
Abstract
Background:
In recent years, musculoskeletal pain (MSP) has gained widespread attention globally and has become a significant public health issue affecting people of all ages, especially those affected by adolescence. Many musculoskeletal problems have a biomechanical origin, often linked to foot type and plantar pressure.
Objectives:
The aim of this study is to provide new insights into the multifactorial nature of MSP by exploring its associations with foot type, plantar pressure, physical activity, psychosocial factors, and daily living habits in adolescents.
Design:
A cross-sectional observational study was conducted among adolescents recruited from community and schools in Guangzhou, China
Methods:
Chi-square tests and logistic regression analysis were employed to investigate the associations between the prevalence of musculoskeletal pain and various factors, including foot type, plantar pressure, physical activity levels, psychosocial factors, study pressure and daily living habits like sleep duration, sleep quality, and screen time. Given the high prevalence and clinical relevance, we further analyzed factors associated with neck, back, and foot pain.
Results:
This study included 216 adolescents (15.83 ± 1.05 years). The analysis revealed that physical activity, sleep duration, and study pressure significantly associated with the incidence of neck pain. Emotional symptoms at the threshold or abnormal and poor sleep quality both associated with low back pain. Foot type and plantar pressure did not show statistical significance in association with overall musculoskeletal pain. However, when specific pain sites were examined, foot pain was significantly associated with maximum plantar pressure ⩾ 1000 N/dm2, average plantar pressure ⩾ 180 N, and flatfoot or high-arched foot.
Conclusions:
Our study found that while foot type and plantar pressure were not associated with overall musculoskeletal pain, they were significantly associated with foot pain specifically. Low physical activity, insufficient sleep, and high study pressure were linked to neck pain, while poor sleep quality and emotional symptoms were associated with low back pain. These findings highlight the multifactorial nature of musculoskeletal pain and the need for comprehensive assessments in primary care.
Clinical trial number:
This study was registered at Chinese Clinical Trials Registry (http://www.chictr.org.cn/) on August 12, 2024. Clinical trial number: ChiCTR2400088109.
Introduction
Musculoskeletal pain (MSP) is caused by damage to the body’s biomechanical structure or tissues and manifests as pain in muscles, tendons, joints, bones, nerves, ligaments, cartilage, and intervertebral disks. 1 Chronic pain during adolescence not only burdens the body and mind but also imposes significant economic costs on society. 2 The World Health Organization’s Global Burden of Disease Report ranks neck pain and other MSP as the fourth and tenth leading causes of disability in adolescents. 3 A systematic review indicated that the prevalence of chronic pain among children and adolescents is approximately 20.8%, which is equivalent to 1 in 5 children and adolescents experiencing chronic pain. 4 Studies indicate that the prevalence of MSP increases with age. Musculoskeletal pain experienced in childhood and adolescence can develop into chronic MSP syndrome. 5
Musculoskeletal pain is a multifactorial condition influenced by various biological, psychological, and lifestyle factors.6 -9 Gender differences in MSP have been well documented, with females generally reporting higher prevalence and intensity of pain compared with males. 7 Physical inactivity is associated with chronic MSP and can exacerbate symptoms. Conversely, regular physical activity can improve pain management and overall health outcomes. 10 Psychosocial factors such as study pressure and mental health can significantly affect pain perception and coping mechanisms, making it crucial to assess these variables in adolescents. 11 Poor sleep quality and insufficient sleep duration are associated with increased pain sensitivity and MSP. 12 Excessive screen time is linked to sedentary behavior and MSP, particularly in the neck and upper back. 13
Meanwhile, many pathologies are biomechanical in origin and often associated with plantar pressure and foot type. The study of plantar pressure distribution has emerged as a critical area in biomedical and health-related research. Plantar pressure refers to the mechanical loads exerted on the soles of the feet during standing or walking. 14 Patients with foot pain, such as metatarsalgia and plantar fasciitis, often present with abnormal plantar pressure distribution. 15 This biomechanical disorder not only directly induces soft tissue microtrauma and bone stress remodeling in the foot but may also trigger a series of progressive musculoskeletal disorders through abnormal stress transmission along the lower limb kinetic chain, including knee osteoarthritis, hip joint dysfunction, and spinal postural compensations.16 -18 Previous studies have shown that different foot types influence the distribution of plantar pressure.19,20 Plantar pressure can be detected using The Plantar Pressure Testing Plate. 21 Foot type can be classified as high-arched, normal, or flat based on the Staheli Index (SI), a measurement derived from foot images. 22 A normal arch distributes body weight evenly across the foot and that a high arch causes excessive pressure on the heel and forefoot. 23 A low arch reduces the ability of the foot to absorb impact while walking or running, increasing the risk of injury. 24
Despite growing recognition of biomechanical contributions to MSP, critical gaps persist in adolescent populations. While adult studies have established strong associations between plantar pressure distribution and MSP,25 -27 these findings may not extrapolate to adolescents due to developmental differences in gait patterns and musculoskeletal maturation. 28 Unlike adults with fully ossified, stable feet, adolescents exhibit ongoing foot development, with ossification continuing until 16 to 18 years 29 and influenced by weight, genetics, and activity. These structural differences underscore the need for research specifically investigating the relationship between plantar pressure and MSP in adolescents. Furthermore, the systemic impact of altered plantar loading on MSP across multiple body regions remains unexamined. This gap is particularly notable given evidence that adolescents’ pain profiles differ fundamentally from adults’ in both prevalence and mechanical triggers.30,31 Finally, while multifactorial models increasingly dominate MSP research, 32 few studies have integrated quantifiable biomechanical measures with psychosocial and lifestyle variables in a unified framework. Our study addresses these gaps by examining how foot type, plantar pressure, physical activity, psychosocial, and lifestyle factors collectively influence MSP in a healthy adolescent population. These findings could inform targeted interventions and preventive measures, aligning with the World Health Organization’s emphasis on promoting musculoskeletal health in adolescents.
Methods
Participants
This cross-sectional study was conducted in Guangzhou, a major city in China, from September to December 2024. The sample was stratified by age and sex and a structured sampling method was used for recruitment to minimize selection bias. Sampling was conducted face-to-face in the community and schools. Random number sequences were generated via Excel software. Three researchers selected for this study were trained in administering the questionnaires and plantar equipment, and all measurement conditions for the participants, such as the time of day, the hardness of the surface on which they stand barefoot, and the temperature of the testing platform, were kept consistent to minimize measurement bias. Researchers conducted a centralized survey, provided detailed instructions on how to fill out the questionnaires before the survey, answered questions onsite, and asked participants to correct any errors or omissions immediately. Researchers explained the purpose of data collection and the method for completing the questionnaires and encouraged participants to complete the questionnaires accurately and comprehensively to ensure the authenticity, completeness, and high return rate of the questionnaires. After collection, 2 other researchers checked and verified the completeness of the returned questionnaires to reduce information bias.
The sample size was calculated via the formula n = Z2× (p × (1 − p)/d2),33,34 where Z = 1.96 (95% confidence level), p = 73.5% represents the estimated prevalence of musculoskeletal pain derived from a previous study, 35 and d = 0.1p, resulting in a minimum sample size of 138.5. A total of 225 questionnaires were distributed, of which 216 were valid and included in the final analysis; the remaining 9 were excluded due to withdrawal during data collection.
The inclusion criteria for this study were participants aged between 12 and 17 years, with good communication skills to ensure consistency and reliability in the data collection process. Effective communication is essential for accurate data collection. Communication skills were assessed using the Communication Competence Scale (CCS), which demonstrated excellent reliability (Cronbach’s α = .96) and good construct validity (comparative fit index = 0.94),36,37 with a score above 108 indicating adequate communication abilities. 38 Notably, while the high α value may suggest item redundancy, the scale remains useful given its established validity and widespread use. Participants were excluded if they had other diseases that significantly affected their quality of life, such as cardiovascular diseases, COPD, tumors, strokes, or if they had a history of musculoskeletal injuries or diseases requiring surgery. In addition, those with diseases affecting foot type or plantar pressure measurements or who were involved in other clinical trials that could affect the results of this study were excluded. By excluding these individuals, we aimed to create a more homogeneous study population where the outcomes could be more reliably assessed. This trial was conducted with the approval of the Ethics Committee of the Sixth Affiliated Hospital of Sun Yat-sen University (2024ZSLYEC-333) and was registered at the Chinese Clinical Trials Registry (ChiCTR2400088109). This trial was performed in accordance with ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All participants and their parents/guardians provided patient consent. This cross-sectional study was performed in line with the guidelines of the STROBE statement.
Musculoskeletal Pain
We developed the “Musculoskeletal Disorders and Health Status Questionnaire” to adapt the Dutch Musculoskeletal Questionnaire (DMQ) 39 for the specific learning environment of Chinese adolescents. The original DMQ demonstrates high reliability (Cronbach’s α = .83-.88) and strong content validity (content validity ratio = 0.96, content validity index = 0.91). 40 This questionnaire evaluated pain intensity across various body regions in adolescents, including the neck, shoulder, elbow, wrist, upper back, low back, hip, knee, and foot. Pain intensity was assessed via a numerical rating scale (NRS). The scale ranges from 1 to 10, where 1 to 3 indicates mild pain, 4 to 6 indicates moderate pain, and 7 to 10 indicates severe pain. Musculoskeletal pain was defined as pain in any part of the body in the past year, with neck pain referring specifically to pain in the neck, low back pain referring to pain in the low back, and foot pain referring to pain in the foot. Clinically, neck, low back, and foot pain are commonly reported. Low back and foot pain are often associated with abnormal plantar biomechanics. Therefore, based on their prevalence and clinical relevance in adolescent musculoskeletal pain, we selected neck, back, and foot pain as variables for logistic regression.
Foot Type and Plantar Pressure
Foot type and pressure were determined by static measurements. Because dynamic measurement requires specialized equipment and controlled environments, the results can vary significantly due to individual differences, making standardization challenging.
The Intelligent Foot Type Scanner (Ottobock Industrial Co., Ltd., China) (Figure 1) is a foot scanning device that performs static measurements. It quickly captures images and morphological features of the foot, producing a plantar image. The device is reliable, user friendly, and enhances the visibility of the foot.41,42 On the basis of the scanned foot images, the Staheli index (SI), a highly reliable metric, is used to assess the foot type.22,43 The SI is calculated by dividing the narrowest width of the midfoot (line a) by the widest width of the heel (line b) (SI = a/b) (Figure 2). A value below 0.50 indicates a high-arch foot, a value between 0.50 and 0.70 signifies a normal foot, and a value above 0.70 denotes a flatfoot.

The intelligent foot type scanner (Ottobock Industrial Co., Ltd., China).
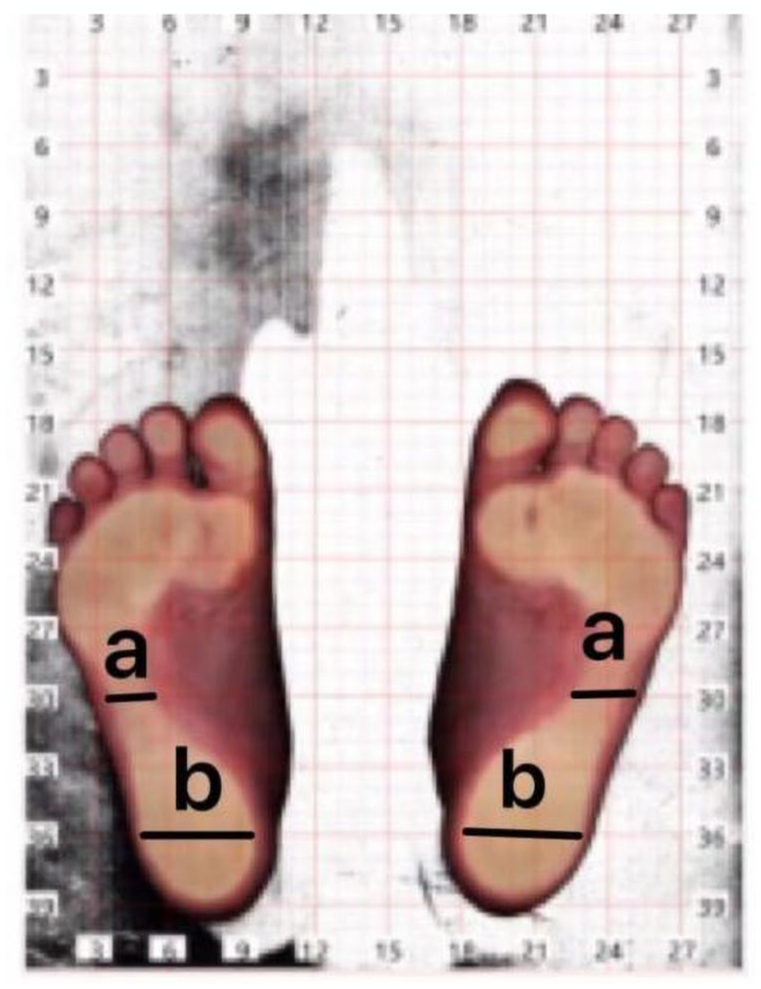
Foot type image.
The Plantar Pressure Testing Plate (Easystep Biotechnology Co., Ltd., China) (Figure 3) performs static measurements using resistive sensors to detect plantar stress, ensuring sensitivity and accuracy.21,44 Prior to measurement, the participants’ feet were thoroughly cleaned with alcohol. The participants were instructed to evenly distribute their weight on both feet while standing still on the pressure plate for 5 seconds. The plantar pressure data (Figure 4) including the maximum plantar pressure, average plantar pressure, maximum intensity of plantar pressure, average intensity of plantar pressure, and plantar contact area were recorded on a computer. High-pressure region of the foot refers to specific areas on the plantar surface of the foot that experience significantly higher vertical pressure compared with other regions during walking or standing. 45 We collected the pressure in high-pressure region by maximum plantar pressure and maximum intensity of plantar pressure. The maximum plantar pressure was categorized into 2 groups: <550 N and ⩾550 N.46,47 The average plantar pressure was divided into <180 N and ⩾180 N. Maximum intensity of plantar pressure was categorized into 2 groups: <1000 N/dm2 and ⩾1000 N/dm2, average intensity of plantar pressure was similarly divided into <300 N/dm2 and ⩾300 N/dm2.

Plantar pressure testing plate (Easystep Biotechnology Co., Ltd., China).

Plantar pressure.
Physical Activity
The International Physical Activity Questionnaire (IPAQ) is one of the most widely used and validated instruments for measuring physical activity, 48 demonstrating good reliability (Spearman’s ρ = 0.8) and acceptable criterion validity against accelerometry (Spearman’s ρ = 0.3), with its validity coefficient aligning with those typically observed for other self-report measures. 49 According to the IPAQ grading criteria, the metabolic equivalents (METs) are assigned to different intensities of activity: low-intensity activities (eg, walking) have a MET value of 3.3, moderate-intensity activities (eg, cycling) have a MET value of 4.0, and high-intensity activities (eg, running) have a MET value of 8.0. The activity level is classified as “low,” “moderate,” or “high.”
Psychosocial Factors
The Strengths and Difficulties Questionnaire (SDQ) is a self-report instrument designed to assess emotional and behavioral problems related to mental health in children and adolescents, 50 and has demonstrated satisfactory reliability (Cronbach’s α = .71-.81) and appropriate construct validity (Pearson’s r = 0.51-0.72). 51 It measures difficulties in 4 domains (emotional symptoms, conduct problems, hyperactivity, and peer problems) and includes prosocial behavior. The total difficulty score or individual dimension score in the abnormal range indicates potential emotional and behavioral issues. The abnormal SDQ score ranges are as follows: 7 to 10 points for emotional symptoms, 5 to 10 points for conduct problems, 7 to 10 points for hyperactivity, 6 to 10 points for peer relationship problems, 0 to 4 points for prosocial behavior, and 20 to 40 points for overall difficulties.
The 5-point Likert-type scale is used to assess the level of study stress experienced by the subjects and is rated from 1 to 5. A higher score indicates greater study stress.52,53
Habits of Daily Living
A self-designed questionnaire on daily living habits covering the following aspects over the past year was used: daily sleep duration, sleep quality, and average daily screen time for entertainment. The American Academy of Sleep Medicine and the Sleep Research Society jointly issued a consensus statement recommending that the optimal sleep duration for healthy adults is 7 to 9 hours per night. 54 Sleeping less than 7 hours per night on a regular basis is associated with chronic pain. Therefore, sleep duration was classified into 2 groups: less than 7 hours and 7 hours or more. Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), which has demonstrated satisfactory test-retest reliability (ICC = 0.721-0.753) and construct validity (comparative fit index = 0.960). 55 The PSQI yields a global score ranging from 0 to 21, with higher scores indicating poorer sleep quality; scores of 16 to 21 is classified as indicative of poor sleep.56,57 Average daily screen time was dichotomized into 2 groups: less than 2 hours and 2 hours or more.58 -60
Statistical Analysis
All data were entered into Excel and analyzed using SPSS version 27.0. Categorical data are summarized as frequencies (percentages). To reduce the impact of outliers on the analysis, address issues arising from non-normal distribution or violations of model assumptions and enhance the stability and reliability of statistical models, continuous variables such as age and time were converted into categorical variables. The χ2 test was used to examine the associations between each potential risk factor (gender, foot type, plantar pressure, physical activity, psychosocial factors, sleep quality, sleep duration, average screen time, and study pressure) and the prevalence of musculoskeletal pain. Fisher exact test was applied when the expected frequencies did not meet the requirements for the χ2 test. Logistic regression analysis was performed to determine the factors associated with the prevalence of MSP, neck, low back, and foot pain. Odds ratios (ORs) with 95% confidence intervals (CIs) were computed for each predictor variable. A P value of less than .05 was considered statistically significant. Sampling weights were not applied in the analysis, as the primary aim was to examine associations between risk factors and musculoskeletal pain rather than to estimate population prevalence. Furthermore, the stratification variables (age and sex) were included as covariates in the regression models to adjust for potential confounding related to the sampling design. No missing data were present for any of the variables included in the analysis.
Results
Of the 225 questionnaires distributed, 216 were valid and included in the final analysis, and the remaining 9 were excluded due to participant withdrawal during data collection. The 216 participants comprised 112 males (51.9%) and 104 females (48.1%), with a mean age of 15.83 ± 1.05 years (range: 12-17), with no significant sex-based differences (males: 15.83 ± 1.26; females: 15.84 ± 0.82; P = .932). No missing data were present for any variable. Further demographic characteristics are shown in Table 1.
Demographics of the Participants (means ± SD).

Abbreviations: BMI, body mass index; cm, centimeter; kg, kilogram; SD, standard deviation.
MSP, Foot Type, Physical Activity, and Psychosocial Factors of the Participants
Among the 216 participants, the prevalence of MSP in the past year was 65.3%. The most common pain sites were the neck (52.3%), while the least reported was elbow pain (6.9%). Regarding foot type, normal feet were the most prevalent (69.4%), followed by high-arched feet (26.9%) and flatfoot (3.7%). Physical activity levels were distributed across middle (43.5%), high (31.9%), and low (24.5%) intensity. Among the emotional and behavioral problems, the highest anomaly rate was for emotional symptoms (13.0%) (Figure 5).

MSP, foot type, physical activity, and psychosocial factors of the participants.
Univariate Analysis of Factors Associated With MSP in Participants
Statistical differences in MSP prevalence were observed on the basis of sex, emotional symptoms, average screen time, average intensity of plantar pressure, and plantar contact area (P < .05). Statistically significant differences in neck pain incidence were noted in terms of physical activity, sleep duration, and study pressure (P < .05). For low back pain incidence, statistically significant differences were observed in terms of sex, emotional symptoms, hyperactivity, total difficulties, sleep quality, and sleep duration (P < .05). Foot pain incidence was statistically significant associated with emotional symptoms, sleep duration, study pressure, average plantar pressure, average intensity of plantar pressure, maximum intensity of plantar pressure, and foot type (P < .05) (Table 2).
Univariate Chi-Square Analysis of Factors Associated With MSP in Participants [Number/Percentage (%)].
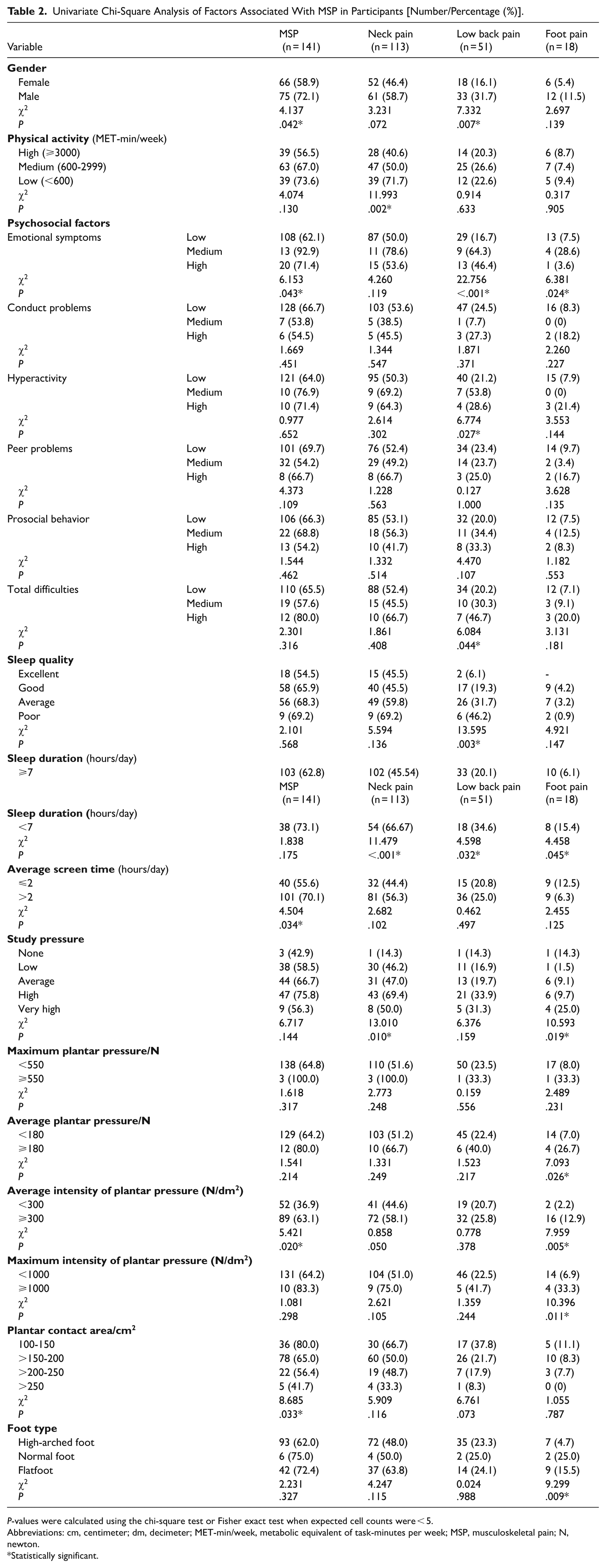
P-values were calculated using the chi-square test or Fisher exact test when expected cell counts were < 5.
Abbreviations: cm, centimeter; dm, decimeter; MET-min/week, metabolic equivalent of task-minutes per week; MSP, musculoskeletal pain; N, newton.
Statistically significant.
Multivariate Logistic Regression Analysis of MSP in Participants
Using the significant factors from Table 2 as independent variables, multivariate logistic regression analysis was performed with dummy variables assigned. The results indicated that physical activity, sleep duration, and study pressure were significantly associated with the prevalence of neck pain (P < .05). Emotional symptoms at the threshold or abnormal and poor sleep quality statistically significantly increased the risk of low back pain (P < .05). The risk of foot pain increased with a maximum intensity of plantar pressure ⩾ 1000 N/dm2, average plantar pressure ⩾ 180 N, and flatfoot or high-arched foot (P < .05). The multivariate logistic regression analysis results are detailed in Tables 3 to 6.
Multivariate Logistic Regression Analysis of MSP in Participants.
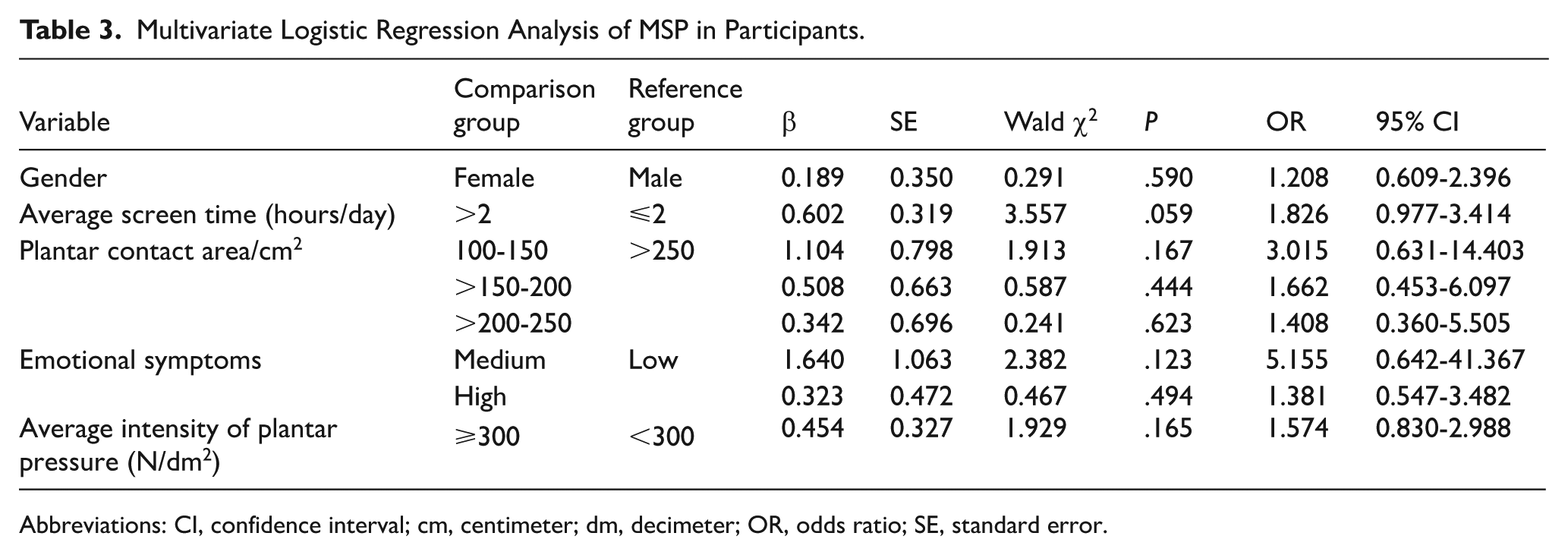
Abbreviations: CI, confidence interval; cm, centimeter; dm, decimeter; OR, odds ratio; SE, standard error.
Multivariate Logistic Regression Analysis of Neck Pain in Participants.
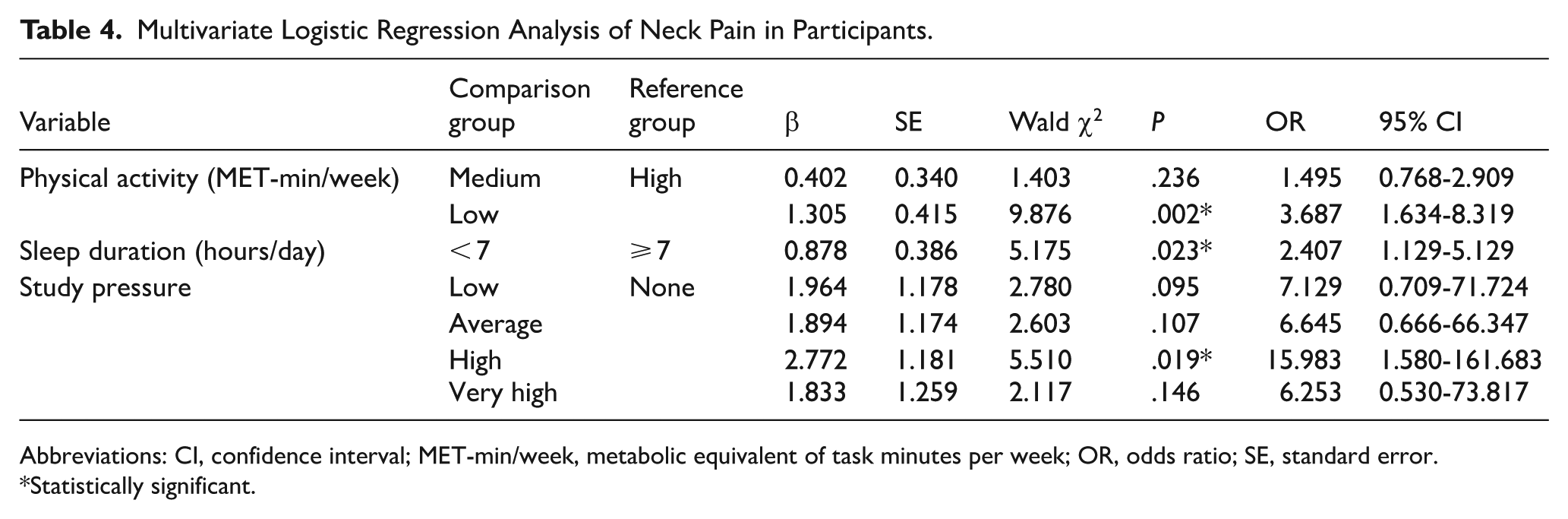
Abbreviations: CI, confidence interval; MET-min/week, metabolic equivalent of task minutes per week; OR, odds ratio; SE, standard error.
Statistically significant.
Multivariate Logistic Regression Analysis of Low Back Pain in Participants.
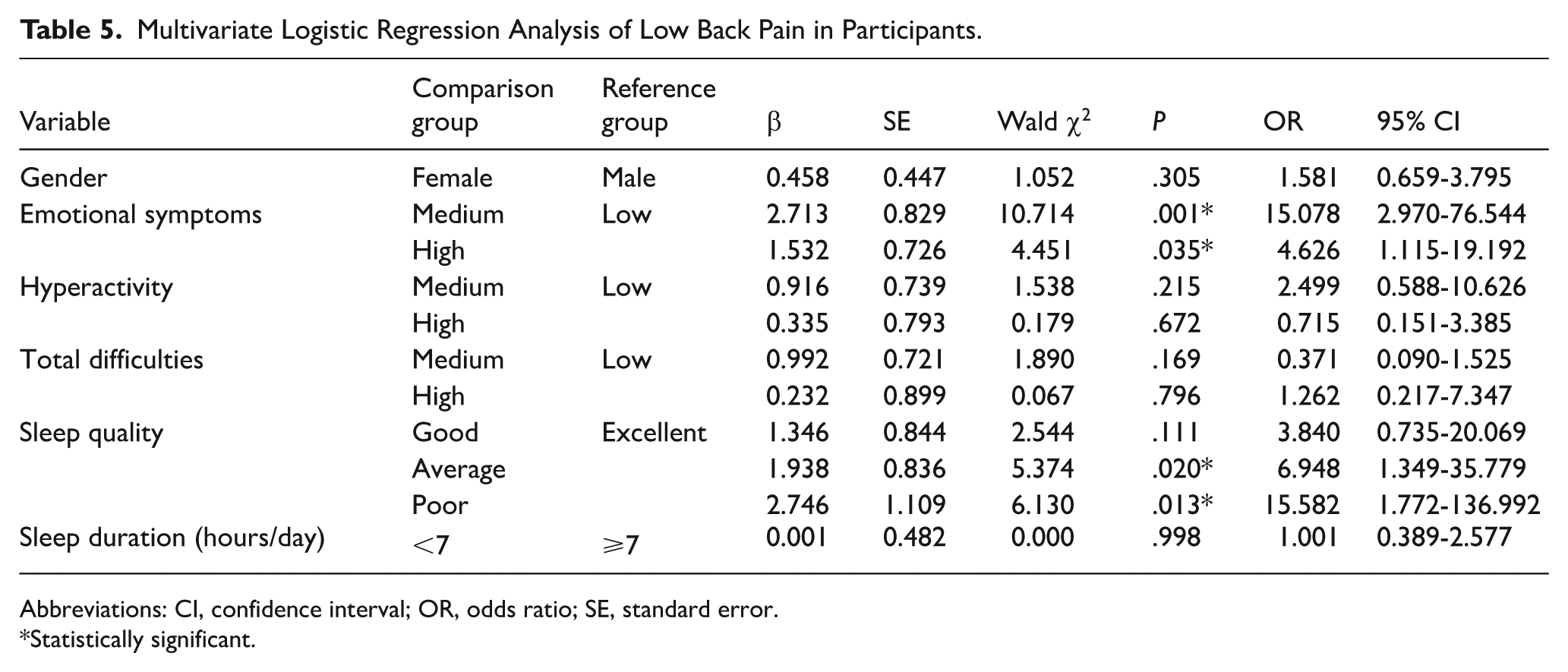
Abbreviations: CI, confidence interval; OR, odds ratio; SE, standard error.
Statistically significant.
Multivariate Logistic Regression Analysis of Foot Pain in Participants.

Abbreviations: CI, confidence interval; cm, centimeter; dm, decimeter; N, newton; OR, odds ratio; SE, standard error.
Statistically significant.
Discussion
Musculoskeletal pain is a prevalent issue among adolescents that significantly affects their quality of life and daily functioning. In this study, we found that adolescents with flatfeet or high-arched feet are more likely to experience foot pain, highlighting the importance of biomechanical factors in MSP. We also found that low physical activity, insufficient sleep, and high study pressure are significant risk factors for neck pain, while poor sleep quality and emotional symptoms are associated with low back pain. Although previous studies have investigated various factors contributing to MSP, including biomechanical, 15 psychological,61,62 and lifestyle factors,10,63 the integrated effects of these factors on MSP in adolescents remain underexplored. The present study addresses this gap by comprehensively analyzing the associations between MSP and multiple factors, including foot type, plantar pressure, physical activity, psychosocial factors, and daily living habits, these findings underscore the complex interplay of factors contributing to MSP and emphasize the importance of multidimensional evaluations in primary care.
Foot Type and Plantar Pressure
Existing studies primarily focus on the characteristics and influencing factors of foot type and plantar pressure in adolescents. For instance, Cimolin et al 64 reported that obese participants had significantly higher area of contact in forefoot and midfoot. Our study innovatively integrated quantifiable biomechanical measures with psychosocial and lifestyle variables. We found that adolescents with flatfoot, high-arched foot, or high plantar pressure were more prone to suffer from foot pain. This association can be explained by the biomechanical function of the foot arch. A normal, healthy arch of the foot provides appropriate load-bearing pressure on the plantar surface, helping the body withstand pressure during movement and reduce the likelihood of injury due to excessive load on the feet. 65 However, abnormalities in the arch can lead to changes in the distribution of load and pressure.66,67 Flatfeet reduce the ability to absorb impact forces while walking or running, which leads to compensatory overloading of the plantar fascia and posterior tibial tendon. Such biomechanical alterations may further increase the risk of various conditions, such as tendonitis, plantar fasciitis, and metatarsal pain. 68 High-arched foot pressure is concentrated on the heel and forefoot, and excessive plantar pressure contributes to fatigue and inflammation of the plantar muscles, leading to plantar pain and heel pain. 69
Importantly, the biomechanical effects of foot abnormalities may extend beyond the foot itself. According to the kinetic chain theory, abnormal foot posture can disrupt the alignment of the lower limb, leading to compensatory changes that propagate upward through the ankle, knee, hip, and pelvis to the spine, thereby increasing the risk of low back pain.70,71 Although our study did not find a direct association between foot-related factors and low back pain, this does not necessarily contradict the kinetic chain theory. Instead, it may suggest that psychological factors play a more dominant role in low back pain among adolescents, potentially masking any biomechanical contributions.
Since abnormal foot type and elevated plantar pressure are significantly associated with foot pain in adolescents, early identification and targeted intervention are essential. Abnormal plantar pressure often precedes the onset of pain 72 ; therefore, plantar pressure measurement can identify individuals at risk before symptoms emerge. Early detection is particularly critical because adolescent foot pain frequently recurs and may persist into adulthood. This allows for timely interventions, such as custom orthotic insoles and foot muscle strengthening exercises. These strategies can effectively prevent the onset and progression of foot pain.
Physical Activity and Neck Pain
Our study revealed that physical inactivity is associated with an increased risk of neck pain. A study on office workers by Luis et al 73 revealed a significant association between sedentary behavior and the incidence of neck pain and low back pain, which underscores the broader implications of prolonged sitting, particularly for adolescents who may be at increased risk of developing neck pain due to insufficient physical activity during activities such as studying or playing computer games. Ucan et al 74 found that older adults diagnosed with chronic pain had lower levels of physical activity. In contrast, higher levels of physical activity can serve as a predictive factor for pain reduction in adolescents with chronic pain. 75 A total of 81.0% of adolescents worldwide are physically inactive. 76 Exercise has been shown to reduce sensitivity to painful stimuli in healthy individuals, indicating that exercise might be an effective strategy for preventing chronic pain and alleviating persistent pain symptoms in those with chronic conditions. 77 The link between exercise and endogenous pain regulation is increasingly recognized. The evidence suggests that more active individuals tend to have better pain regulation. 78 The mechanism behind this effect involves the activation of the endogenous opioid system, 79 which can modulate pain perception. Animal studies have demonstrated that regular aerobic exercise can mitigate neuropathic pain by increasing opioid release from the central nervous system. 80 Consequently, encouraging adolescents to engage in regular exercise and reduce sedentary behavior can serve as a beneficial rehabilitation approach for managing MSP.
Psychosocial Factors and Musculoskeletal Pain
Several studies have investigated the associations between psychosocial factors and MSP. For example, Trevelyan and Legg 81 reported that abnormal behavior problems were linked to low back pain in children aged 11 to 14 years. These findings suggest that psychosocial factors alongside physical factors may significantly contribute to MSP in adolescents. Our study supports this view, showing that psychological problems as measured by the SDQ scale are key factors associated with low back pain and that increased study stress is correlated with a greater incidence of neck pain. From a neurobiological perspective, psychological factors such as depression, anxiety, and stress may disrupt pain regulation and enhance nociceptive pathways. 82 Stress can lead to overactivation of the HPA axis, resulting in excessive cortisol release which heightens pain perception. 83 During adolescence, the HPA axis exhibits a more pronounced and prolonged cortisol response to stress compared with adulthood. 84 Meanwhile, the emotion-regulating amygdala-prefrontal cortex circuitry remains immature, leading to poorer emotional regulation and increased stress vulnerability. 85 These neurodevelopmental characteristics render adolescents more susceptible to stress-induced hyperalgesia.
Sleep Quality and Musculoskeletal Pain
Our study revealed that adolescents who sleep less than 7 hours per day experience a notable increase in neck pain, whereas poor sleep quality is linked to a greater prevalence of low back pain. A meta-analysis by Santos et al 86 indicates that the prevalence of sleep problems and sleep disorders in patients with chronic musculoskeletal pain is remarkably high, approximately 75% and 44%, respectively. The research by Marin et al 87 suggests a significant positive correlation between sleep quality and the intensity of low back pain which supports our findings. Their study population mainly comprised middle-aged and older adults, whereas our study contributes to understanding the relationship between musculoskeletal pain and sleep in adolescents. The interaction between chronic pain and sleep often creates a vicious cycle: sleep deprivation can worsen chronic pain and lead to increased sensitivity to pain.56,88 Pain can interfere with the ability to fall asleep and diminish overall sleep quality. Therefore, adequate sleep is crucial for adolescents maintaining overall health. 89
Limitation
This study has several methodological limitations. First, the distribution of foot types in our sample was imbalanced, with few cases of flatfoot or high-arched feet. This limitation is unavoidable, as foot type abnormalities are uncommon in the general adolescent population. Nonetheless, the small number of cases limited statistical power for subgroup analyses, resulting in wide confidence intervals and imprecise estimates. Second, the present study employed static plantar pressure measurement which captures foot pressure only during quiet standing and does not reflect dynamic biomechanics during weight-bearing activities such as walking or running. Third, physical activity was measured using the International Physical Activity Questionnaire (IPAQ), which tends to overestimate activity levels in adolescents, and pain was self-reported, which may introduce recall bias. Moreover, constrained by the cross-sectional design, this study was unable to establish causal relationships between the risk factors and musculoskeletal pain. In summary, while our findings provide preliminary insights into the associations between MSP and multiple factors, they should be interpreted with caution. Future research should address these limitations by adopting a prospective study design to further elucidate the causal relationships between risk factors and musculoskeletal pain, employing larger and more diverse samples to ensure adequate representation of participants with abnormal foot types, incorporating dynamic plantar pressure measurements, and using objective tools for data collection. Such tools include wearable devices such as smartwatches to provide precise quantification of physical activity intensity and patterns, as well as ecological momentary assessments via mobile applications to capture real-time pain experiences, thereby minimizing recall bias inherent in retrospective self-reports.
Conclusions
This study provides new insights into the associations of musculoskeletal pain with foot type and plantar pressure, through an analysis of its incidence across various body parts among adolescents recruited from schools and communities in Guangzhou, China. Our findings indicate that factors such as flatfeet or high-arched feet, increased plantar pressure, low physical activity, insufficient sleep, poor sleep quality, high study pressure, and abnormal psychological status are significantly associated with a higher likelihood of MSP. These findings provide empirical data supporting the understanding of MSP among urban adolescents and highlight the multifactorial nature of this condition, underscoring the necessity of a comprehensive assessment in primary care settings. Further research is needed to determine whether these findings extend to adolescents in other geographic or cultural contexts.
Footnotes
Acknowledgements
The authors would like to thank the librarians and statisticians at Sun Yat-sen University for their technical support.
Ethical Considerations
This study received approval from the Ethics Committee of the Sixth Affiliated Hospital of Sun Yat-sen University (2024ZSLYEC-333) and was performed in accordance with ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. This study has been registered with the Chinese Clinical Trials Registry (ChiCTR2400088109).
Consent to Participate
All participants and their parents/guardians provided informed consent.
Consent for Publication
Written informed consent was obtained from all participants prior to publication.
Author Contributions
Conceptualization: YYL, JL, PHW; Acquisition of data for the work: YQZ, JZY, YXL, BNW, HQJ, YXL, YYX; Review and analysis: YQZ, JZY, LJL, LSS, YXL; Manuscript drafting: YQZ, JZY, LJL, YXL, BNW; Paper review and revision: YYL, JL, PHW.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received support from the National Natural Science Foundation of China (Grant No. 8227090290), the Program of Guangdong Provincial Clinical Research Centre for Rehabilitation Medicine (Grant No. 2023B110003), and the “1010” Program of Clinical Research at The Sixth Affiliated Hospital of Sun Yat-Sen University (Grant No. 1010PY-2022-54).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.