
Abstract
Background
Antimicrobial resistance (AMR) is a rapidly expanding worldwide health concern, disproportionately affecting low- and middle-income countries. The Eastern Mediterranean Region (EMR) presents unique issues, including war, inadequate surveillance systems, and widespread antibiotic abuse.
Objective
This study evaluates AMR burden, mortality changes between 2013 and 2023, and progress toward AMR reduction milestones in EMR nations using Global Burden of Disease (GBD) AMR-based indicators.
Methods
This ecological analysis used publicly available IHME and GBD-AMR estimates to examine AMR mortality rates (per 100,000), burden categories, milestone achievements, and AMR ranking among the top 10 causes of death in 2013 and 2023 across EMR countries.
Results
AMR mortality in the EMR ranged from 4 to 75 deaths per 100,000, with Gulf countries reporting the lowest rates and Pakistan, Afghanistan, Somalia, Yemen, and Djibouti the highest. Twelve countries made no progress between 2019 and 2023, while nine achieved reductions in AMR mortality. In Pakistan, Afghanistan, Somalia, Yemen, and Sudan, AMR ranked among the top 10 causes of death in 2013 and/or 2023, unlike most other EMR countries.
Conclusion
AMR burden in the EMR varies widely, rising in high-burden, conflict-affected countries with little improvement. Strengthening labs, stewardship, and surveillance is essential. This study provides regional baseline data to guide targeted interventions and national AMR plans.
Introduction
Antimicrobial drugs are essential for preventing and treating infectious diseases. 1 The problem of antibiotic resistance emerged shortly after the first antibiotic was discovered. 2 Antimicrobial agents are categorized as either bactericidal or bacteriostatic, and they employ several strategies to stop germs from causing disease. 3 One class of antimicrobial drugs with distinct targets is the class of antibiotics. 4 As a result, bacteria constantly employ various strategies to evade the effectiveness of antibiotics. 5
Antimicrobial resistance (AMR), which directly caused 1.27 million deaths in 2019 and is predicted to cause 10 million deaths annually by 2050 if left uncontrolled, is a danger to world health. 6 Methicillin-resistant Staphylococcus aureus (MRSA), carbapenem-resistant Enterobacteriaceae, and extensive drug-resistant tuberculosis are examples of resistant pathogens that make treatments ineffective, according to the World Health Organization (WHO). 7 Antibiotic overuse in human health, agriculture, and industry creates resistance through selective pressure, leading to longer hospital stays, higher mortality rates, and increased financial expenses.6,8,9
A rapidly expanding global health problem, antimicrobial resistance (AMR) makes first-line treatments for several dangerous infectious diseases, such as gonorrhea, HIV, tuberculosis, and malaria, ineffective.7 and 10 Regional factors like violence, inadequate health services, and restricted access to effective medications exacerbate the problems associated with antimicrobial resistance (AMR) in the Eastern Mediterranean Region (EMR).11 and 12 The absence of coordinated AMR surveillance exacerbates these problems and makes it challenging to determine the actual scope of the issue.11 and 13 Recent data indicates concerning patterns in resistance levels throughout the EMR, especially in nations impacted by violence.14
There are still large data gaps in EMR nations, despite improvements in worldwide AMR surveillance. A consistent framework for comprehending mortality changes between 2013 and 2023 and burden patterns is provided by estimates from the Global Burden of Disease (GBD) research and IHME. Nevertheless, AMR burden, mortality categories, milestone accomplishments, and changes in AMR as a primary cause of death throughout the EMR have not been thoroughly investigated in any regional study. This study aims to estimate AMR mortality rates across EMR countries, categorize nations by AMR burden levels, identify those achieving AMR mortality reduction milestones, and determine whether AMR ranked among the top 10 causes of death in 2013 and 2023. Unlike prior GBD-based reports, this study goes beyond descriptive estimates by integrating trend analysis, milestone-based performance assessment, burden stratification, and cause-ranking contextualization to provide a policy-oriented regional evaluation of AMR in the EMR.
Methods
Study Design
A descriptive ecological analysis was conducted using GBD-based AMR indicators to compare antimicrobial resistance mortality and burden patterns across countries in the Eastern Mediterranean Region.
Data Collection
Data were compiled using IHME Health Metrics’ “Health by Location Profiles” and GBD AMR burden outputs for 2013-2023. The analysis included four key indicators: AMR mortality rates (all drug-resistant pathogens per 100,000 population), AMR burden categories adapted into six severity levels, milestone achievement defined as a ≥20% reduction in AMR-related mortality from 2013 to 2023, and AMR’s ranking among the top 10 causes of death in 2013 and 2023.
Milestone achievement was defined as a ≥20% reduction in AMR-attributable mortality rates between 2013 and 2023. This threshold was selected to represent a substantial and policy-relevant improvement in population-level AMR outcomes over a decade. The choice of the 20% cut-off was informed by several considerations. First, it aligns with commonly used benchmarks in global health, where relative reductions of 20–30% are frequently applied to denote meaningful progress in mortality reduction across infectious diseases and public health programs. Second, a 20% reduction exceeds expected random variation and short-term fluctuations in mortality estimates, thereby increasing the likelihood that observed changes reflect true improvements in antimicrobial stewardship, infection control, or healthcare system performance. Third, exploratory assessment of the data distribution indicated that a 20% threshold provided adequate discrimination between countries, avoiding excessive classification of minor changes as success while still identifying a meaningful subset of countries demonstrating progress. Lower thresholds (e.g., 10%) risk overestimating progress due to variability, whereas higher thresholds (e.g., ≥30%) would be overly restrictive and potentially overlook important but realistic gains within the study period. Accordingly, the ≥20% reduction threshold was adopted as a balanced and interpretable indicator of meaningful progress, suitable for comparative analysis across countries with heterogeneous baseline burdens.
Study Population and Eligibility Criteria
The unit of analysis for this ecological study was country-level population estimates, rather than individual subjects. All countries classified within the Eastern Mediterranean Region (EMR) by the World Health Organization were initially considered for inclusion.
The Eastern Mediterranean Region (EMR), as defined by the World Health Organization, comprises 22 countries. All EMR countries were initially assessed for eligibility.
Inclusion criteria included: (1) classification as an EMR country, and (2) availability of complete antimicrobial resistance (AMR) mortality and burden estimates from the Institute for Health Metrics and Evaluation Global Burden of Disease (GBD) and GBD Antimicrobial Resistance (GBD-AMR) databases for both baseline year (2013) and endpoint year (2023). No countries were excluded, as all 22 EMR countries had complete and comparable AMR data across the study period. Accordingly, all 22 EMR countries were included in the final analysis: Afghanistan, Bahrain, Djibouti, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Pakistan, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, United Arab Emirates, Yemen, and Palestine.
Ethical Approval
All data used in this study were obtained from publicly accessible datasets provided by the Institute for Health Metrics and Evaluation through the Global Burden of Disease Study Results Tool and Health by Location Profiles. These data are available for research use with appropriate attribution, and all analyses conducted in this study comply with IHME data use and citation requirements. No primary data collection involving human participants was performed. Therefore, ethical approval and informed consent were not required. The authors independently extracted, analyzed, and synthesized the data to generate novel comparative indicators and region-specific interpretations.
Data Analysis
All data were analyzed descriptively using aggregated, country-level estimates. AMR mortality rates were compared across EMR countries, and each nation was classified into one of six predefined AMR burden categories. Milestone achievement was assessed by calculating the relative percentage change in AMR-related mortality between 2013 and 2023, with a 20 percent or greater reduction indicating progress. AMR rankings within the top ten causes of death were identified using CODEm-derived mortality profiles for both years. Results were synthesized using tables and visual comparisons to highlight regional patterns and disparities; no individual-level data were used.
Results
AMR Mortality Rate per 100,000 Population in EMR Countries
AMR Mortality Rate per 100,000 Population in EMR Countries (2021)

Note. AMR = Antimicrobial Resistance; EMR = Eastern Mediterranean Region; UI = Uncertainty Interval. All values represent estimated AMR-attributable mortality rates per 100,000 population for the year 2021, presented as point estimates with uncertainty intervals.
AMR Burden Categories
To facilitate comparative analysis across the region, countries were classified into six burden tiers based on their estimated AMR-attributable mortality rates (deaths per 100,000 population). Six categories were chosen to provide sufficient granularity to distinguish meaningful epidemiological differences while remaining clinically and operationally interpretable — a smaller number of categories would obscure important heterogeneity (e.g., between Somalia at 1,510 and Kuwait at 286), while more categories would introduce artificial precision given the inherent uncertainty in AMR mortality estimates.
The cutoff thresholds were determined using a tiered, data-driven approach informed by the distribution of values across the study population. The highest tier (Extremely High: >1,000) was defined to capture statistical outliers — countries whose burden is qualitatively distinct from the remainder of the distribution. The Very High tier (700–1,000) and High tier (500–699) demarcate countries with substantially elevated burden where systemic AMR infrastructure failures are likely dominant drivers. The Moderate tier (400–499) represents a cluster of countries with burdens near the regional median, while the Low (300–399) and Very Low (<300) tiers capture countries whose burden, though not negligible, falls below the regional mean and may reflect relatively stronger health system capacity or reporting differences. The 300 deaths per 100,000 lower threshold approximates the regional mean minus one standard deviation, providing a statistically grounded anchor for the scale.
AMR Burden Categories

Note. AMR = Antimicrobial Resistance; EMR = Eastern Mediterranean Region. Burden tiers are based on estimated AMR-attributable mortality rates (deaths per 100,000 population) for 2021. Six categories were defined using a data-driven tiered approach to capture meaningful epidemiological heterogeneity across the region. Values in parentheses represent country-specific mortality rates.
Countries That Achieved AMR Mortality Reduction Milestones (2013–2023)
Countries That Achieved AMR Mortality Reduction Milestones (2013–2023)

Note. AMR = Antimicrobial Resistance; EMR = Eastern Mediterranean Region; NA = Not Applicable (milestone not yet attained as of the study period). Milestone attainment reflects status recorded at available data points within the 2013–2023 study period and does not represent a continuous year-by-year trend analysis. UAE = United Arab Emirates.
Associated and Attributable AMR Deaths
Associated and Attributable AMR Deaths
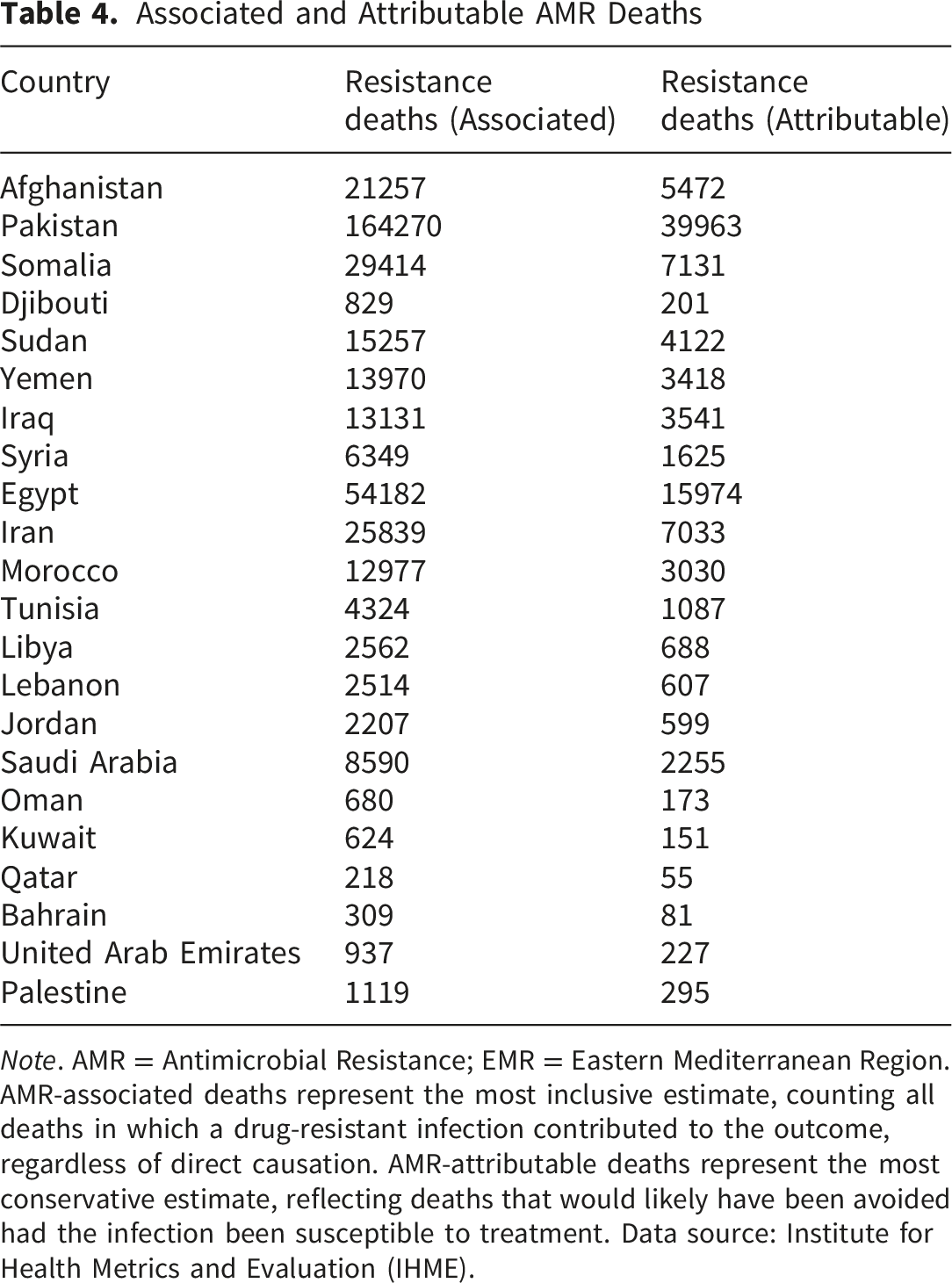
Note. AMR = Antimicrobial Resistance; EMR = Eastern Mediterranean Region. AMR-associated deaths represent the most inclusive estimate, counting all deaths in which a drug-resistant infection contributed to the outcome, regardless of direct causation. AMR-attributable deaths represent the most conservative estimate, reflecting deaths that would likely have been avoided had the infection been susceptible to treatment. Data source: Institute for Health Metrics and Evaluation (IHME).
AMR in the Top 10 Causes of Death
AMR in the Top 10 Causes of Death (2013 Vs. 2023)
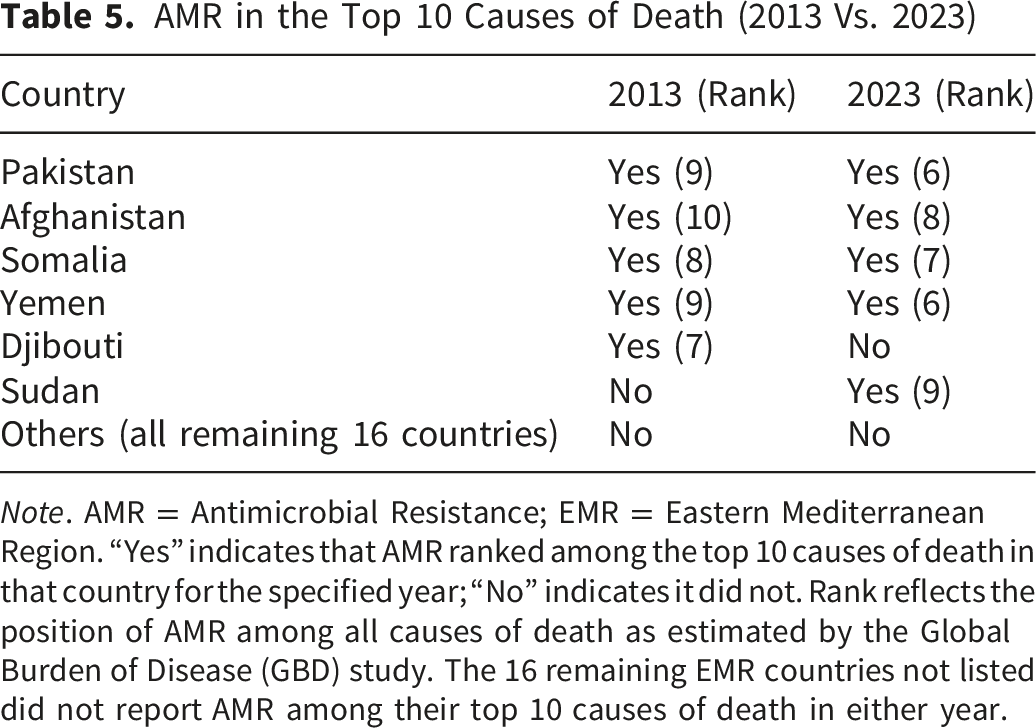
Note. AMR = Antimicrobial Resistance; EMR = Eastern Mediterranean Region. “Yes” indicates that AMR ranked among the top 10 causes of death in that country for the specified year; “No” indicates it did not. Rank reflects the position of AMR among all causes of death as estimated by the Global Burden of Disease (GBD) study. The 16 remaining EMR countries not listed did not report AMR among their top 10 causes of death in either year.
Discussion
This study demonstrates substantial heterogeneity in antimicrobial resistance (AMR)–related mortality across countries in the Eastern Mediterranean Region (EMR) between 2013 and 2023. The highest burdens were consistently observed in Pakistan, Afghanistan, Somalia, Yemen, and Djibouti. While the study design does not permit causal inference, these patterns are consistent with previously documented structural vulnerabilities in these settings — including unregulated antibiotic use, limited healthcare access, weak laboratory infrastructure, and conflict-driven disruption — which have been identified in the literature as drivers of AMR burden in comparable contexts.
Our findings align with previous regional and global reports. Mestrovic et al. identified bacterial AMR as a major public health challenge in the EMR for more than three decades, with a considerable fatal and non-fatal burden linked to priority pathogens and pathogen–drug combinations. 17 Similarly, evidence highlighting disproportionately high mortality in low-resource settings, such as Somalia, underscores the vulnerability of fragile healthcare systems and the urgent need for targeted resource allocation. 18 Global surveillance data further contextualize these patterns, showing a 65% increase in resistant infections between 2000 and 2023, with resistance rates three to four times higher in low- and middle-income countries compared with high-income countries, and AMR-associated deaths approaching 5 million annually. 19
In contrast, Gulf Cooperation Council (GCC) countries consistently demonstrated lower AMR-associated mortality and were more likely to have achieved AMR mortality reduction milestones by the end of the study period. These patterns are consistent with documented investments in healthcare infrastructure, antimicrobial stewardship programs (ASPs), and antibiotic prescribing regulation in these settings, though the present analysis cannot establish a direct causal link between these policies and the observed trends. Evidence from Krishnamoorthy et al. highlights the clinical and economic benefits of ASPs across diverse healthcare settings, 20 while Enani et al. reported significant reductions in hospital-acquired infections and broad-spectrum prescribing in GCC states implementing stewardship initiatives. 21 Taken together, these findings suggest that coordinated stewardship and regulatory frameworks may contribute to lower AMR burden, a hypothesis consistent with — though not confirmed by — the present data.
Notably, AMR emerged as a top ten cause of death only in a subset of EMR countries, further illustrating the profound disparities in AMR burden documented in this analysis. This observation is consistent with global assessments identifying AMR as one of the leading threats to human health worldwide, responsible for millions of deaths annually.22-25
The patterns observed in this study — including the concentration of high burden in fragile and conflict-affected states and the comparatively lower burden in higher-income GCC countries — point to the relevance of systemic and contextual factors that prior literature has linked to AMR outcomes, such as infection prevention capacity, diagnostic availability, and stewardship enforcement. 11 ’26-31 While the present analysis cannot quantify the contribution of these determinants, the findings may help prioritize which country contexts warrant urgent attention and support further targeted investigation.
Strengths and Limitations
This study has several notable strengths, including an EMR-wide standardized analysis of AMR mortality using GBD-compliant methodologies and a milestone-based assessment aligned with global AMR progress-tracking frameworks. The findings provide a descriptive regional overview that may serve as a reference point for future surveillance efforts and hypothesis generation. However, significant limitations should be recognized. The reliance on GBD-based estimations introduces uncertainty due to modeling assumptions and variable data availability across EMR nations, potentially affecting precision. Significant diversity in monitoring capacity and data quality across the region limits comparability, and the analysis does not distinguish pathogen- or drug-specific AMR mortality, thereby masking more granular resistance patterns.
It should be noted that the milestone achievement classification in Table 3 is based on a comparison between 2013 baseline estimates and 2023 endpoint data, and does not reflect a continuous year-by-year trend analysis. Intermediate annual data were not available for the countries included, and therefore, no trend-based inference should be drawn from these findings. Future studies with access to annually resolved data should consider interrupted time-series or joinpoint regression approaches to more rigorously characterize AMR mortality trajectories across the region.
A further important limitation is the absence of country-level contextual review or in-depth national situation assessments. While aggregate regional estimates are presented, this study does not incorporate country-specific factors that are critical for interpreting AMR mortality patterns, such as national antimicrobial stewardship program implementation, healthcare infrastructure capacity, antibiotic prescribing and dispensing practices, infection prevention and control measures, or the regulatory environment governing antibiotic access. This omission limits the interpretability of country-level findings and makes it difficult to draw policy-relevant conclusions at the national level. Observed differences in AMR mortality across EMR countries may reflect disparities in surveillance capacity and data quality as much as true epidemiological variation. Accordingly, the findings presented here should be regarded as hypothesis-generating rather than definitive country-level assessments, and future work should integrate national situational analyses to enable more contextually informed and actionable policy recommendations.
Conclusion
AMR continues to pose a significant threat to public health in the EMR, with high-burden countries showing no progress toward reductions in AMR mortality. Immediate investment in laboratory systems, stewardship programs, and the implementation of a national action plan are essential. The findings serve as a regional baseline for AMR monitoring and provide policymakers with actionable insights to strengthen AMR response strategies.
Future research should prioritize the establishment of longitudinal, standardized surveillance systems across EMR countries to enable trend monitoring and cross-country comparisons over time. Prospective studies are needed to evaluate the effectiveness of national action plans and stewardship interventions, particularly in high-burden settings where progress has stalled. Research exploring the health-system and socioeconomic determinants of AMR burden in the region would further inform targeted policy responses. Additionally, studies examining clinical outcomes associated with resistant pathogens — including mortality, length of hospital stay, and treatment costs — are warranted to strengthen the economic case for AMR investment. Collaborative, multi-country research frameworks will be critical to addressing data gaps and generating the evidence base needed to guide sustained regional action.
Footnotes
Acknowledgement
The authors extend their appreciation to Prince Sattam bin Abdulaziz University for funding this research work through the project number (PSAU/2025/01/33952).
Ethical Considerations
This study utilized publicly available, de-identified secondary data obtained from the Institute for Health Metrics and Evaluation (IHME) Global Burden of Disease (GBD) and GBD Antimicrobial Resistance (GBD-AMR) study databases. As the analysis was based exclusively on anonymized, aggregated data with no individual-level identifiers, ethical approval and informed consent were not required, in accordance with international research ethics guidelines.
Author Contributions
The author was responsible for the conception, design, data collection, analysis, interpretation, and writing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors extend their appreciation to Prince Sattam bin Abdulaziz University for funding this research work through the project number (PSAU/2025/01/33952).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data used in this study are publicly available from the Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease (GBD) data can be accessed at: https://vizhub.healthdata.org/gbd-results/. Data from the Global Burden of Disease Antimicrobial Resistance (GBD-AMR) study are available at: ![]() . No additional proprietary datasets were used. Any data processing scripts or derived datasets generated during the current study are available from the corresponding author upon reasonable request.
. No additional proprietary datasets were used. Any data processing scripts or derived datasets generated during the current study are available from the corresponding author upon reasonable request.