
Abstract
Background
Early Essential Newborn Care (EENC) is an evidence-based strategy to reduce neonatal morbidity and mortality, yet implementation gaps persist in many low- and middle-income countries. In Vietnam, a multi-site quality improvement initiative, including clinical training, on-site coaching, supportive supervision, and facility-level quality improvement planning, was implemented to strengthen EENC practices across diverse hospital settings.
Methods
A repeated cross-sectional study was conducted in 14 hospitals across four provinces using data from three assessment rounds (December 2022, March 2024, and August 2024). Targeted EENC quality improvement activities were implemented between Rounds 1 and 2 and reinforced between Rounds 2 and 3. Medical record reviews, maternal interviews, and facility assessments were used to evaluate changes in EENC implementation. Indicators were selected based on WHO EENC standards, clinical and programmatic relevance, alignment with the intervention package, and availability across all three rounds. Proportions were compared using chi-square or Fisher’s exact tests, as appropriate.
Results
Improvements were observed in several technical practices. Immediate skin-to-skin contact increased from 32.5% in Round 1 to 73.8% in Round 3, and sustained skin-to-skin contact from 8.2% to 38.4% (p<0.001). Vitamin K1 administration rose from 93.0% to 99.3%, and non-application of antibiotic eye ointment from 88.8% to 98.8% (p<0.001). However, several indicators declined, including non-separation of mother and newborn (96.8% to 81.0%), early breastfeeding initiation (83.1% to 73.5%), no prelacteal feeding (28.0% to 19.1%), uterotonic use (99.3% to 94.6%), and uterine contraction monitoring (98.9% to 90.2%) (all p≤0.03). In Round 3, cesarean births showed persistent gaps compared with vaginal births.
Conclusion
The quality improvement initiative was associated with gains in selected technical EENC practices. However, declines in maternal monitoring and mother–infant support practices, and persistent gaps after cesarean birth, indicate that training and supervision alone are insufficient. Broader health-system strengthening is required to sustain full EENC implementation.
Keywords
Introduction
The immediate postnatal period is a critical window for ensuring the survival and well-being of both mothers and newborns. Globally, most neonatal deaths occur within the first few days of life, with preventable causes such as hypothermia, infection, and breathing difficulties being major contributors.1,2 To address these challenges, the World Health Organization (WHO) has endorsed Early Essential Newborn Care (EENC), a package of simple, low-cost, and evidence-based interventions proven to reduce neonatal mortality and morbidity. 3 The core components of EENC include immediate and thorough drying, sustained skin-to-skin contact, delayed umbilical cord clamping, and early initiation of breastfeeding. Strengthening EENC is central to achieving global commitments under the Sustainable Development Goals, particularly SDG 3.1 to reduce maternal mortality and SDG 3.2 to end preventable newborn deaths.
Despite the availability of clear WHO recommendations, translating EENC recommendations into routine clinical practice remains challenging, and implementation fidelity often varies across facilities.4,5 Evaluating the impact of quality improvement activities, therefore, requires systematic monitoring to understand whether clinical practices change as intended. Implementation fidelity, defined as the degree to which an intervention is delivered as designed, is crucial for interpreting program effectiveness and identifying persistent gaps that require further attention. 6
In response to this global agenda and the need to strengthen implementation fidelity, the Ministry of Health’s Maternal and Child Health Department, in collaboration with the WHO and with financial support from the Government of the Russian Federation, implemented a multi-year project to improve the quality of hospital-based maternal and newborn care in Vietnam. As part of this initiative, EENC was a core focus of targeted quality improvement activities implemented after the December 2022 assessment and reinforced after the March 2024 assessment. These activities included clinical training, on-site coaching, supportive supervision, and facility-level quality improvement planning. They were designed to increase the consistency and fidelity of EENC practices across diverse hospital settings and to support national progress toward SDG targets on maternal and newborn health.
This study uses repeated cross-sectional data collected at three time points within the project’s monitoring and evaluation framework to assess changes in EENC implementation following these targeted quality improvement activities. While the broader project addressed multiple components of maternal and child health, this paper focuses specifically on EENC. Understanding both the status and the trajectory of EENC practices after implementation is essential for identifying remaining gaps, recognizing areas of progress, and informing the next phase of quality improvement efforts.
Therefore, this study aims to (i) assess the fidelity of implementing core EENC practices against WHO-recommended standards and (ii) examine trends in EENC implementation across three assessment rounds to identify improvements and remaining gaps following the project’s quality improvement activities.
Methods
Study Design and Setting
This repeated cross-sectional study evaluated changes in Early Essential Newborn Care (EENC) implementation across three assessment rounds (in December 2022, March 2024, and August 2024) conducted as part of the quality improvement initiative Improving the Quality of Hospital Care to Reduce Maternal, Newborn, and Child Deaths. The initiative was implemented by the Ministry of Health’s Administration of Maternal and Child Health in collaboration with the World Health Organization (WHO) and funded by the Government of the Russian Federation. Assessment findings informed successive EENC quality improvement activities, including clinical training, on-site coaching, supportive supervision, and strengthening of documentation and clinical workflows.
Interventions were guided by WHO EENC recommendations, assessment findings, and facility-specific action plans developed to address identified gaps. Monitoring and supervision findings were used to refine implementation between assessment rounds.
The study was conducted in 14 purposively selected hospitals across four provinces (Thanh Hoa, Ha Giang, Dak Lak, and Soc Trang), including four provincial and ten district hospitals. These provinces were selected to represent diverse geographic and socioeconomic settings across Viet Nam, including mountainous, north-central, Central Highlands, and Mekong Delta regions.
Study Population and Sampling
Data sources included maternal and newborn medical records, postpartum interviews with mothers, and facility observations of essential medicines, supplies, and environmental hygiene. Medical records were selected through simple random sampling from eligible records within the six months preceding each assessment round. As this study was conducted within a program monitoring framework rather than a hypothesis-driven trial, no formal sample size calculation was performed. The monitoring protocol targeted approximately 50 records per round at provincial hospitals and 30 at district hospitals, with final sample sizes determined by delivery volume, record availability, documentation completeness, and data-collection capacity.
Eligible records included deliveries occurring within the six months before each assessment round and containing sufficient information to assess study indicators. Maternal and newborn records were sampled independently using separate sampling frames and therefore did not represent matched mother–newborn pairs.
Postpartum interviews were conducted with all eligible, consenting mothers present during the facility visit. Eligible participants were recently delivered mothers who were clinically stable and able to provide informed consent. Mothers who declined participation, were unavailable, or were unable to complete the interview were excluded. Interview participants were recruited independently of the sampled medical records.
Variables and Measurement
Key indicators were selected based on WHO-recommended Early Essential Newborn Care (EENC) standards, clinical relevance, alignment with the quality improvement package, and consistent availability across all three assessment rounds. Because EENC practices are recommended for all eligible mothers and newborns, universal or near-universal coverage was considered the expected programmatic benchmark; substantially lower coverage was interpreted as an implementation gap.
EENC implementation was assessed using dichotomous indicators reflecting the main components of the care sequence. Immediate and sustained skin-to-skin contact were defined as newborn placement on the mother’s bare chest or abdomen immediately after birth and uninterrupted contact for at least 60 minutes, respectively. Additional essential care indicators included documented respiratory monitoring among preterm or low-birth-weight newborns and non-separation/continuous rooming-in until discharge. Breastfeeding support indicators included breastfeeding within the first hour after birth and absence of prelacteal feeding. Maternal postpartum care indicators included prophylactic uterotonic administration immediately after delivery and documented monitoring for postpartum hemorrhage. Newborn prophylactic and additional care indicators included vitamin K1 injection, no prophylactic antibiotic eye ointment in accordance with current national recommendations, and documented birth weight measurement.
The main independent variable for trend analysis was assessment round (Round 1, Round 2, Round 3). Subgroup analyses were conducted by hospital level (provincial vs district) and mode of delivery (vaginal vs cesarean birth).
Data Collection
Data were collected by trained research assistants using standardized WHO-aligned tools and the project monitoring framework. Each facility assessment was completed within one day per round by teams consisting of public health professionals reviewing maternal and newborn medical records and trained interviewers conducting postpartum interviews. Different data sources were used for different indicators. Newborn medical records assessed documented newborn care practices, including skin-to-skin contact, respiratory monitoring, vitamin K1 administration, avoidance of antibiotic eye ointment, and newborn weighing. Maternal medical records assessed postpartum maternal care practices such as uterotonic use and monitoring for postpartum hemorrhage and uterine contractions. Maternal interviews captured mother-reported experiences, including skin-to-skin contact, mother–newborn separation, early breastfeeding initiation, and prelacteal feeding. Facility observations assessed the availability of essential medicines, supplies, and hygiene conditions, although these were not included in the main trend analyses. Immediate skin-to-skin contact was assessed using both newborn medical records and maternal interviews because the two sources reflected complementary dimensions of EENC implementation: documented clinical practice and maternal experience. These measures were therefore analyzed separately. Postpartum interviews were conducted face-to-face in private or semi-private ward areas after written informed consent. The structured questionnaire assessed immediate skin-to-skin contact, mother–newborn separation, breastfeeding initiation within the first hour, and prelacteal feeding.
The interview questionnaire, record-review forms, and facility observation checklist were adapted from WHO-aligned monitoring tools and reviewed by maternal and newborn health experts. All tools were pilot-tested over three days at Thanh Hoa Provincial General Hospital to assess clarity, feasibility, consistency of record abstraction, workflow, and completion time. Findings from the pilot informed refinements to wording, interviewer guidance, abstraction procedures, and field organization before implementation across the three assessment rounds. The tools were not independently psychometrically validated and are provided in Supplementary File 1.
Data Analysis
Data were analyzed using Stata 19. Frequencies and percentages summarized EENC practices across the three rounds. Trend analyses included all eligible births unless otherwise specified. Round 3, representing the post-reinforcement assessment, was analyzed separately to describe current implementation levels and identify remaining gaps, particularly by mode of delivery. Subgroup analyses by hospital level (provincial vs. district) were conducted to explore contextual variation. Because stratification reduced sample sizes for some indicators, especially interview-based measures and those with restricted denominators, these analyses were considered exploratory and interpreted cautiously. Stratification by socioeconomic context was not performed due to insufficient relevant data. Differences across rounds were assessed using chi-square or Fisher’s exact tests, with Bonferroni-adjusted pairwise comparisons when appropriate. Assumptions for chi-square tests were assessed by examining expected cell frequencies, and Fisher’s exact test was used when expected cell counts were too small for the chi-square approximation to be appropriate. A two-sided p-value <0.05 was considered statistically significant. Missing values were not imputed. Analyses used eligible observations with non-missing data for each indicator; denominators, therefore, varied and are reported in the tables.
Ethical Considerations
This study received ethical approval from the University of Public Health Ethics Committee (Decision No. 440/2022/YTCC-HD3, dated 28/11/2022). Data were collected during three assessment rounds: 1–10 December 2022, 10–17 March 2024, and 20–30 August 2024. In each round, eligible mothers were interviewed after providing written informed consent; no minors were included in the study. Clinical information was also extracted from selected maternal and newborn medical records during the same assessment periods. All medical-record data were fully de-identified before analysis, and investigators had no access to personal identifiers. Participant confidentiality and data security were maintained throughout the study.
Results
Sample Characteristics
Distribution of Study Sample by Data Source and Hospital Level Across Three Survey Rounds
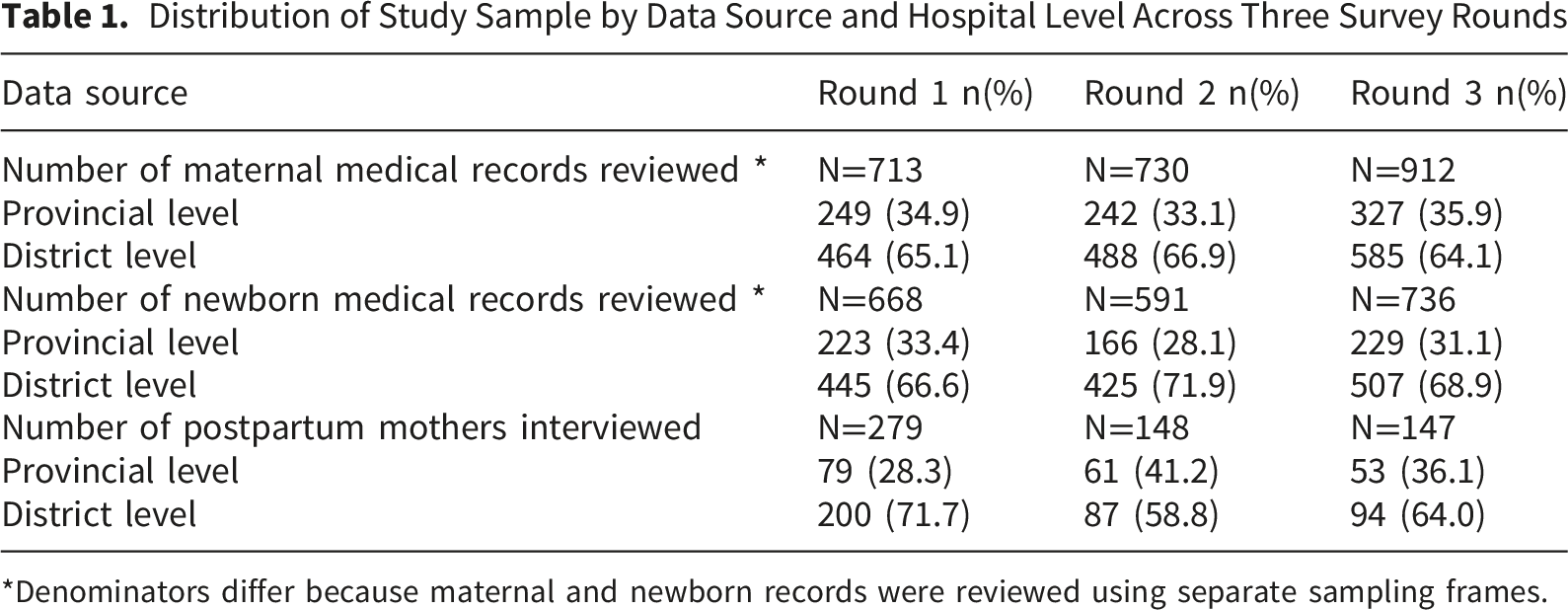
*Denominators differ because maternal and newborn records were reviewed using separate sampling frames.
Approximately two-thirds of observations came from district hospitals, consistent with the sampling design. Maternal and newborn records were reviewed independently and did not represent matched mother–newborn pairs, resulting in varying sample sizes across data sources and rounds. Participating hospitals were located in geographically diverse regions of Viet Nam, including north-central, northern mountainous, Central Highlands, and Mekong Delta provinces (More information can be found in Supplement table 1). Individual-level socioeconomic and demographic data were not collected in the monitoring dataset.
We first examined changes in EENC implementation across the three assessment rounds to describe overall trends. We then analyzed Round 3 data separately because it represented the most recent assessment after implementation and reinforcement of the QI activities, and it allowed us to identify remaining gaps by mode of delivery.
Trends in EENC Implementation
Trends in Implementation of EENC Practices Across Three Survey Rounds
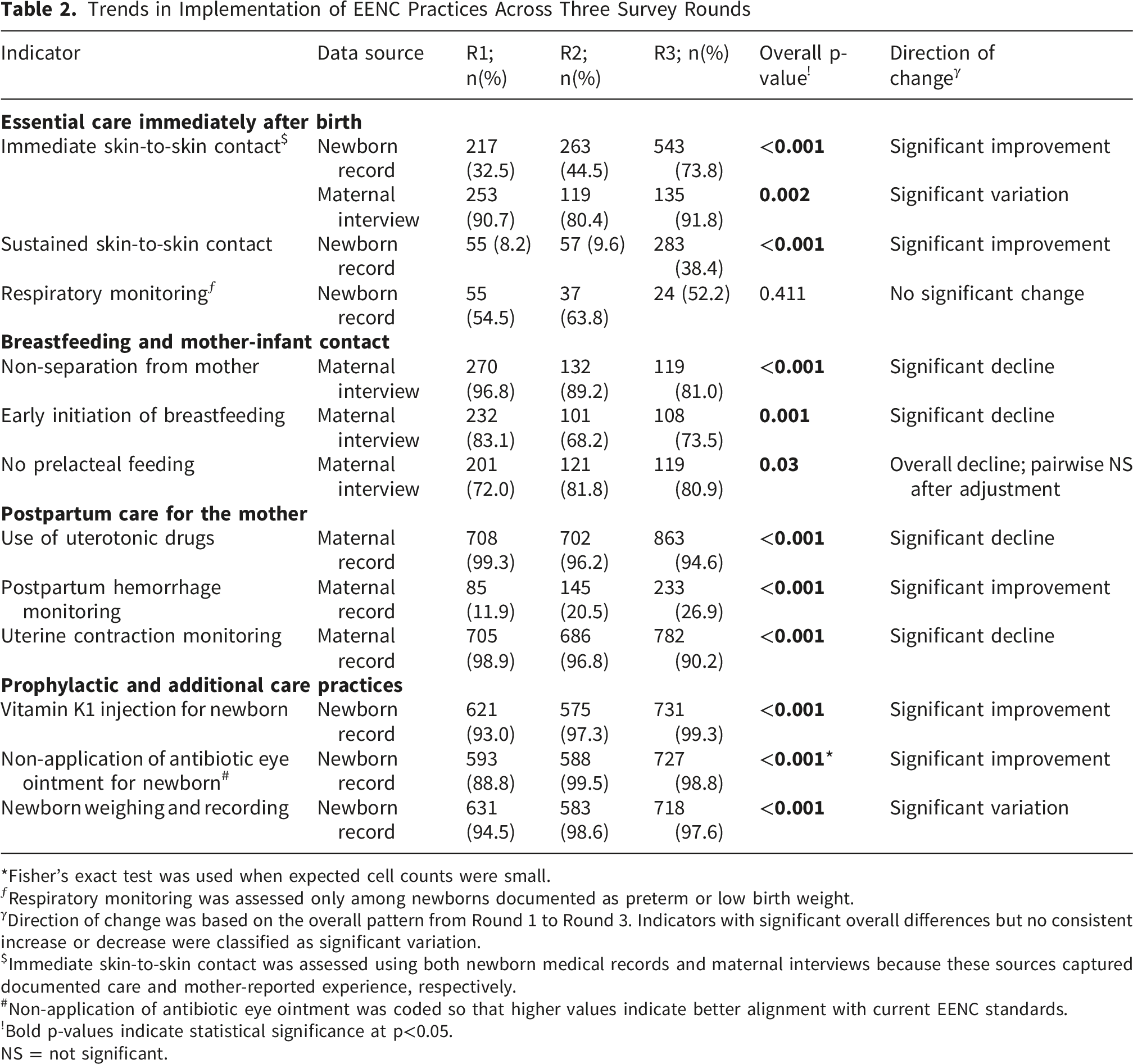
*Fisher’s exact test was used when expected cell counts were small.
ƒRespiratory monitoring was assessed only among newborns documented as preterm or low birth weight.
γDirection of change was based on the overall pattern from Round 1 to Round 3. Indicators with significant overall differences but no consistent increase or decrease were classified as significant variation.
$Immediate skin-to-skin contact was assessed using both newborn medical records and maternal interviews because these sources captured documented care and mother-reported experience, respectively.
#Non-application of antibiotic eye ointment was coded so that higher values indicate better alignment with current EENC standards.
!Bold p-values indicate statistical significance at p<0.05.
NS = not significant.
Bonferroni-adjusted pairwise comparisons were conducted for indicators with significant overall differences across rounds and are presented in Supplementary Table 2.
EENC Implementation Practices by Delivery Method in Round 3
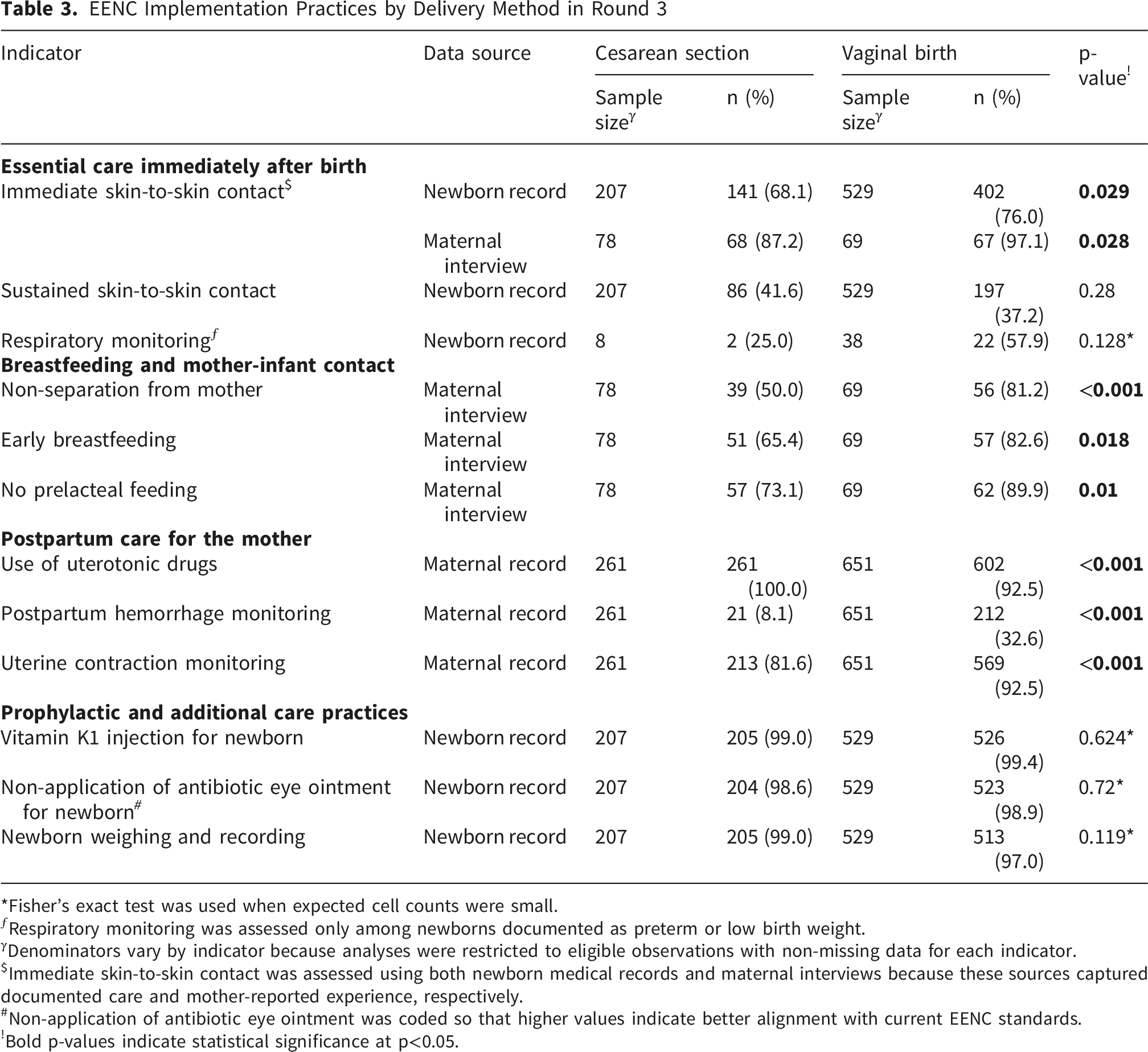
*Fisher’s exact test was used when expected cell counts were small.
ƒRespiratory monitoring was assessed only among newborns documented as preterm or low birth weight.
γDenominators vary by indicator because analyses were restricted to eligible observations with non-missing data for each indicator.
$Immediate skin-to-skin contact was assessed using both newborn medical records and maternal interviews because these sources captured documented care and mother-reported experience, respectively.
#Non-application of antibiotic eye ointment was coded so that higher values indicate better alignment with current EENC standards.
!Bold p-values indicate statistical significance at p<0.05.
Compared with vaginal births, CS births had lower rates of immediate skin-to-skin contact in both newborn records (68.1% vs. 76.0%) and maternal reports (87.2% vs. 97.1%). Mothers undergoing CS were also less likely to report remaining with their newborns after birth (50.0% vs. 81.2%, p<0.001), and early breastfeeding initiation was less common (65.4% vs. 82.6%, p=0.018). Although uterotonic administration was universal among CS deliveries, postpartum hemorrhage monitoring (8.1% vs. 32.6%) and uterine contraction monitoring (81.6% vs. 92.5%) remained significantly lower than among vaginal births. No significant differences were observed for respiratory monitoring, vitamin K1 administration, non-application of antibiotic eye ointment, or newborn weighing and documentation.
Exploratory Subgroup Analysis by Hospital Level
Exploratory subgroup analyses by hospital level are presented in Supplementary Table 3. In Round 3, documented immediate skin-to-skin contact was higher in district hospitals than in provincial hospitals, whereas postpartum hemorrhage monitoring and uterine contraction monitoring were higher in provincial hospitals. Vitamin K1 administration, non-application of antibiotic eye ointment, and newborn weighing and recording were high in both hospital levels. No substantial hospital-level difference was observed for mother-reported immediate skin-to-skin contact, non-separation, early breastfeeding, no prelacteal feeding, or respiratory monitoring. Because stratification reduced the number of observations for some indicators, particularly interview-based indicators and respiratory monitoring among preterm or low-birth-weight newborns, the subgroup results were interpreted descriptively. The purpose was to identify contextual patterns that may inform facility-tailored QI recommendations rather than to make definitive statistical comparisons between hospital levels.
Discussion
This study examined changes in Early Essential Newborn Care (EENC) across three assessment rounds following targeted quality improvement interventions in 14 hospitals in Vietnam. The findings showed clear improvements in several technical components of EENC. Documented immediate skin-to-skin contact in newborn medical records more than doubled, from 32.5% in Round 1 to 73.8% in Round 3. Maternal reports of immediate skin-to-skin contact remained consistently high across all rounds, and the narrowing gap between record-based and interview-based estimates may indicate improvements in both clinical practice and documentation. However, differences between these two data sources should be interpreted cautiously. Medical records reflect documented care, whereas maternal interviews reflect mothers’ reported experience. Lower values in newborn records compared with maternal reports may indicate under-documentation, differences in recall or interpretation, or both. From a quality improvement perspective, this distinction is important because accurate documentation is itself a component of implementation fidelity and continuity of care.
Sustained skin-to-skin contact and vitamin K1 administration also improved significantly. These improvements are consistent with the expected effects of on-site coaching and supportive supervision provided between assessment rounds. Such approaches are especially relevant in Vietnam, where some remote provinces continue to face shortages of skilled health workers and limited access to routine training opportunities. Similar improvements have been documented in other low- and middle-income countries (LMICs), where hands-on mentoring and regular supervision are recognized as effective strategies for improving provider performance in essential newborn care.7,8 These gains also support global commitments under the Sustainable Development Goals (SDGs), 9 particularly SDG 3.1 on maternal mortality and SDG 3.2 on ending preventable newborn deaths, building on earlier progress from the Millennium Development Goal (MDG) era.
Interpreting the findings against the benchmark of universal or near-universal implementation showed that by Round 3, vitamin K1 administration, newborn weighing/documentation, and non-application of antibiotic eye ointment achieved high coverage, indicating strong adherence to discrete prophylactic and documentation-based EENC practices. In contrast, sustained skin-to-skin contact, non-separation of mother and newborn, early breastfeeding initiation, avoidance of prelacteal feeding, and postpartum hemorrhage monitoring remained well below full coverage, highlighting persistent gaps in practices requiring sustained coordination, mother–infant support, and ongoing postpartum monitoring. Although several technical practices improved, declines were observed in indicators requiring continuous support and coordination. These declines should be interpreted cautiously because the repeated cross-sectional design lacked a control group. The QI intervention may have been more effective for discrete protocolized tasks, such as skin-to-skin initiation and vitamin K1 administration, than for practices requiring coordination across delivery rooms, operating rooms, and postnatal wards. In addition, indicators such as non-separation, early breastfeeding, and avoidance of prelacteal feeding depend on staffing, bed availability, breastfeeding support, ward routines, and cesarean-delivery workflows, which may not have been fully addressed by training and supervision alone. Smaller maternal interview samples in later rounds and changes in case mix, cesarean workload, and facility-level constraints may also have influenced trends over time. Overall, the findings suggest that training, coaching, and supervision were more effective for discrete technical tasks than for sustained behavioral and organizational practices.Consistent with evidence from other LMICs, challenges in supportive postpartum care often arise from system constraints such as heavy workloads, limited staffing, and the lack of dedicated breastfeeding support. The persistent gaps in EENC following cesarean births observed in this study mirror global patterns. 10 In many countries, operating room workflows, anesthesia routines, and physical space limitations continue to hinder early skin-to-skin contact and breastfeeding after surgical delivery. These challenges demonstrate that facility-level organization and workflow, rather than just staff knowledge, play a significant role in determining whether EENC can be implemented consistently.11,12
The findings have several policy implications for Vietnam and similar health-system settings. First, quality improvement efforts should extend beyond clinical training to address workflow, staffing, documentation, ward organization, and breastfeeding support. While improvements in immediate and sustained skin-to-skin contact, vitamin K1 administration, newborn weighing, and non-application of antibiotic eye ointment suggest that training and supervision can strengthen protocolized practices, indicators requiring sustained coordination, such as non-separation, early breastfeeding, avoidance of prelacteal feeding, and postpartum monitoring, require broader system-level support. Second, persistent gaps after cesarean birth highlight the need for specific EENC protocols in operating and recovery areas. Clear staff roles, stronger coordination across obstetrics, anesthesia, neonatal, and postnatal teams, and enhanced postoperative breastfeeding support are essential. Third, subgroup findings suggest the need for facility-tailored strategies. District hospitals may require continued supportive supervision and practical tools, while provincial hospitals may need improved cross-departmental coordination, particularly for cesarean deliveries. Although socioeconomic stratification was not available, geographic diversity among participating hospitals underscores the importance of adapting EENC strategies to local contexts. These priorities are relevant to LMICs aiming to scale up WHO-recommended newborn care and advance SDG maternal and newborn health targets.3,13,14
Strengths and Limitations
This study has several strengths. The multi-site design, including provincial and district hospitals across diverse provinces, provides practical insight into EENC implementation in varied service contexts. Repeated cross-sectional assessments enabled examination of changes over time in relation to staged quality improvement activities. The use of multiple data sources, maternal and newborn records, maternal interviews, and facility observations, allowed assessment of both documented care and mother-reported experience. Exploratory hospital-level analyses further supported context-specific interpretation.
Several limitations should be noted. The repeated cross-sectional design without a control group limits causal inference; improvements cannot be attributed solely to the intervention. Medical record review may introduce documentation bias, while interviews may be affected by recall and social desirability biases. Postpartum interviews were conducted only among mothers present and consenting on data-collection days, potentially introducing selection bias; smaller interview samples in later rounds also limit comparability. No formal sample size calculation was conducted, and some subgroup analyses may have had limited statistical power; hospital-level comparisons should therefore be considered exploratory. The dataset lacked socioeconomic and detailed contextual variables, limiting the analysis of demographic and community factors. Although data-collection tools were WHO-aligned and pilot-tested, they were not formally validated, and findings were interpreted in terms of their magnitude and programmatic relevance rather than solely on statistical significance.
Future research should examine facility-level mechanisms influencing EENC implementation, particularly after cesarean birth, and incorporate standardized contextual indicators. Controlled or quasi-experimental designs would strengthen causal inference.
Conclusion
This multi-site evaluation found that targeted quality improvement activities were associated with improvements in several technical EENC practices, including immediate and sustained skin-to-skin contact, vitamin K1 administration, newborn weighing, and non-application of antibiotic eye ointment. However, gaps persisted in mother - infant support and maternal monitoring practices, particularly after cesarean birth. These findings indicate that training and supervision alone are insufficient for full EENC implementation. Sustained improvement will require workflow redesign, clearer staff roles, strengthened breastfeeding support, improved postpartum monitoring, and context-specific strategies across hospital levels.
Supplemental Material
Supplemental Material - Supplemental Material for Evaluating a Multi-Site Quality Improvement Intervention for Early Essential Newborn Care: Trends and Persistent Gaps Across Three Assessment Rounds in Viet Nam
Supplemental Material for Evaluating a Multi-Site Quality Improvement Intervention for Early Essential Newborn Care: Trends and Persistent Gaps Across Three Assessment Rounds in Viet Nam by Bui Thi Tu Quyen, Vu Thi Hoang Lan, Nguyen Van Chi, Hoang Anh Tuan, Hoang Tran, Pham Quynh Nga, Marzia Lazzerini and Nuhu Omeiza Yaqub JR in Health Services Insights.
Supplemental Material
Supplemental Material - Supplemental Material for Evaluating a Multi-Site Quality Improvement Intervention for Early Essential Newborn Care: Trends and Persistent Gaps Across Three Assessment Rounds in Viet Nam
Supplemental Material for Evaluating a Multi-Site Quality Improvement Intervention for Early Essential Newborn Care: Trends and Persistent Gaps Across Three Assessment Rounds in Viet Nam by Bui Thi Tu Quyen, Vu Thi Hoang Lan, Nguyen Van Chi, Hoang Anh Tuan, Hoang Tran, Pham Quynh Nga, Marzia Lazzerini and Nuhu Omeiza Yaqub JR in Health Services Insights.
Supplemental Material
Supplemental Material - Supplemental Material for Evaluating a Multi-Site Quality Improvement Intervention for Early Essential Newborn Care: Trends and Persistent Gaps Across Three Assessment Rounds in Viet Nam
Supplemental Material for Evaluating a Multi-Site Quality Improvement Intervention for Early Essential Newborn Care: Trends and Persistent Gaps Across Three Assessment Rounds in Viet Nam by Bui Thi Tu Quyen, Vu Thi Hoang Lan, Nguyen Van Chi, Hoang Anh Tuan, Hoang Tran, Pham Quynh Nga, Marzia Lazzerini and Nuhu Omeiza Yaqub JR in Health Services Insights.
Footnotes
Acknowledgements
The authors thank the provincial health authorities and participating hospitals for facilitating data collection and acknowledge the support of the WHO Vietnam Office for funding the data-collection activities awarded to Dr. Bui Thi Tu Quyen.
Ethical Considerations
The University of Public Health Ethics Committee approved the study under Decision No. 36/2023/YTCC-HD3. Written informed consent was obtained from all participating mothers prior to any observation or interview.
Consent to Participate
Participant anonymity and data confidentiality were strictly maintained throughout the research process. All data collection adhered to international guidelines for ethical conduct and participant confidentiality.
Author Contributions
Conceptualization: Bui Thi Tu Quyen (BTTQ), Vu Thi Hoang Lan (VTHL); Data curation and verification: VTHL, BTTQ; Formal analysis: BTTQ and VTHL; Writing original draft: All authors; Writing, review & editing: All authors. VTHL and BTTQ directly accessed and verified the underlying dataset. All authors had full access to all data in the study and accepted responsibility for the decision to submit for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. No funding was received for writing or publishing this manuscript. Data collection activities were supported by a grant from the World Health Organization (WHO) Vietnam awarded to Dr. Bui Thi Tu Quyen.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the study are not publicly available due to institutional restrictions but are available from the corresponding author, Dr. Bui Thi Tu Quyen (email:
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.