
Abstract
Aim:
To evaluate the efficacy and safety of the HeartMate 3 (HM3) left ventricular assist device (LVAD) as a destination therapy (DT) for patients with end-stage heart failure (HF) ineligible for transplantation, from a Peruvian healthcare perspective.
Methods:
A health technology assessment (HTA) was conducted, which included a systematic review of clinical effectiveness and safety, complemented by a critical appraisal of relevant evidence. Searches were performed in 3 databases, complemented by manual searches in HTA organizations and clinical practice guidelines (CPGs) repositories. The search included CPGs, HTAs, randomized clinical trials (RCTs), and high-quality observational studies evaluating LVADs for DT. Cost-effectiveness analyses and device costs specific to the Peruvian context were also reviewed.
Results:
All the CPGs supported the use of the HM3 LVAD, emphasizing its significant survival benefits demonstrated in primary studies. The HM3 showed a 5-year survival rate exceeding 50%, compared to 25% at 1 year and 8% at 2 years with optimal medical therapy (OMT). Functional and quality of life outcomes also improved significantly. However, common adverse events included bleeding and infections. Cost-effectiveness analyses from high-income settings indicated that the HM3 exceeded conventional willingness-to-pay thresholds but highlighted its critical clinical benefits for high-risk patients with no alternative therapies.
Conclusion:
The HM3 LVAD offers significant survival and quality of life improvements for patients with end-stage HF ineligible for transplantation. Despite challenges in cost-effectiveness, the adoption of the HM3 as DT in Peru is justified to address a critical unmet clinical need, provided robust medical device surveillance is implemented.
Introduction
End-stage heart failure (HF) represents the terminal phase of a progressive and debilitating condition characterized by the persistent inability of the heart to maintain adequate cardiac output despite optimal medical therapy. 1 This advanced stage, often categorized as New York Heart Association (NYHA) Class III or IV or Stage D according to the American Heart Association (AHA)/American College of Cardiology (ACC) classification, is marked by severe functional limitations, dyspnea at rest or with minimal exertion, fatigue, and peripheral edema.2 -5 These symptoms profoundly diminish patients’ quality of life and increase the risk of recurrent hospitalizations and short-term mortality.5,6
Standard management strategies, including angiotensin-converting enzyme inhibitors (ACEIs), beta-blockers, and aldosterone antagonists, are frequently inadequate for patients with refractory HF.4,5 Although heart transplantation remains the gold standard treatment for select patients, many are ineligible due to contraindications such as advanced age, irreversible renal or hepatic dysfunction, or severe comorbidities like active malignancies or systemic diseases.7 -10 Moreover, pulmonary hypertension, characterized by elevated pulmonary vascular resistance and fixed hemodynamic changes, further limits transplant candidacy in this population.7,10
Left ventricular assist devices (LVADs) have emerged as a viable alternative for patients with contraindications to transplantation, particularly as destination therapy (DT), where the device serves as a permanent replacement for left ventricular function. 11 Unlike its use as a bridge to transplantation, DT aims to provide long-term hemodynamic support, improving tissue perfusion and sustaining quality of life. 12 Recent studies have reported significant survival benefits and symptomatic improvement with LVADs in patients with otherwise limited therapeutic options.13 -15
In Peru, LVADs have received commercial authorization from the Directorate General of Medicines, Supplies, and Drugs (DIGEMID, by its acronym in Spanish), ensuring regulatory approval for clinical use. The Thoratec® HeartMate 3™ Left Ventricular Assist System (LVAS) is currently the only long-term LVAD available in Peru with an indication for DT in patients with end-stage HF. Currently, the Peruvian Social Health Insurance System (EsSalud, by its acronym in Spanish), provides short-term ventricular support devices; however, there is no provision for long-term LVADs for patients with terminal HF who are not candidates for transplantation. This situation highlights a critical unmet clinical need for advanced therapies capable of offering continuous circulatory support and improving outcomes in this high-risk population. In response to this gap, a health technology assessment (HTA) was conducted to evaluate the efficacy and safety of LVADs as DT in patients with end-stage HF from a Peruvian healthcare perspective.
Methods
Design
This assessment followed an HTA-based methodological framework, which integrates a systematic review of clinical effectiveness and safety with additional components such as appraisal of CPGs, review of HTA reports, contextual considerations, and economic evidence.16,17 The objective was to synthesize and evaluate the available evidence on the efficacy and safety of long-term LVADs as destination therapy in patients with end-stage HF.
Clinical (PICO) Question
The HTA was guided by a PICO framework that defined the clinical question to be addressed. This PICO question was proposed by an HTA working group and validated by a multidisciplinary team of methodologists and clinicians specializing in heart failure management.
Population: Patients with end-stage heart failure (NYHA III-IV or Stage D according to AHA/ACC classification) who are ineligible for heart transplantation.
Intervention: Implantable left ventricular assist device with indication for destination therapy.
Comparator: Best supportive care or optimal medical therapy (OMT), defined as reported in each primary study.
Outcomes: Overall survival, adverse events (device-related or procedure-related), quality of life.
Search of Evidence
A systematic search of the literature was conducted in September-October 2024 to identify the best available evidence regarding the efficacy and safety of implantable LVAD with an indication for DT in patients with end-stage HF. The search was performed using the PubMed, Cochrane Library, and LILACS (Latin American and Caribbean Literature on Health Sciences) databases. Details of the search strategies, including terms and results, are provided in Supplemental Tables S1-S3.
In addition, manual searches were conducted on the websites of institutions and organizations developing HTAs. These included the Centro Nacional de Excelencia Tecnológica en Salud (CENETEC), the National Institute for Health and Care Excellence (NICE), the Agency for Healthcare Research and Quality (AHRQ), the Scottish Intercollegiate Guidelines Network (SIGN), and the Guidelines International Network (GIN). Other resources reviewed included BRISA (Regional Base of HTA Reports of the Americas), CONITEC (National Commission for Technology Incorporation in the Unified Health System), the Agencia Gallega de Conocimiento en Salud, the Institute of Health Technology Assessment (IETS), the Institute of Clinical and Health Effectiveness (IECS), the Scottish Medicines Consortium (SMC), Canada’s Drug Agency (CDA), the German Institute for Quality and Efficiency in Health Care (IQWiG), and the Hauté Autorité de Santé (HAS).
CPGs from cardiology societies and institutions specializing in heart failure and transplantation were also reviewed. These included the European Society of Cardiology (ESC), the American College of Cardiology (ACC), the International Society for Heart and Lung Transplantation (ISHLT), the American Heart Association (AHA), the Heart Foundation, and the Cardiac Society of Australia and New Zealand (CSANZ). Finally, searches for ongoing or unpublished clinical trials were performed on ClinicalTrials.gov and the International Clinical Trial Registry Platform (ICTRP).
Selection Criteria
The search targeted CPGs, HTAs, and primary studies without restrictions on language, time, or country. CPGs were included if they outlined a systematic development process, provided a detailed description of evidence appraisal, employed grading systems for recommendations and evidence levels, and offered recommendations specific to the PICO population. HTAs were included if they addressed the PICO population and intervention, described systematic evidence search and appraisal processes, and included a critical appraisal or recommendation.
For primary studies, we prioritized phase-3 randomized controlled trials (RCTs) and systematic reviews of RCTs. In their absence, high-quality observational studies were considered if they addressed the PICO question. High-quality observational studies were defined as those with adequate sample size, clearly defined DT populations, and sufficiently detailed reporting of outcomes relevant to the PICO framework. Single-arm studies were eligible for inclusion when they provided specific data for DT in patients meeting the PICO-defined characteristics, even in the absence of a comparator group. Publications such as abstracts and observational studies with fewer than 50 patients in the arm of interest or insufficient subgroup data were excluded. This threshold was applied to avoid the imprecision and instability typically associated with very small cohorts.18 -20
Selection Process
The selection process followed a 3-stage framework (Figure 1). In the first stage, 2 independent reviewers screened titles and abstracts using the Rayyan web application (https://www.rayyan.ai/). Conflicts were resolved by consensus, and studies requiring additional information were included for full-text review. In the second stage, 1 reviewer evaluated the full text of selected studies to confirm eligibility. In the final stage, the methodological team reviewed the included studies to ensure they addressed the PICO question. This stage also allowed for the exclusion of studies that, upon closer analysis, did not meet the predefined inclusion criteria or provided insufficient evidence.
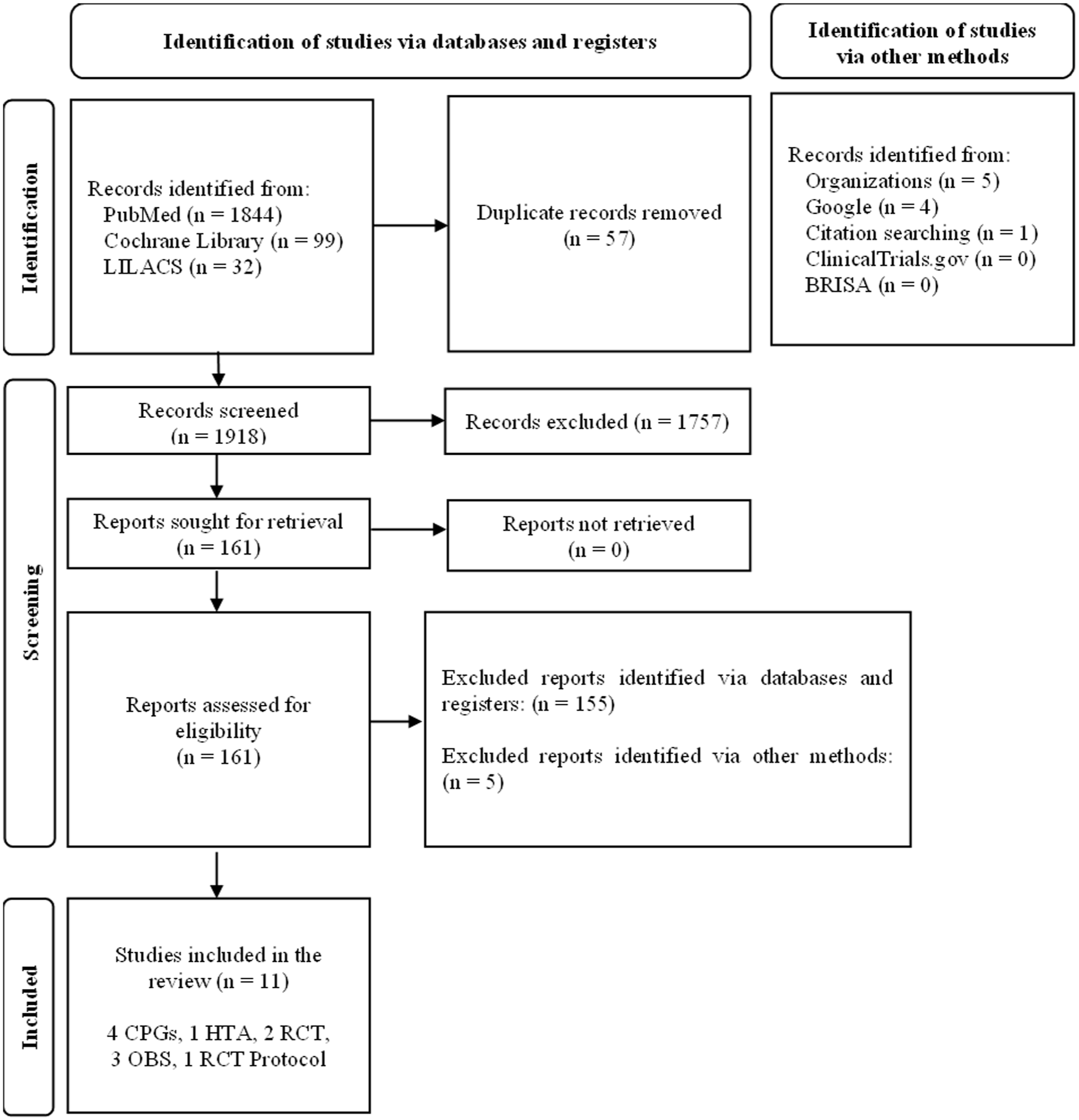
Flowchart adapted from PRISMA 2020.
Data Extraction
Information from all included evidence sources was extracted by 1 reviewer, focusing on the elements relevant to addressing the PICO question. These included study design, population characteristics, DT-specific subgroups, device characteristics, outcomes (survival, adverse events, functional status, and quality of life), follow-up duration, and key methodological features. The extracted information was then presented and verified in a meeting with the full methodological team to ensure accuracy and completeness.
Appraisal of Methodological Quality
Formal risk-of-bias tools (eg, RoB 2.0, ROBINS-I, AMSTAR) were not applied because this HTA integrated heterogeneous evidence sources (CPGs, HTAs, trials, and observational studies) and aimed to provide a contextualized assessment rather than tool-based scoring. Instead, the methodological strengths and limitations of each evidence source were appraised qualitatively using pre-specified domains aligned with the constructs typically assessed by these frameworks.
For primary studies, domains included: (i) study design and internal validity features; (ii) clarity and appropriateness of the DT population definition and eligibility criteria; (iii) outcome definitions and ascertainment (including whether outcomes were adjudicated and whether reporting was DT-specific); (iv) completeness of follow-up and missing data; (v) sample size and precision; and (vi) risk of confounding and selection bias (particularly for observational and single-arm studies). For CPGs and HTA reports, domains included: transparency and reproducibility of the evidence search and selection process; explicit linkage between evidence and recommendations/conclusions; use of evidence grading systems; and disclosure and management of conflicts of interest. These qualitative appraisals were used to guide evidence inclusion, interpretability, and the level of caution applied in the narrative synthesis, and their main findings are summarized in the Results section.
Evidence Synthesis
This HTA followed the synthesis model routinely used in our agency, which relies on structured descriptive analysis rather than quantitative pooling. Even if a quantitative synthesis had been planned, it would not have been feasible because no primary studies directly compared HM3 with OMT in our PICO population. The evidence was therefore organized by type of source (CPGs, HTAs, RCTs, observational studies) and by clinical domain (survival, adverse events, functional outcomes, and quality of life). For studies involving mixed indications or multiple LVAD generations, only DT-specific and HM3-specific information was extracted. Indirect descriptive comparisons were incorporated when relevant to contextualize findings within the PICO framework.
Focus on HeartMate3
Although the HTA was not designed to evaluate specific LVAD brands, a preliminary review identified that only the HeartMate 3 (HM3) has regulatory approval for DT in Peru. Other devices, such as the HeartWare and HeartMate II (HMII), while providing important historical contributions to the evolution of centrifugal-flow designs through evidence from the ADVANCE 21 and ENDURANCE 22 trials, are either no longer available or lack regulatory approval in the Peruvian market. HM3 incorporates notable advancements, including a fully magnetic levitated pump, which may reduce the risk of blood trauma and the intensity of anticoagulation requirements compared to earlier-generation devices. Previous studies have compared HM3 with its predecessors, demonstrating improved outcomes in terms of device-related complications and survival.13,23,24
Given these technical and clinical considerations, HM3 was selected as the primary focus of this HTA. Hence, when studies compared HM3 with earlier devices, only data from the HM3 arm were extracted, as the objective of the HTA was to characterize outcomes specifically for the device approved for DT in Peru.
Complementary Search and Cost Information Analysis
For exploratory purposes, a complementary search was conducted exclusively for economic evaluations. We included full cost-effectiveness or cost-utility analyses and decision-analytic modeling studies that evaluated long-term LVADs, particularly HM3, in populations comparable to the PICO question. These studies were identified from the main database searches and through targeted searches of HTA reports and reference lists (Supplemental Tables S4-S6). Additionally, we described the costs of the HM3, based on the Peruvian context for the Social Health Insurance system. Cost information was sourced from the National Cardiovascular Institute (INCOR), a leading specialized reference center in Peru, and from the manufacturer.25,26
Results
Selected Studies
After the comprehensive literature search conducted on September 6, 2024, 4CPGs,4,27 -29 1 HTA, 30 2 RCTs,31,32 3 observational studies33 -35 (233,34 of which were derived from MOMENTUM 3), and 1 RCT protocol 36 were included. A summary of the key characteristics and outcomes of the included evidence is presented in Supplemental Table S7. Registry-derived publications (eg, ELEVATE and INTERMACS/IMACS outputs) were screened during full-text assessment but were excluded when they did not report outcomes stratified for HM3 used as DT, reported outcomes aggregated across LVAD generations and/or therapeutic indications (eg, bridge-to-transplant and DT), or focused on surgical-technique comparisons or prediction modeling rather than the prespecified PICO outcomes.
Due to the absence of primary studies directly comparing the HM3 with OMT in patients with end-stage heart failure who are ineligible for heart transplantation, single-arm data from studies evaluating HM3 for destination therapy or medical therapy in similar populations were used. Indirect descriptive comparisons were performed using data from studies comparing HM3 with its predecessor, the HeartMate II (HMII). Only data from the HM3 arm were extracted and analyzed when relevant to the PICO question
Overview of the Evidence
Clinical Practice Guidelines
Regarding the population of interest, 4 CPGs issued recommendations on the use of implantable LVADs in patients with end-stage HF. The ESC 2021 guideline 27 recommended considering long-term mechanical circulatory support (MCS) in patients with advanced heart failure with reduced ejection fraction (HFrEF) who are unresponsive to optimized medical and device therapy, not eligible for heart transplantation or other surgical options, and without severe right ventricular dysfunction. The CPG stated that this intervention is indicated to reduce mortality risk and improve symptoms.
The AHA/ACC/HFSA 2022 guideline 4 suggested that in selected patients with advanced HF and NYHA class IV symptoms despite guideline-directed medical therapy, durable MCS is beneficial for improving symptoms, functional class, and reducing mortality. They also noted that durable MCS should be considered in patients dependent on intravenous inotropes, as destination therapy provides significant survival and health-related quality of life benefits.
The NHFA/CSANZ 2018 guideline 29 recommended referral to a specialized center for consideration of LVAD implantation in patients with severe, intractable HF despite guideline-directed medical and device therapy, who do not have major comorbidities. The CPG stated that this approach aims to reduce mortality in this patient population.
It is important to note that the evidence used in these 3 guidelines include studies comparing earlier versions of the HM3 with OMT, as well as results from the MOMENTUM 3 trial. Additionally, both authors and reviewers of these CPGs have received honoraria from Abbott, as detailed in the conflict-of-interest statements of each guideline.
The fourth guideline, ISHLT 2023, 28 recommended that patients with advanced HF symptoms (NYHA class IIIB-IV), refractory to maximal medical management, dependent on inotropes or temporary circulatory support, should be considered for durable MCS as long-term support if transplantation is unlikely in the short term, if a period of support could improve transplant candidacy, or as destination therapy for patients not eligible for transplantation. Additionally, in cases with increased propensity for recurrent pump thrombosis, the ISHLT recommended considering a switch to the HM3 from a previous device if clinically indicated. Unlike the previous 3 guidelines, the ISHLT 2023 guideline presents methodological limitations. Although the ISHLT has general directives indicating the need for comprehensive literature search and integration of expert opinion to support recommendations, the document lacks specific details on the search strategy or systematic process followed. Instead of explicitly associating evidence with each recommendation, it provides a list of references grouped by topic, limiting transparency regarding the support for each recommendation. Furthermore, several authors and reviewers have received honoraria from Abbott; however, these conflicts of interest are not disclosed in the document and had to be identified manually.
Health Technology Assessment
The HTA conducted by Beese et al in the United Kingdom 30 addressed the use of LVADs, particularly the HM3, as destination therapy in patients with advanced HF who are not candidates for transplantation. The authors concluded that although the HM3 demonstrated a survival advantage compared to OMT in this population, cost-effectiveness criteria applied in the UK suggest that its use may not be affordable. The economic model did not find the HM3 to be cost-effective compared to OMT, considering a willingness-to-pay threshold of £50 000 per quality-adjusted life year (QALY) gained. The analysis suggested that despite clinical evidence supporting the survival benefit of LVADs in end-stage HF, there may not be sufficient evidence to justify their use within the UK’s health system in terms of cost-effectiveness. The systematic review within the HTA included an analysis of clinical effectiveness and a network meta-analysis, concluding that LVADs have significantly improved in reducing complications and adverse events compared to previous models like the HeartMate II. However, the lack of direct comparative studies between the HM3 and OMT limits the generalizability of the findings. This prompted the use of economic models with extrapolation beyond the available follow-up period, introducing uncertainty in cost-effectiveness estimates. Additionally, the HTA evidenced significant variations in cost-effectiveness results influenced by device type, analytical approach, and geographic and temporal context.
The economic model included methodological limitations and assumptions, such as projecting major events using data from earlier-generation devices. The authors assumed that each patient could experience only one major event per month and that prior events did not impact the probability of subsequent events. Mortality rates were extrapolated using the observed risk at 24 months, assuming it remained constant in future model cycles, potentially overestimating long-term risk and increasing the incremental cost per QALY.
Primary Studies
Evidence for Optimal Medical Therapy (Comparator)
To obtain information on the OMT, data from the REMATCH trial 31 were used. This multicenter RCT evaluated the efficacy of LVADs, specifically the HeartMate VE, in patients with end-stage HF not eligible for transplantation. The study included NYHA class IV patients with contraindications for transplantation, such as advanced age or comorbidities. A total of 129 patients were randomized: 68 received an LVAD, and 61 received OMT.
In the OMT group, with a mean age of 68 ± 8.2 years and 82% male, Kaplan-Meier estimated survival rates were 25% at 1 year and 8% at 2 years, with a median survival of 150 days. Fifty-four deaths occurred, primarily due to end-stage HF. The OMT group had a lower mean rate of serious adverse events (2.75 per patient-year) compared to the LVAD group (6.45 per patient-year). Neurological dysfunction and non-neurological bleeding were significantly lower in the OMT group.
Quality of life outcomes were worse in the OMT group after 1 year, with significant differences favoring the LVAD group in physical function, emotional role, and depression scores. The LVAD group reached a median NYHA class II, while the OMT group remained in class IV.
It is noteworthy that REMATCH used the HeartMate VE, a predecessor of the HM3, which is no longer available. Methodological limitations include the inability to blind due to surgical risks and device presence, potentially introducing biases. Quality of life and functional analyses were conducted per protocol, which may limit general interpretation due to potential selection bias.
HeartMate 3 (Intervention)
Data on the HM3 LVAD were obtained from 4 studies,32 -35 3 of which are results from the MOMENTUM 3 trial. Survival data were extracted from Mehra et al,33,34 while adverse event information came from Goldstein et al, 32 Mehra et al, 33 and Jimenez Contreras et al 35 Quality of life was evaluated based on Goldstein et al. 32
Mehra et al 34 presented a 5-year follow-up of the MOMENTUM 3 trial. In the HM3 group (n = 515), the median age was 62 years, and 79.6% were male. The 5-year survival for DT patients was 54.8%; excluding those who received transplantation, the survival rate was 51.5%. This extension did not include quality of life data.
Mehra et al 33 , including the Continued Access Protocol (CAP) arm, involved 1685 patients, with 75.6% receiving the HM3 as DT. The 2-year survival rate was 79.1%. Hemocompatibility-related adverse events included pump thrombosis (1.1%), strokes (9.1%), and bleeding episodes (50.1%). Non-hemocompatibility-related events included major infections (57.4%), right HF (37.4%), and arrhythmias (33.7%).
Goldstein et al 32 analyzed quality of life and functional status in HM3 patients. At 24 months, 78% reached NYHA class I or II (P < .001). The 6-minute walk distance increased significantly, and quality of life scores improved beyond the minimal clinically important difference.32,37 -40 Adverse events included pump thrombosis (1.9%), strokes (10.7%), bleeding (49.2%), and infections (59.3%).
Jimenez et al 35 conducted a retrospective analysis comparing HMII and HM3 devices. In the HM3 group (n = 252), 96.3% were destination therapy patients. Device replacement occurred in 4.4%, pump thrombosis in 2.4%, and postoperative infections averaged 0.3 per patient.
Ongoing Trial
The SWEdish evaluation of left Ventricular Assist Device (SweVAD) Trial 36 is an ongoing RCT designed to evaluate the HM3 compared to standard medical therapy in patients with advanced HF not eligible for transplantation. The multicenter study in Sweden plans to recruit 80 patients, with a 2-year follow-up to assess survival, quality of life, functional capacity, and cost-effectiveness. Completion is estimated for December 2025.
Cost Analysis
Cost-Effectiveness Studies
The systematic review of cost-effectiveness studies identified 2 relevant analyses.30,41 Both studies evaluated the HM3 in patients with advanced HF not eligible for transplantation in the UK context. The incremental cost-effectiveness ratios (ICERs) ranged from £47 361 to £58 244 per QALY. Considering the UK’s cost-effectiveness threshold of £50 000 per QALY for treatments extending life in patients with short life expectancy, one study concluded the device could be cost-effective with a 97% probability, while the other did not find it cost-effective.
Device Cost Description
The required equipment for implantation and post-discharge care, along with estimated product lifespans and costs, is presented in Table 1. The total cost of required components was PEN 1 074 211.24 (USD 285 694.48, with a conversion rate of 1 PEN = 3.76 USD). Optional components added minimal additional costs (Supplemental Tables S8 and S9), with total costs ranging from PEN 1 074 811.24 to PEN 1 075 899.24 (USD 285 854.05-USD 286 143.41).
Valuation of Required Components for the HeartMate 3.
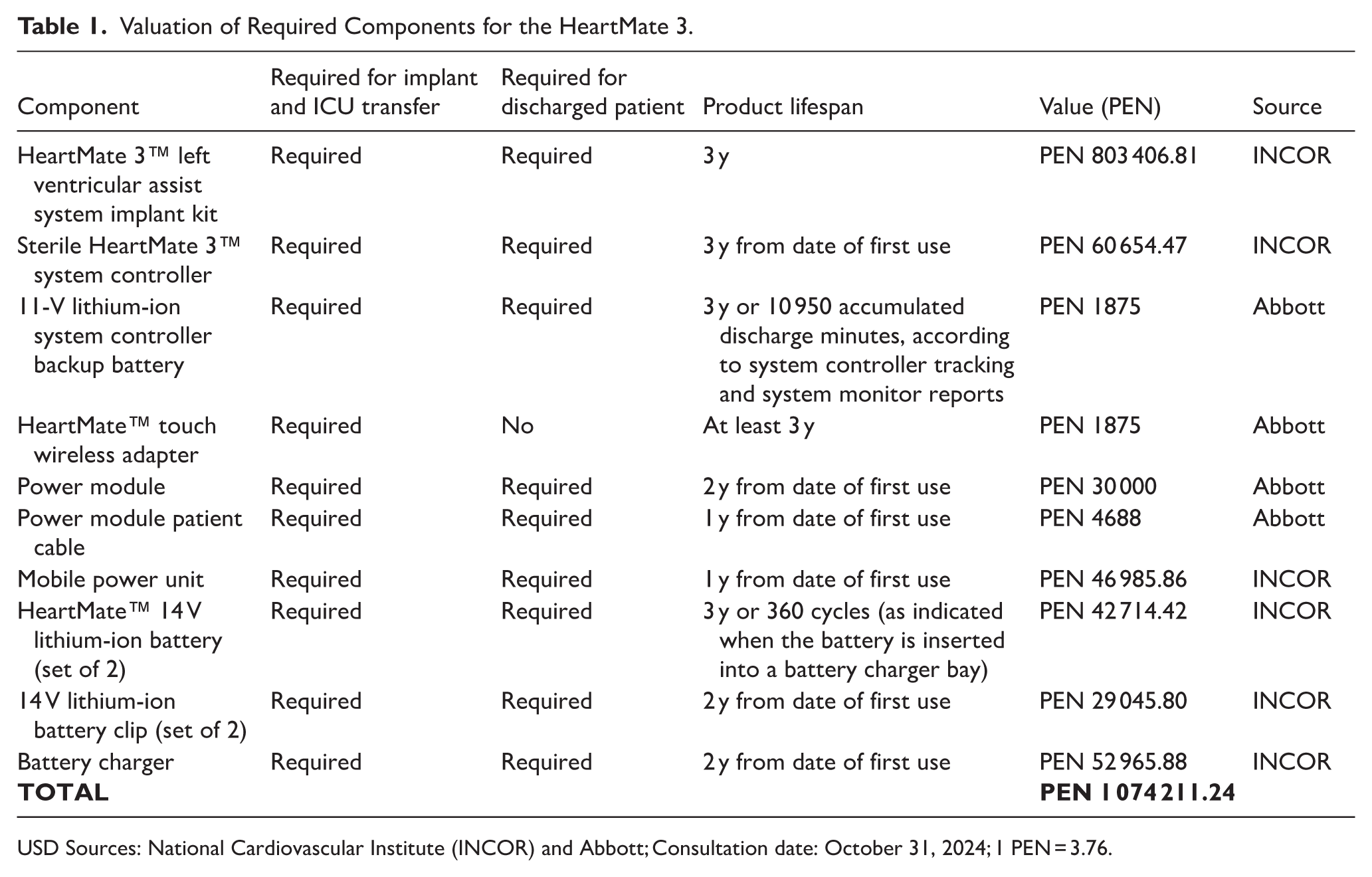
USD Sources: National Cardiovascular Institute (INCOR) and Abbott; Consultation date: October 31, 2024; 1 PEN = 3.76.
Summary of the Methodological Quality of the Evidence
Overall, the evidence base relevant to the PICO question was limited by the absence of direct comparative studies of HM3 versus OMT in patients receiving LVAD as DT. Consequently, comparative inferences relied on indirect evidence, including (i) historical OMT outcomes derived from earlier-generation LVAD trials and (ii) HM3 outcomes obtained primarily from studies comparing HM3 with previous devices and from large observational cohorts. Across HM3 studies, DT subgroup reporting was variably detailed, with some outcomes presented for mixed indications (bridge-to-transplant and DT combined) or without complete DT-specific stratification, which limited interpretability for the target population. In addition, single-arm and retrospective studies were considered only when DT-specific HM3 outcomes were extractable, but these designs remained susceptible to selection bias, confounding, and heterogeneity in baseline risk profiles and follow-up duration.
Regarding evidence sources beyond primary studies, most included CPGs provided structured recommendation classes and evidence levels; however, the supporting evidence frequently included studies of earlier LVAD generations and mixed indications, limiting direct applicability to HM3 used as DT. Conflicts of interest with manufacturers were disclosed in several guidelines and were considered when interpreting recommendations. One guideline presented lower methodological transparency, with limited reporting of the underlying systematic search and an unclear mapping between individual recommendations and cited evidence, which reduced confidence in the reproducibility of its recommendation process. Finally, the included HTA and economic evidence required interpretation in light of modeling assumptions and outcome extrapolation beyond observed follow-up, which introduced additional uncertainty when translating findings to the Peruvian health-system context.
Discussion
Despite limited evidence from studies without direct comparisons, the HM3 LVAD appears to have significant advantages in survival and quality of life for patients with end-stage HF not eligible for transplantation. In the reviewed studies, the 5-year survival rate with the HM3 exceeds 50%, 34 compared to 25% at 1 year and 8% at 2 years with OMT. 31 Significant improvements in functionality and quality of life were observed, including better NYHA classifications, increased 6-minute walk distances, and higher quality of life scores.32 -35
Notwithstanding these favorable outcomes, it is important to acknowledge that the current evidence base is largely derived from indirect comparisons rather than head-to-head trials. Specifically, no contemporary randomized studies directly comparing HM3 with OMT in transplant-ineligible patients are available. Consequently, comparative inferences rely on historical control data and on studies evaluating HM3 in relation to earlier-generation devices or mixed populations. Similarly, the OMT benchmarks used for comparison originate from earlier clinical trials and may not fully reflect current standards of medical management. While this limits the ability to draw definitive causal conclusions, the consistency of findings across multiple data sources, together with biologically plausible mechanisms and concordant improvements in survival and functional outcomes, might support the clinical relevance of the observed benefits in this patient population. Importantly, these limitations do not negate the observed effectiveness of HM3 but underscore the need for cautious interpretation and continued evidence generation.
In EsSalud, patients currently lack therapeutic alternatives beyond conventional medical therapy, as only short-term ventricular assist devices are available. In addition, according to Peruvian healthcare statistics, it is estimated that 2 to 3 patients per year could benefit from the HM3. This highlights the pressing need for effective long-term solutions for patients with end-stage HF who are not eligible for heart transplantation.
The MOMENTUM 3 trial demonstrated HM3′s superior safety profile compared to its predecessor, the HeartMate II.32,34,42 However, potential complications such as hemocompatibility-related adverse events and infections necessitate active medical device surveillance to monitor safety and efficacy in the local context. The ongoing SweVAD Trial, 36 once results are available, may provide additional evidence to reinforce or adjust the current recommendations for HM3’s use in similar population.
Several arguments support the adoption of the HM3 in this setting. Patients with end-stage HF lack destination therapy options beyond medical therapy, and international guidelines recommend long-term LVADs like the HM3 based on studies showing significant survival and quality of life improvements.4,27 -29 Evidence indicates over 50% 5-year survival with the HM3, 34 along with significant functional and quality of life improvements. 32 Although risks exist, these can be managed through appropriate clinical monitoring, reinforcing the importance of medical device surveillance systems.
While cost-effectiveness analyses exceed thresholds typically considered acceptable in high-income settings, investment in this technology could be justified to improve quality and life expectancy for patients without effective treatment options. In Peru, there is not yet an explicit cost-effectiveness threshold nor a formal standard decision rule for funding medical devices, and EsSalud does not apply willingness-to-pay criteria comparable to those used in settings such as the UK. Decisions rely instead on unmet clinical need, evidence of superior efficacy and safety, feasibility of implementation, and expected budget impact. Within this context, the justification for adopting HM3 is grounded both in its potential clinical benefit and in the absence of alternative DT options for transplantation-ineligible patients. Incorporating the HM3 could therefore fill a significant therapeutic gap, offering a clinically effective long-term alternative for patients who currently lack viable treatment options in the Peruvian healthcare system.
Conclusion
Considering the significant benefits in survival and quality of life, along with the lack of alternative therapies for this patient population, the adoption of the HM3 LVAD with active medical device surveillance was considered justified in the Peruvian context. The ongoing SweVAD Trial 36 may provide additional evidence to reinforce or adjust current recommendations once results are available. Additionally, as newer pharmacologic options such as ARNIs or SGLT2 inhibitors continue to expand guideline-directed therapy,43,44 future studies may help clarify whether these advancements have any meaningful impact on outcomes for transplant-ineligible patients with end-stage disease.
Supplemental Material
sj-docx-1-cic-10.1177_11795468261433692 – Supplemental material for Efficacy and Safety of Implantable Left Ventricular Assist Devices for Destination Therapy: A Peruvian Health Technology Assessment
Supplemental material, sj-docx-1-cic-10.1177_11795468261433692 for Efficacy and Safety of Implantable Left Ventricular Assist Devices for Destination Therapy: A Peruvian Health Technology Assessment by Carlos J. Toro-Huamanchumo, Andrea M. Rivera-Santillán, Carolay Z. Vasquez-Quispe, Julissa E. Venancio-Huerta, Lucy J. Gendrau-Castillo, Verónica Peralta, Maribel M. Castro-Reyes and José A. Zavala-Loayza in Clinical Medicine Insights: Cardiology
Supplemental Material
sj-docx-2-cic-10.1177_11795468261433692 – Supplemental material for Efficacy and Safety of Implantable Left Ventricular Assist Devices for Destination Therapy: A Peruvian Health Technology Assessment
Supplemental material, sj-docx-2-cic-10.1177_11795468261433692 for Efficacy and Safety of Implantable Left Ventricular Assist Devices for Destination Therapy: A Peruvian Health Technology Assessment by Carlos J. Toro-Huamanchumo, Andrea M. Rivera-Santillán, Carolay Z. Vasquez-Quispe, Julissa E. Venancio-Huerta, Lucy J. Gendrau-Castillo, Verónica Peralta, Maribel M. Castro-Reyes and José A. Zavala-Loayza in Clinical Medicine Insights: Cardiology
Footnotes
Author Contributions
Conceptualization: CJTH, AMRS, LJGC, VP, MPCR, JAZL; Data curation: CJTH, CZVQ, JEVH; Formal analysis: All authors; Methodology: All authors; Writing – original draft: CJTH, CZVQ, JEVH; Writing – review & editing: AMRS, LJGC, VP, MMCR, JAZL. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.