
Abstract
Background and Objective
Burnout among surgeons has become an increasing concern due to its impact on physician well-being, healthcare quality, and patient safety. This systematic review and meta-analysis aims to estimate the global prevalence of burnout and examine variations according to burnout assessment tools and surgical subspecialties.
Methods
A systematic search of PubMed, Scopus, and Web of Science was conducted from inception to November 2025 for studies assessing burnout prevalence among pediatric surgeons and trainees, using validated tools such as the Maslach Burnout Inventory (MBI) or alternatives. Two reviewers independently screened studies, extracted data, and assessed quality using the JBI Critical Appraisal Checklist. A single-arm meta-analysis with a random-effects model was used to calculate pooled prevalence rates, with subgroup analyses based on the assessment tool.
Results
Eighteen cross-sectional studies met the inclusion criteria. A total of 17 studies were included in the meta-analysis. The pooled prevalence of burnout was 30% (95% CI: 21%–41%), with high heterogeneity (I2 = 96.5%). Subgroup analysis revealed a lower burnout prevalence among studies using the MBI (23%, 95% CI: 16%–31%), compared to studies using other tools (50%, 95% CI: 25%–75%). Orthopedic subspecialty had the highest pooled burnout proportion at 42% with a very wide 95% CI of (3% to 94%). Urology had the lowest pooled rate at 26% with a 95% CI of (17% to 37%).
Conclusion
Burnout represents a significant issue among pediatric surgeons. These findings highlight the need for a proactive approach to recognize burnout in healthcare professionals and implement effective strategies for its prevention and management.
1. Introduction
Burnout, a psychological syndrome marked by emotional exhaustion, depersonalization, and a diminished sense of personal accomplishment, is an increasingly recognized occupational hazard in medicine. 1 Burnout was first defined by Freudenberger in 1974 and later formalized by Maslach and her colleagues in the early 1980s.2,3 Burnout is especially common in high-intensity healthcare environments where emotional requirements, workload, and professional demands intersect. 4 Among surgeons, burnout has emerged as a significant concern, with recent data suggesting that over 50% of both trainees and attending surgeons experience symptoms at some point in their careers.5,6
Beyond its impact on physicians themselves, burnout has significant implications for healthcare systems and patient outcomes.4,7 Numerous studies have linked physician burnout with reduced quality of care, increased medical errors, lower patient satisfaction, and higher staff turnover.8,9 In surgical specialties, these consequences may be particularly critical due to the high-stakes nature of operative care, where cognitive fatigue, impaired decision-making, and emotional exhaustion can directly affect patient safety. 10 Furthermore, burnout contributes to decreased productivity, early retirement, and workforce shortages, which may further strain already limited healthcare resources. 11 Recognizing the prevalence and drivers of burnout among surgeons is therefore essential not only for protecting physician well-being but also for maintaining high-quality, sustainable surgical care.
While burnout has been extensively studied across medical and surgical specialties, pediatric surgery provides a unique blend of clinical and systemic stressors that might elevate the risk of burnout.12-14 Pediatric surgeons face a dual burden: the technical demands of managing complex congenital and acquired conditions in infants and children, and the emotional weight of dealing with critically ill young patients and their families.15,16 Furthermore, pediatric surgeons are frequently required to engage in emotionally charged discussions with distressed parents, and navigate complex ethical dilemmas—particularly in cases involving end-of-life care or situations where neonates and children are expected to survive with significant disabilities, or lifelong comorbidities. 17
These dynamics may exacerbate emotional exhaustion and moral distress, core features of burnout. Compounding these challenges are systemic issues: shortages in pediatric surgical workforce, under-resourced pediatric healthcare systems in many regions, and the increasing non-clinical responsibilities associated with modern surgical practice. 18 Although burnout has been examined across surgical specialties, evidence specific to pediatric surgeons remains dispersed across subspecialties, regions, and training levels, making it difficult to form a clear understanding of overall burden.6,12,19-21 The objective of this study was to estimate the pooled prevalence of burnout among pediatric surgeons and to examine variations according to burnout assessment tools and surgical subspecialties.
2. Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 22 The protocol was registered in PROSPERO (CRD420251181384).
2.1. Search Strategy
A comprehensive search was conducted in PubMed, Scopus, and Web of Science (WOS) from inception to November 2025, using the following search terms: burnout, emotional exhaustion, occupational stress, psychological stress, pediatric, paediatric, surgery, surgeon, surgeons, pediatric surgeon, paediatric surgeon, pediatric surgery, surgical trainee, surgical trainees, resident, residents, fellow, and fellows. These terms were selected to capture literature addressing both trainees and practicing pediatric surgeons. Details of search strategies across the databases are demonstrated in Table S1. All retrieved records were imported into EndNote, and duplicates were removed. Two independent reviewers screened titles and abstracts for relevance based on predefined inclusion and exclusion criteria. Full-text articles of potentially eligible studies were then assessed for final inclusion. Additionally, we manually searched the reference lists of included studies and screened the gray literature to ensure that no relevant studies were missed. Any discrepancies between reviewers were resolved through discussion with a third reviewer.
2.2. Eligibility Criteria
We included studies that assessed the prevalence of burnout among pediatric surgeons, including both attending surgeons and trainees, with no restrictions on geographic location, healthcare setting, or publication year. Only studies published in English were eligible. Observational studies such as cross-sectional, cohort, or survey-based designs were considered. We excluded studies not specific to pediatric surgery, as well as conference abstracts, posters, and other publications without full-text availability. Studies that included multiple surgical specialties were only considered if data specific to pediatric surgery could be clearly extracted or analyzed separately, or if the majority were pediatric surgeons. Editorials, commentaries, reviews, and studies lacking clear data on burnout prevalence or sufficient methodological detail were also excluded.
2.3. Data Extraction and Quality Assessment
Two independent reviewers extracted relevant data from each included study using a pre-designed spreadsheet, and any disagreements were resolved through discussion or consultation with a third reviewer. Extracted data included general information (specialty/subspecialty, country, study design, and duration), population and sample characteristics (type of participants, sample size, response rate, complete response rate, gender distribution, and age), and burnout-related data (including assessment tool, definition of burnout, prevalence [events/total], and associated factors). For analysis, we extracted the number of burnout events and total sample size, and subgrouped studies based on the assessment tool used—particularly distinguishing those using the (MBI) from others. In the context of the MBI, burnout is identified when an individual scores high on Emotional Exhaustion (EE) and Depersonalization (DP), and low on Personal Accomplishment (PA). When these patterns emerge consistently in MBI responses, they indicate significant occupational burnout. Quality assessment was conducted using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Studies. 23
2.4. Statistical Analysis
Statistical analysis was performed using R software. A single-arm meta-analysis was conducted to calculate the pooled proportion of burnout among pediatric surgeons, with corresponding 95% confidence intervals (CI), using a random-effects model (REM) to account for between-study variability. Studies were subgrouped based on the burnout assessment tool used, either the MBI or other tools. Moreover, another subgroup analysis based on the surgical subspecialties. Statistical heterogeneity was assessed using the I2 statistic and Cochran’s Q test, with I2 values greater than 50% or a p-value less than 0.1 indicating significant heterogeneity. 24 A funnel plot was generated to visually assess the potential for publication bias. 25 The trim-and-fill method was applied to estimate the number of potentially missing studies and to determine whether adjusting for these studies would meaningfully alter the pooled prevalence estimate.
3. Results
3.1. Search Results
The database search yielded a total of 1,610 records. After removing duplicates, 1,261 records remained for screening. Based on the title and abstract review, 54 full-text articles were assessed for eligibility according to the inclusion criteria. Ultimately, 18 studies were included. Of these, 17 were included in the meta-analysis26-42; one study was excluded as it reported only the mean score of the MBI rather than the proportion of burnout.
43
The PRISMA flowchart illustrating the study selection process is presented in Figure 1. The PRISMA flowchart
3.2. Study Characteristics and Qualitative Synthesis
Characteristics of the Included Studies
ASPN: American Society of Pediatric Neurosurgeons; WBI: Well-Being Index; NA: Not Available; CF: Compassion Fatigue; BO: Burnout; CS: Compassion Satisfaction; MBI: Maslach Burnout Inventory; CFST: Compassion Fatigue and Satisfaction Self-Test; EE: Emotional Exhaustion; DP: Depersonalization; PPA: Personal and Professional Achievement; PA: Personal Accomplishment; PSQI: Pittsburgh Sleep Quality Index; POSNA: Pediatric Orthopedic Society of North America; CMBI-GS: Chinese version of Maslach Burnout Inventory-General Survey.
Summary of Burnout Definition, Measurement Instruments, and Contributing Factors
ASPN: American Society of Pediatric Neurosurgeons; WBI: Well-Being Index; NA: Not Available; CF: Compassion Fatigue; BO: Burnout; CS: Compassion Satisfaction; MBI: Maslach Burnout Inventory; CFST: Compassion Fatigue and Satisfaction Self-Test; EE: Emotional Exhaustion; DP: Depersonalization; PPA: Personal and Professional Achievement; PA: Personal Accomplishment; PSQI: Pittsburgh Sleep Quality Index; POSNA: Pediatric Orthopedic Society of North America; CMBI-GS: Chinese version of Maslach Burnout Inventory-General Survey.
The study by Tangul et al wasn’t included in the meta-analysis since it didn’t report the proportion of participants experiencing burnout, making direct comparison difficult. 43 However, it still provides valuable insights into how working night shifts and being on-call can affect pediatric surgeons’ sleep quality and burnout levels. The study looked at 181 doctors, splitting them into those who worked night shifts or had on-call duties and those who didn’t. Although both groups were similar in terms of age and hours worked, the surgeons with night or on-call shifts had significantly poorer sleep quality and higher burnout scores, including emotional exhaustion and feelings of depersonalization. Interestingly, younger surgeons and those with fewer years of experience tended to have higher burnout, and poorer sleep was closely linked to higher burnout. These findings underscore the detrimental impact of sleep disruption due to night and on-call duties on surgeons’ mental health and suggest that interventions aimed at improving sleep quality may be critical for mitigating burnout and enhancing overall well-being, both professionally and personally.
3.3. Quality Assessment
Table S2 presents the quality assessment of included cross-sectional studies using the JBI Critical Appraisal Checklist. Out of the 18 studies, 14 were rated as being of good quality. Three studies received moderate ratings, each scoring 6 due to limitations in addressing confounding factors and outcome validity.26,28,37 One study was rated as low quality, scoring only 4 points, primarily due to insufficient detail in exposure measurement and confounding control. 34 Overall, most included studies were of satisfactory quality, supporting the reliability of the review’s findings.
3.4. Meta-Analysis
Figure 2 presents a forest plot of burnout prevalence across 17 studies, including a total of 3,104 participants, of whom 1,253 were identified as experiencing burnout based on different tools. The pooled prevalence of burnout was 30% with a 95% confidence interval (CI): 21% to 41%. This variability is statistically supported by a high I2 statistic of 96.5%. Forest plot shows the pooled prevalence of overall burnout among participants across 17 studies using different assessment tools
After subgrouping the included studies based on the burnout assessment tool used, 11 studies that specifically utilized the MBI were analyzed separately. As shown in Figure 3, the pooled burnout prevalence among these MBI-based studies was 23% (95% CI: 16% to 31%). Notably, there was still significant heterogeneity across these studies (I2 = 76%). Forest plot of studies that used the Maslach Burnout Inventory (MBI) to assess burnout prevalence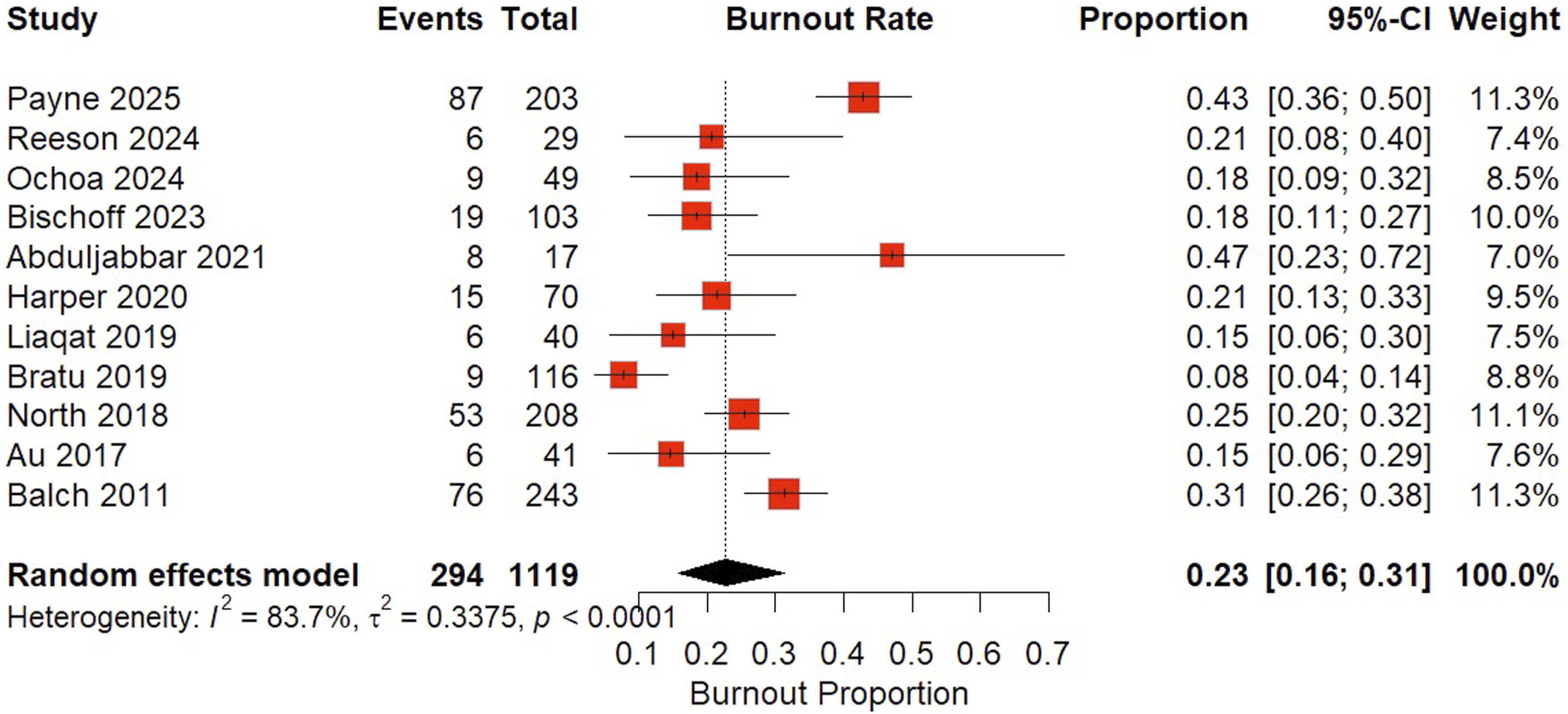
On the other hand, pooling studies that used assessment tools other than the MBI yielded a higher pooled burnout prevalence of 50% (95% CI: 25% to 75%), as illustrated in Figure 4. Forest plot of studies using burnout assessment tools other than the Maslach Burnout Inventory (MBI)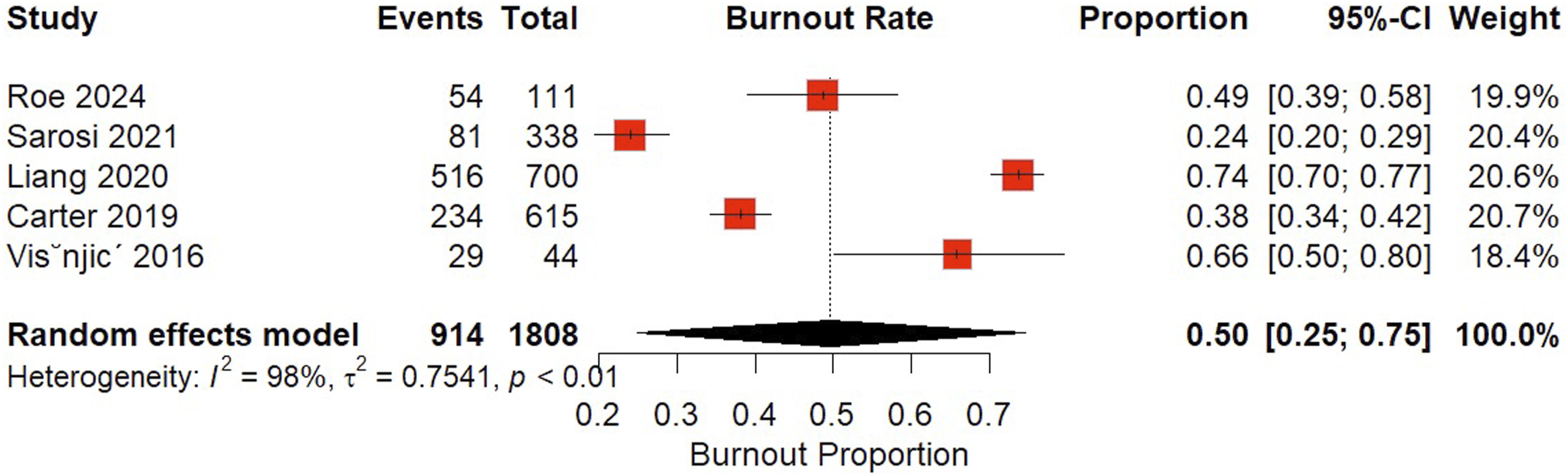
The subgroup analysis of burnout proportions across medical subspecialties (Figure 5) shows that orthopedics had the highest pooled burnout proportion at 42%, with a very wide 95% CI (3% to 94%) and extremely high heterogeneity (I2 = 99%). Urology had the lowest pooled rate at 26% with a 95% CI of (17% to 37%), with high heterogeneity (I2 = 81.1%). The “Other subspecialty or unspecified” subgroup showed a pooled rate of 29% with a 95% CI of (15% to 49%) and high heterogeneity (I2 = 91%). Forest plot of the pooled burnout proportion stratified by subspecialty of pediatric surgery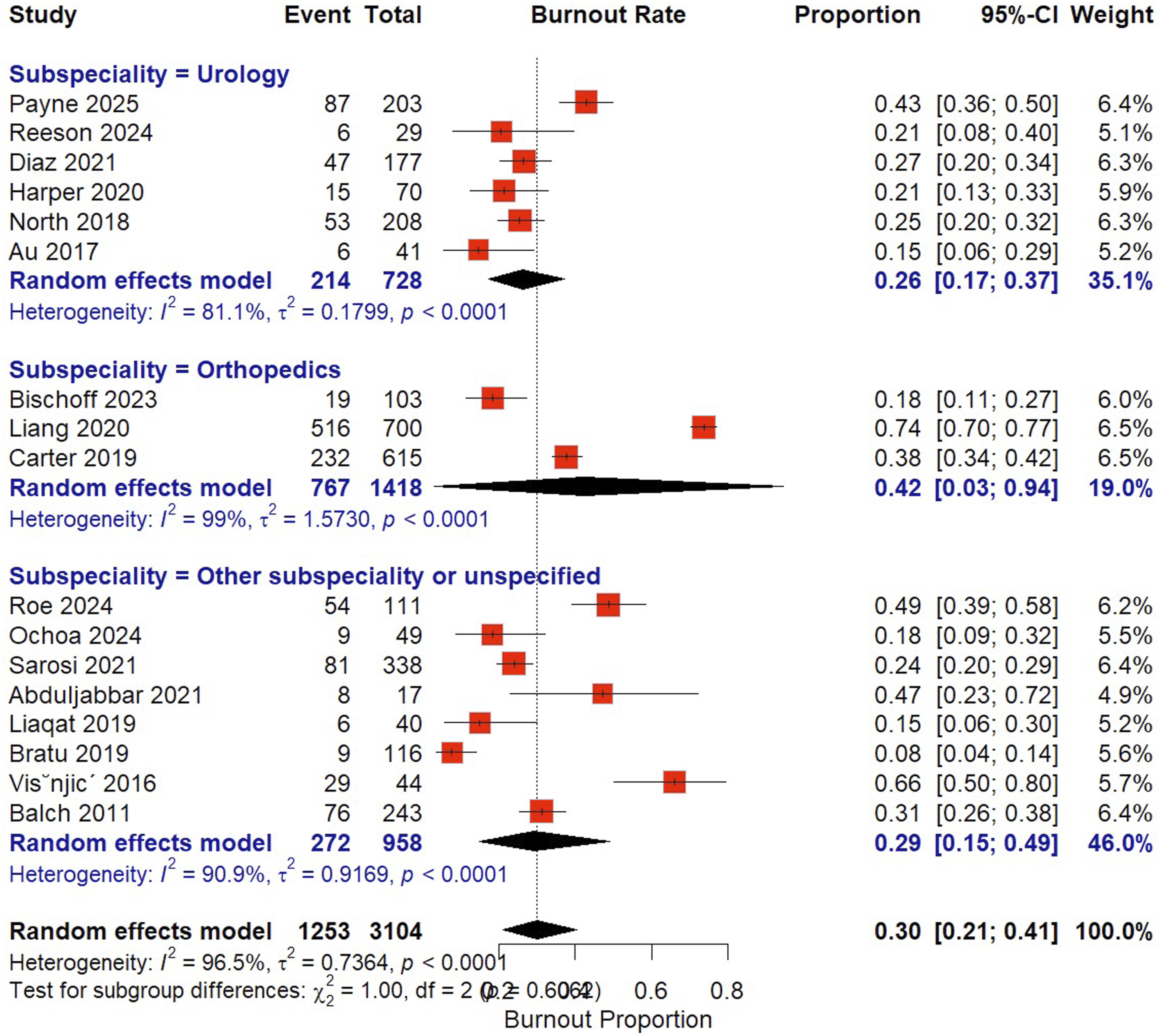
The funnel plot demonstrates the relationship between the logit-transformed event proportion (burnout prevalence) and the standard error across included studies. Visual inspection of the plot shows an approximately symmetrical distribution of studies around the pooled estimate, suggesting no major publication bias (Figure S1). This was supported by Egger’s test (p = 0.0558) and Begg’s test (τ = 0.20, p = 0.2018), both indicating no statistically significant small-study effects (Figure S2).
4. Discussion
We brought together data from eighteen studies examining burnout prevalence among pediatric surgeons of different subspecialties from various parts of the world. Our analysis showed that approximately one in three pediatric surgeons experience burnout, highlighting how common and concerning this issue is in such a demanding subspecialty. However, the numbers varied widely across studies, with high statistical heterogeneity. Further analysis showed that much of this variation was tied to the different tools used to measure burnout. When we looked specifically at studies that used the MBI, the reported burnout rates were notably lower. On the other hand, studies that relied on alternative tools reported much higher burnout rates, up to 50%. These findings underscore two key insights: burnout is a pervasive and serious issue in pediatric surgery, and its assessment methodology critically shapes our understanding and interpretation of its prevalence and impact. The observed differences in burnout prevalence across subspecialties should be interpreted cautiously, as studies varied in geographic settings, working environments, and populations; moreover, the very wide confidence interval for the orthopedic subspecialty (3%–94%) likely reflects the small number of studies, limited sample sizes, and high variability, resulting in an imprecise estimate.
The study by Liang et al reported the highest burnout rate (74%) among the included studies, focusing on Chinese pediatric orthopedic surgeons. 29 They found that younger age, fewer years of experience, longer working hours, and lower income were significant risk factors for burnout. No differences were observed by sex or employment status. The high prevalence in this subspecialty may contribute to the heterogeneity observed across studies. A study of French pediatric orthopedic trainees reported a lower prevalence of burnout compared to the Chinese cohort, 27 with moderate to severe burnout affecting 26% of interns and 13.9% of registrars. Suicidal ideation was reported by 20.8% of the former and 9.2% of the latter. Roe et al reported a higher burnout rate of 49% among pediatric neurosurgeons. 32 The combination of technical difficulty, emotional demands, and systemic challenges likely explains why burnout is more prevalent in pediatric neurosurgery and orthopedic surgery than in general pediatric surgery. 44
Lowe figures from studies using the MBI, in contrast to the high numbers among those employing alternative instruments, demonstrate the impact of measurement tools on the estimated prevalence of burnout. Studies using non-MBI tools often reported substantially higher rates, likely due to reduced specificity, or lower diagnostic thresholds. 45 As a result, they might capture general psychological distress or overlapping conditions rather than clinically significant burnout, potentially leading to inflated prevalence Figure. 46 These observations highlight the importance of utilizing validated tools, such as MBI, in burnout research. Without a consistent methodology, inter-study comparisons become unreliable, and the actual burden of burnout may be either underestimated or exaggerated. The persistent substantial heterogeneity observed in the MBI-based subgroup (I2 = 76%) is likely attributable to differences in surgical subspecialties. In particular, the study by Abduljabbar et al (2021), which focused on spine surgeons, reported a notably higher burnout prevalence (47%), thereby contributing significantly to the observed variability. 35
To contextualize our findings on burnout among pediatric surgeons, it is important to compare them with burnout rates reported in broader physician populations, particularly among residents across various specialties. A previous meta-analysis, including 4,664 residents from both medical and surgical specialties, reported a pooled burnout prevalence of 35.7%. 20 Burnout rates varied by specialty, with higher prevalence observed in general surgery, anesthesiology, obstetrics/gynecology, and orthopedics (40.8%), moderate rates in internal medicine, pediatrics, and plastic surgery (30.0%), and lower rates in neurology and otolaryngology (15.4%). 20 These findings reinforce that burnout is a global issue affecting the medical profession as a whole. However, the magnitude and nature of stressors contributing to burnout differ across specialties, shaped by the clinical environment, emotional demands, and training structure.
Across the studies included, a range of personal, work-related, and organizational factors consistently emerged as contributors to burnout among pediatric surgical subspecialists. Many studies pointed to long working hours, and struggles with work-life balance as common stressors.29,32,43 Emotional challenges—like stress related to coworkers, dealing with difficult cases, and lacking emotional support—were emphasized in other reports.28,33 Other studies also noted that female physicians appeared more at risk,28,32 potentially due to added pressures related to gender-based role expectations, greater household responsibilities, and lack of support in male-dominated surgical environments. Younger surgeons and those early in their careers, like interns and junior fellows, were found to be especially vulnerable.27,29,31 Institutional issues—such as a lack of mentorship, frustrations with electronic medical records, and an unsupportive work environment—were also frequently mentioned. 34 A lack of administrative and organizational leadership support was commonly cited, particularly by junior staff who may feel underrepresented in decision-making and undervalued by senior leadership. 31 In contrast, a few protective factors came up, including having a non-physician spouse, holding multiple advanced degrees, and working in private practice, as reported by Liaqat et al. 30
Although highly prevalent, burnout among pediatric surgeons is an addressable condition that can be reduced through targeted interventions. Multiple strategies—spanning personal habits, and institutional policy—can help prevent and mitigate it. 47 At the individual level, promoting healthy work-life balance, and maintaining regular sleep hygiene have been shown to reduce burnout risk.5,48,49 Within the professional environment, collegial support, and a collaborative and respectful workplace culture have been identified as protective factors against burnout. 50 Additionally, structured coaching and professional development programs have demonstrated benefits in improving well-being, professional fulfillment, and reducing burnout among surgical trainees and residents.51,52 Given the burden of burnout and its consequences for both surgeons and patients, institutions must take the lead in building robust support system. 53 Institutional support should include fair compensation, protected time for academic development, and responsiveness to staff feedback. In addition, structural interventions aimed at optimizing workload distribution and ensuring adequate staffing levels are critical to sustaining workforce well-being and reducing burnout risk.54,55 Prospective research should focus on intervention studies specific to pediatric surgeons, especially in under-resourced settings wherein systemic challenges might exaggerate stress. Qualitative studies exploring surgeons’ lived experiences may also uncover nuanced stressors and protective factors not captured in survey data.
This systematic review focused specifically on burnout in pediatric surgeons, a group uniquely burdened by both technical challenges and emotional stressors. Our analysis brings together global data and reveals wide variation in burnout prevalence, likely influenced by differences in measurement tools and subspecialties. Still, several limitations should be noted. First, the number of eligible studies was small, and some of the included studies were not specific to pediatric surgeons, which limits the generalizability of the findings. Second, definitions and assessment methods for burnout varied widely across studies. Third, the analyses demonstrated substantial statistical heterogeneity across studies, which may reflect differences in study populations, geographic settings, burnout assessment tools, and healthcare systems, and therefore the pooled estimates should be interpreted with caution. Fourth, A potential limitation is that different burnout assessment instruments were used across studies, which vary in their conceptual frameworks and dimensions; however, as outcomes were reported dichotomously (presence vs. absence of burnout), we were unable to account for these differences using standard methods for continuous measures. Fifth, large regions with significant surgical populations, such as Latin America, India, Russia, and many countries across Africa and the Middle East, remain underrepresented or entirely unstudied. This geographic gap restricts the comprehensiveness of global estimates and highlights the need for region-specific research. Furthermore, differences in surgical training systems, including whether pediatric surgeons train locally or abroad, may influence mental health outcomes. Relocating for training, adjusting to unfamiliar healthcare systems, and lack of support networks may contribute to increased burnout risk, an area that remains insufficiently explored.
5. Conclusion
Burnout is a common issue among pediatric surgeons worldwide, with approximately one in three surgeons experiencing symptoms. The substantial variability in prevalence across studies highlights the influence of assessment tools, subspecialty differences, and contextual factors such as healthcare systems and working environments. Addressing burnout requires coordinated efforts at both individual and institutional levels, including supportive workplace cultures, workload optimization, and access to professional development and well-being programs. Future research should focus on region-specific studies and intervention strategies to better understand and mitigate burnout among pediatric surgeons globally.
Authors’ contributions: Amani N. Alansari: Project administration, conceptualization, methodology, analysis. writing original draft. Imen Tabia: Methodology, data collection, data extraction, quality assessment. Marwa Messaoud: Data collection, data extraction, analysis. Hanan Youssif: Conceptualization, quality assessment, writing original draft. All authors reviewed the manuscript and agreed with its submission.
Supplemental Material
Supplemental Material - Burnout Among Pediatric Surgeons of Different Subspecialties Worldwide: A Systematic Review and Meta-Analysis
Supplemental Material for Burnout Among Pediatric Surgeons of Different Subspecialties Worldwide: A Systematic Review and Meta-Analysis by Amani N. Alansari, Imen Tabia, Marwa Messaoud, Hanan Youssif in Health Services Insights
Footnotes
Acknowledgments
This research recevied fund by Hamad Medical Corporation’s Medical Research Center (MRC).
Funding
This research received fund by Hamad Medical Corporation’s Medical Research Center (MRC).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings are available upon request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.