
Abstract
Background
Obstructive hypertrophic cardiomyopathy (HCM) is defined by left ventricular hypertrophy with outflow tract obstruction. Despite clear guideline-directed medical therapy recommendations from the European Society of Cardiology (ESC), it remains unclear whether real-world treatment aligns with these guidelines. This study evaluates adherence to ESC guidance in Germany, focusing on pharmacological and invasive therapies and identifying gaps in real-world care for patients with obstructive HCM.
Methods
A retrospective cohort analysis was conducted using the WIG2 Benchmark database, containing administrative claims data from German statutory health insurers. Patients aged ≥18 years who received an International Classification of Diseases (ICD)-coded diagnosis of HCM between 2012 and 2018 were included. Treatment alignment was assessed against ESC guidelines on HCM.
Results
Of 6793 patients with an HCM diagnosis, 1141 had obstructive HCM. Mean age was 59.7 years and 62% were male. Following initial HCM consultation, 18% received beta-blocker (BB) monotherapy and 12% received calcium channel blocker (CCB) monotherapy, in accordance with ESC guidelines. However, 43% of treatment combinations were not aligned with the ESC guidelines, including use of contraindicated dihydropyridine CCBs and vasodilating BBs, and 22% of patients did not receive any HCM-related pharmacological treatment. Overall, only 57% of the prescribed treatments were consistent with ESC guidelines for obstructive HCM management.
Conclusions
This study reveals substantial gaps in alignment with the ESC guidelines for obstructive HCM management in Germany, underscoring the need for enhanced clinician education on existing therapies. Greater uptake of guideline-directed medical therapy is critical to improving patient well-being, functional status and outcomes.
Keywords
Introduction
Hypertrophic cardiomyopathy (HCM) is a complex myocardial disorder characterized by left ventricular hypertrophy that cannot be explained by other cardiac or systemic conditions.1-3 This form of cardiomyopathy is associated with significant morbidity and healthcare resource utilization, particularly among patients with obstructive HCM who often present with progressive symptoms and a greater clinical and economic burden than those with non-obstructive HCM. 4
The management of obstructive HCM has evolved substantially over the past decade, with the European Society of Cardiology (ESC) issuing specific guidelines in 2014 and updating them in 2023 to reflect additional pharmacological options derived from randomized clinical trials.5,6 In both the original and updated guidelines, the recommended first-line treatments (Class I B) for symptomatic patients with left ventricular outflow tract (LVOT) obstruction (gradient ≥50 mm Hg) include non-vasodilating beta-blockers (BBs) or non-dihydropyridine (DHP) calcium channel blockers (CCBs). They also recommended avoidance of digoxin and arterial or venous dilators (Class IIa C). In asymptomatic patients, the use of BBs or CCBs can be considered (Class IIb). If these treatments are inadequate, additional therapies such as disopyramide (not available in Germany and many other countries) or newer agents like mavacamten, a cardiac myosin inhibitor, are recommended (Class IIa A). 6 Although the use of disopyramide was included in both original and updated guidelines, the use of mavacamten was only recommended in the updated 2023 guidelines, because it was only approved for use in June 2023. Despite these guideline recommendations, the uptake and alignment with them in routine clinical practice in Germany remains uncertain.
This retrospective cohort study aims to assess whether patients with obstructive HCM in Germany are receiving guideline-directed BB/CCB medical therapies as outlined in the 2014 and 2023 ESC guidelines. Although this is only a theoretical consideration of the 2023 ESC guidelines, which were not published at the time of the study, it provides important insights and an indication of how the treatment strategies during the study period would be evaluated under the current knowledge. This study focuses only on BB/CCB treatment, given that disopyramide is not available in Germany and mavacamten was not yet approved during the study period. By analyzing nationally representative administrative claims data from 2012 to 2018, this study aims to identify treatment patterns, compare the identified treatment patterns with guideline recommendations and evaluate potential gaps in clinical practice. The findings of this study will provide insight into the real-world management of obstructive HCM in Germany and help to identify opportunities for improving patient outcomes through better alignment with evidence-based guidelines.
Methods
Study Design and Data Source
This retrospective cohort study analyzed administrative claims data from a nationally representative cohort of patients in Germany who received a diagnosis of obstructive HCM during the period from 2012 to 2018. We used the WIG2 (Scientific Institute for Health Economics and Health System Research) Benchmark database, which contains comprehensive healthcare claims data from several German statutory health insurance (SHI) providers and was shown to be representative of the German population. 7 This dataset includes diagnostic codes, prescribed medications, procedures, and inpatient and outpatient visits. The data were anonymized and de-identified in compliance with European and German data protection laws, allowing us to perform analyses without the need for written informed consent.
Patients were eligible for inclusion in the study if they met the following criteria. 1. Adults aged ≥18 years at index HCM diagnosis. 2. Received a diagnosis between 2012 and 2018 of obstructive HCM, which was defined as the presence of International Classification of Diseases 10th Revision-German Modification (ICD-10-GM) code I42.1 or a combination of any HCM diagnosis (ICD-10-GM codes I42.2 or I42.9) with documented septal reduction therapy (e.g. alcohol septal ablation or surgical myectomy; operation and procedure classification (OPS) codes 8-837.70 or 5-354.03). 3. At least 1 year of continuous health insurance coverage both prior to and following the index date (i.e. the first obstructive HCM diagnosis received during the study period), ensuring a minimum follow-up period of 12 months.
Patients were excluded if they had received diagnoses suggestive of HCM phenocopies, including aortic stenosis (ICD-10-GM codes I06.0, I06.2, I35.0, or I35.2), hypertensive heart disease (ICD-10-GM codes I11.0 or I11.9), storage diseases (ICD-10-GM codes E74.*, E75.*, E76.*, or Q87.1) or amyloidosis (ICD-10-GM codes E85.4 or E85.8).
The index date was defined as the first recorded date in a quarter when patients met the eligibility criteria for obstructive HCM. Baseline characteristics, including demographic data, comorbidities and prescribed treatments, were assessed at index and during the 12 months prior to the index date. Patients were followed up for a minimum of 12 months from their index date up to the end of their enrolment in the SHI or the end of the study period. Medication use was analyzed based on prescriptions recorded during both the baseline and follow-up periods. Treatments were classified according to their alignment with the 2014 and 2023 ESC guidelines for obstructive HCM. Alignment was defined as the use of guideline-recommended treatments including non-vasodilating BBs (e.g. bisoprolol and metoprolol) and non-DHP CCBs (verapamil and diltiazem); these recommendations were consistent in both guidelines. Disopyramide use was not present in the data as expected, and mavacamten had not been approved before or during the study period. Deviations from the guidelines, including the use of angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), vasodilating BBs or DHP CCBs, were also summarized.
Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. Continuous variables were reported as means with standard deviations, whereas categorical variables were summarized as frequencies and percentages. Data quality management was integrated into the primary processing systems, utilizing Structured Query Language and R for data processing to assess quality metrics. The central statistical software employed by WIG2 for data evaluation was R version 4.1.
Ethics Approval
As this study utilized anonymized retrospective data, it was exempt from formal ethics approval in accordance with the local regulatory requirements; however, the research was conducted following the principles of the Declaration of Helsinki.
Results
Patient Characteristics
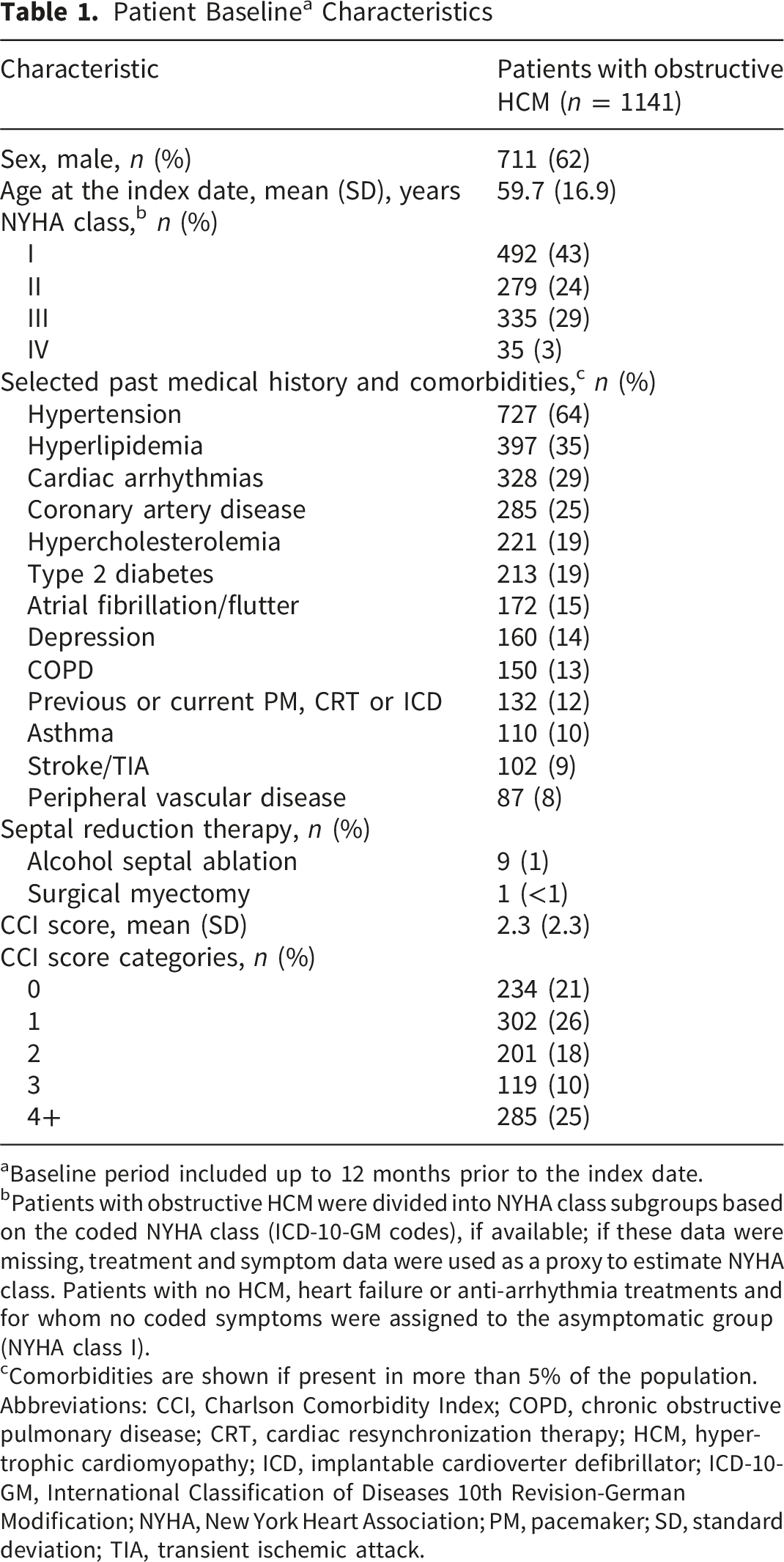
In total, 6793 patients with HCM were identified between 2012 and 2018, of whom 1141 met the inclusion criteria for obstructive HCM (Figure 1). The mean follow-up duration for this cohort was 4.7 years. The baseline characteristics of the patients are summarized in Table 1. The mean age at the index date was 59.7 years, and 62% of the patients were male. Many patients presented with comorbid conditions, with hypertension (64%) and hyperlipidemia (35%) being the most common. The mean (standard deviation [SD]) Charlson Comorbidity Index (CCI) score was 2.3 (2.3). Only a small fraction of the cohort underwent septal reduction therapy. Flowchart of study design and sample selection, showing the inclusion and exclusion criteria used to identify patients with obstructive HCM between 2012 and 2018. HCM, hypertrophic cardiomyopathy; ICD-10-GM, International Classification of Diseases 10th Revision-German Modification; SRT, septal reduction therapy Patient Baseline
a
Characteristics aBaseline period included up to 12 months prior to the index date. bPatients with obstructive HCM were divided into NYHA class subgroups based on the coded NYHA class (ICD-10-GM codes), if available; if these data were missing, treatment and symptom data were used as a proxy to estimate NYHA class. Patients with no HCM, heart failure or anti-arrhythmia treatments and for whom no coded symptoms were assigned to the asymptomatic group (NYHA class I). cComorbidities are shown if present in more than 5% of the population. Abbreviations: CCI, Charlson Comorbidity Index; COPD, chronic obstructive pulmonary disease; CRT, cardiac resynchronization therapy; HCM, hypertrophic cardiomyopathy; ICD, implantable cardioverter defibrillator; ICD-10-GM, International Classification of Diseases 10th Revision-German Modification; NYHA, New York Heart Association; PM, pacemaker; SD, standard deviation; TIA, transient ischemic attack.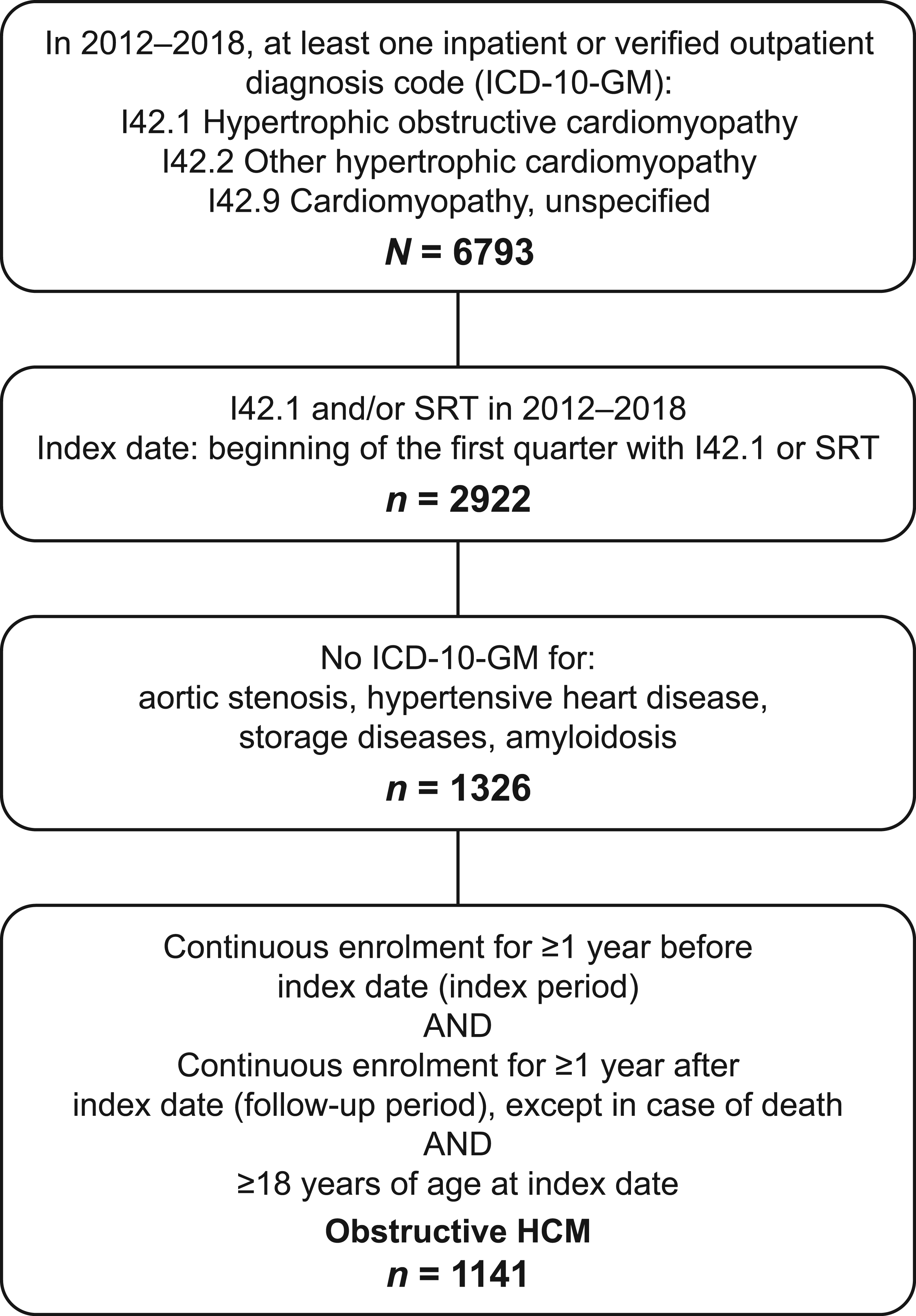
Medication Use at Baseline
Prescribed Medications in Patients With Obstructive HCM at Baseline a
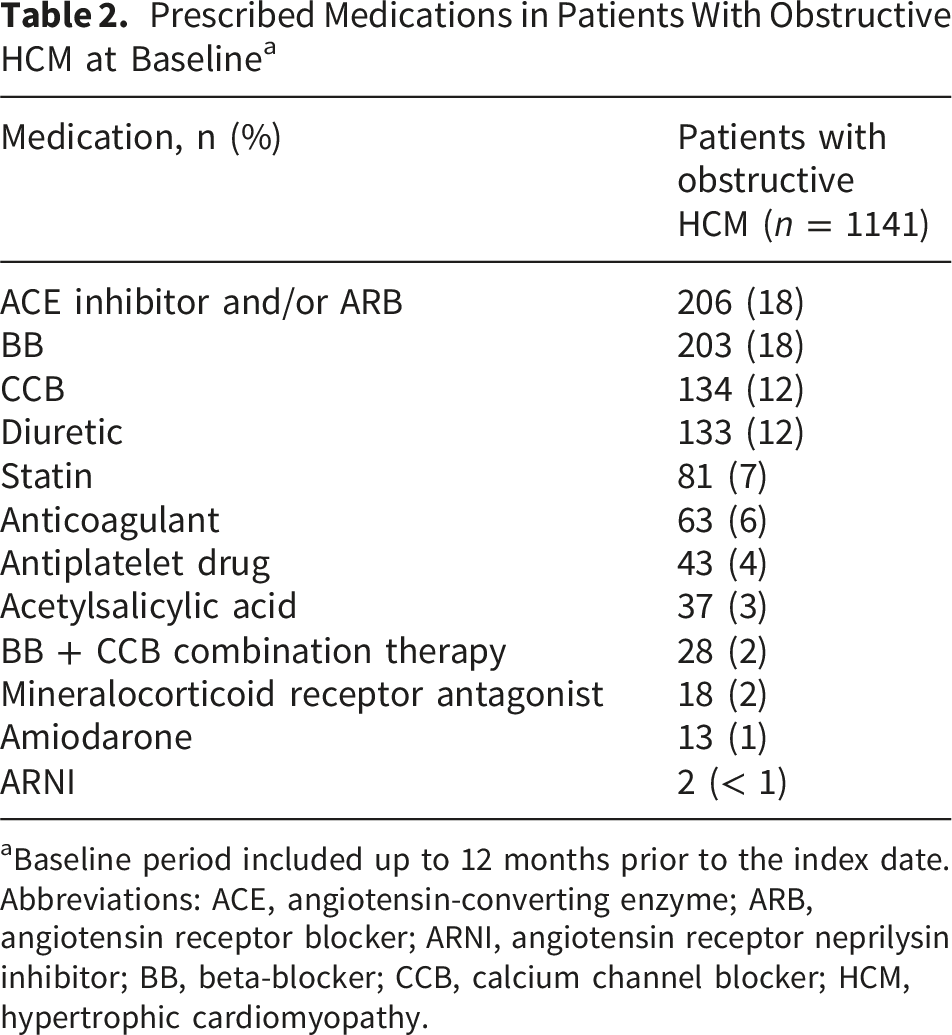
aBaseline period included up to 12 months prior to the index date.
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor neprilysin inhibitor; BB, beta-blocker; CCB, calcium channel blocker; HCM, hypertrophic cardiomyopathy.
Treatment Patterns
After the index obstructive HCM diagnosis, 78% (n = 894) of patients received treatment with monotherapy or combinations (dual/triple therapies) of BBs and/or CCBs. Specifically, 41.5% (n = 473) were prescribed non-vasodilating BB monotherapy and 13.4% (n = 153) received non-DHP CCB monotherapy in accordance with ESC guidelines (Figure 2). The two most commonly prescribed BBs were bisoprolol and metoprolol, prescribed to 21% and 19% of patients, respectively. The two most commonly prescribed CCBs were verapamil and amlodipine, prescribed to 13% and 7% of patients, respectively. Sankey plot of the treatment trajectories of patients with obstructive HCM with prescriptions for non-vasodilating BB monotherapy and non-DHP CCB monotherapy after the index date. The number of occurrences that progressed to the next line of treatment is illustrated using grey lines. BB, beta-blocker; CCB, calcium channel blocker; DHP, dihydropyridine; EOFU, end of follow-up; HCM, hypertrophic cardiomyopathy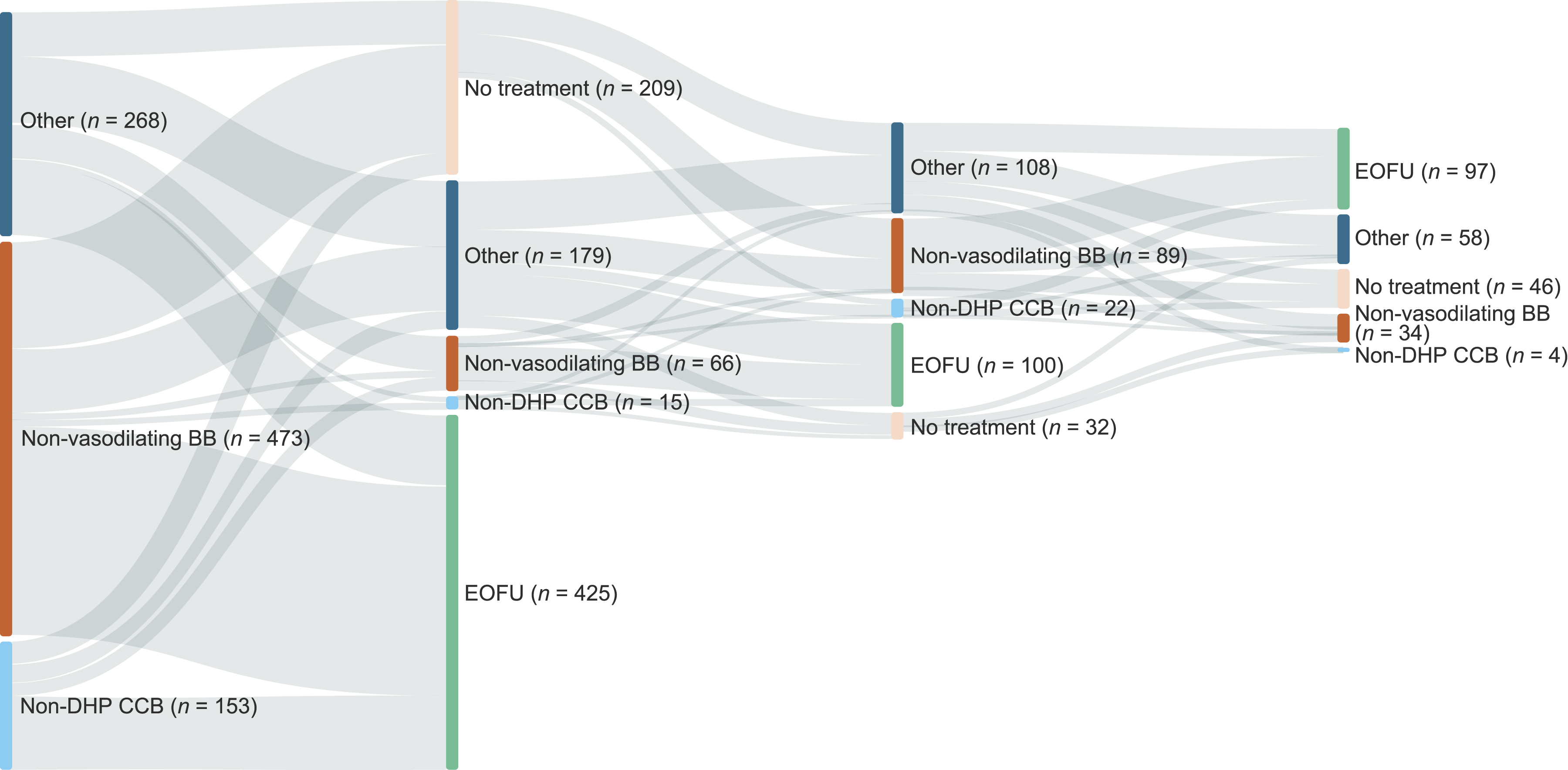
Among patients who changed HCM therapy prior to the end of the follow-up period (n = 469), only 17.3% (n = 81) received guideline-compliant treatment and 44.6% (n = 209) received no HCM-related treatment. Patients who initiated treatment with BB monotherapy were more likely to escalate to combination therapy with CCBs or switch to alternative medications.
Most Frequent Obstructive HCM Treatment Combinations after the Index Date
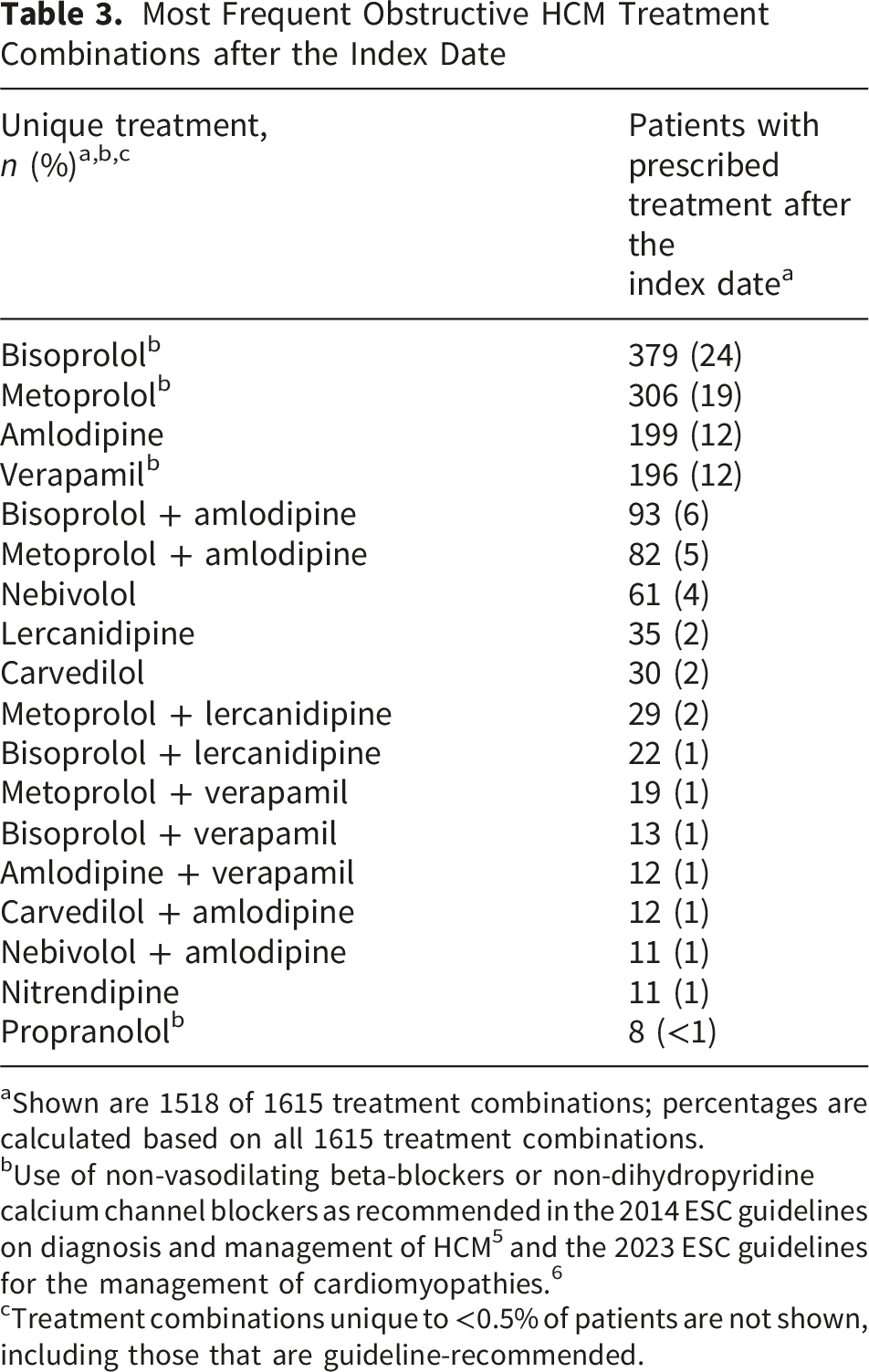
aShown are 1518 of 1615 treatment combinations; percentages are calculated based on all 1615 treatment combinations.
bUse of non-vasodilating beta-blockers or non-dihydropyridine calcium channel blockers as recommended in the 2014 ESC guidelines on diagnosis and management of HCM 5 and the 2023 ESC guidelines for the management of cardiomyopathies. 6
cTreatment combinations unique to <0.5% of patients are not shown, including those that are guideline-recommended.
Alignment With the ESC Guidelines
Overall, 57% of the prescribed pharmacological treatments were consistent with the ESC guidelines for the management of obstructive HCM (Table 3). The most frequent deviation from these guidelines was the use of DHP CCBs, such as amlodipine, which are contraindicated owing to their vasodilating effects. Additionally, some patients received vasodilating BBs, such as nebivolol, which are also not recommended for obstructive HCM. Approximately 43% of the treatment combinations used in the study cohort were not aligned with current guideline recommendations, underscoring the need for improved alignment with evidence-based therapies. Despite the availability of guideline-directed medical therapy, 22% of patients with obstructive HCM were not receiving any treatment for their condition during the entire study period.
Discussion
This study provides a detailed examination of real-world treatment patterns for obstructive HCM in Germany, revealing a gap between clinical practice and guideline-directed medical therapy. Although 57% of HCM-related pharmacological treatments were aligned to ESC guidelines, a substantial proportion of treatments were not in alignment; moreover, patients with obstructive HCM experienced periods with no HCM-related treatments. The ESC guidelines for the management of HCM, first issued in 2014 and subsequently updated in 2023, recommended non-vasodilating BBs or non-DHP CCBs as first-line therapy for patients with symptomatic obstructive HCM.5,6 In our study, the majority of treated patients received these drugs, with bisoprolol and metoprolol being the most commonly prescribed BBs. A notable deviation from the guidelines was the frequent use of DHP CCBs, such as amlodipine, which are not recommended (IIb) because of their vasodilating properties, which can exacerbate LVOT obstruction. 9 In a subset of patients, inappropriate use of other vasodilating therapies, such as ACE inhibitors and ARBs, was also observed. These agents, although useful in other cardiovascular conditions, are not recommended in obstructive HCM, owing to their potential to lower systemic vascular resistance and, thereby, increase the LVOT gradient.9,10 Such prescribing patterns may reflect either therapeutic inertia or limited familiarity with obstructive-HCM-specific treatment guidelines among primary care physicians and non-specialist cardiologists.
The observation that some patients with obstructive HCM experienced periods with no HCM-related treatment or somewhat frequent changes in medication suggests an unmet need and potentially a lack of adequate control of available therapies. The ESC guidelines do recommend disopyramide, a negative inotrope, as a second-line therapy for patients who remain symptomatic despite optimal BB or CCB therapy. 6 However, disopyramide is not available in Germany and many other regions of the world, limiting the therapeutic options for patients with obstructive HCM. Mavacamten, a first-in-class cardiac myosin inhibitor, has emerged as a promising therapy for obstructive HCM by directly targeting the underlying pathophysiology of the disease.11,12 It reduces hypercontractility, alleviating LVOT obstruction. 13 Several clinical trials have demonstrated its efficacy in improving exercise capacity, reducing symptoms and normalizing LVOT gradients and cardiac biomarkers in a large proportion of patients with obstructive HCM.13-15
It is likely that the treatment challenges observed in Germany mirror those in other healthcare systems; studies from Sweden and Denmark have also identified gaps in obstructive HCM-specific knowledge.16,17 Our findings have significant implications for the management of obstructive HCM in Germany and potentially in other regions. The inappropriate use of contraindicated treatments highlight the need for ongoing education and training among healthcare providers. Multidisciplinary approaches involving cardiologists, primary care physicians and specialists in HCM, may be necessary to ensure that patients receive optimal care. Additionally, a relatively low rate of septal reduction therapy was observed despite a substantial proportion of patients with advanced symptoms (NYHA III–IV). While this may indicate potential underutilization of invasive treatment strategies, the lack of detailed clinical data precludes assessment of eligibility for septal reduction therapy, including LVOT gradient severity, treatment response, contraindications, and patient preference. As such, improving referral pathways and access to septal reduction therapy could lead to better symptom control and quality of life for patients whose disease is refractory to pharmacological treatment.
Potential Limitations
Our study has several limitations that should be acknowledged. The retrospective design and the reliance on administrative claims data limit detailed insight into the clinical rationale behind treatment decisions and patient compliance rates. In addition, the study used secondary data primarily collected for reimbursement purposes rather than clinical characterization and as such, may have resulted in an underestimation of the prevalence of obstructive HCM, which is known to be underdiagnosed and misdiagnosed in routine clinical practice. Furthermore, this analysis was conducted before the availability of cardiac myosin inhibitors, which limits its applicability to current treatment practices; however, this timing offers an important baseline to assess current practices and potential deficits before the introduction of an alternative pharmacological therapy. Future studies should incorporate real-world data on mavacamten use and assess its impact on long-term outcomes.
Conclusion
In conclusion, our study reveals considerable gaps in the management of obstructive HCM in Germany, with many patients receiving suboptimal care despite clear recommendations in ESC guidelines. The under-utilization of invasive procedures, coupled with the inappropriate use of contraindicated medications, underscores the need for targeted interventions to improve alignment with evidence-based treatments. Efforts to enhance clinician education, increase access to developed therapies as they become available and improve referral pathways for septal reduction therapy will be critical in optimizing care for patients with obstructive HCM.
Footnotes
Acknowledgements
We would like to acknowledge Yue Zhong of Bristol Myers Squibb for her valuable contributions to data interpretation. We would also like to acknowledge Oxford PharmaGenesis for their support in distributing drafts, assisting with manuscript preparation and editorial assistance under the guidance and direction of the author team, and this was funded by Bristol Myers Squibb. Their expertise and collaboration were instrumental in the completion of this work.
Ethical Considerations
As this study utilized anonymized retrospective data, it was exempt from formal ethics approval in accordance with the local regulatory requirements; however, the research was conducted following the principles of the Declaration of Helsinki.
Author Contributions
All authors contributed to drafting and/or critically reviewing the manuscript, approved the final version and agree to be accountable for all aspects of the work. Carla Zema, Michael Schultze, Nils Kossack and Ervant Maksabedian-Hernandez contributed to conception or design, data acquisition, data analysis and data interpretation. Farbod Sedaghat-Hamedani, Tobias Bluhmki, Taryn Krause, Johanna Schmoelders and Benjamin Meder contributed to conception or design, data analysis and data interpretation. Tarcyane Garcia contributed to data acquisition, data analysis and data interpretation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Bristol Myers Squibb.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Farbod Sedaghat-Hamedani received honoraria for advising Bristol Myers Squibb; participates in clinical trials sponsored by Bristol Myers Squibb; has served as a scientific adviser for Bristol Myers Squibb; and has engaged in the planning and execution of clinical trials for mavacamten. Carla Zema was a contractor for Bristol Myers Squibb at the time the study was conducted. Michael Schultze is an employee of ZEG Berlin, which received funding from Bristol Myers Squibb to conduct this study. Tarcyane Barata Garcia and Nils Kossack are employees of WIG2 GmbH, which received funding from Bristol Myers Squibb to conduct this study. Ervant J. Maksabedian Hernandez, Tobias Bluhmki and Johanna Schmoelders are employees of Bristol Myers Squibb and may own stock in Bristol Myers Squibb. Taryn Krause was an employee of Bristol Myers Squibb at the time the study was conducted. Benjamin Meder received honoraria for advising Bristol Myers Squibb. He also received travel support and speaker honoraria from Bristol Myers Squibb and research support.