
Abstract
Background
Self-perceived health status is an important outcome for older adults recovering from acute illness, yet little is known about what predicts this outcome at discharge in Norwegian admission avoidance service. This study aimed to assess the change in self-perceived health of patients between admission and discharge in municipal in-patient acute care units (MIPACs) – a type of admission avoidance service in Norway – and to explore the association of individual and MIPAC institutional level factors on perceived health.
Methods
Cross-sectional design with retrospective pre-test design was employed. Staff at eight MIPAC units collected data from patients who were willing and cognitively able to participate. Self-perceived health was measured with two outcome variables, the EQ-5D-5L index and the EQ-VAS, at admission and discharge, using a pre-post-test design. Missing data was handled using multiple imputation. Linear regression models were estimated in Stata.
Results
Among the 89 included patients, the mean age was 77 (median = 81, Q1–Q3 = 70–87, minimum–maximum 35–98), and 66% were women. All patients showed significant improvement in self-perceived health from admission to discharge. The mean increase of EQ-5D-5L index was 0.27 points (95% CI = 0.21–0.33), and the mean increase of the EQ-VAS score was 15 points (95% CI = 9.70–19.90). Other individual or institutional characteristics, including age, comorbidity, length of stay, and bed count, were not statistically significantly associated with changes in EQ-5D-5L and EQ-VAS scores.
Conclusions
The study found that patients receiving care in MIPACs showed significant improvements in self-perceived health between admission and discharge. Some individual-level predictors were identified, but institutional factors appeared unrelated to the change. These findings highlight that individual characteristics influenced patient’s perceived health more than the institutional differences between the units. Future studies should incorporate larger samples and explore additional factors, such as interpersonal or community, to show a more comprehensive understanding of how the care environment shapes self-perceived health.
Keywords
Introduction
Self-perceived health status is a widely used and important outcome measure for assessing overall health and evaluating the impact of treatments, interventions, and health policies. 1 It is a multidimensional construct which reflects physical, emotional, mental, social, and behavioural aspects of well-being and functioning. 2 It represents an evaluation made by the individual about their own health, rather than an assessment by clinicians or objective measures. Self-perceived health provides insight into subjective experiences that often predict health outcomes, utilization of healthcare services, and adherence to treatment,3,4 making it an important area of study. Furthermore, it provides insight into patients’ perceived needs, which can support healthcare services delivering patient-centred care, inform policies, and assess the quality of providers. 5
This study focuses on self-perceived health status in the Municipal Inpatient Acute Care (MIPAC) setting using an ecological model as a conceptual framework. MIPAC units are admission avoidance care institutions in Norway, established to reduce unnecessary hospital admissions and overutilization of specialist care by shifting healthcare to the primary healthcare level and closer to the patients’ homes. 6 Countries such as Denmark and the United Kingdom have implemented models like acute care teams 7 or admission avoidance hospitals at home, 8 while MIPAC units represent a distinct Norwegian approach. Across countries, there is a shared goal of delivering care in less resource-intensive settings to help reduce dependence on specialist health services and contribute to a more sustainable and patient-centred healthcare system. Studying self-perceived health status admission avoidance services is particularly important given the relatively recent implementation of some models (e.g., the Norwegian MIPAC and Danish acute care team), limited research base, and growing role in healthcare policy.
This study adopts an ecological model to examine self-perceived health status. At its core, an ecological model posits that individual outcomes are shaped by multiple, interacting levels of influence, including individual, inter-personal, institutional, community, physical environment, and policy level.9,10 In this study, we explore how individual- and institutional-level factors are associated with self-perceived health status. The care trajectory of an elderly individual framed by an ecological model can illustrate how different levels of influence shape their well-being. At the individual level, they may be frail with mobility limitations. Support from their family and social network – the interpersonal level – may be essential to manage daily activities. In case of medical issues, the way care is structured and delivered within services such as MIPAC – the institutional level – is essential, including communication and coordination practices, staffing level, admission and discharge routines, and follow-up procedures. At the community level, transportation and recreational activities can further enhance their quality of life. Simultaneously, policy-level factors like health and social policies and regulations are necessary to ensure sufficient funding and support for the institutional- and community-level services.
Previous research on self-perceived health status in the MIPAC setting is limited, while studies in the general population show mixed results on which factors influence self-perceived health, including factors such as age, gender, education and geography.11-18 Nonetheless, across studies, there appears to be a consistent pattern suggesting that perceived health is influenced by a combination of individual, social, and structural factors.11-18
In this study, we use the term ‘self-perceived health’ rather than the broader concept of health-related quality of life (HRQoL). Our data collection tool, the EQ-5D-5L is often used as a proxy for HRQoL; however, it has been argued to primarily reflect current health status and functioning, rather than broader aspects of quality of life. 19 To contextualize the findings in our study, we still refer to previous research that has examined HRQoL.
Previous research comparing patients in MIPAC units and hospitals found a greater improvement in HRQoL among those treated in MIPAC units. 11 Another study on MIPAC patients found no significant association between patient experience and HRQoL 12 Furthermore, studies report no significant associations between HRQoL and socio-demographic characteristics such as age, gender, and marital status,1,13-18 while others found that older age, female gender, limitations in instrumental activities of daily living (IADL), urban residence, longer lengths of stay, and higher levels of education were associated with poorer HRQoL.14-18
There is limited research on the relationship between patients’ self-perceived health and characteristics of healthcare institutions that treat them, such as the institution’s location, size or availability of diagnostic procedures. One multilevel study that assessed institutional-level variation found that although the hospital characteristics were associated with self-perceived health, differences between hospitals were small compared to individual-level variation. 13 While no specific hospital-level characteristics were found to significantly influence patients’ self-reported health, the observed variation in outcomes was attributable to individual-level factors rather than treatment-site differences. 13 To address the gap in understanding how institutional-level factors are associated with self-perceived health status, this study seeks to generate empirical insights relevant to MIPACs and key stakeholders, including municipalities, to support evaluation of unit performance and inform organizational planning.
Moreover, understanding changes in patients’ self-perceived health during their stay in MIPAC is critical for evaluating care effectiveness. 20 Yet, systematic assessments in these units remain scarce, limiting the ability to appraise care from the patient perspective and constraining stakeholders’ insight into recovery experiences. To address this, the present study uses the EQ-5D-5L to examine patients’ self-perceived health during their stay. The study aims to inform national, regional, and local policy development so that future strategies better align with patient needs and contribute to high-quality, patient-centred services, independent of any changes in national policy. 21 This study has the following objectives: 1) to estimate the mean change in self-perceived health status scores from admission to discharge, and 2) to examine the association between patient-level and MIPAC institutional-level predictors and self-perceived health status at discharge.
Material and Methods
We adopted a within-patient cross-sectional design using retrospective pre-post self-assessment to determine the relationship between self-perceived health among MIPAC patients and multilevel factors. This approach aligns with the research questions and was feasible given the short length of stay and potential vulnerability of the population. We follow the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for cross-sectional studies when reporting this study.
Study Setting
Norway’s tax-funded healthcare system provides universal coverage through a semi-decentralized model. 22 The central government manages specialist care through regional health authorities, while the 357 municipalities are responsible for primary, preventive, and long-term care. 23 The healthcare system aspires to provide care at the lowest effective level and, whenever safe and appropriate, in patients’ homes and communities.24,25 MIPAC services were established to bridge the gap between specialist and municipal care.
MIPAC Organization, Legal Framework and Profile
MIPAC units deliver acute inpatient care in the municipal care setting, vary in organization and care delivery. MIPAC services typically consist of designated beds located within existing institutions, such as nursing homes, urgent care, or medical centres, though some operate as stand-alone units. Every municipality is required by law to provide MIPAC services. In 2022, a third of the total 226 units were established and run as intermunicipal collaborations 26 where smaller municipalities bought dedicated MIPAC bed(s) from a larger host municipality.
General practitioners or an attending physician at urgent care refers patients to MIPACs. Admission criteria include adults (over 18 years old) with an acute exacerbation of a known and/or diagnosed medical condition, or with a low risk of severe deterioration. The latest published data from 2022 showed that 60% of patients in MIPAC were women, and 72% of patients were aged 67 years or older, 27 with musculoskeletal, respiratory, and general or unspecified issues accounting for about 55% of admissions. 27
Study Recruitment and Participants
We conducted the study in eight MIPAC units from October 2024 to April 2025. The municipalities were selected through a random sampling process using an online random number generator. 28 Random numbers between 0 and 1 were generated and assigned to the corresponding municipalities with MIPACs that had reported unit information to the Directorate of Health (DOH). 29 The list was then sorted in ascending order, and the first 60 municipalities out of 215 municipalities which had reported to DOH were selected for inclusion in the study to obtain a sample that was both random and represented variation in the units. Of the 60 units, 8 agreed to participate, 16 declined, and the remaining did not reply. As a result, the sample did not fully capture the intended variation.
This study was exploratory and recruitment was conducted with the aim of collecting data from as many eligible patients as possible across the units, limiting the final sample to 89 patients. The expected number of eligible patients admitted to participating units was informed by the data on the organization of MIPACs provided by the DOH in the previous years. 29
MIPAC staff, mostly registered nurses, recruited patients who met the following inclusion criteria: sufficient cognitive ability to understand the study information and provide informed consent, and sufficient Norwegian language skills to do so. The exclusion criteria were cognitive impairment that prevented understanding of the study, insufficient Norwegian language skills to understand the questionnaire or consent process, or clinically unstable patients at the time of recruitment.
Data Sources
Overview of Study Variables
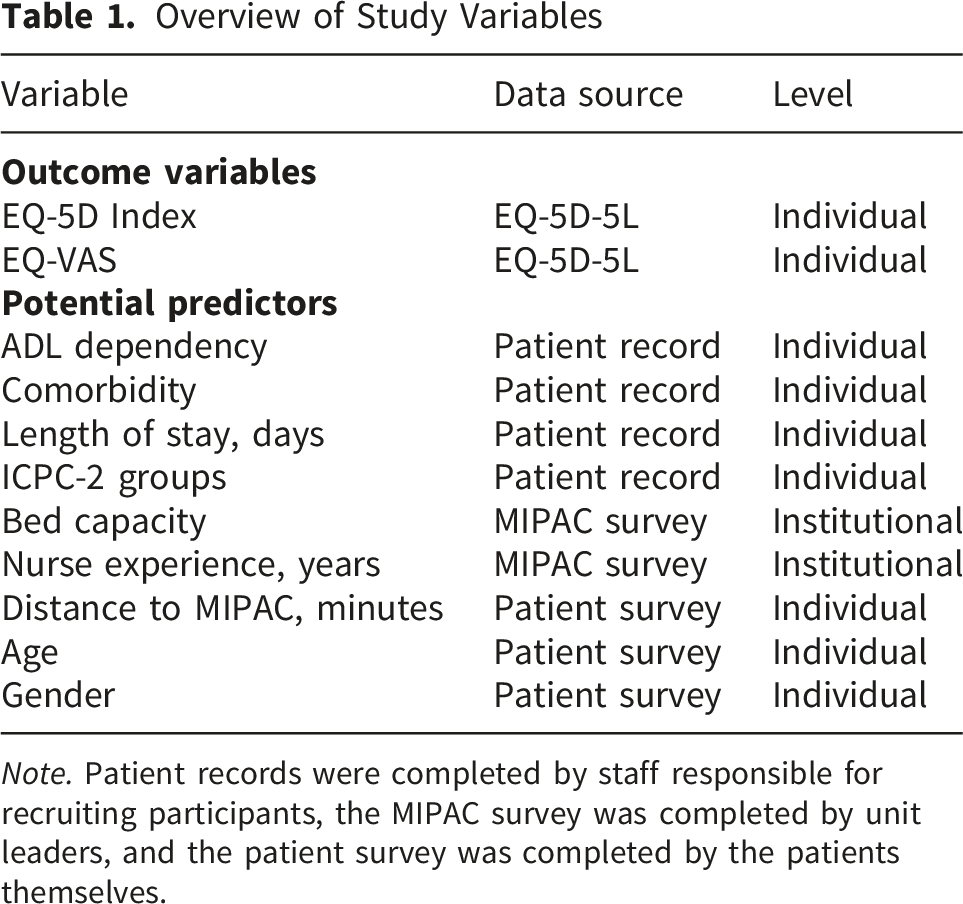
Note. Patient records were completed by staff responsible for recruiting participants, the MIPAC survey was completed by unit leaders, and the patient survey was completed by the patients themselves.
The outcome variable, self-perceived health status, was collected with the EQ-5D-5L, yielding two scores – an index score and a VAS score. The EQ-5D-5L comprises five dimensions – mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, each scored on a five-level scale (1 = no to problems to 5 = extreme problems/unable to perform the activity). 30 The EQ-VAS consists of a straight line with two endpoints, labelled 0 and 100, representing the extremes of the patient’s health status (i.e.,the worst imaginable health and the best imaginable health. Respondents mark a point on the line that best reflects how they feel, and the score (0-100) is based on where the mark is placed along the scale. The EQ-VAS is a complementary self-reported measure where respondents rate their own health, and it shows an independent perception of an individual’s health. 31
The research team created three data collection tools to obtain information about our predictors: (1) a patient survey, including the EQ-5D-5L, which was self-administered by patients, (2) a patient record form, completed by clinic staff based on patients’ medical records), and (3) a MIPAC survey, completed by the MIPAC leader (see Supplement 1).
The patient survey included questions about patient sociodemographic variables, such as whether they live alone, their education, whether they received help from family members when needed, and more.
The patient record collected clinical information about the patient from their electronic medical records, including age, gender, dependency in Activities of Daily Living (ADL) (basic everyday tasks), reason for MIPAC admission, referring doctor, and discharge location. This patient record tool also included the Charlson Comorbidity Index (CCI) 32 to get the patients’ comorbidity score ranging from 0 to 37, with higher scores indicating greater comorbidity burden. In the analysis, CCI was grouped as 0 and ≥1, where 0 indicated no comorbidities and ≥1 indicated presence of at least one comorbidity. 33 Diagnosis information was obtained from the patient record. The diagnoses were then categorized according to the International Classification of Primary Care (ICPC-2) 34 which categorizes health problems and diagnoses into chapters based on body systems (e.g., cardiovascular, respiratory, psychological), and includes symptom codes, diagnostic codes, and process codes. 33
The MIPAC survey collected information about characteristics of the MIPAC unit, such as number of beds, whether the MIPAC is in a nursing home or urgent care, number of staff, and proportion of nurses with higher education.
Pilot Testing
We piloted the EQ-5D-5L and the self-developed tools from May to July 2024 to check the feasibility of the data collection process and the relevance and clarity of our data collection tools. The pilot was carried out in two MIPAC units with a total of nine patients filling in the forms and two registered nurses giving feedback on the data collection process. We conducted the pilot with our initial data collection plan, which was to get the patients to fill in the questionnaire about self-perceived health status at two different time points – one shortly after they had been admitted, and one during their discharge. The pilot demonstrated that it was tiresome for the patients to complete the questionnaire on two separate occasions.
Consequently, for the final data collection, we collected data at a single time point – during discharge – where the patient filled out the EQ-5D-5L twice. This design enabled comparison of self-reported health at two time points, admission and discharge, based on data collected at a single time point. Although retrospective self-assessment may introduce bias, it was the most feasible approach given the short length of stay and the vulnerability of the patient population.
Items included in the self-developed tools were reviewed and adjusted after discussing them in a pre-pilot phase and testing them in a pilot study. A few revisions were made after the pilot to improve clarity, relevance and privacy. For example, we used the patients’ travel time to MIPAC rather than address data as an indicator of geographic accessibility. Furthermore, questions about doctors’ and nurses’ availability, e.g., number of hours per day a physician was physically present on site, were excluded because they exceeded the level of detail necessary for the study aims.
We are excluding the pilot data from the analyses due to significant changes in the data collection process.
Data Collection
Recruitment staff approached patients once their clinical condition had improved sufficiently to allow participation without undue burden. Patients received both written and oral information about the study and provided written informed consent.
At discharge, the participating patients completed a set of questionnaires themselves, including the EQ-5D-5L and the patient survey. In cases where patients were unable to complete the questionnaire independently, MIPAC staff helped by reading the questions aloud and recording the patient’s responses.
The MIPAC unit staff extracted data from the electronic patient records using the second tool – the patient record. The unit leader completed the third tool about MIPAC administration once per unit.
Statistical Analyses
We used descriptive statistics to describe the characteristics of patients and units. The distribution of outcome variables was assessed using histograms. The differences in EQ-VAS scores and EQ-5D-5L index scores between groups were tested using the Mann–Whitney test for variables gender, comorbidity score, problems with ADL, and living alone, while the Kruskal–Wallis test was used for variables age, education, length of stay, and patients’ travel time to MIPAC. We calculated the means of EQ-5D-5L index, EQ-VAS, and EQ-5D-5L domains at admission and discharge. To assess the statistical significance of changes in means, paired t-tests were used. Wilcoxon signed-rank tests were also conducted given the ordinal nature of the response scale and to check for robustness.
Missing data on our outcome variable – self-perceived health status measured with the EQ-5D-5L, were handled using multiple imputation (MI) using chained equations, which add missing values in multiple variables repeatedly. 35 Missingness was partial rather than complete at the domain level. Some patients had responses on three or four of the five EQ-5D-5L domains but were missing one or two. MI was therefore applied at the domain level instead of imputing index score directly. The EQ-5D-5L index was treated as a passive variable, calculated directly from other domain scores after each imputation step rather than imputed as an outcome.35,36Seventy-four participants had complete data for the outcome variable, and data was missing primarily due to the older and frail participants being unable to complete the whole questionnaire. We used the default setting of the imputation procedure, which selects appropriate logistic models for binary and categorical variables and predictive mean matching for continuous variables. 36 We selected variables based on theoretical relevance and literature, including sociodemographic (age, gender), clinical (baseline EQ-5D score, comorbidity, ADL dependency, length of stay, respiratory problems, general and unspecified problems), and MIPAC level characteristics (patients’ travel time to MIPAC, number of beds, and nurse experience in years).
We used multiple linear regression to explore whether the factors were associated with patients’ self-perceived health at discharge, measured by EQ-5D-5L and EQ-VAS. First, we fitted a null model, which included the random intercept for MIPAC level, to decide the necessity of multilevel modelling. We used the random intercept multilevel model to calculate the intraclass correlation coefficients (ICCs), which is an index showing variation in self-perceived health due to differences between MIPAC units.
37
The between-unit variance 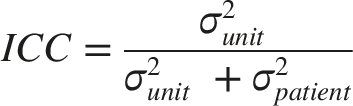
Result
Overview of all the Eight Participating MIPAC Units
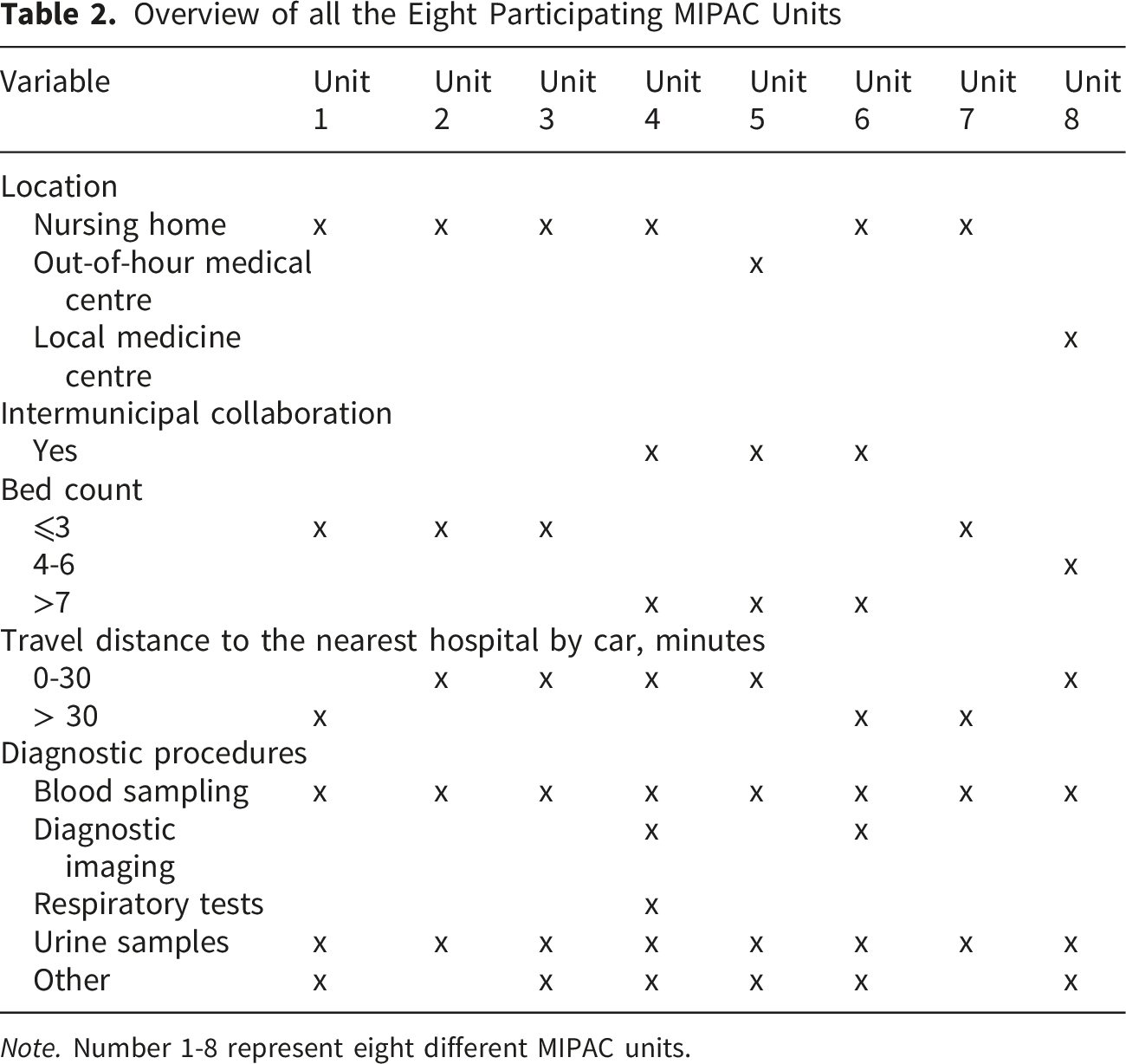
Note. Number 1-8 represent eight different MIPAC units.
Demographic Characteristics of Patients (N = 89)
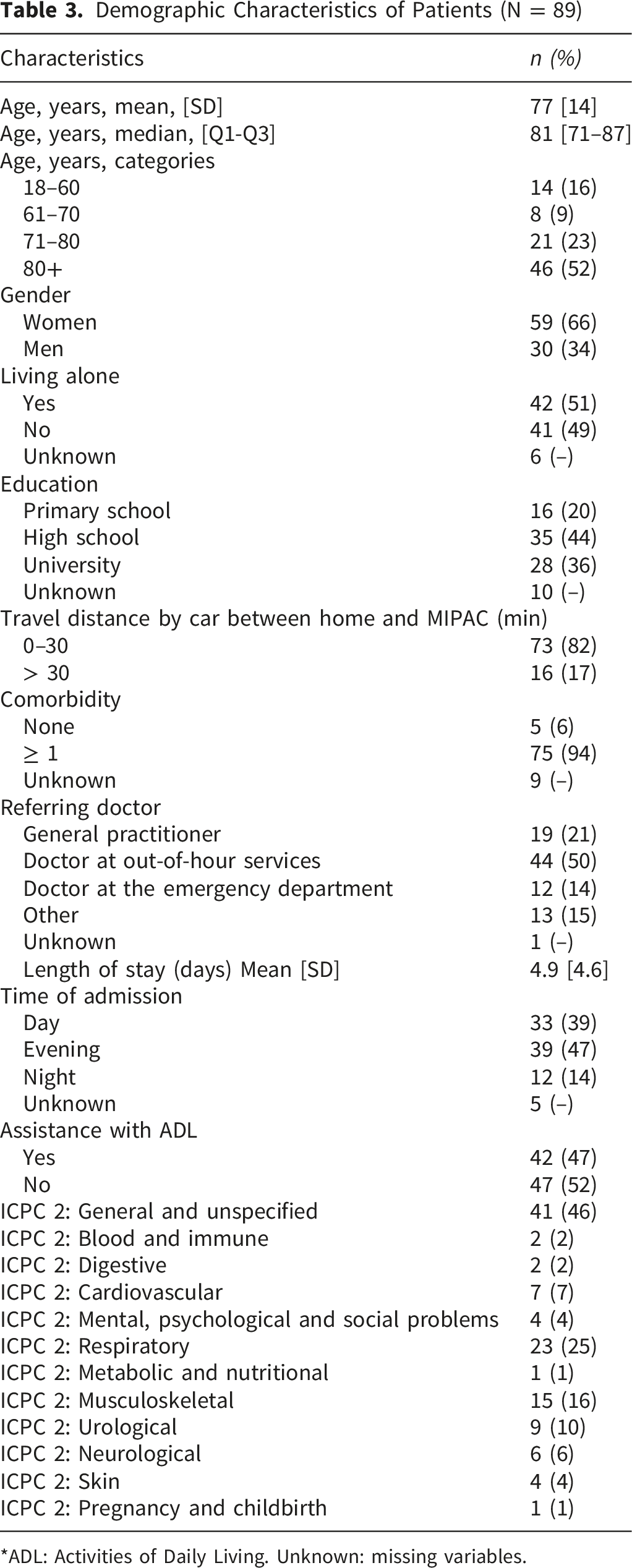
*ADL: Activities of Daily Living. Unknown: missing variables.
Means of EQ-5d Index, EQ-VAS, and EQ-5d Domains at Admission and Discharge
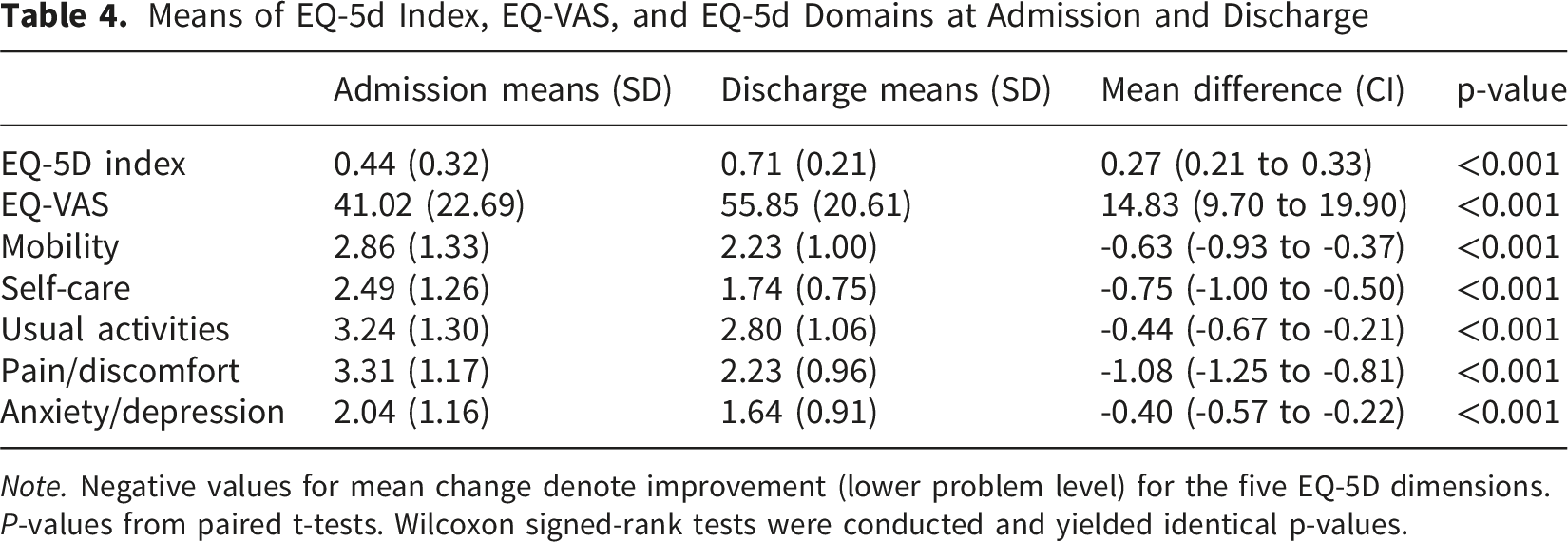
Note. Negative values for mean change denote improvement (lower problem level) for the five EQ-5D dimensions.
P-values from paired t-tests. Wilcoxon signed-rank tests were conducted and yielded identical p-values.
EQ-5D-5L Index Scores and EQ-VAS Scores by Different Patient Characteristics
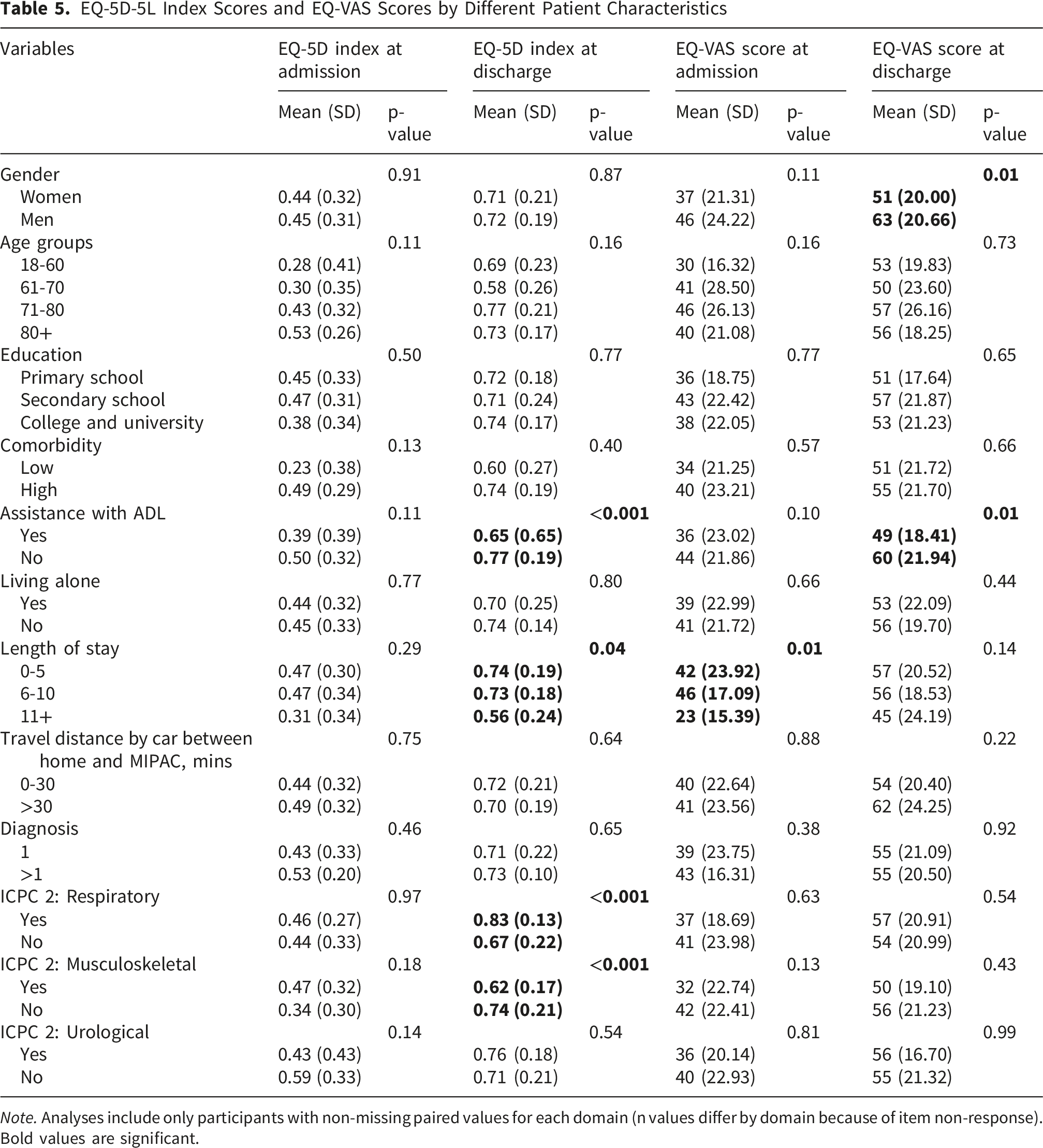
Note. Analyses include only participants with non-missing paired values for each domain (n values differ by domain because of item non-response). Bold values are significant.
Table 5 also presents EQ-VAS scores across patient characteristics, demonstrating overall improvement in self-perceived health. Men reported better self-perceived health than women both at admission (46 vs. 37) and discharge (63 vs. 51), showing a consistent difference. Similarly, participants who were independent in ADL rated their health more positively than those who required assistance at both admission (44 vs. 36) and discharge (60 vs 49). No significant differences in EQ-VAS scores were observed for other patient characteristics.
We calculated the intraclass correlation coefficients (ICC) to assess variance attributable to the differences between MIPAC units. Clustering by MIPACs was negligible (ICC ≈ 0.00, 95% CI ≈ 0.00–0.00) and the likelihood ratio test showed no improvement of the multilevel model over a single-level model (LR χ2(1) = 0.00, p= 1.00). 39 We found that the MIPAC-level variance was not statistically different from zero, and ICC was very small suggesting minimal clustering due to MIPACs. Thus, multilevel modelling was not used.
Multiple Regression Models of EQ-5D-5L Index Scores and EQ-VAS Scores at Discharge
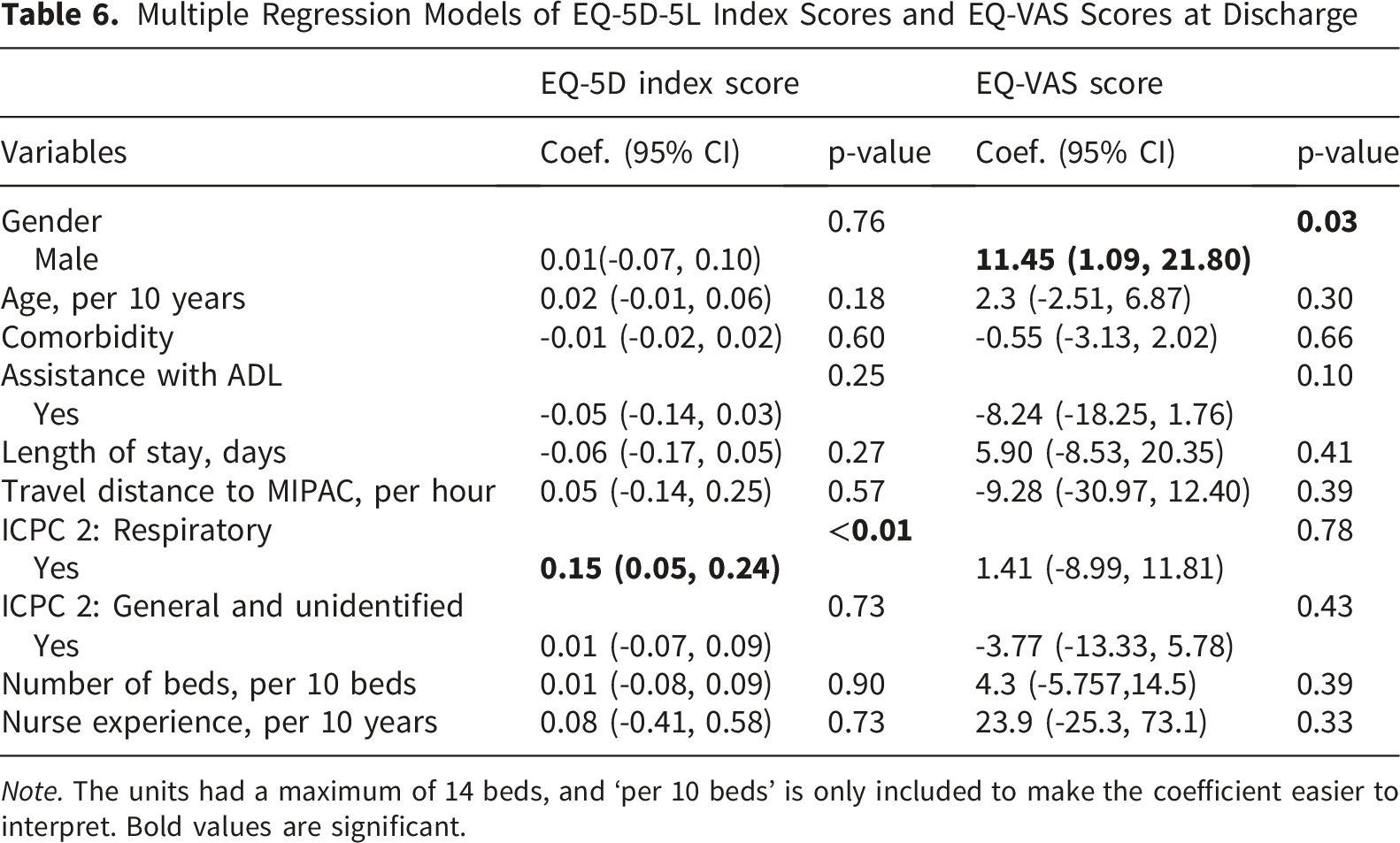
Note. The units had a maximum of 14 beds, and ‘per 10 beds’ is only included to make the coefficient easier to interpret. Bold values are significant.
Discussion
The purpose of this study was to assess changes in self-perceived health between admission and discharge in MIPAC units and to examine the association between self-perceived health status and patient-level and MIPAC unit-level predictors at discharge. Both measures of self-perceived health, the EQ-5D-5L index and the EQ-VAS, showed significant perceived improvement at discharge, indicating that patients experienced better perceived health after their MIPAC stay. Improvements were reported across all EQ-5D-5L domains, with the largest gains in pain/discomfort and the smallest in anxiety/depression. However, these findings should be interpreted cautiously because the retrospective pre-post-test design is prone to bias. Our findings indicate that higher dependency in ADL and longer stays in MIPAC were associated with lower EQ-5D index scores at discharge. Gender and having a respiratory condition were the only significant predictors of EQ-VAS, with men and patients with respiratory diagnoses reporting higher perceived health at discharge. No other patient-level or MIPAC-level factors were significantly associated with self-perceived health. Across all analyses, while patients reported improvement during their stay, two individual factors were associated with perceived health, and institutional-level factors were not associated with it, owing to the small number of units included. Most of the improvements could not be attributed to factors in our analysis, suggesting a need for research on both similar and other factors, like patient experience or care processes.
The increase of 0.27 in the EQ-5D-5L index and 15 in the EQ-VAS score represents a meaningful improvement in self-perceived health. Changes of 0.03–0.52 in the EQ-5D index and about 7 points in EQ-VAS are considered clinically meaningful, reflecting noticeable improvements in perceived health.40,41 Together, these findings suggest that the recovery experienced by patients was not only statistically significant but also meaningful in everyday terms, reflecting less severe symptoms and everyday functioning.
Descriptively, the mean EQ-5D-5L index score at discharge was higher in our study than reported in the Norwegian MIPAC study from 2024 (0.71 at discharge vs. 0.50, respectively). 11 The difference in mean may be due to the 2024 study using the UK value set to calculate the EQ-5D-5L index score, as the Norwegian value set was not yet developed. It could also reflect the timing involved in administering the survey, as the authors of the 2024 study received their follow-up survey after 4–6 weeks. Additionally, the 2024 study was more constrained geographically as it included five MIPACs in the southeastern region. The EQ-5D index score in our sample (0.71) was consistent with the Norwegian population norm for people aged 80 years and older (0.71), 18 consistent with the age distribution of our sample, where 51% of our patients were over 80 years of age. Although the mean EQ-5D-5L score at discharge (0.71) was lower than the general population mean (0.80), 18 the findings suggest that patients in MIPAC may reach a level of self-perceived health comparable to their age-matched peers in the general population.
In our study of MIPAC patients, the mean EQ-VAS score at discharge was 55 compared to the mean of 62 in an elderly cohort in six European countries. 42 That study included individuals aged 75 and older from the general population, interviewed at their homes. Compared to these older adults, MIPAC patients reported poorer self-perceived health likely reflecting their greater frailty and clinically burdened during recovery from acute illness. Despite improvement being observed during the MIPAC stay, their perceived health remained below that of older adults living independently. Similarly, when comparing the general Norwegian population (EQ-VAS 78) and people aged 80 or more (EQ-VAS 68), the patients in our sample reported substantially poorer self-perceived health status (EQ-VAS 55). This highlights the need for continued follow-up after discharge, as older and frail patients often require extended recovery periods.43,44 Nonetheless, the observed improvement from admission to discharge suggests that acute care in MIPACs contributes positively to health restoration.
Our study found no significant associations between EQ-5D-5L scores and sociodemographic variables such as gender, age, education level, or whether the patient lived alone. Likewise, no associations were observed with institutional factors of the units, including bed capacity and the experience of nurses in years. These findings are consistent with studies with short-stay inpatient settings, which found non-significant differences in health improvement measured by EQ-5D-5L across age groups.45,46 However, our findings differed from population-based studies showing associations with EQ-5D-5L scores and social and individual determinants.14,17,18 The lack of such gradients in our sample may reflect the acute nature of the MIPAC population, where patients’ immediate health needs may be more influential than demographic or institutional factors. Prior research15,18 indicate that functional ability influences EQ-5D index among older adults with comorbidities; however, this association was not detected in our study. In contrast, women reported lower EQ-VAS scores than men, consistent with studies showing gender differences in self-perceived health.45,46 This can be credited to gendered morbidity patterns, where women encounter a higher number of chronic conditions, disability and pain, which are linked to self-perceived health. 15 The absence of gender differences in EQ-5D-5L index score in our study, supports that EQ-VAS and EQ-5D-5L capture distinct constructs, with differing sensitivity to sociodemographic variables. 47
The ecological model helps interpret our findings by emphasizing the potential significance of interactions across individual, inter-personal, institutional, community, physical environment, and policy factors.10,48 Although our analysis did not identify associations between self-perceived health and the organizational-level variables included, this absence of evidence does not imply that such factors are unimportant. It may instead reflect the small number of units in the study and the limited scope of variables examined, which did not capture relational dynamics, community context, or broader environmental and cultural influences. In MIPACs, patients’ well-being may be shaped not only by clinical interventions, but also by features of the care environment, such as social interactions, perceived support, and everyday routines. This aligns with the concept of activity settings, which suggests that health is not solely produced within the individual, but co-produced through interactions with the surrounding context, including cultural norms, social relationships, organizational practices, and policy frameworks. 48 Broader contextual conditions, such as environmental features, social networks, and cultural norms, may exert greater influence on self-perceived health than stable individual characteristics. 48 The lack of observed associations at the institutional level may therefore point to the relevance of more dynamic and context-sensitive factors that were not captured by our current set of predictors.
Implications
A notable practical challenge concerning the participants when assessing self-perceived health in the MIPAC settings is that they are often acutely ill, frail, and elderly, and their stays are typically short. These factors limit both the feasibility and suitability of self-reporting, particularly at admission when patients may be too unwell to participate in assessments. While discharge is a more feasible time point to collect perceived health data, questions remain about how such information can be meaningfully applied in practice.
It may be necessary to integrate evaluations of self-perceived health into structured discharge routines to enhance the utility of such health assessments in MIPAC. For example, responses could inform a brief discharge summary, providing insights into patients perceived needs, functioning, and recovery trajectory. This could ensure the patient receives a better follow-up support. However, for such data to contribute effectively to quality improvement, further work is needed to clarify how these measures can be interpreted in context, how they relate to other clinical indicators, and how staff can be supported in using them as part of reflective practice and service development.
Furthermore, this study found no clear association between patients’ self-perceived health at discharge and the characteristics of MIPAC units, such as unit size or co-location with other services. Given the small sample size of the units, larger studies are needed to assess whether institutional factors influence patient outcomes and the extent of the influence.
However, it is important to note that the study did not include institutional-level process characteristics, such as clinical routines or care practices. Future research should therefore explore whether such process-related factors are associated with patients’ self-perceived status. If meaningful associations are identified, this could inform the development of shared standards or promising practices across MIPAC units. Such standards could help ensure consistent care quality while still allowing for local adaptation and responsiveness to community needs.
Future research on self-perceived health in MIPAC should expand upon the findings by exploring additional levels of influence and methodological approaches. Beyond individual and institutional levels, studies could explore interpersonal factors, such as communication, teamwork, staff and patient relationships, and community-level factors, such as access to other municipal health resources. Mixed-method or qualitative designs could capture the subjective and contextual dimensions of perceived health. Larger longitudinal studies are needed to explore whether the short-term improvements during the MIPAC stay are maintained after discharge and translate into longer-term well-being, and reduced readmissions.
Strengths and Limitations
By collecting data directly from routine MIPAC practice, this study reflects real-world conditions, which strengthens the ecological validity of the findings. The participating MIPAC units varied in size, location, and institutional setup, and included both municipal and intermunicipal services, which supports the generalizability of the findings to other MIPAC services in municipalities across the country.
A major limitation is that we used a retrospective pre–post-test design, asking participants to remember how they felt before admission. Baseline score relied on memory, which is prone to recall bias, including under- or overestimation of baseline health along with memory errors.49,50 In addition, participants likely judge their baseline health in reference to their current health, making the two ratings not fully comparable. This introduces recalibration bias as the two scores are no longer measured on the same metric, making it difficult to capture true change in score. 49 Prior studies show that the level of perceived improvement can be overstated, particularly on items where a more positive answer can be socially desirable, such as items suggesting independence or more recovery. 49 Studies also indicate that adding retrospective pre-test questions changes participant responses to post-test questions, introducing more bias. In a randomized trial, individuals completing pre-test questions had significantly higher post-test score compared to those who completed only post-test questions. 51 Thus, the findings on health improvement from baseline to discharge should be treated as exploratory. At the same time, this approach minimized continued response burden for acutely ill patients and made data collection feasible in an acute care setting. 52 Despite the limitations above, the changes should reflect the patient’s subjective evaluation of change from admission to discharge.
Other limitations of the study include a small sample size, affecting the ability to detect the subtle effects of individual or institutional factors. The unit-level response rate was 13.3%, creating a risk of institutional selection bias. Participating units may differ from non-participating units in staffing, resources, or care quality, which limits the generalizability of institutional-level findings. Furthermore, the eight units that agreed to participate could have better staffing, resources, or patient outcomes than those that declined participation, introducing institutional selection bias. 53 The absence of a sample size calculation is a limitation as recruitment of eligible patients was dependent on the flow across a small number of participating units. Our findings should be interpreted as exploratory and need to be confirmed by larger studies. Despite the limitations, assessing changes in self-perceived health over a short period, from admission to discharge, provided valuable insight into perceived health improvement within MIPAC. 52
Conclusion
This study examined changes in self-perceived health among patients receiving care in MIPACs using an ecological perspective. Patients perceived significant improvement in self-perceived health from admission to discharge, though this improvement was not clearly related to institutional-level variables, and individual-level variables explained little of the variation in improvement. The study highlights the need for future research to explore additional levels of the ecological model – such as interpersonal and community factors – to better understand how the MIPAC care environment contributes to patients’ perceived health.
Supplemental Material
Supplemental Material - Patient- and Institutional-Level Determinants of Self-Perceived Health at Municipal In-Patient Acute Care Units in Norway Tools used to collect data from the patients and staff
Supplemental Material for Patient and Institutional-Level Determinants of Self-Perceived Health at Municipal In-Patient Acute Care Units in Norway by Susan Sitoula, Karl Ove Hufthammer and Hanne Marie Rostad in Health Services Insights.
Footnotes
Acknowledgments
The authors thank the Norwegian University of Science and Technology (NTNU) for funding support. We also want to express our gratitude to the staff at the MIPAC units for their support and assistance which made data collection possible. Finally, we are grateful to Associate Professor Marianne Sundlisæter Skinner for her valuable contributions and help throughout.
Ethical Considerations
This study was conducted following the ethical principles of the World Medical Association Declaration of Helsinki. 54 The Regional Committees for Medical and Health Research Ethics (REC) in Norway (ref. No 701673) waived the need for ethical approval for this study, as it is not medical and health research, but health services research. The Norwegian Agency for Shared Services in Education and Research (SIKT) (ref. No 973026) assessed project’s privacy and concluded that it complied with applicable privacy laws and regulations.
Consent to Participate
Written consent was obtained from all the study participants.
Author contributions
Sitoula conceived and designed the study, collected and analysed the data, and drafted the manuscript. Hufthammer provided statistical expertise, contributed to data analysis and interpretation, and critically revised the manuscript. Rostad contributed to conceiving and designing the study, interpretating data, and critically revising the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted as part of Susan Sitoula’s PhD position funded by NTNU strategic recruitment funds.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study were collected directly from patients and are not available publicly. Participants did not provide consent to data sharing outside the research team.
Supplemental Material
Supplemental material for this article is available online.