
Abstract
Background:
Microplastics (MPs) and nanoplastics (NPs) are increasingly detected in human tissues, prompting concern about potential biological effects. Yet, for most outcomes, the literature remains dominated by detection studies and preclinical toxicology, with limited human dose-response data.
Methods:
We conducted a narrative review of peer-reviewed literature (2000-2025), prioritizing human biomonitoring and tissue-detection studies, observational health-outcome studies, and mechanistic evidence that plausibly links exposure to cardiometabolic, reproductive, and neuroinflammatory pathways. Certainty of evidence was appraised using GRADE principles where applicable and explicitly separated from mechanistic plausibility.
Results:
MPs/NPs have been reported in blood, lung, placenta, atherosclerotic plaques, brain, liver, and testicular tissue. The most clinically salient human outcome signal to date is an association between plaque microplastics and subsequent major adverse cardiovascular events in an observational cohort (hazard ratio 4.53, 95% CI 2.00-10.27). However, polymer quantification approaches vary (particle counts vs polymer mass), contamination control is method-dependent, and inter-study comparability remains limited.
Conclusion:
The current evidence base supports aggressive exposure reduction as the most defensible “first-line” strategy. Nutritional approaches (dietary fiber, gut-barrier support, and microbiome modulation) are best framed as adjunctive, mechanistically plausible risk-mitigation strategies rather than proven methods to remove plastics from the body. Well-designed human trials and standardized analytical protocols are needed before clinical “detoxification” claims can be justified.
Keywords
Introduction
Global plastic production exceeds 400 million metric tons per year, and environmental fragmentation generates microplastics (1 μm-5 mm) and nanoplastics (1 nm-1 μm) that contaminate air, water, and food chains.1,2
Human exposure is unavoidable but modifiable. The dominant pathways are ingestion (food and water) and inhalation (indoor and outdoor air), with early-life exposures highlighted by microplastic release from polypropylene feeding bottles during formula preparation.3,4
A critical distinction for clinicians is between (i) detection of polymers in tissue, (ii) biological plausibility of harm, and (iii) proven causation. Most human data currently support the first, suggest the second, and remain insufficient for the third.
Accordingly, this review focuses on what the best available evidence can support now, where uncertainty remains high, and how nutrition-related interventions can be responsibly discussed without overstating detoxification claims. A schematic overview of the exposure-to-detection pathway and the clinical mitigation hierarchy is provided in Figure 1.
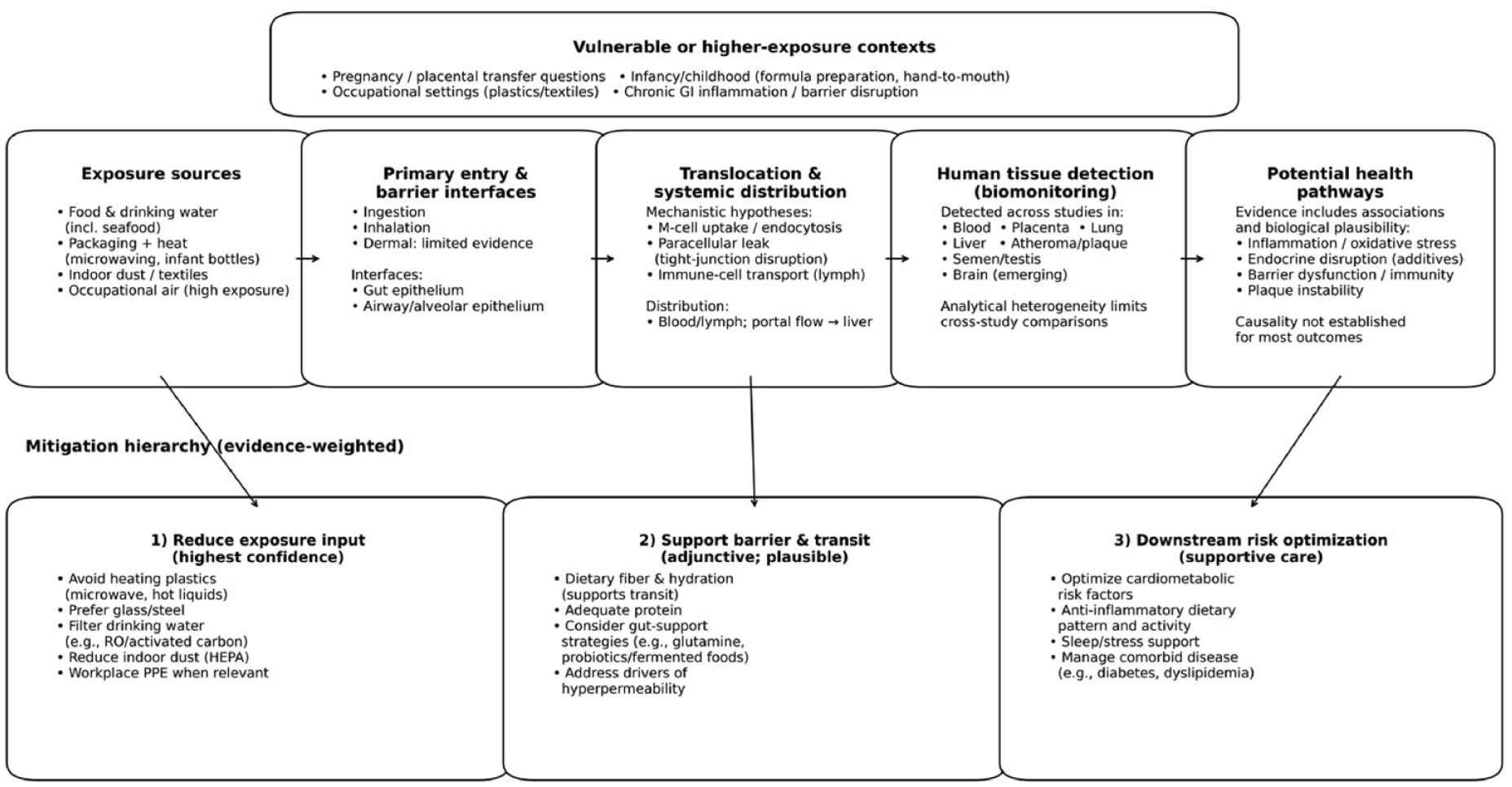
Conceptual pathway from exposure to tissue detection and potential health pathways, with an evidence-weighted mitigation framework. Evidence is strongest for exposure reduction; barrier-support and downstream strategies require human trials using MP/NP burden endpoints.
Methods
We conducted a narrative review of peer-reviewed literature published between January 2000 and December 2025. Searches were performed in PubMed/MEDLINE and supplemented with Google Scholar for citation-chaining of key papers. We used combinations of terms including “microplastic*,” “nanoplastic*,” “human,” “biomonitoring,” “blood,” “placenta,” “lung,” “liver,” “brain,” “testis/testes,” “semen,” “atheroma/atherosclerotic plaque,” “pyrolysis GC/MS,” “FTIR,” “Raman,” “cardiovascular,” “pregnancy,” “fertility,” “gut barrier,” “dietary fiber,” “bile acid*,” and “probiotic*.”
Because the field spans environmental analytics and clinical outcomes, we prioritized: (i) human biomonitoring studies with polymer identification and explicit contamination control, (ii) human observational studies relating internal detection to clinical outcomes, and (iii) systematic reviews and mechanistic studies that clarify biological plausibility. We did not use purely environmental surveys without human exposure relevance to support clinical claims. Preprints were included only when clearly labeled as non-peer reviewed.
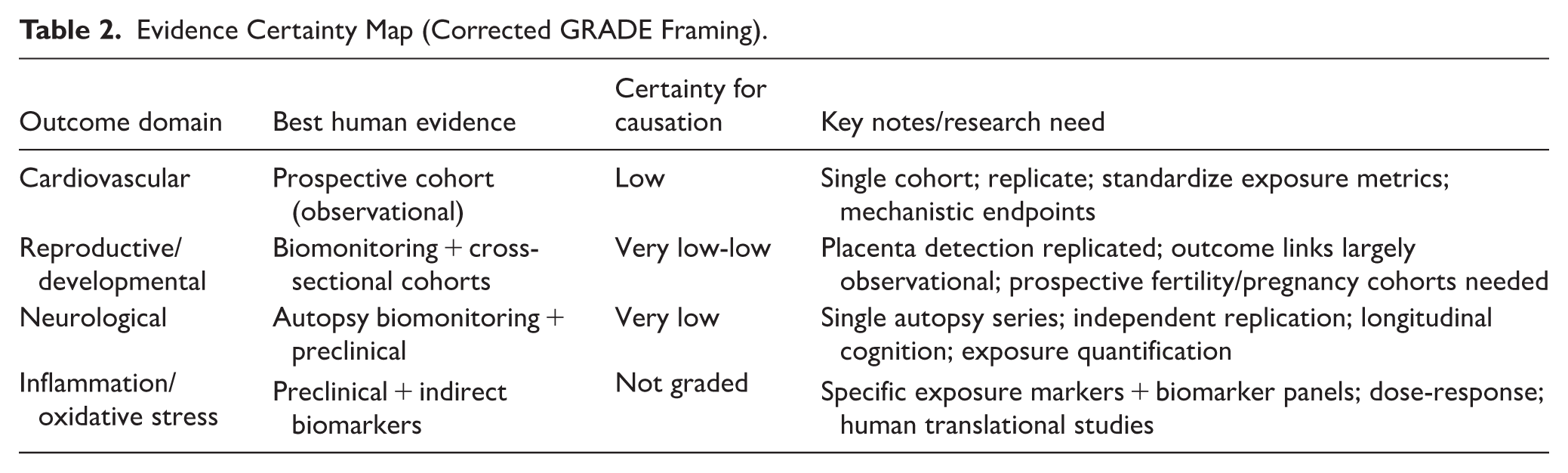
Evidence appraisal followed GRADE principles where applicable: observational human associations were treated as low certainty for causation in the absence of randomized trials and standardized exposure quantification, and preclinical studies were used to illustrate mechanism rather than intervention efficacy. Because exposure metrics and analytical methods are heterogeneous (particle counts vs polymer mass, varying size cutoffs), we did not perform a meta-analysis; instead, we summarize evidence qualitatively and explicitly flag key findings as replicated versus emerging when the human evidence rests on single studies.
Exposure Sources and Biokinetic Pathways
Primary Exposure Routes
Food and beverage contamination has been reported across multiple matrices, including bottled water, seafood, and foods with high packaging contact.4-7
Thermal stress markedly increases microplastic release from plastics. In a widely cited experimental study, standard infant formula preparation with polypropylene bottles generated microplastic particles in the prepared liquid, raising concern for exposure during sensitive developmental windows.3,8
Airborne microplastic fibers are present in indoor dust and can be inhaled, with subsequent swallowing through mucociliary clearance; occupational settings may substantially increase inhalational burden.9-13
Biokinetics and Translocation
Translocation across mucosal barriers appears to be size- and surface-dependent. Experimental work suggests that smaller particles can be taken up by M cells in Peyer’s patches, phagocytosed by immune cells, or cross a disrupted epithelial barrier.14-18
Once systemically available, polymers have been reported in blood 19 and in multiple tissues including placenta, atherosclerotic plaques, liver, brain, and testes.20-24
Vulnerable Populations and High-Exposure Contexts
Placental detection studies indicate that microplastic polymers can be present in placental tissue,20,25 and observational studies suggest associations between placental polymer burden and preterm birth or birth weight,26,27 though confounding and exposure misclassification remain important concerns.
The notion of a safe threshold remains premature. Even when emission rates are high in specific contexts (eg, infant formula preparation), the fraction that reaches systemic circulation is unknown. 11
Ingestion dominates exposure, with contributions from food contact materials, bottled water, and infant formula preparation. 3 Inhalation contributes via indoor dust and microplastic fibers, with subsequent swallowing of cleared particles.9,10 Dermal exposure appears minor for intact skin but may increase with cosmetics or occupational contact.
Tissue Detection and Analytical Considerations
A recurring challenge is that tissue “burden” is measured using different analytical paradigms. Spectroscopic approaches (eg, μFTIR/Raman) tend to report particle counts and size distributions, often with lower size cutoffs that can miss smaller microplastics and nanoplastics, whereas pyrolysis-GC/MS quantifies total polymer mass without resolving particle number or morphology. These are not interchangeable metrics.
Contamination control (airborne fibers, lab plastics, procedural blanks), limits of detection, and the choice of digestion protocols can materially influence results. Even in high-quality human tissue studies, measured concentrations may approach detection thresholds, and blank correction can shift findings. 23
For this reason, absolute values should be interpreted as “reported in a specific analytical context” rather than as directly comparable concentrations across studies or organs.
Particles that translocate to lymph or blood may be distributed systemically and potentially deposited in tissues, depending on size, surface properties, and protein corona formation. 17
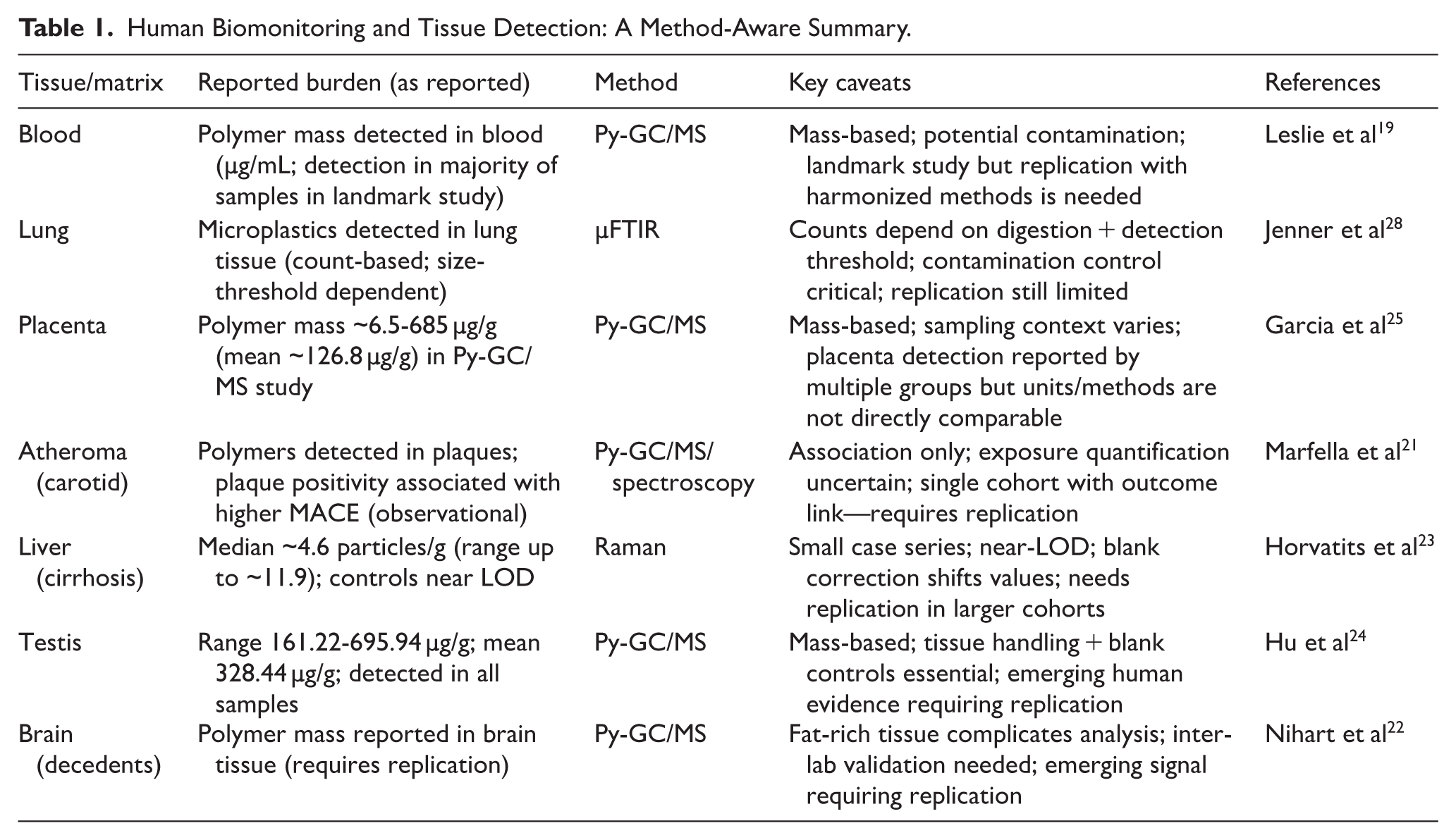
Despite these limitations, converging evidence supports internal exposure. Polymer detection in human placenta has been reported by multiple groups using both spectroscopic and mass-based approaches,20,25,27 and polymers have also been reported in blood, 19 lung tissue, 28 and male reproductive samples.24,29 Findings linking plaque polymer positivity to subsequent cardiovascular events 21 and polymer mass detection in decedent human brain tissue 22 are especially influential but currently rest on a limited number of studies; they should therefore be considered emerging signals requiring independent replication and harmonized analytical standards.
Health Outcomes: What is Known Versus What is Suggested
Cardiovascular Outcomes
The most prominent human outcome signal currently comes from a single observational cohort of patients undergoing carotid endarterectomy, in which detection of micro- and nanoplastics in plaques was associated with higher rates of subsequent major adverse cardiovascular events over follow-up. 21
Although this association is clinically concerning, the study does not establish causation and may be affected by residual confounding, exposure misclassification, and analytical heterogeneity. It should therefore be interpreted as hypothesis-generating; independent replication and mechanistic follow-up are needed, particularly around inflammation, endothelial dysfunction, and plaque instability pathways. 21
Reproductive and Developmental Outcomes
Microplastics have been detected in human semen and testes, supporting the plausibility of exposure to the male reproductive system; however, these human observations remain relatively limited and should be considered emerging until replicated across laboratories and populations.24,29 Recent reviews synthesize a broader preclinical literature suggesting possible sperm and reproductive effects, but causal inference in humans remains limited.30,31
In a Toxicological Sciences study using Py-GC/MS, microplastics were detected in all human testes analyzed, with substantial inter-individual variability. Associations with reproductive parameters were explored in canine samples as a bioindicator model, but such correlations do not imply causation. 24
For pregnancy outcomes, polymer mass has been quantified in placental specimens, and several studies suggest associations with fetal growth parameters; however, these findings are largely observational and require careful control for socioeconomic and environmental confounders.25-27
Neurological Outcomes
Neurobiological concern is driven by (i) experimental evidence that small particles may cross barriers under certain conditions18,32 and (ii) recent human autopsy findings reporting polymer mass in brain tissue. 22 These brain findings are early-stage and currently rely on limited datasets, with important analytical challenges in fatty tissues.
At present, the neurological evidence should be treated as hypothesis-generating rather than definitive evidence of neurodegenerative causation; replication across laboratories and longitudinal human studies linking standardized exposure metrics to cognitive outcomes are priorities.
Dose-Response Uncertainty and Exposure Thresholds
Across outcome domains, a central barrier to clinical risk assessment is the absence of validated dose-response relationships. Intake estimates vary widely (sometimes summarized as grams per week) depending on assumptions about particle size distributions, polymer densities, and sampling matrices. 33 Biomonitoring studies typically provide a single-timepoint measurement in 1 tissue, using either particle counts or polymer mass, making it difficult to reconstruct cumulative exposure or compare across cohorts.
Consequently, no consensus exposure thresholds or clinically actionable “internal burden” cutoffs exist. Risk likely depends not only on total mass or number but also on particle size (nano vs micro), shape (fibers vs fragments), polymer chemistry, and associated additives or sorbed persistent contaminants (eg, PFAS).16,17,34 Until standardized assays and longitudinal dose-response data are available, counseling should prioritize exposure reduction and established cardiometabolic risk reduction rather than numeric microplastic targets.
Elimination Pathways and the Limits of Current Evidence
The natural history of microplastic elimination in humans is not well quantified. It is likely that most larger particles are not absorbed and are eliminated in stool, consistent with stool detection studies and with size constraints on epithelial translocation.16,17
For smaller particles, animal studies using uniform microspheres suggest hepatic uptake and potential hepatobiliary handling, but translating such controlled pharmacokinetic models to heterogeneous environmental MPs/NPs in humans is uncertain.17,35
Accordingly, statements about fixed percentages of biliary excretion or fecal removal should be avoided; current evidence supports plausible pathways but not human quantitative clearance rates.
Nutrition and Lifestyle: A Responsible Mitigation Hierarchy
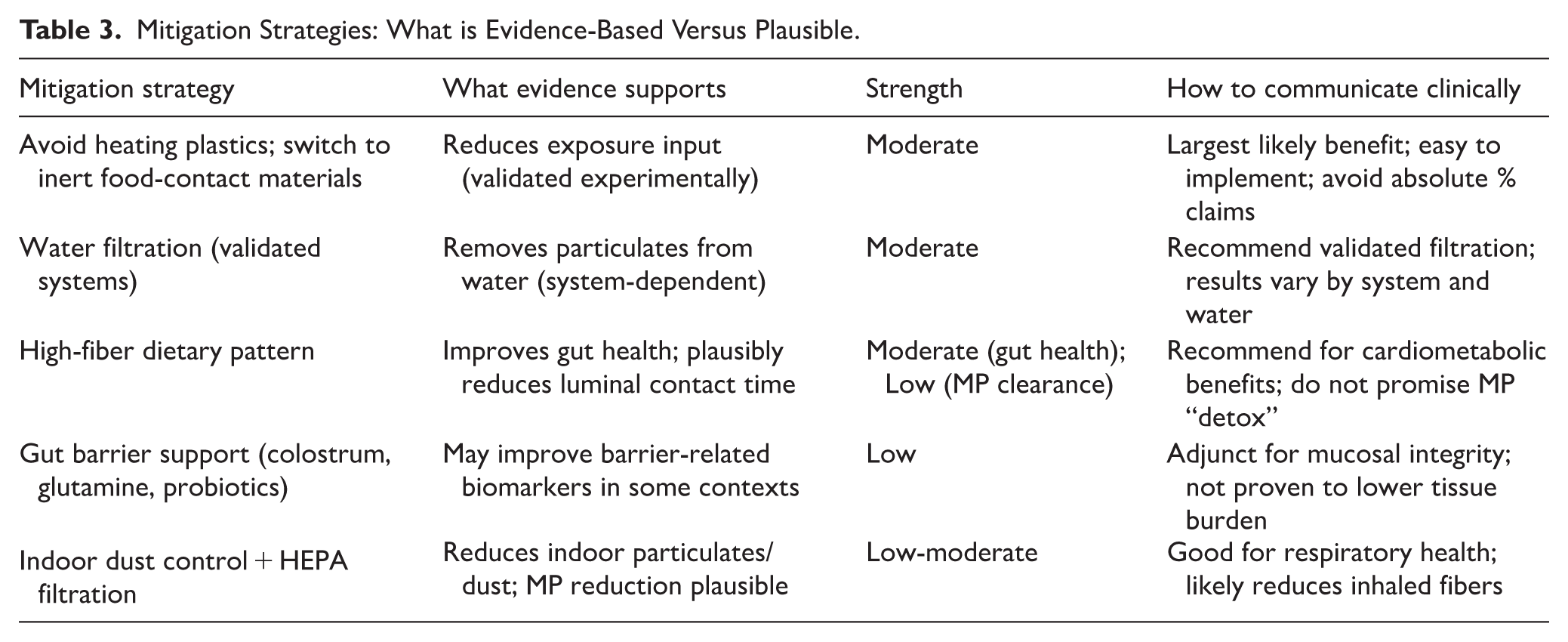
Given evidentiary uncertainty, mitigation should follow a hierarchy: first reduce exposure input, then reduce opportunities for translocation (barrier integrity and transit time), and finally address downstream oxidative/inflammatory effects. This hierarchy is more defensible than promoting unproven “detoxification” protocols. 36
Exposure Reduction (Highest-Confidence Lever)
Prefer glass, stainless steel, or ceramic for food storage and hot foods; avoid microwaving or heating food in plastic containers.
Reduce reliance on bottled water and consider filtration approaches that are validated for particulate reduction (performance varies by system and local water characteristics).
Minimize contact between fatty/hot foods and plastic packaging when feasible, as these conditions can increase additive migration and particle shedding.
Reduce indoor dust load (wet dusting, vacuuming with HEPA filtration) and improve ventilation to lower airborne fiber exposure.
Dietary Fiber, Bile Acids, and the Enterohepatic Axis
Dietary fiber is a low-risk intervention with multiple established metabolic benefits. In the context of MPs/NPs, fiber may reduce luminal residence time, increase stool bulk, and potentially entrap particulates within the gut matrix, thereby reducing contact with the epithelium. Direct human evidence that fiber increases microplastic excretion is not yet available.37,38
The bile acid pool is clinically relevant because bile mediates fecal excretion of many lipophilic compounds. The notion of “biliary sequestration” of microplastics remains speculative: bile acid sequestrants (eg, cholestyramine, colesevelam) are proven to bind bile acids and can reduce enterohepatic recirculation of some chemicals, but binding and elimination of plastic particles in humans has not been demonstrated.
Choleretic botanicals (eg, artichoke leaf, dandelion) can increase bile flow in animal models; this may support lipid digestion but should not be presented as evidence-based microplastic detoxification.39,40 More broadly, polyphenol-rich foods and supplements (eg, green tea catechins, citrus flavonoids such as naringin, and resveratrol) have evidence for modulating oxidative stress and inflammatory markers, but they have not been tested for reducing MP/NP burden in humans.41-44
Strengthening the Gut Mucosal Barrier: Colostrum, Glutamine, and Probiotics
A more evidence-aligned nutritional angle is to treat the intestinal barrier as a modulator of translocation risk. Increased permeability (“leaky gut”) is associated with metabolic inflammation, and experimental work suggests that barrier disruption may facilitate uptake of small particles. 23
Colostrum contains immunoglobulins and growth factors that may support mucosal repair; glutamine is a primary fuel for enterocytes; and selected probiotics can improve barrier-related biomarkers in certain gastrointestinal contexts. These interventions may plausibly reduce the probability of translocation, but they have not been shown to reduce human tissue microplastic burden.
Where supplements are considered, the clinical framing should be: supportive of mucosal integrity and inflammation control, not detoxification of plastics. Safety, contraindications, and product quality variation should be emphasized.
Microbiome Modulation and Fermented Foods
Probiotics have attracted attention because some strains can adsorb microplastics in vitro and improve gut outcomes in animal models. A recent preclinical study reported enhanced fecal excretion and reduced intestinal accumulation in vivo using selected strains, but human efficacy remains unknown. 45
Fermented foods may improve microbiome diversity and barrier function; small clinical trials in other diseases (eg, kefir in inflammatory bowel disease) show effects on symptoms and microbiota, but do not address microplastic clearance. 46
What We Should Not Claim as “Microplastic Detox” (Yet)
Popular “detox” approaches such as sauna, sweating protocols, or fasting-induced autophagy should be discussed with restraint. Sweat studies demonstrating elimination of certain plastic-associated chemicals (eg, BPA) cannot be generalized to elimination of plastic particles, and autophagy markers do not demonstrate clearance of exogenous polymers.47-49
At present, the most defensible clinical recommendation is exposure reduction coupled with general cardiometabolic and gut-health optimization, pending definitive human clearance studies and intervention trials.
What This Review Adds: Standardization and Testable Clinical Questions
A useful way forward is to treat MPs/NPs as a measurable internal exposure marker and to standardize a minimal reporting set: polymer identification method, procedural blank correction, size distribution (where applicable), reporting units (mass vs count), and sampling/handling protocols. Without this, the field cannot build reliable dose-response models or compare interventions.
We further propose that nutrition research prioritize 3 testable questions: (1) does increased dietary fiber reduce stool microplastic counts or polymer mass?, (2) do barrier-support interventions reduce circulating polymer detection in blood?, and (3) do exposure-reduction bundles measurably reduce internal biomarkers over time? These are feasible trial designs that would materially advance clinical guidance.
Conclusion
Micro- and nanoplastics are increasingly reported in human tissues, confirming internal exposure. The best available clinical evidence suggests potential associations with cardiovascular events and reproductive parameters, but causality remains unproven for most outcomes.
Nutritional strategies should be presented as risk-mitigation and barrier-support tools rather than detoxification therapies. Until standardized biomonitoring and interventional trials mature, clinicians should emphasize exposure reduction, dietary patterns that support gut integrity (fiber-rich, minimally packaged foods), and cautious interpretation of emerging biomonitoring studies. Upstream policy and systems interventions to reduce plastic inputs—alongside individual-level exposure reduction—are likely required to meaningfully lower population-level burden (Tables 1-3).36,50
Human Biomonitoring and Tissue Detection: A Method-Aware Summary.
Evidence Certainty Map (Corrected GRADE Framing).
Mitigation Strategies: What is Evidence-Based Versus Plausible.
Footnotes
Author Contributions
Conceptualization, S.A. and K.S.; methodology, S.A. and K.S.; validation, S.A.; formal analysis, S.A.; investigation, S.A.; data curation, S.A.; writing—original draft preparation, S.A.; writing—review and editing, K.S.; visualization, K.S.; supervision, K.S.; project administration, K.S; revising and responding to reviewer concerns, M.A. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.