
Abstract
Background
Acute rheumatic fever (ARF) and rheumatic heart disease (RHD) remain major public health challenges in low- and middle-income countries, where limited awareness, delayed care-seeking, and inadequate provider training contribute to preventable morbidity and mortality.
Methods
A narrative review was conducted using an integrative synthesis framework to examine educational and awareness strategies implemented between 2010 and 2025. Searches across MEDLINE, Scopus, CINAHL, DOAJ, and grey literature sources identified studies reporting educational interventions targeting community members, mothers, students, or healthcare workers. Seven eligible studies were synthesised thematically based on intervention type, delivery modality, and outcomes.
Result
Across the seven included studies, educational and awareness interventions consistently improved knowledge, attitudes, preventive practices, or clinical competencies related to ARF/RHD. Although study designs, target populations, and delivery modes varied widely, all interventions demonstrated positive short-term effects. Healthcare-worker programmes reported notable gains in clinical understanding and confidence, particularly regarding diagnosis and benzathine penicillin use. Maternal education improved awareness and preventive practices, while school-based sessions enhanced immediate understanding despite a gradual decline over time. Community-level mass-media campaigns achieved broad reach and generated substantial increases in both knowledge and seeking care for sore throat. Collectively, the evidence demonstrates clear beneficial trends, though long-term sustainability and comparative effectiveness remain insufficiently evaluated.
Conclusion
Educational and awareness interventions consistently improve ARF/RHD-related knowledge, behaviours, and clinical competencies. Sustained impact, however, depends on integrated, multi-level approaches that combine school-based reinforcement, maternal education, health-worker training, and community-wide communication.
Introduction
Rheumatic heart disease (RHD) remains a major cause of preventable morbidity and premature mortality in low- and middle-income countries, where delayed recognition of streptococcal pharyngitis and limited access to timely prophylaxis continue to drive new cases.1,2 The condition arises from an autoimmune response to Streptococcus pyogenes (group A streptococcus, GAS), which, if inadequately managed, can progress to acute rheumatic fever (ARF) and permanent cardiac valvular damage.3-5 The World Health Organization (WHO) estimates that RHD accounts for over 288,348 deaths annually. 2 This burden is felt most acutely in resource-limited settings, where overcrowding and poverty exacerbate the spread of infection.6-8
Although effective preventive strategies exist, a substantial gap remains between recommended practices and their real-world implementation at the community level. Effective control of ARF and RHD depends on primary prevention (early and appropriate antibiotic treatment of streptococcal sore throat) and secondary prevention (regular prophylaxis with Benzathine penicillin G injections).9-11 However, limitations in community awareness, health worker knowledge, and health seeking behaviour continue to hinder effective implementation, underscoring the need for structured educational intervention. Over the past decade, diverse approaches such as school-based intervention, community campaigns, and clinical training programs have been implemented across resource-limited settings to improve recognition, prevention, and management of ARF and RHD.9,10,12-15 However, evidence on their effectiveness is limited and heterogeneous, with considerable variation exists across studies in terms of design, target populations, and delivery methods, which limits the ability to draw generalizable conclusions.16-18 While many pilot programs have demonstrated short-term success, consistency in long term outcomes across different settings remains unclear. Moreover, there is a lack of consolidated evidence identifying which specific educational modalities, ranging from mass media to digital tools, offer the most sustainable impact in low-resource contexts.17,19
Using an integrative synthesis approach, this narrative study analyses educational and awareness interventions carried out between 2010 and 2025 and interprets various intervention strategies uses in contexts with limited resources. By analyzing data across four key target groups: healthcare workers, mothers, students, and the general community. This narrative review synthesizes current evidence to examine how educational and awareness interventions influence knowledge, attitudes, practices, and clinical competencies related to ARF/RHD, and to identify lessons that can inform scalable, contextually appropriate prevention.
Method
This study is a narrative review using an integrative synthesis approach. A structured search strategy was employed, the review did not aim to be fully systematic or exhaustive, but rather to provide a comprehensive and interpretive synthesis of available evidence.
During the preliminary literature search, variation was observed among the existing studies in terms of study design, intervention type, target population, and outcome measures. Due to this heterogeneity, an integrative narrative review approach was adopted.
The review included quasi-experimental, pre–post interventional, randomized, and community-based studies.
Data were synthesized using an integrative framework adapted from Whittemore and Knafl (2005). 20 to allow contextual interpretation of diverse interventional strategies. The quality of narrative review was evaluated using the Scale for the Assessment of Narrative Review Articles (SANRA). 21
The Framework review process was carried out in five stages: (i) problem identification, (ii) literature search, (iii) data evaluation, (iv) data analysis, and (v) presentation of findings.
Problem Identification and Finalization of the Research Question
Educational and awareness interventions have long been recognized as critical pillars components of primary and secondary prevention of RHD; existing studies are scattered and lack consolidated evaluation. However, existing evidence remains scattered and lacks a consolidated evaluation across different implementation contexts. Given that prevention strategies for ARF and RHD involve multiple stakeholders, including healthcare workers, caregivers, school-aged children, and community members, this review adopts a broad perspective to capture interventions delivered at different levels of the health system and community.
This gap informed the development of the research question guiding this review: What types of educational and awareness interventions have been implemented for the prevention and control of ARF and RHD in resource-limited settings, and what lessons can be drawn to inform evidence-based policy and scalable practice?
Search Strategy
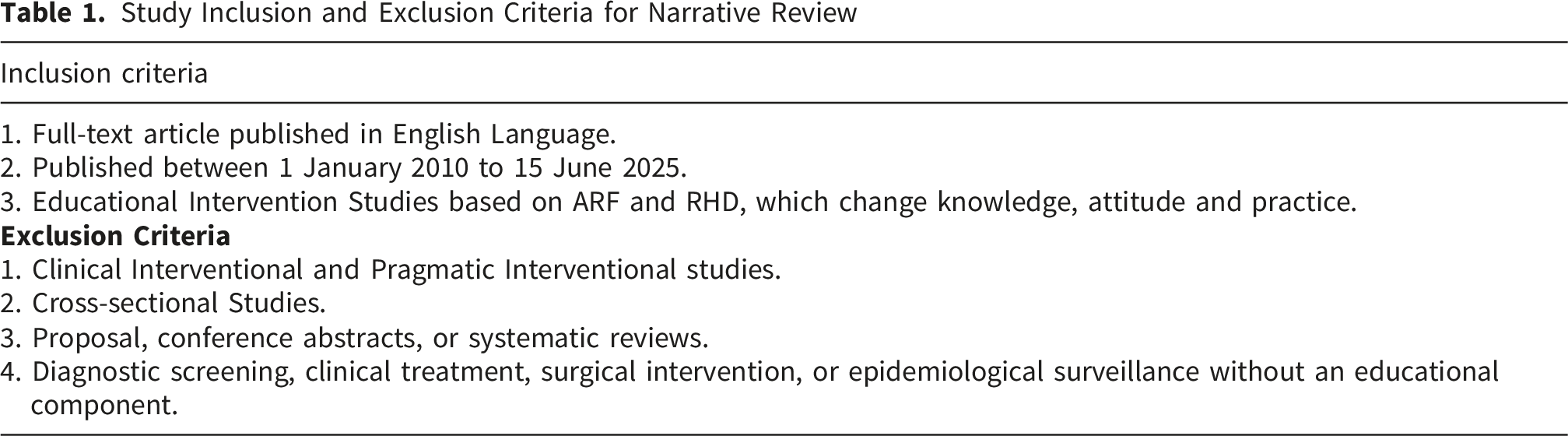
A comprehensive search of MEDLINE, Scopus, CINAHL, and the Directory of Open Access Journals (DOAJ) Was conducted to identify studies published between 1 January 2010 to 15 June 2025, a period selected to reflect the era in which renewed global advocacy for RHD control emerged. Additional articles were identified through the reference lists of the retrieved articles and the Google Scholar search engine. The search combined keywords and Medical Subject Headings (MeSH) terms, including (“rheumatic heart disease” OR “acute rheumatic fever”) AND (“education” OR “training” OR “awareness” OR “health promotion” OR “community intervention”). Grey literature, including WHO and World Heart Federation reports, was also reviewed. Additional sources were identified through backward citation searching of included studies. Because this is a narrative review, the search did not aim for exhaustive retrieval, but for comprehensive coverage of the major educational interventions implemented in low-resource settings.
Study Inclusion and Exclusion Criteria for Narrative Review
Charting Data and Data Evaluation
All titles and abstracts retrieved from the search were independently screened by two researchers (GS and PK), followed by full-text review of potentially eligible studies. Any discrepancies were resolved through discussion to ensure consistent application of the eligibility criteria. Data were extracted using a structured form in Microsoft Excel, capturing study setting, design, duration, sample size, population characteristics, nature of the educational intervention, delivery modality, and outcome measures. This standardized approach facilitated cross-study comparison and provided a coherent foundation for synthesis.
Data Synthesis and Presentation
Data from the included studies were analyzed using a structured narrative synthesis approach appropriate for heterogeneous quantitative evidence. After the extraction process was completed, research team members SP, GS, and PK repeatedly reviewed the study characteristics, intervention components, delivery strategies, and reported outcomes to gain complete familiarity with the evidence base. The extracted information was then organized systematically into categories that reflected the central features of the interventions, including their target populations, the educational approaches employed, and the outcomes assessed. This categorization allowed meaningful comparison across studies and enabled the identification of consistent patterns in how different types of educational interventions influenced knowledge, attitudes, practices, confidence, and related behavioural measures.
Summary of Findings by Intervention Category
Result
The comprehensive search across four major databases and supplementary sources initially identified 507 records. After removing 50 duplicates, 457 unique titles and abstracts were screened. Of these, 306 records were excluded due to non-interventional study designs or topics unrelated to ARF and RHD. A total of 151 articles were assessed for eligibility, of which 144 articles were excluded for reasons such as focusing solely on patients already diagnosed with RHD, targeting primary or secondary prevention interventions, addressing pragmatic interventions, focusing on clinical or therapeutic management, self-management, diagnostic or screening interventions, or being limited to educational content for medical professionals. Narrative reviews, commentaries, and editorials were also excluded. Ultimately, 7 studies met all inclusion criteria and were included in this narrative synthesis.
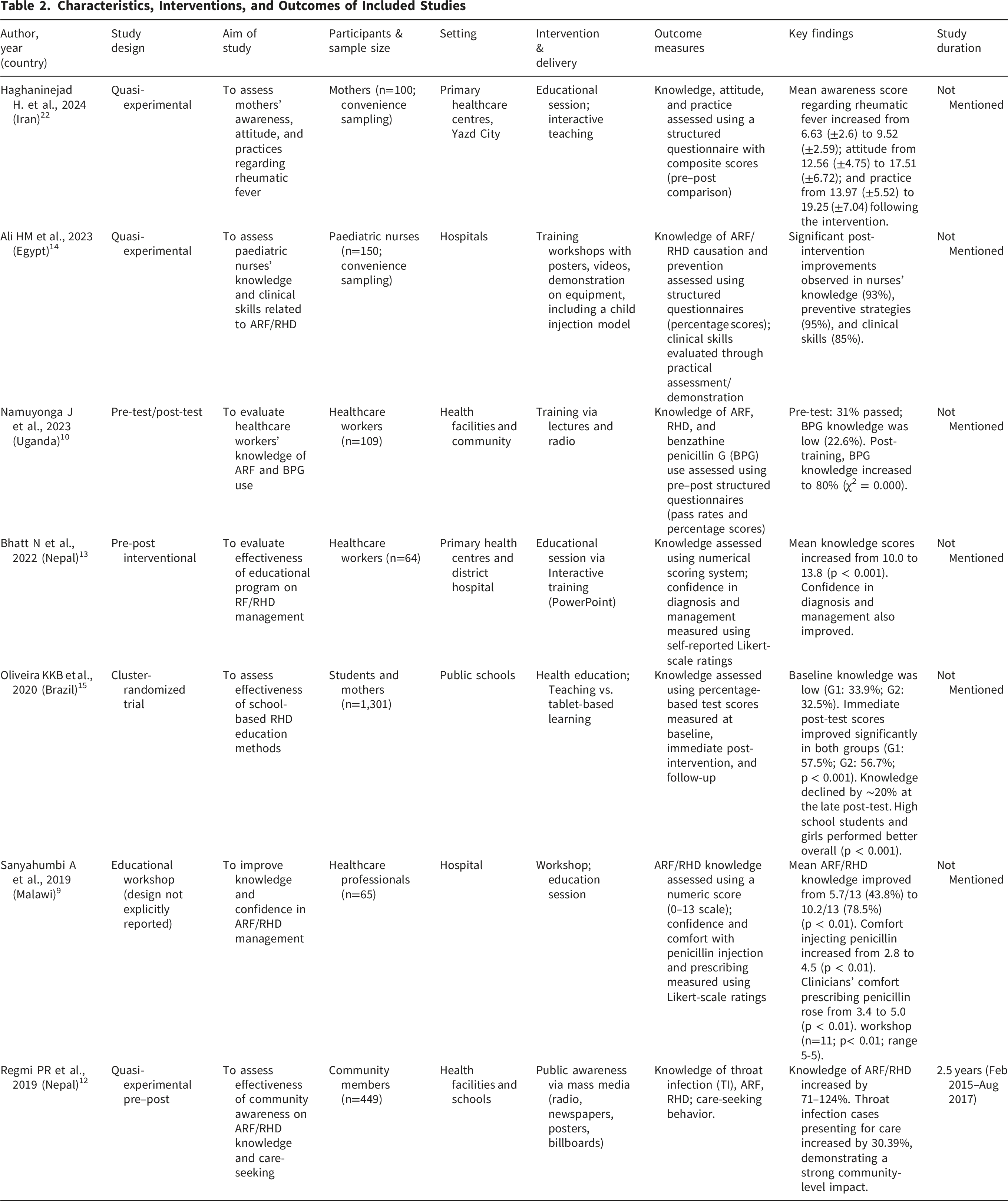
The seven included studies originated from Nepal (n=2), Iran (n=1), Brazil (n=1), Egypt (n=1), Malawi (n=1), and Uganda (n=1), reflecting a wide spectrum of educational strategies for ARF/RHD prevention. Study designs included quasi-experimental pre–post interventions, cluster-randomized trials, and interventional training programs. Sample sizes ranged from 14 to 1,301 participants, and the interventions targeted four major population groups: Community members and schoolteachers 12 Healthcare workers,9,10,13,14 Mothers of reproductive age 22 School students. 15
Interventions varied in delivery modality, including mass media campaigns 12 structured workshops 9,14 didactic lectures, 10 and tablet-based digital learning tools.14,15 All studies assessed changes in knowledge, attitudes, practices, confidence, or clinical skills related to streptococcal pharyngitis, ARF, or RHD. Table 2 provides an overview of each study’s author, year, design, aim, participants, sample size, setting, intervention, delivery, outcome measures, key findings and duration. Together, the studies illustrate the broad spectrum of educational strategies currently used in ARF/RHD prevention across resource-limited settings.
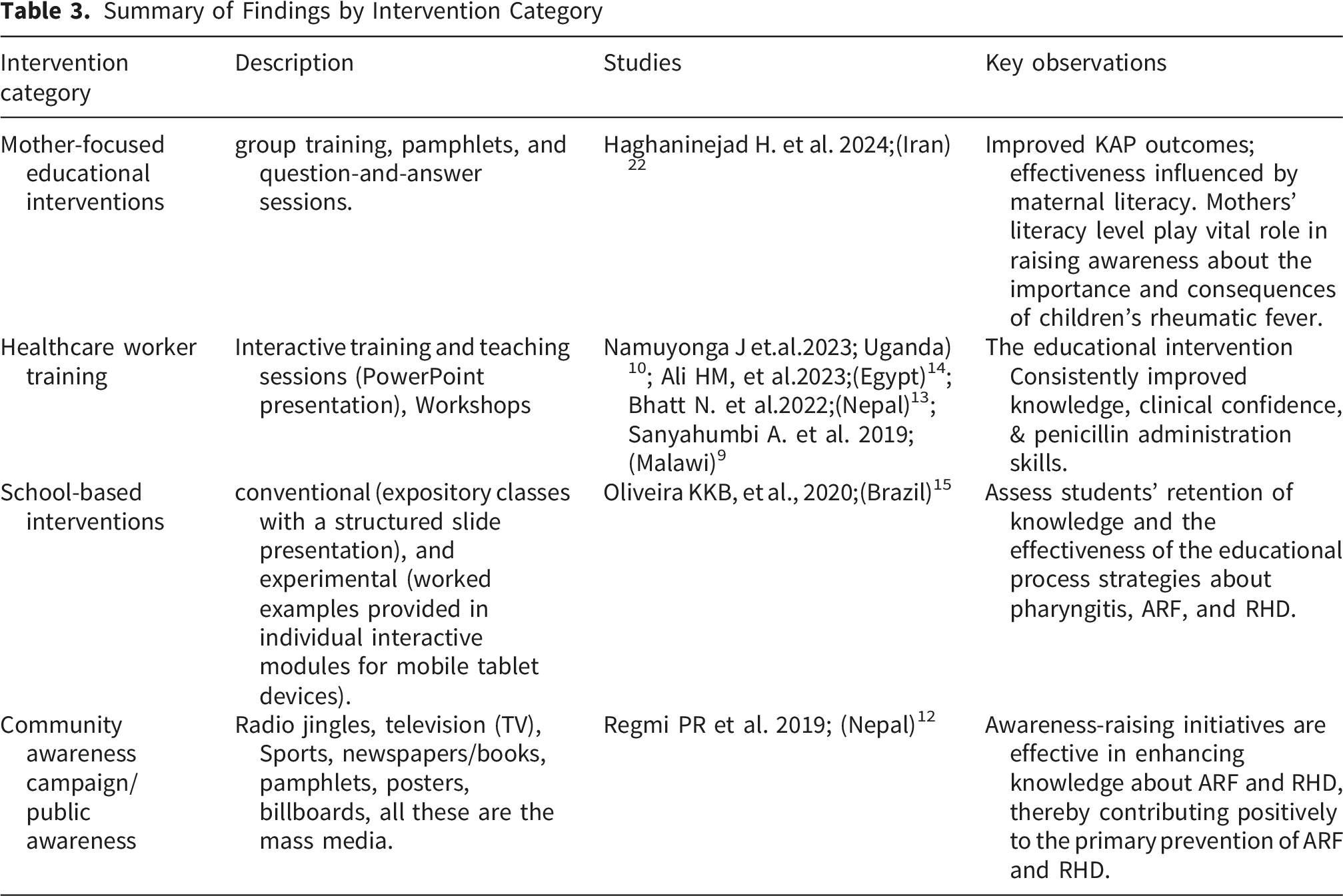
The seven studies demonstrated considerable diversity in the types of interventions implemented, the delivery strategies employed, and the outcomes assessed. Intervention components included mass media campaigns, structured workshops, interactive teaching sessions, hands-on practical demonstrations, and digital learning tools. Across all studies, the primary outcomes assessed were related to knowledge, attitudes, practices, skills, or confidence in recognising and preventing ARF and RHD. The table summarises intervention content, mode of delivery, target audience, outcome measures, and the main findings of each existing studies are in Table 3.
The synthesis of findings across the included studies demonstrates that educational and awareness interventions consistently improved knowledge, attitudes, skills, and preventive practices related to acute rheumatic fever and rheumatic heart disease, although the magnitude and nature of improvement varied by target group and delivery approach. Community-level awareness campaigns using mass media, such as radio, television, and posters, were effective in reaching large populations and substantially enhancing general knowledge, contributing positively to primary prevention efforts. Interventions targeting healthcare workers, delivered through interactive training sessions, lectures, and workshops, showed strong improvements in clinical understanding and confidence in the diagnosis and management of rheumatic fever and rheumatic heart disease, with additional gains observed when practical, hands-on components such as throat examination and penicillin administration were included. Educational programmes for mothers of reproductive age improved awareness, attitudes, and preventive practices, though effectiveness was influenced by maternal literacy and age, highlighting the need for accessible and context-sensitive materials. School-based health education initiatives improved students’ short-term understanding of pharyngitis, acute rheumatic fever, and rheumatic heart disease irrespective of whether conventional or tablet-based methods were used, although knowledge retention diminished over time, indicating the importance of reinforcement. Collectively, these findings underscore that while diverse educational strategies are effective in improving immediate knowledge and competencies across community, clinical, and school settings, sustained impact requires ongoing engagement, practical skill-building, and adaptation to contextual factors such as literacy levels, health-system support, and learner characteristics.
Discussion
This narrative review demonstrates that educational and awareness interventions are generally associated with improvements in knowledge, attitudes, skills, and preventive practices related to ARF and RHD across diverse low-resource settings. However, the strength and consistency of these effects vary across studies, populations, and delivery approaches. Given the small number of included studies and their methodological diversity, these findings should be interpreted with caution. Nonetheless, the available evidence indicates that education remains a potentially important component of both primary and secondary RHD prevention in endemic regions.
Across the included studies, interventions targeting healthcare workers appeared to yield substantial improvements. Health workers demonstrated substantial gains in understanding ARF diagnostic criteria, RHD pathophysiology, and the correct use of benzathine penicillin.9,10,13,14 These findings align with broader global evidence that competency-based, practical training outperforms purely didactic approaches in low- and middle-income countries (LMICs), particularly when focused on neglected diseases.23,24 The inclusion of experiential learning elements mirrors recommendations in the World Heart Federation’s and the WHO guideline on prevention and diagnosis of RHD, which explicitly advocate blended theoretical–practical models to address persistent gaps in frontline provider capacity.11,25,26
School-based education interventions were generally effective in improving short-term knowledge. However, the consistent decline in knowledge at later follow-ups highlights the limitations of one-time instruction and underscores the need for curricular integration and repeated reinforcement. 15 This pattern aligns with cognitive psychology research on the Ebbinghaus forgetting curve and with longitudinal evaluations of one-off health education in adolescents.27,28 Integration of ARF/RHD content into routine school health curricula, coupled with periodic teacher-led reinforcement, has been successfully implemented in high-income countries that eliminated endemic RHD and offers a feasible, low-cost model for LMICs.29-32 The comparable performance of digital and traditional approaches in the included trial indicates that reinforcement frequency and content relevance may be more influential than modality alone. Embedding RHD content into school curricula and enabling teacher-led periodic refreshers may yield more sustainable outcomes.
Community-level mass-media campaigns showed potential for scalability and wide population reach. The quasi-experimental study from Nepal, utilising radio broadcasts, posters, and community events, achieved widespread knowledge gains and a >30% increase in care-seeking for sore throat. 12 Comparable behavioural shifts have been documented in large-scale campaigns for tuberculosis, malaria, and vaccine-preventable diseases in LMICs, where repeated, culturally resonant messaging through accessible channels modifies health-seeking behaviour even in the absence of intensive face-to-face contact.32-34 These findings suggest a potentially important role for mass media for primary prevention in settings where healthcare access remains limited, and delays in recognising streptococcal pharyngitis are a major driver of ARF incidence.
Only one study focused on mothers of reproductive age, despite evidence that maternal knowledge strongly influences children’s health-seeking behaviour and early recognition of sore throat. The intervention led to significant improvements in knowledge, attitudes, and preventive practices. This observation is consistent with extensive global literature showing that maternal health literacy is a critical determinant of childhood illness recognition and timely care-seeking, including for streptococcal infections.35,36 The scarcity of maternal-focused interventions in the current evidence base represents a missed opportunity, given that mothers are often the primary decision-makers for childhood healthcare in endemic communities.
Taken together, the limited evidence suggests that no single educational modality alone may be sufficient on its own. Rather, effective ARF and RHD prevention requires a coordinated, multilevel approach that simultaneously strengthens community awareness, school-based learning, caregiver understanding, and health-worker capacity. Historically, countries that achieved major reductions in RHD adopted integrated public health strategies combining education with strong primary care systems and consistent access to prophylaxis.29,30,32 Similar comprehensive models may be essential for contemporary endemic settings, especially where structural barriers such as limited health infrastructure, low literacy, or inconsistent medication supply undermine the impact of stand-alone interventions.
This review also highlights several important research gaps. There remains a notable absence of long-term follow-up in most studies, making it difficult to assess whether improvements in knowledge translate into sustained behavioral change or reductions in ARF incidence. Few interventions evaluated cost-effectiveness, limiting policymakers’ ability to determine which strategies offer the greatest impact for limited resources. There is also limited evidence on culturally tailored interventions, the influence of gender norms on health-seeking behaviour, and the role of the broader community, such as teachers, fathers, youth leaders, and peer educators, in shaping awareness and response to sore throat and ARF. Finally, digital education tools, although increasingly accessible, remain underexplored in combination with community-based reinforcement approaches. However, the evidence indicates that educational interventions are a powerful component of ARF and RHD prevention, but their impact depends on context, reinforcement, and integration within broader health systems. Strengthening caregiver education, enhancing practical training for healthcare workers, and embedding RHD content into school health curricula could meaningfully expand the reach and sustainability of current efforts. Future research should prioritize long-term evaluation, culturally grounded strategies, and multi-component programs that reflect the complex determinants of ARF and RHD in endemic communities. Together, these approaches offer a promising foundation for reducing the preventable burden of rheumatic heart disease across low-resource settings.
Limitations
This review has several limitations that should be acknowledged. First, a narrative review approach was adopted due to the limited availability of studies specifically addressing interventions for RHD and ARF. Consequently, the review does not adhere to a fully systematic methodology, which may affect the comprehensiveness and reproducibility of the findings. Second, the number of eligible studies identified was small, reflecting the scarcity of research in this area. This limited evidence base constrains the strength of the conclusions and underscores the need for further primary research. Third, the inclusion of only English-language publications may have resulted in the exclusion of relevant studies published in other languages, thereby introducing potential language bias. Fourth, there was substantial heterogeneity among the included studies in terms of study design, population characteristics, and types of interventions. This variability limited the comparability of findings across studies and precluded the possibility of conducting a quantitative synthesis. Finally, the available studies provided limited data on long-term outcomes, restricting the ability to assess the sustained effectiveness of interventions for RHD and ARF. Despite these limitations, this review offers a useful synthesis of the existing evidence and highlights important gaps that should be addressed in future research.
Conclusion
Educational and awareness interventions appear to play an important role supporting the prevention and control of acute rheumatic fever and rheumatic heart disease across low-resource settings. Across communities, schools, households, and health facilities, these interventions were generally associated with improvements in knowledge, attitudes, preventive practices, and clinical competencies. However, the evidence base remains limited, and the observed effects vary across settings and intervention types.
While one-off or isolated interventions may improve short-term outcomes, their impact on behaviour and disease prevention remains uncertain. Strengthening educational strategies across multiple levels of the health system may enhance their effectiveness, particularly when combined with ongoing reinforcement and integration into existing health and education structures. Further research with larger samples, standardized outcome measures, and longer follow-up is needed to better understand the sustainability and real-world impact of these interventions.
Footnotes
ORCID iDs
Author Contributions
GS: Conceptualization, Project Administration, Writing Original Draft. PK: Conceptualization, Project Administration, Writing Original Draft. DK: Conceptualization, Project Administration, Manuscript Review, and Editing. RPH: Project Administration, Manuscript Review, and Editing. YC: Writing Original Draft, Review, and Editing. SP: Conceptualization, Project Administration, Manuscript Review, and Editing. SK: Conceptualization, Manuscript Review, and Editing. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.