clinical environments, the application of this theory provides the best information regarding the factors related to and effective in nurses’ behavior. 27 This study aimed to predict the factors affecting medical error reporting among nurses working in teaching hospitals of Shiraz University of Medical Sciences in 2024.
Model Fit and Predictive Power
The results indicated that the model demonstrated a relatively strong overall fit, and all constructs were associated with and demonstrated predictive power for behavior and had significant direct and indirect paths on behavior. Accordingly, the model based on the theory of planned behavior has acceptable predictive power and shows consistent associations with nurses’ behavior in reporting medical errors.
Furthermore, the findings showed that among the constructs influencing nurses’ behavior in this study, perceived behavioral control and behavioral intention were the strongest direct predictors of behavior (both with medium effect sizes), while control beliefs and normative beliefs had the largest indirect contributions via perceived behavioral control and subjective norms.
Perceived Behavioral Control
The results of the present study revealed that perceived behavioral control was significantly associated with behavior. This means that nurses are more likely to report medical errors when they feel they have sufficient control over the implementation of the behavior, and there are no significant barriers to reporting medical errors. In other words, perceived behavioral control means nurses’ beliefs about their capabilities, resources, opportunities, and facilities needed to perform the reporting behavior, and the stronger and more positive these beliefs are, the stronger their intention and the greater the likelihood that they will actually report medical errors. This strong association may reflect cultural and organizational realities such as fear of punitive consequences, hierarchical work environments, the absence or weakness of clear non-punitive reporting systems, and consistent managerial support that undermine nurses’ perceived ability and willingness to report errors. 28 In general, when a nurse is in an environment where he/she is not afraid of the negative consequences of reporting an error and is supported, his/her perceived behavioral control increases, leading to desirable behavior. This result aligns with the findings of Alotaibi in Saudi Arabia, 29 Braiki et al in Canada, 16 Fernandez et al in Australia, 14 Abuliezi et al in Japan, 30 Woo and Avery in Singapore, 31 as well as Khosravi et al, 32 Ghaseminik et al, 27 Mollaei et al 33 in Iran.
Behavioral Intention
The findings also demonstrated that behavioral intention was significantly associated with behavior. The stronger the individual’s behavioral intention, the greater the likelihood of performing the behavior. In other words, the stronger the nurse’s desire and intention to perform error reporting behavior, the greater the likelihood of actually performing the reporting behavior, and this intrinsic motivation plays an important role in guiding his/her performance. This result is consistent with the results of the studies by Braiki et al in Canada, 16 Abdelmaksoud et al in Australia, 12 Abdollahi et al, 34 and Ghaseminik et al 27 in Iran. Taken together, these findings support the view that behavioral intention is a key driver of reporting behavior in our TPB-based model, partly mediating the influences of attitude, subjective norms, and perceived behavioral control.
Indirect Effects of Attitude, Norms, and Perceived Behavioral Control
Furthermore, the findings of the present study showed that the constructs of attitude toward behavior, subjective norms, and perceived behavioral control had significant indirect relationships with behavior. This means that these 3 constructs were indirectly associated with actual behavior through their influence on the individual’s intention (behavioral intention). In other words, the findings suggest that nurses who have a positive attitude toward error reporting, believe that reporting errors contributes to improving patient safety, reducing injuries, and enhancing work processes, show greater willingness and intention to perform error reporting behavior, which indirectly leads to the actual performance of this behavior, that is, reporting errors, through increased behavioral intention. Moreover, if a nurse perceives that important individuals in their work environment (such as the healthcare team or managers) expect or approve of error reporting, this social pressure may strengthen the nurse’s intention to report errors. Also, if nurses feel that they can report errors easily and without obstacles, this feeling is associated with increased willingness to report medical errors. And ultimately, this willingness and intention may lead to the behavior. This result is consistent with the findings of the studies by Dargahi et al 35 and Dionisi et al in Italy. 36 Overall, these findings support the TPB assumption that attitude toward behavior, subjective norms, and perceived behavioral control shape actual reporting behavior mainly by strengthening their behavioral intention.
Indirect Influences of Beliefs
Moreover, the findings of the present study indicated that behavioral beliefs, normative beliefs, and control beliefs had significant indirect relationships with behavior. In other words, nurses who have positive beliefs about the outcomes of error reporting (eg, helping to improve treatment processes), perceive that they have the necessary control to report, and believe that important others (such as colleagues, managers, or the professional community) expect them to report errors, tend to report stronger intentions to report errors, and such intention in turn are linked to a higher likelihood of actually engaging in error reporting behavior. Also, control beliefs, which include perceptions of barriers (such as fear of negative consequences or lack of support from colleagues) and environmental facilitators related to reporting (such as managers’ attitudes and sense of personal responsibility), are important factors that are indirectly linked to nurses’ error reporting behavior. In other words, even if nurses are aware of the positive consequences of error reporting and are aware of social expectations about performing this behavior, their success in converting this intention into actual action largely depends on the extent to which they feel they can overcome the barriers and whether their work environment provides the necessary support. This suggests that providing a supportive environment and reducing barriers play a key role in nurses’ error reporting behavior, and without considering these factors, even positive intentions may not translate into actual action. These results are in line with the findings of studies by Munn et al in the United States, 37 as well as the studies by Khajouei et al 8 and Abry et al 38 in Iran.
Taken together, these findings highlight a hierarchical pathway from behavioral, normative, and control beliefs to the main TPB constructs (attitude toward behavior, subjective norms, and perceived behavioral control) and then to behavioral intention and behavior, suggesting that effective interventions should target both underlying beliefs and the immediate determinants of behavior (intention and perceived control).
Study Limitations
Like other studies, this study has some limitations. First, its cross-sectional design precludes causal inference; therefore, the reported relationships should be interpreted as non-causal associations and predictive relationships within the TPB framework rather than causal. Second, data were collected only from nurses working in teaching hospitals, which may limit the generalizability of the findings to nurses in non-teaching, private, or rural hospitals and also to other regions or countries with different healthcare systems. In addition, all variables were measured using the self-report questionnaire, and the model focused only on TPB constructs.
Finally, it should be noted that in countries characterized by hierarchical organizational structures and a blame-oriented culture toward error disclosure, social desirability bias in self-reported responses can be prevalent, and the existence of the collectivist cultural orientation in such countries may shape subjective norms differently from other countries, which can limit the cross-cultural generalizability of the findings.
Conclusion
Based on the study results, the model used in this research demonstrated appropriate measurement, structural, and overall fit. Perceived behavioral control, behavioral intention, and control beliefs were identified as the most important predictors of nurses’ behavior in reporting medical errors. In other words, nurses who feel that they have the necessary resources, a safe environment, opportunities, and skills to report errors, along with a strong intention to perform this behavior, are more likely to engage in error reporting. These findings highlight the importance of the organizational environment and individual perceptions in shaping error reporting behavior. In addition to explaining behavior, these results provide a clear framework for designing managerial interventions and educational programs aimed at creating a safe and motivating environment for error reporting, ultimately contributing to improved patient safety and healthcare quality.
Based on the findings of the present study and to increase medical error reporting, it is recommended to facilitate access to error reporting systems to reduce existing technical and time-related barriers in the reporting process; giving continuous feedback about reported errors to nurses and providing them with positive consequences to continue this behavior; conducting regular training courses on the importance of error reporting to strengthen nurses’ intention to report medical errors; offering various rewards to nurses for timely and accurate reporting of medical errors to maintain their motivation; and creating continuous supportive mechanisms such as counseling and advisory systems, removal of barriers to reporting, and ensuring explicit and active support from managers.
Future studies can be conducted on investigating interventions aimed at strengthening nurses’ intention and perceived control to enhance reporting behaviors, and also studying other individual, organizational, and system-level factors contributing to error reporting using other models predicting the behavior.
Footnotes
Appendix
Construct CV Com Values for Latent Variables.

| Construct | CV Com |
|---|---|
| Behavioral intention | 0.252 |
| Attitude toward behavior | 0.404 |
| Behavior | 0.289 |
| Behavioral beliefs | 0.294 |
| Control beliefs | 0.210 |
| Normative beliefs | 0.381 |
| PBC | 0.405 |
| Subjective norms | 0.336 |
| Mean | 0.322 |
Abbreviations: CV Com, cross-validated communality; PBC, perceived behavioral control.
Acknowledgements
The present article was extracted from the thesis written by Omolbanin Izadi and was financially supported by Shiraz University of Medical Sciences grant no 30734. The researchers would like to thank the studied nurses for their kind cooperation with the researchers in collecting and analyzing the data.
Ethical Considerations
The study received ethical approval from the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.NUMIMG.REC.1403.057 in 2024.9.7) and commenced after obtaining official authorization letters.
Consent to Participate
Participating nurses were fully informed about the study objectives, voluntary participation, and data confidentiality protocols before enrollment. Written informed consent was obtained from all participants who agreed to participate in the research.
Author Contributions
RR and OI contributed to the idea and design. OI and MN contributed to the data collection. RR, ARM, SD, and OI contributed to the data analysis. All authors contributed to the manuscript writing and revision. All authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.