
Abstract
The kynurenine pathway (KP), the primary route of tryptophan (TRP) metabolism, is influenced by inflammation and hypoxia and has been linked to immune dysregulation and oxidative stress. This study investigated the relationship between KP activity and hypoxia in periodontal inflammation, as well as their association with clinical periodontal parameters. A total of 23 systemically healthy patients with stage III, grade B periodontitis and 22 periodontally healthy individuals were included. Salivary and serum levels of tumor necrosis factor-alpha (TNF-α), hypoxia-inducible factor-1 alpha (HIF-1α), and 8-hydroxy-2′-deoxyguanosine (8-OHdG) were measured using ELISA. KP metabolites were analyzed via liquid chromatography-mass spectrometry. Results showed that salivary TNF-α, HIF-1α, and 8-OHdG levels were significantly higher in the periodontitis group (P < .05). Both salivary and serum kynurenine/tryptophan (KYN/TRP) ratios and picolinic acid (PA), along with salivary 3-hydroxykynurenine (3OHKYN) and serum kynurenine (KYN), were elevated in periodontitis (P < .05). In contrast, TRP levels in both saliva and serum were significantly reduced (P < .001). Correlation analyses revealed that TRP levels were negatively associated with periodontal disease severity, whereas the salivary KYN/TRP ratio, 3OHKYN, HIF-1α, 8-OHdG, and TNF-α were positively associated (P < .05). Strong correlations were observed between the saliva and serum compartments, with a strong positive relationship between salivary and serum TRP and a moderate correlation for the KYN/TRP ratios. Multivariate logistic regression identified salivary KYN/TRP ratio and HIF-1α as independent predictors of periodontitis after adjusting for age and gender, with male gender also emerging as a significant factor (P < .05). Overall, the findings suggest that KP alterations, hypoxia, and oxidative stress are closely interconnected in periodontal inflammation. However, due to the cross-sectional design, these associations should not be interpreted as causal. The KP and hypoxia pathways may serve as potential non-invasive biomarkers for periodontitis.
Introduction
Hypoxia, a defining feature of inflamed and diseased tissues, 1 plays a central role in driving chronic inflammation. Characterized by reduced oxygen availability, hypoxia activates cellular adaptation mechanisms primarily through hypoxia-inducible factor-1 alpha (HIF-1α). 2 HIF-1α regulates critical responses, including angiogenesis, metabolic reprograming, and immune signaling, all of which are aimed at preserving tissue homeostasis under stress. 3 Under persistent hypoxic conditions, the expression of pro-inflammatory mediators such as tumor necrosis factor-alpha (TNF-α) 4 and vascular endothelial growth factor5,6 is significantly upregulated. These cytokines sustain inflammation, leading to progressive tissue destruction and the maintenance of a hypoxic microenvironment, creating a self-perpetuating cycle of inflammation and tissue injury.7,8 This mechanism is particularly relevant in periodontitis, where unresolved inflammation and hypoxia converge to accelerate periodontal breakdown. 9
One of the key downstream consequences of hypoxia and inflammation is the activation of the kynurenine pathway (KP), the major route of tryptophan (TRP) catabolism. 10 TRP is metabolized to kynurenine (KYN) by enzymes such as indoleamine 2,3-dioxygenase (IDO1/IDO2) and tryptophan 2,3-dioxygenase (TDO). 11 These enzymes are differentially expressed, with IDO1 present in most tissues and TDO primarily in the liver. 12 Pro-inflammatory cytokines, particularly interferon-gamma (IFN-γ) and TNF-α, strongly induce IDO1 expression during inflammation.13,14 As a result, TRP metabolism shifts toward KP, leading to the accumulation of biologically active metabolites, including KYN, kynurenic acid (KYNA), 3-hydroxykynurenine (3OHKYN), picolinic acid (PA), and quinolinic acid (QA).15,16 Each of these metabolites exerts specific, diverse effects on immune regulation, oxidative stress, and tissue integrity. Oxidative stress is a key mechanistic link between KP overactivation and tissue destruction in chronic inflammatory conditions. 16 Pro-oxidant metabolites, such as 3OHKYN and QA, enhance the production of reactive oxygen species (ROS), thereby promoting oxidative damage and further amplifying inflammation.17,18 Although KYNA may offer antioxidant and immunomodulatory effects, 19 this protective balance is often lost in disease states. In periodontitis, the accumulation of oxidative KP metabolites may intensify connective tissue degradation and bone loss, accelerating disease progression. Notably, pharmacological modulation of KP activity has shown therapeutic potential in a range of inflammation-associated disorders, including autoimmune and metabolic diseases.20-22 However, the precise molecular mechanisms linking chronic inflammation, KP dysregulation, oxidative stress, and progressive tissue damage remain incompletely understood.
Although previous studies have identified associations between KP metabolites and systemic diseases,23-26 the specific role of KP metabolites in oral inflammatory conditions remains less well characterized. Our prior research demonstrated significant correlations between KP metabolite levels and clinical periodontal parameters, suggesting a role for the pathway in disease severity and progression.27,28 Yet, the interconnected roles of hypoxia, KP activation, and oxidative stress in periodontitis have not been comprehensively investigated. Therefore, the aim of this study is to investigate the potential interplay between hypoxia, KP activation, and oxidative stress in the pathogenesis of periodontitis by exploring their associations with clinical periodontal parameters in patients with generalized Stage III periodontitis.
Materials and Methods
Study Population and Design
This cross-sectional study comprised 23 patients with generalized periodontitis (P group; n = 23; Stage III, Grade B; female = 9, male = 14; mean age: 41.39 ± 7.13 years) and 22 periodontally healthy control subjects (C group; n = 22; female = 14, male = 8; mean age: 40.05 ± 7.00 years). The study was carried out at the Department of Periodontology, Faculty of Dentistry, Istanbul Medipol University, between January 2023 and January 2024. The study’s design and implementation received approval from the Istanbul Medipol University Human Research Ethics Committee (No: E-10840098-772.02-7723, dated December 23, 2022). The study protocol was retrospectively approved by ClinicalTrials.gov (NCT07187323) on September 22, 2025. The research adhered to the principles outlined in the Declaration of Helsinki, as revised in 2013. Before participation, all individuals who agreed to be part of the study provided formal informed consent by signing a consent form.
A comprehensive periodontal evaluation was conducted, which included radiographic imaging and clinical assessment. Specifically, probing depth (PD), plaque index (PI), bleeding on probing (BOP), and clinical attachment loss (CAL) were documented during clinical assessment. Participants who had at least 20 natural teeth were included. The clinical diagnosis of patients’ periodontal status was categorized according to the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. 29 The exclusion criteria were (1) being under 18 and over 65 years of age; (2) having a diagnosis of diabetes, cancer, cardiovascular diseases, and/or any autoimmune diseases such as rheumatoid arthritis; (3) being pregnant or breastfeeding; (4) smoking; (5) using antibiotics, anti-inflammatory medications, immunosuppressive drugs, or contraceptives within the past 3 months; (6) receiving periodontal treatment within the past 6 months.
Saliva and Serum Sampling
Unstimulated saliva samples were collected from each patient after the protocol was explained in detail. Initially, patients were instructed to rinse their mouths thoroughly with filtered water and sit calmly while they spat into a disposable tube for 5 minutes. After centrifugation of the samples at 3000× g for 10 minutes, they were transferred into Eppendorf tubes. 30
Standard venipunctures were used to collect blood, and serum was prepared from the blood samples by centrifugation at 4000× g for 10 minutes, then transferred into Eppendorf tubes. All serum and saliva samples have been preserved at −80°C.
Determination of Salivary and Serum TNF-α, HIF-1α, and 8-OHdG Levels
Levels of the TNF-α, HIF-1α, and 8-hydroxy-2′-deoxyguanosine (8-OHdG) in saliva and serum samples were measured using a commercial ELISA kit (USCN, Cloud-Clone Corp, USA) according to instructions provided by the manufacturer. The standard curve of the assay was used to determine the analyte concentrations in each sample. The assay’s intra- and inter-assay precision values were 10% and 12%, respectively. The detection range of the commercial kit for TNF-α, HIF-1α, and 8-OHdG quantification was specified as 7.8-500 pg/mL, 0.156-10 ng/mL, and 74.07-6000 pg/mL, respectively. All samples were analyzed twice, and the mean values were used for subsequent calculations.
Determination of Salivary and Serum TRP, KYN, and KYN Metabolites’ Levels
TRP, KYN, and KYN metabolites were analyzed by liquid chromatography-mass spectrometry (LC-MS/MS) in accordance with our previous article. 27 The method is described in detail in our article, 27 where we utilize a modified version of the method described by Tömösi et al. 31
Statistical Analysis
A priori sample size analysis was conducted using specialized software (3.1.9.2 G*Power; https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-undarbeitspsychologie/gpower.html). Using a large effect size (Cohen’s d = 1.39) for 2 groups, based on differences in the KYN/TRP ratio reported by Kurgan et al, 27 a .05 α-error, and 95% power, the required total sample size was calculated as 30 participants (n = 15 per group). To account for potential confounding factors and possible incomplete data collection, the target sample size was set higher than the minimum requirement.
Statistical software (SPSS for Windows v.26, IBM SPSS Inc., New York, NY, USA), which is commercially available, was used for all analyses. Data normality was assessed using the Shapiro–Wilk test. Normally distributed data were evaluated using the Student’s t-test, and non-normally distributed data were evaluated using the Mann-Whitney U test. The χ2 test was used for intergroup comparison of the gender variable. To identify relationships between biochemical and periodontal clinical data, Spearman correlation analysis was employed. A significant level of .05 was used for all tests.
Results
Study Population and Periodontal Clinical Parameters
A total of 92 individuals were evaluated for this study. Among the 57 patients diagnosed with periodontitis, 4 declined to participate, 9 were excluded due to recent antibiotic use, 7 were excluded due to recent periodontal therapy, and 14 were excluded for having systemic diseases. This resulted in a final sample of 23 patients with stage III grade B generalized periodontitis. Similarly, of the 35 individuals identified as periodontally healthy, 5 were excluded due to recent antibiotic use, and 8 were excluded because they had systemic diseases, leaving 22 periodontally healthy controls (Figure 1).
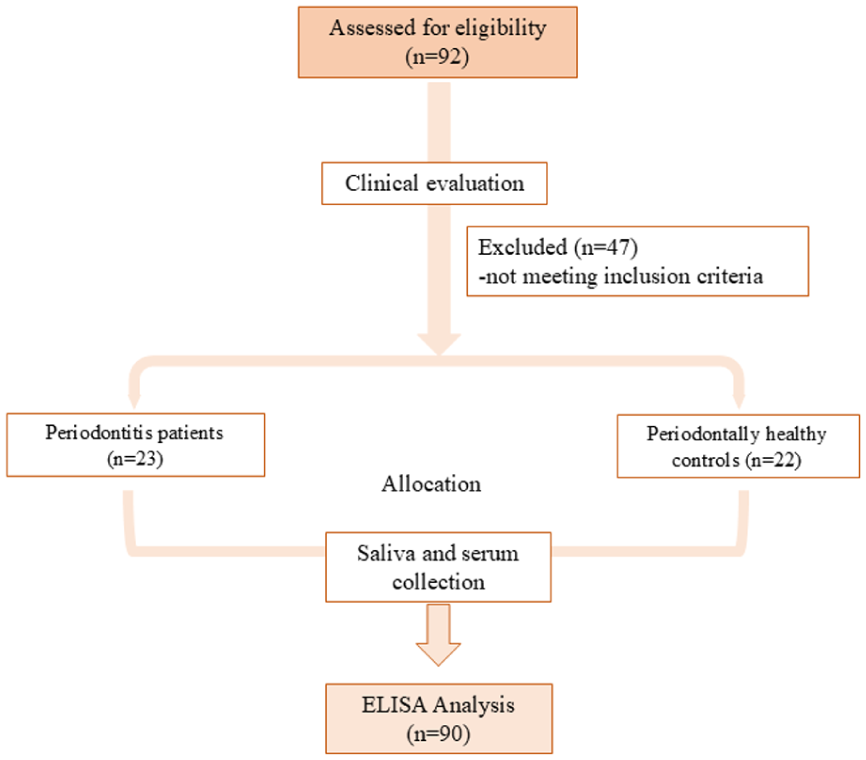
Flowchart and study protocol.
Twenty-three periodontitis patients (9 females, 14 males, and mean age: 41.39 ± 7.13 years) and 22 periodontally healthy control individuals (14 females, 8 males, and mean age: 40.05 ± 7.00 years) completed all procedures. There were no significant differences between groups in terms of age (P = .527) or sex distribution (P = .100; Table 1).
Intergroup Comparison of Demographic and Clinical Parameters.
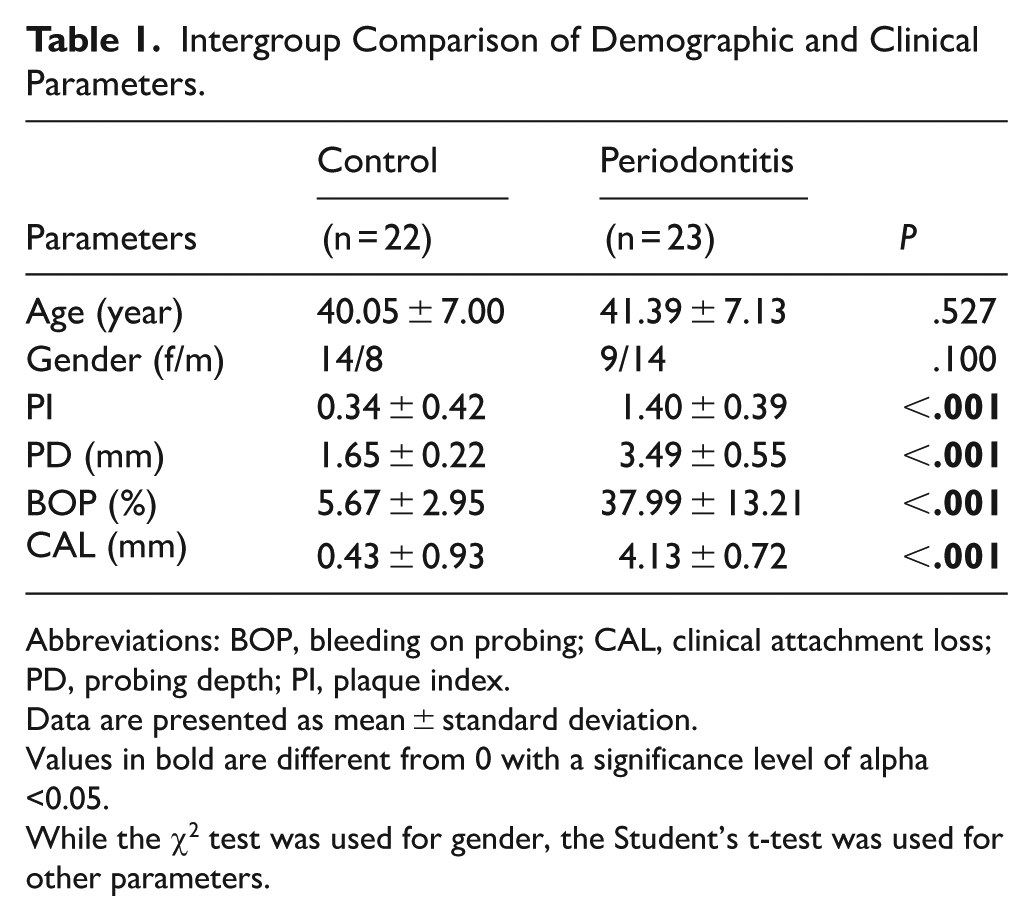
Abbreviations: BOP, bleeding on probing; CAL, clinical attachment loss; PD, probing depth; PI, plaque index.
Data are presented as mean ± standard deviation.
Values in bold are different from 0 with a significance level of alpha <0.05.
While the χ2 test was used for gender, the Student’s t-test was used for other parameters.
All clinical periodontal parameters (PI, PD, BOP, and CAL) were significantly higher in the periodontitis group compared to the control group (P < .001; Table 1).
Biochemical Parameters
Salivary and serum levels of TNF-α, HIF-1α, 8-OHdG, TRP, KYN, and KYN metabolites are presented in Figure 2. Salivary TNF-α, HIF-1α, and 8-OHdG levels were significantly higher in the periodontitis group than in the control group (P = .020, P < .001, and P = .001, respectively). Additionally, salivary and serum KYN/TRP ratio and PA, salivary 3OHKYN, and serum KYN levels were statistically significantly higher in the periodontitis group than in the control group (P < .001, P < .001, P = .012, P < .001, P = .002, P = .002, P = .002, and P = .031, respectively). In contrast, salivary and serum TRP levels were significantly lower in the periodontitis group compared to the control group (P < .001).
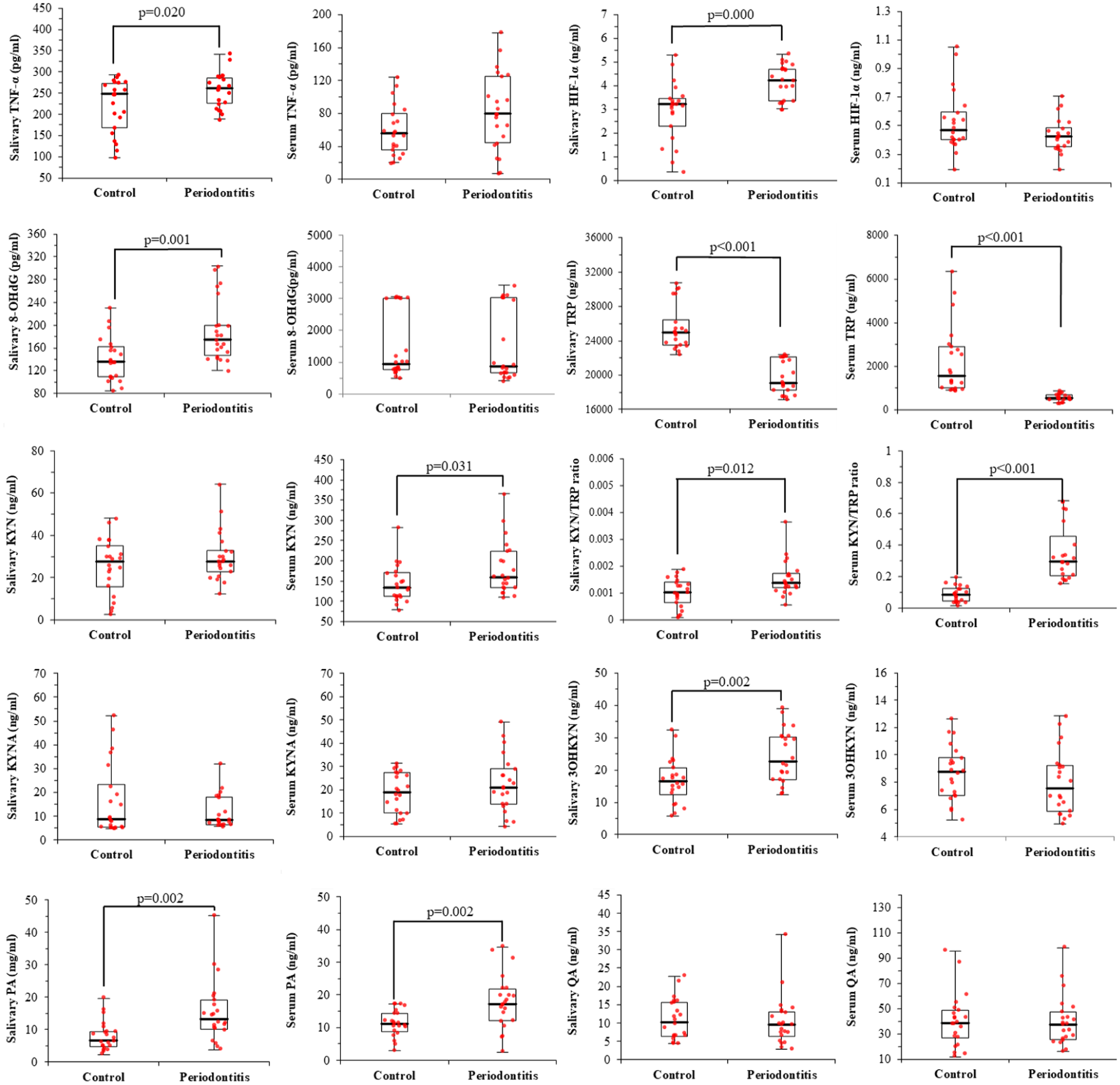
Intergroup comparison of serum and saliva biomarker levels.
Correlations Between Clinical Periodontal and Biochemical Parameters
Data from all 45 individuals were included in the analysis. Correlation analyses revealed distinct but interconnected patterns within salivary and serum compartments, as well as between them (Table 2).
Correlation of the Clinical Parameters and Salivary and Serum Levels of Biomarkers.
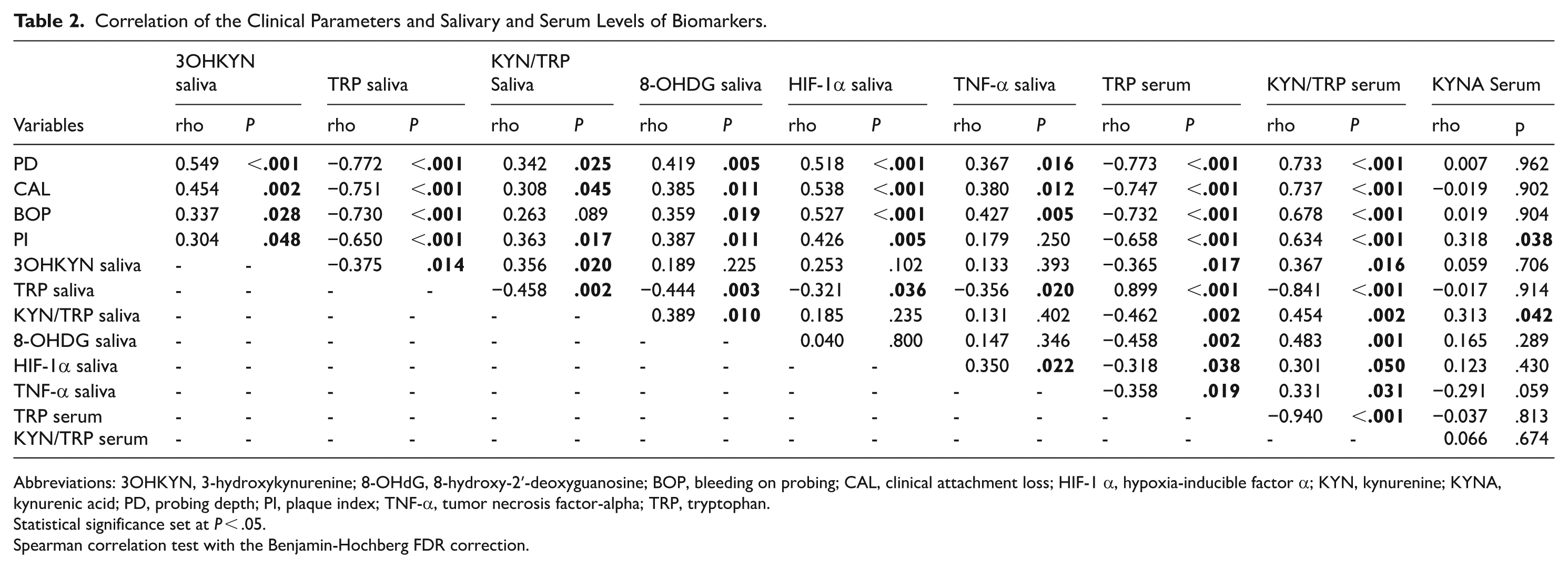
Abbreviations: 3OHKYN, 3-hydroxykynurenine; 8-OHdG, 8-hydroxy-2′-deoxyguanosine; BOP, bleeding on probing; CAL, clinical attachment loss; HIF-1 α, hypoxia-inducible factor α; KYN, kynurenine; KYNA, kynurenic acid; PD, probing depth; PI, plaque index; TNF-α, tumor necrosis factor-alpha; TRP, tryptophan.
Statistical significance set at P < .05.
Spearman correlation test with the Benjamin-Hochberg FDR correction.
Within saliva, TRP demonstrated strong negative correlations with all clinical periodontal parameters, including PD (r = −.772, P < .001), CAL (r = −.751, P < .001), BOP (r = −.730, P < .001), and PI (r = −.650, P < .001). In contrast, salivary 3OHKYN was positively correlated with PD (r = .549, P < .001), CAL (r = .454, P = .002), BOP (r = .337, P = .028), and PI (r = .304, P = .048). Similarly, salivary KYN/TRP ratio showed positive correlations with PD (r = .342, P = .025), CAL (r = .308, P = .045), and PI (r = .363, P = .017), while its association with BOP (r = .263, P = .089) was insignificant.
Salivary 8-OHdG was positively correlated with PD (r = .419, P = .005), CAL (r = .385, P = .011), BOP (r = .359, P = .019), and PI (r = .387, P = .011), while salivary HIF-1α showed positive correlations with PD (r = .518, P < .001), CAL (r = .538, P < .001), BOP (r = .527, P < .001), and PI (r = .426, P = .005). Salivary TNF-α was positively correlated with PD (r = .367, P = .016), CAL (r = .380, P = .012), and BOP (r = .427, P = .005), but not with PI (r = .179, P = .250).
In addition to clinical associations, strong intra-salivary relationships were observed. Salivary TRP was negatively correlated with KYN/TRP (r = −.458, P = .002), 8-OHdG (r = −.444, P = .003), HIF-1α (r = −.321, P = .036), and TNF-α (r = −.356, P = .020). Salivary 3OHKYN showed a negative correlation with salivary TRP (r = −.375, P = .014) and a positive correlation with KYN/TRP (r = .356, P = .020). Salivary 8-OHdG was positively correlated with salivary KYN/TRP (r = .389, P = .010) and negatively correlated with TRP (r = −.444, P = .003) and KYNA (r = −.321, P < .05). Furthermore, salivary TNF-α was positively correlated with HIF-1α (r = .350, P = .022).
Within serum, TRP was negatively correlated with PD (r = −.773, P < .001), CAL (r = −.747, P < .001), BOP (r = −.732, P < .001), and PI (r = −.658, P < .001). In contrast, serum KYN/TRP ratio showed strong positive correlations with PD (r = .733, P < .001), CAL (r = .737, P < .001), BOP (r = .678, P < .001), and PI (r = .634, P < .001). Serum KYNA did not show significant correlations with PD (r = .007, P = .962), CAL (r = −.019, P = .902), or BOP (r = .019, P = .904), but demonstrated a weak positive correlation with PI (r = .318, P = .038).
Strong intra-serum relationships were also identified. Serum TRP was strongly negatively correlated with serum KYN/TRP ratio (r = −.940, P < .001), while no significant correlation was observed between serum KYN/TRP ratio and KYNA (r = .066, P = .674).
Direct comparisons between saliva and serum for the same analytes demonstrated significant concordance. Salivary and serum TRP levels were strongly positively correlated (r = .899, P < .001). Similarly, salivary and serum KYN/TRP ratios showed a moderate positive correlation (r = .454, P = .002). No significant saliva-serum correlations were observed by other analytes.
Logistic Regression Analysis of Risk Factors for Periodontitis
Variables that were statistically significant in the univariate analysis were included in a multivariate logistic regression model to identify independent risk factors for periodontitis (Table 3).
Logistic Regression Analysis Results Between Periodontitis and Control Groups.
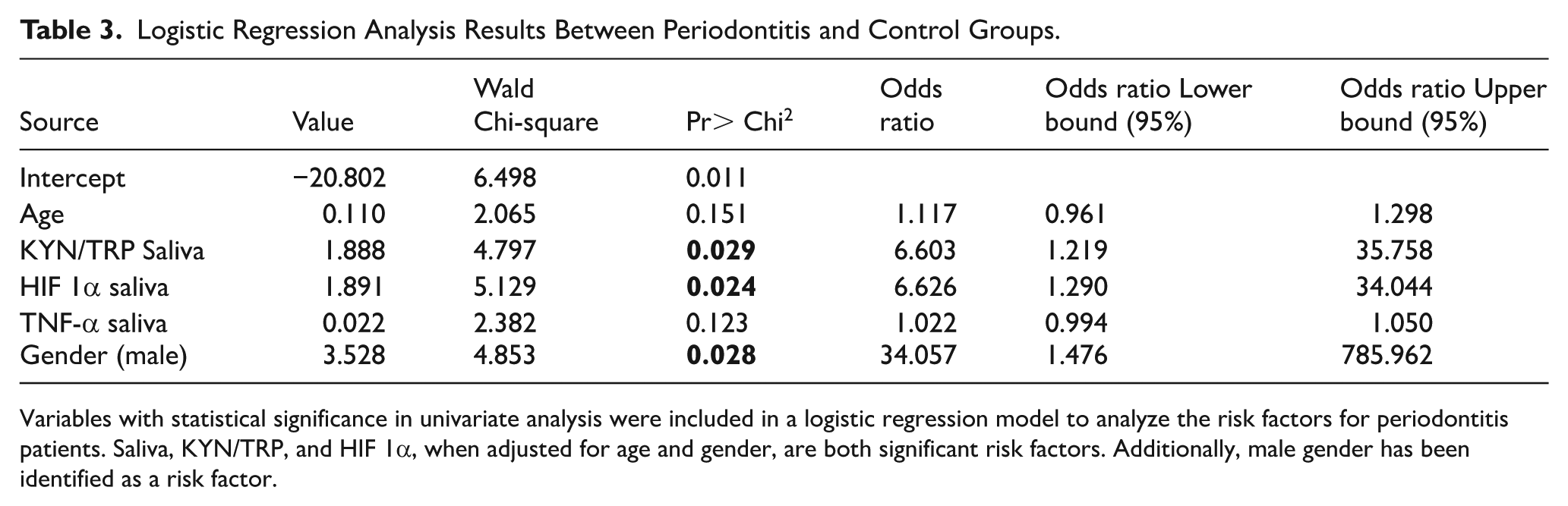
Variables with statistical significance in univariate analysis were included in a logistic regression model to analyze the risk factors for periodontitis patients. Saliva, KYN/TRP, and HIF 1α, when adjusted for age and gender, are both significant risk factors. Additionally, male gender has been identified as a risk factor.
The model revealed that salivary KYN/TRP ratio and salivary HIF-1α levels were independently associated with periodontitis after adjustment for age and gender. Specifically, salivary KYN/TRP ratio showed a significant effect (β = 1.888, Wald χ2 = 4.797, P = .029), corresponding to an odds ratio (OR) of 6.603 (95% CI: 1.219-35.758). Similarly, salivary HIF-1α was identified as a significant predictor (β = 1.891, Wald χ2 = 5.129, P = .024), with an OR of 6.626 (95% CI: 1.290-34.044), indicating that higher levels of this marker were associated with markedly higher odds of periodontitis.
Gender also emerged as a significant factor in the model. Male individuals had significantly higher odds of periodontitis than females (β = 3.528, Wald χ2 = 4.853, P = .028), with an OR of 34.057 (95% CI: 1.476-785.962).
In contrast, age (β = .110, Wald χ2 = 2.065, P = .151; OR = 1.117, 95% CI: 0.961-1.298) and salivary TNF-α (β = .022, Wald χ2 = 2.382, P = .123; OR = 1.022, 95% CI: 0.994-1.050) were not statistically significant predictors in the adjusted model.
The intercept of the model was statistically significant (β = −20.802, Wald χ2 = 6.498, P = .011), indicating the model’s overall validity.
Overall, these findings demonstrate that the salivary KYN/TRP ratio and HIF-1α are independent biochemical risk factors for periodontitis, whereas male sex is a strong demographic risk factor, independent of age.
Discussion
The KP, the principal route for TRP degradation, is activated during inflammation and immune responses through the upregulation of IDO. 32 Hypoxia, a hallmark of inflamed tissues, further amplifies KP activity by inducing the expression of inflammatory mediators and altering metabolic conditions in favor of TRP catabolism. 16 While our previous studies identified the role of the KP in periodontal disease pathogenesis,27,28 to date, no study has comprehensively investigated the interaction among hypoxia, the KP, and oxidative stress in the context of periodontal inflammation.
To address this gap, we investigated the potential interplay between hypoxia and KP activation by analyzing the salivary and serum levels of TRP, KYN, and their metabolites, as well as HIF-1α, TNF-α, and 8-OHdG, in patients with Stage III periodontitis compared to periodontally healthy controls. Our findings revealed a consistent increase in the salivary and serum KYN/TRP ratios and PA, along with elevated salivary TNF-α, HIF-1α, 8-OHdG, and 3OHKYN, and elevated serum KYN levels in the periodontitis group. Conversely, TRP levels significantly decreased in both saliva and serum.
Correlation analyses demonstrated that TRP levels in both saliva and serum were strongly and consistently negatively associated with clinical periodontal parameters, whereas the salivary KYN/TRP ratio, 3OHKYN, HIF-1α, 8-OHdG, and TNF-α were positively associated with disease severity. These findings indicate a coordinated relationship between KP-related metabolic changes, oxidative stress, and periodontal inflammation, rather than a direct causal effect.
The observed TRP depletion and elevated KYN/TRP ratio are consistent with increased IDO activity, a feature also reported in systemic inflammatory diseases, including diabetes and cardiovascular disorders.33,34 TRP catabolism via the KP represents a metabolic adaptation to inflammation, in which its depletion suppresses T-cell proliferation and promotes activation of regulatory T cells, contributing to immune tolerance. 35 These mechanisms have also been described in HIV and systemic lupus erythematosus, where TRP reduction reflects chronic immune activation.36,37 In the context of periodontitis, TRP depletion may reflect the metabolic demands of chronic inflammation and may be associated with immune dysregulation and tissue breakdown.
It is essential to acknowledge that oral microbiota can impact local TRP metabolism. Certain bacteria can enzymatically convert TRP into indoles and KYNs, thereby modulating local KP activity. The elevated KYN/TRP ratios observed in both saliva and serum in this study support the notion of both systemic and localized KP activation, echoing patterns seen in lupus erythematosus and neurodegenerative conditions.38,39 The strong positive correlation between salivary and serum TRP levels, together with the moderate correlation in KYN/TRP ratios, suggests a systemic–local association in KP metabolism, rather than a direct mechanistic linkage.
Among the KP metabolites, 3OHKYN is recognized for its dual roles in immune modulation and oxidative stress. In our study, it was significantly elevated in saliva and positively correlated with clinical parameters, supporting its association with oxidative stress-related processes, including ROS generation, mitochondrial dysfunction, and apoptosis.40,41 The selective increase in saliva, rather than serum, suggests that localized inflammatory processes in periodontal tissue may be linked to its production. This finding underscores 3OHKYN’s potential contribution to the persistence of oxidative damage and chronic inflammation in periodontitis. QA, another pro-oxidant KP metabolite, has previously been associated with mitochondrial dysfunction and inflammatory tissue damage. 42 While QA was significantly elevated in periodontitis patients in our previous study, 27 no significant difference was observed here, suggesting a dose- or stage-dependent role. Similarly, KYNA, a metabolite with its antioxidant and neuroprotective properties, did not show significant differences between the groups. The lack of elevated KYNA levels, unlike our previous findings,27,28 may reflect variability in its immunomodulatory role, influenced by local inflammation or systemic regulation. This variability may reflect compensatory shifts in metabolic flux or differences in local versus systemic regulation of KYNA. Further studies exploring interactions among KP metabolites may better define KYNA’s role in the immunopathology of periodontal disease.
Importantly, PA was significantly elevated in both saliva and serum in the periodontitis group. PA has been implicated in macrophage activation, cytokine production, and the maintenance of chronic inflammation. 43 Its observed correlations with TNF-α and HIF-1α suggest an association with inflammatory signaling pathways in periodontitis, although causality cannot be inferred.
It is crucial to note that KP metabolites exhibit both pro-oxidant and antioxidant properties, with effects that are context-dependent. 44 Metabolites such as KYN, KYNA, anthranilic acid (AA), 3OHKYN, xanthurenic acid (XA), cinnabarinic acid (CA), 3-hydroxyanthranilic acid (3-HAA), and PA can play dual roles in either mitigating or amplifying oxidative damage. The outcome appears to depend on their local concentration, interaction with immune cells, and cellular redox environment. In diseases such as neurodegeneration, cancer, and chronic inflammation, this balance critically influences disease progression. In periodontitis, where oxidative stress and immune dysregulation are central features, these dynamic roles may determine whether KP activity contributes to tissue protection or destruction.
HIF-1α, a master regulator of the cellular response to hypoxia, 45 was significantly elevated in saliva and positively correlated with clinical parameters. This finding supports its localized role in the periodontal environment, reinforcing previous evidence that hypoxia is compartmentalized and more pronounced in inflamed gingival tissues. 46 Its association with the KYN/TRP ratio and TNF-α suggests a potential link between hypoxia, inflammation, and KP activity. However, these relationships should be interpreted as associative rather than causal. Given that HIF-1α can induce IDO expression, 2 this observation may indicate a possible interaction between hypoxia and KP regulation.
Oxidative stress, as assessed by elevated salivary 8-OHdG levels, was also strongly correlated with clinical periodontal parameters. 8-OHdG, a well-established marker of oxidative DNA damage, has been extensively linked to the destruction of periodontal tissue.47,48 Its association with KYN/TRP ratio and inverse relationship with TRP further support a link between oxidative stress and KP activity in periodontal inflammation. The lack of significant systemic changes suggests that oxidative damage is predominantly localized.
Consistent with this localized profile, TNF-α, a key inflammatory cytokine, was significantly elevated in saliva. TNF-α promotes immune cell recruitment and cytokine cascades, and its salivary levels correlated positively with both HIF-1α and 8-OHdG. These findings suggest that TNF-α plays a central role in amplifying hypoxia-driven oxidative damage and sustaining tissue-level inflammation. 49 Its localized activity may explain why systemic TNF-α levels were unchanged despite pronounced clinical inflammation.
Multivariate logistic regression analysis further demonstrated that salivary KYN/TRP ratio and HIF-1α were independently associated with periodontitis after adjustment for age and gender. While these markers may have potential as indicators of disease susceptibility, these findings should not be interpreted as evidence of causation.
Our correlation analysis further elucidates the interplay between metabolic, inflammatory, and oxidative stress markers and clinical outcomes in periodontitis. The significant negative correlations between salivary and serum TRP levels and clinical periodontal parameters highlight the pivotal role of TRP depletion in disease progression. Conversely, positive correlations between salivary HIF-1α, 8-OHdG, KYN/TRP ratio, PA, and 3OHKYN with clinical indices such as PD and CAL confirm their involvement in the tissue-destructive processes characteristic of advanced periodontitis. Notably, salivary 3OHKYN, a strong pro-oxidant, was significantly correlated with clinical parameters, supporting its function in sustaining local oxidative stress and immune dysregulation.
Together, these findings affirm that KP activation, hypoxia, and oxidative stress are closely associated processes in periodontitis. The observed correlations and regression analyses highlight their potential relevance in disease characterization; however, the cross-sectional design of this study precludes any causal inference.
However, this study has limitations. Its cross-sectional design does not allow the determination of temporal or causal relationships between KP activation and periodontal inflammation. Additionally, the sample size limits generalizability. Future longitudinal and mechanistic studies are needed to clarify whether these biomarkers play a causal role or represent downstream effects of periodontal disease. Furthermore, gingival crevicular fluid (GCF), a more site-specific fluid for periodontal biomarker analysis, was not evaluated. Nevertheless, saliva offers clinical practicality, 50 and the observed patterns strongly support the involvement of hypoxia and KP dysregulation in the pathogenesis of periodontal disease.
Conclusion
This study demonstrates that interconnected metabolic pathways, hypoxia, the KP, and oxidative stress are closely associated within the periodontal microenvironment and may contribute to inflammatory and tissue-destructive processes. TRP depletion, elevated KYN/TRP ratios, and increased levels of 3OHKYN, PA, and 8-OHdG were associated with disease severity, reflecting metabolic and oxidative alterations observed in periodontitis. HIF-1α was also associated with KP-related markers, suggesting a potential link between tissue hypoxia and KP activity. The dual role of KP metabolites, as both antioxidants and pro-oxidants, underscores their biological complexity and potential utility as biomarkers rather than definitive therapeutic targets at this stage. Importantly, given the cross-sectional design of this study, these findings should be interpreted as associative rather than causal. Future longitudinal and mechanistic studies, incorporating GCF and stratifying by disease stage, are warranted to further clarify these relationships and evaluate their potential for diagnostic or therapeutic applications in periodontitis.
Supplemental Material
sj-docx-1-try-10.1177_11786469261457028 – Supplemental material for Interaction of Hypoxia and Kynurenine Pathway in Periodontal Inflammation
Supplemental material, sj-docx-1-try-10.1177_11786469261457028 for Interaction of Hypoxia and Kynurenine Pathway in Periodontal Inflammation by Ardita Koci, Sivge Kurgan, Nur Balci, Zeliha Guney, Emrah Turkmen, Ceyhan C. Serdar, Muhittin A. Serdar and Elif Unsal in International Journal of Tryptophan Research
Footnotes
ORCID iDs
Ethical Considerations
This study was approved by the Human Research Ethics Committee of Ankara Medipol University (No: E-10840098-772.02-7723, dated December 23, 2022), and it was carried out in accordance with the Helsinki Declaration.
Consent to Participate
At the start of the trial, all participants provided written permission.
Author Contributions
All authors have made substantial contributions to the conception and design of the study. AK, SK, NB, ZG, CCS, MAS, and EU contributed to the conceptualization and methodology. AK, ZG, and ET performed investigation and data curation. AK, NB, ZG, and MAS carried out the formal analysis, with CCS and MAS providing software support. ZG was additionally responsible for validation and resources. SK and MAS contributed to visualization, while SK also handled funding acquisition and project administration. NB and ZG drafted the manuscript, and SK, MAS, and EU contributed to writing, review, and editing. SK and EU provided supervision. All authors critically revised the manuscript, approved the final version, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.