
Abstract
Variability in novel inflammatory markers (HBP and SAA) post-surgery could indicate ongoing perioperative inflammation. This pilot cohort study collected blood from 99 patients undergoing elective cardiac surgery at baseline, 24 hours, 7 days, and 3 months post-surgery. Inflammatory markers (HBP, SAA, PCT, CRP, IL-6) were measured with a point-of-care device. Demographic and clinical data were extracted from health records. Serum SAA increased significantly in the acute postoperative phase (Me[IQR];SAAbaseline=81.1[87] vs SAA24hr=232.65[88.02];U[72]=2343,p<0.0001), remained elevated at 7 days (Me7d=252.6[88.56];U[57]=1484,p<0.0001) and were still more pronounced than baseline at t3m (Me3m=118.44[101.52];U[38]=448,p=0.0008). HBP showed a significant rise at seven days (HBPbaseline=45[26;89] vs HBP7d=121[69.75;224.5]; U[56]=805,p<0.0001) then returned to near baseline by t3m(Me3m=32.5[15.75;98.5]). Traditional inflammatory markers PCT, CRP, and IL-6 demonstrated a rapid increase at t24h and plateaued at t7d. None of the biomarkers showed variability at baseline or postoperatively with preoperative status or postoperative complications. Cluster analysis of the inflammatory markers at 24 hours (t24h) identified distinct subgroups. Cluster #1-patients with a modest increase in all markers; Cluster#2 characterized with a robust increase in IL-6; Cluster #3 showed increase in CRP and decline in HBP; Cluster #4 showed a modest increase in IL-6 and decline in HBP; Cluster #5 represented a decline in both CRP and SAA. Patients in these clusters differ with respect to age, pre-existing peripheral artery disease, and borderline differences in perioperative acetaminophen use. SAA and HBP remain elevated longer than IL-6, CRP, and PCT after surgery, suggesting that inflammation may persist beyond 3 months.
Keywords
Introduction
Surgical procedures elicit a robust and complex immunological response primarily triggered by the release of danger signals from injured tissues.1-5 This early inflammatory response is highly heterogeneous across individuals and plays a critical role in determining short- and long-term outcomes.6-9 Numerous inflammatory biomarkers have been studied in the perioperative context, with C-reactive protein (CRP), procalcitonin (PCT), and interleukin 6 (IL-6) being the most extensively investigated.10-15 However, relying on a single or limited set of biomarkers may oversimplify the complexity of the host immune response and inadequately capture the pathways that influence long-term recovery.16,17
Several classical markers of the inflammatory response have been extensively studied in surgical settings.2,7,9-16 Among them, procalcitonin (PCT) is a well-established biomarker primarily used to guide antibiotic therapy in septic conditions, including surgical populations.16,18,19 PCT levels typically rise within 4-6 hours following surgery and return to baseline within 24 hours, provided there are no infectious complications. In some cases, PCT levels may persist until postoperative day five.13,18,20 Despite its utility in monitoring bacterial infection and treatment response, PCT has not demonstrated predictive value for the development of secondary infections. 12 Interleukin 6 (IL-6) is another widely investigated marker that responds to a range of pathological conditions, including myocardial injury during cardiac surgery.9,21,22 IL-6 exhibits a rapid peak in the early postoperative period, often preceding both CRP and PCT, but tends to normalize quickly in the absence of further complications.15,23-25 Several factors influence postoperative IL-6 serum levels, including the extent of surgical trauma, preoperative IL-6 levels, and preoperative medication intake.14,21,23,26-28 CRP, an acute-phase reactant synthesized by the liver in response to IL-6 signaling, is released rapidly following tissue injury.8,29 Most studies have reported that CRP peaks shortly after surgery and typically declines by postoperative day six.30-32 However, sustained elevations in CRP have been linked to unfavorable outcomes (myocardial fibrosis, others) in both cardiac and non-cardiac surgical patients.7,11,33,34 Despite their widespread use, existing studies of CRP, IL-6, and PCT have generally documented rapid resolution of elevated levels, with some heterogeneity in inflammatory responses.10,12,13,15,20,24,31,35 Importantly, these investigations have rarely extended biomarker sampling beyond the first postoperative week, limiting insight into longer-term inflammatory dynamics.
In recent years, alternative biomarkers have gained attention as potential complements or substitutes for classical inflammatory markers. Heparin-binding protein (HBP), a mediator stored in neutrophil granules, is released during bacterial sepsis and various non-specific inflammatory conditions.36-38 One of HBP’s most significant physiological effects is the induction of increased vascular permeability and activation of the immune system. 39 Its serum levels are influenced by a range of clinical factors, including renal function (creatinine levels), severity of critical illness, high logistic EuroSCORE, and reduced left ventricular ejection fraction.40,41 Intraoperative HBP concentrations also vary with surgical complexity, surgical type, the use of cardiopulmonary bypass (CBP), and heparin use.41-43 However, the long-term postoperative trajectory of HBP remains poorly understood, as existing studies have limited observation periods of up to 24 hours. 42 Understanding the long-term dynamics of HBP is useful, as sustained elevations may have prognostic value not only for perioperative sepsis or enhanced capillary leak but also for the development of atherosclerosis, myocarditis, and myocardial ischemia.36,39,42-45
Another emerging inflammatory marker is serum amyloid A (SAA), an apolipoprotein primarily synthesized by the liver.35,46 SAA plays diverse biological roles, including regulating leukocyte trafficking, modulating lipid metabolism, and contributing to tissue remodeling. 47 Postoperative SAA levels rise rapidly and may remain elevated for longer than seven days. Importantly, elevated SAA has been associated with adverse outcomes in coronary artery disease and with postoperative complications, highlighting its potential as a prognostic marker in surgical populations.48,49
We evaluated the longitudinal dynamics of serum amyloid A (SAA) and heparin-binding protein (HBP) following cardiac surgery with cardiopulmonary bypass, given their emerging roles in inflammation and tissue repair.10,36,38,39,45,47,48,50 Building on prior studies limited to the immediate postoperative period, we extended the observation window beyond 24 hours to better characterize the sustained inflammatory response. We further assessed whether perioperative trajectories of SAA and HBP parallel those of established inflammatory markers, including C-reactive protein (CRP), procalcitonin (PCT), and interleukin-6 (IL-6). We hypothesized that SAA and HBP would return to preoperative baseline levels within 7 days after surgery, consistent with the temporal patterns observed for conventional inflammatory markers. Finally, we explored the heterogeneity of the established (CRP, PCT, IL-6) and novel (HBP, SAA) inflammatory markers over time.
Methods
Study Population
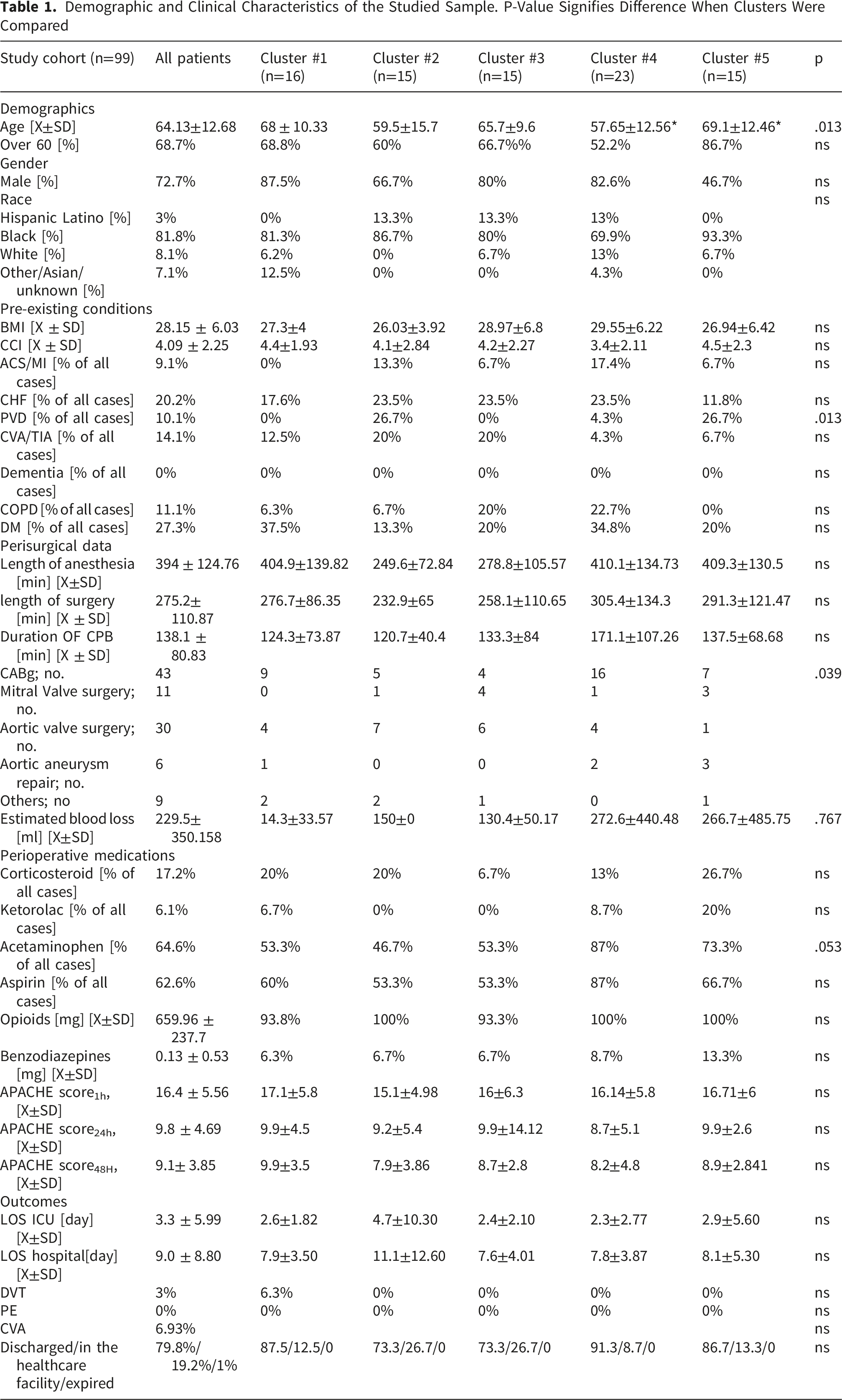
Demographic and Clinical Characteristics of the Studied Sample. P-Value Signifies Difference When Clusters Were Compared
Sample Collections and Analysis
Blood samples were collected at four time points: prior to surgery (baseline), at 24 hours (acute inflammation), 7 days (early recovery), and 3 months (late recovery) postoperatively. The collection period spanned from 2015 to 2020 at a major academic surgical center in the United States. Samples were drawn using BD Vacutainer tubes containing EDTA as an anticoagulant. Within two hours of collection, the tubes were centrifuged at 2000 x g for 10 minutes at 4°C. The resulting serum was aliquoted and stored for further analysis. All processed samples were free of visible hemolysis.41,51
Inflammatory biomarkers—including heparin-binding protein (HBP), serum amyloid A (SAA), interleukin-6 (IL-6), C-reactive protein (CRP), and procalcitonin (PCT)—were quantified using a commercially available, fully validated, and standardized platform according to the manufacturer’s guidelines (Joinstar Biomedical Technology Co, Ltd; Hangzhou, The People’s Republic of China). The platform’s performance has been previously validated against conventional ELISA methods. 51 Detection ranges were as follows: PCT (0.05-36.72 mcg/ml), IL-6 (3-370.5 pg/ml), CRP (0.5-200), HBP (6-300 ng/ml), and SAA (3-300 mcg/ml). To preserve the platform’s operational fidelity, samples were not diluted when values exceeded the detection limit. In such cases, values were capped at the maximal detectable threshold.
Demographic and clinical data were extracted from electronic health records to provide a comprehensive overview of each patient’s medical background. The Charlson’s Comorbidity Index (CCI) was calculated to assess chronic disease burden. Acute Physiology and Chronic Health Evaluation II (APACHE II) scores were recorded at 1 and 24 hours postoperatively to estimate illness severity. Acute kidney injury was defined according to the RIFLE criteria. 52 Documentation of pre-existing or emergent deep venous thrombosis (DVT) and pulmonary embolism (PE) was obtained from the electronic medical records (EMR).
Statistical Analysis
Normality of variable distributions was assessed using the Shapiro-Wilk W test and visual inspection of distribution plots. Parametric variables were expressed as mean (X) ± standard deviation (SD) and compared using t-student statistics (t;[n]). Non-parametric variables were presented as median (Me) with interquartile ranges (IQR:[ 25%;75%]) and analyzed using the U-Mann-Whitney [n;d∫]. For paired comparisons of non-parametric data, the Wilcoxon test (W[n]) was employed. Bonferroni correction\ was applied to adjust for multiple comparisons when appropriate. All analyses involving repeated measures were treated as dependent paired samples with p adjusted using Bonferroni methods when data availability allowed. Unsupervised k-means clustering was performed without predefined initial centers. The number of clusters was determined by a combination of the elbow technique and statistical analysis. Laboratory values for each analyte were standardized using Z-scores for relevant calculations. Correlation momentum was calculated as a r 2 -Pearson. A double-sided p-value less than 0.05 was considered statistically significant for all analyses. Statistical analyses were performed with Statistica 11.0 (StatSoft Inc., Tulsa, OK, USA) or Statistical Package for the Social Sciences v. 26 (IBM, Amon, NY, USA.
Results
Sample Characteristics
Demographic and clinical characteristics of the 99 patients enrolled in the study are presented in Table 1. At baseline, there were no statistically significant differences in inflammatory marker levels based on sex, race, or age >60 years. Additionally, the Charlson Comorbidity Index (CCI) did not show significant correlations with any of the five inflammatory markers assessed. While IL-6 exhibited a borderline association with CCI (r 2 =0.03;p=0.071), this did not reach statistical significance.
Common pre-existing conditions, including congestive heart failure, diabetes mellitus, peripheral vascular disease, chronic obstructive pulmonary disease, history of cerebrovascular events, and body mass index (BMI), were not associated with baseline variations in any of the inflammatory markers.
Perioperative Dynamics of Classical Inflammatory Markers
Procalcitonin (PCT) showed a statistically significant increase at 24 hours postoperatively (W [33]=449; p<0.0001) but returned to near baseline levels by postoperative day 7 (W[31]=179; p<0.079) (Figure 1C). The 24-hour PCT elevation was largely driven by a subset of patients with marked individual increases (Supplemental Material 1). C-reactive protein (CRP) exhibited a robust increase both in the acute and early recovery phases following surgery (W[64]=1928; p<0.0001 at 24 hours; W[59] =1366, p<0.0001 at 7 days) (Figure 1B). Interleukin-6 (IL-6) was significantly elevated in the acute postoperative period (W[31]=496; p<0.0001) and remained elevated through day 7 (W[26] =307;p<0.0001), with levels returning to baseline by 3 months (Figure 1A). Correlation analysis revealed a strong positive relationship between IL-6 and PCT at both 24 hours and 7 days post-surgery (Figure 1D,E), while CRP showed a more modest correlation with either marker. Trends and correlation of IL-6 (A), CRP (B), and PCT (C) at baseline, 24 hours, 7 days, and 3 months following cardiac surgery. * Signifies statistical difference below 0.05 when compared to baseline level. Correlation coefficients at 24 hours (D) and 7 days (E) were presented between clinical markers. Bolded are the statistically significant correlations, and the background color reflects the strength of the correlations
The type of surgery performed did not significantly influence postoperative levels of PCT, CRP, or IL-6 except for CRP, which was lowest among patients undergoing coronary artery bypass grafting (CABG) (Supplemental Material 2). No significant correlations were observed between inflammatory marker levels and intraoperative variables, including duration of anesthesia, total surgical time, or cardiopulmonary bypass duration.
The use of perioperative medications (corticosteroids, ketorolac, benzodiazepines, or opioids) had no measurable effect on PCT, CRP, or IL-6 levels (data not shown). However, intraoperative acetaminophen administration was associated with lower serum CRP levels at 24 hours postoperatively (CRPAcetoPOS+=42.58[10.26;78.14] vs CRPAcetoNEG= 88.26[29.49;118.56]; U[385.5];p=0.008). PCT and CRP levels did not correlate with perioperative intake of benzodiazepines or opioids.
APACHE II scores at 1 hour and 24 hours, as well as the length of hospital and intensive care unit (ICU) stay, did not show significant correlations with CRP or IL-6 levels measured at either 24 hours or 7 days postoperatively. However, PCT levels at 7 days demonstrated a moderate positive correlation with APACHE II scores at 24 hours (r 2 24hrs=0.41; p=0.018). Due to the low overall mortality in the cohort, we were unable to assess associations between inflammatory biomarkers and mortality. However, analysis of discharge disposition revealed that patients not directly discharged home, either transferred to a facility or readmitted, had significantly higher PCT levels at 24 hours compared to those discharged home. PCT (PCTDispHome=0.68[0.35;2.45] versus (PCTDisp-other=3.33[1.96;12.41]; KW [5.68]; p=0.017).
Perioperative Variability of HBP
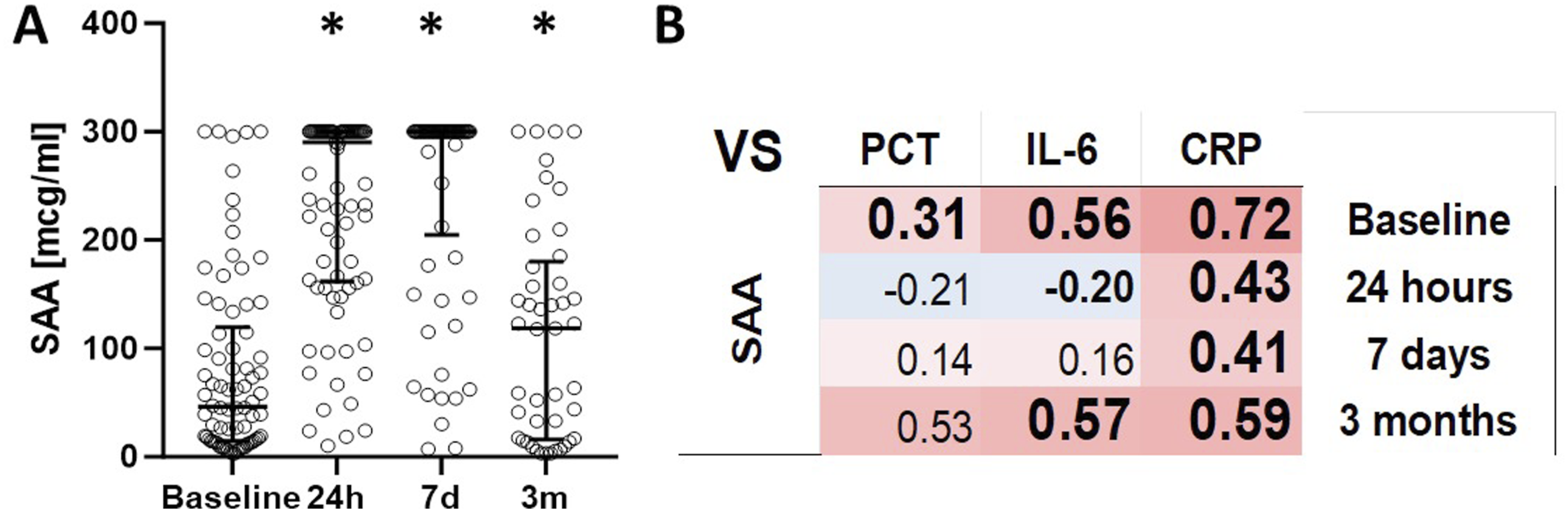
Substantial interindividual variability was observed in baseline HBP levels (Figure 2A). A significant increase in HBP was noted at 7 days postoperatively (W[45]=805;p<0.0001) (Figure 3A; Supplemental Material 3). Although HBP levels decreased by 3 months (MW [59;26]=507;p=0.0125), the reduction was not statistically significant in the pairwise analysis (W[15]=16;p=ns), likely due to the limited number of matched samples (Supplemental Material 3). At 24 hours and 3 months post-surgery, HBP levels demonstrated a significant positive correlation with CRP (Figure 3B). Based on quartile distribution analyses aligned with previous reports, the upper 75th percentile thresholds for HBP were determined as follows: 83 ng/mL preoperatively, 103 ng/mL at 24 hours, 203 ng/mL at 7 days, and 63 ng/mL at 3 months (Supplemental Material 4). Trends and correlation of HBP (A) at baseline, 24 hours, 7 days, and 3 months following cardiac surgery. * Signifies statistical difference below 0.05 when compared to baseline level. Correlation coefficients at 24 hours, 7 days, and 3 months were presented between clinical markers (B). Bolded are the statistically significant correlations, and the background color reflects the strength of the correlations Trends and correlation of SAA (A) at baseline, 24 hours, 7 days, and 3 months following cardiac surgery. * Signifies statistical difference below 0.05 when compared to baseline level. Correlation coefficients at 24 hours, 7 days, and 3 months were presented between clinical markers (B). Bolded are the statistically significant correlations, and the background color reflects the strength of the correlations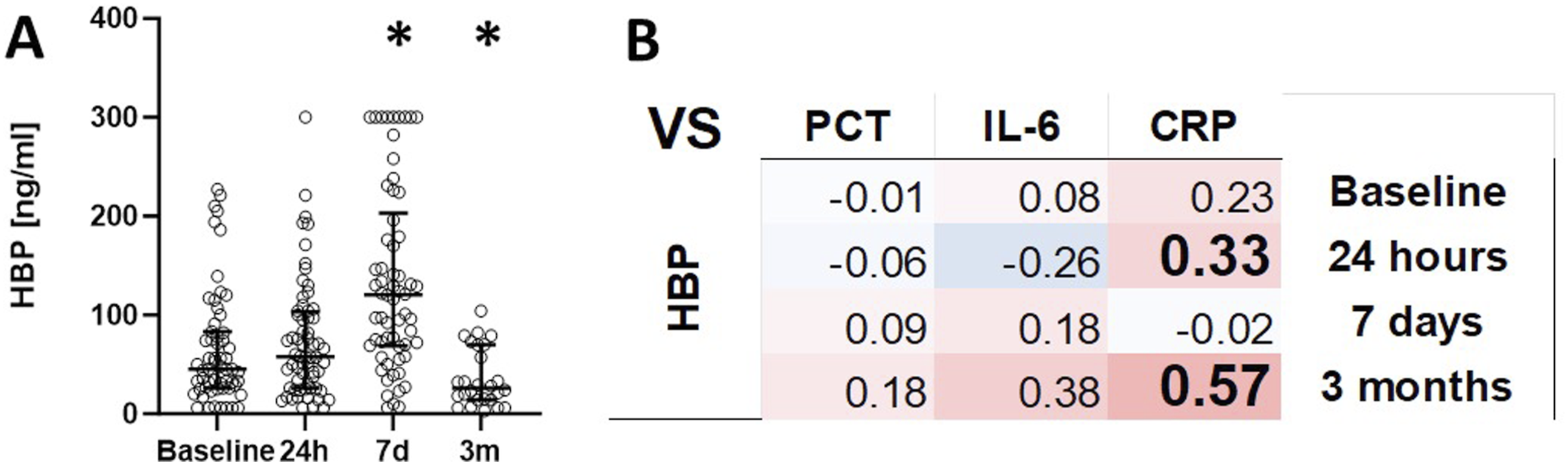
No significant correlations were found between HBP levels and intraoperative variables, including duration of anesthesia, surgical time, or time on cardiopulmonary bypass. Similarly, perioperative administration of corticosteroids, ketorolac, acetaminophen, benzodiazepines, or opioids had no measurable impact on HBP concentrations at either 24 hours or 7 days.
HBP levels at 7 days did not correlate with APACHE II scores at 1 or 24 hours. Additionally, neither hospital nor ICU length of stay was associated with HBP values. Finally, discharge disposition was not significantly related to HBP levels at any postoperative time point.
Given HBP’s role in modulating vascular permeability and its potential link to renal dysfunction, we examined the association between postoperative acute kidney injury (AKI) and serum HBP levels.43,51 At 24 hours postoperatively, patients who developed AKI exhibited higher mean serum HBP levels in a one-sided comparison (p=0.027). However, due to the limited sample size, we were unable to perform meaningful statistical comparisons of HBP levels at 7 days and 3 months between the AKI and non-AKI groups. Of note, 7 out of 8 patients who developed AKI had pre-existing chronic kidney disease (CKD), indicating that the observed AKI likely represented an acute worsening of underlying renal impairment. When comparing the baseline HBP levels between patients with CKD and those with normal renal function, no statistically significant difference was found (Me[IQ] NoCKDHBP=44.5[25.75;103.75] versus CKDHBP=59.5[26.5;7103.75]; p=0.472).
Considering the potential influence of heparin on serum HBP levels, we examined whether anticoagulation therapy in patients with deep venous thrombosis (DVT) and pulmonary embolism (PE) was associated with altered HBP concentrations. We identified 6 patients with preoperative PE and 9 with DVT. No cases of postoperative PE were observed, although 3 new DVT events occurred following surgery. Due to limited sample sizes, we focused our analysis on baseline HBP levels prior to surgery. Patients with a pre-existing diagnosis of DVT or PE exhibited significantly higher baseline HBP levels compared to those without thromboembolic disease (MeNominalHBP=43.5[25.75:79.25] vs MeDVT& PEHBP=128[90.75:192.25]).
Perioperative Variability of SAA
Substantial interindividual variability was observed in baseline serum SAA levels (Figure 3A). Following surgery, SAA levels remained significantly elevated across all postoperative time points: at 24 hours (W [72]=2343; p<0.0001), 7 days (W[57]=1484; p<0.0001), and 3 months (W[38]=449; p=0.0008) (Figure 2A). Among the classical inflammatory markers, CRP demonstrated the strongest correlation with SAA levels across all measured time points (Figure 3B)m, suggesting overlapping inflammatory trajectories.
The duration of anesthesia, total surgical time, or duration of cardiopulmonary bypass did not influence serum SAA at any point (data not shown). Similarly, perioperative administration of corticosteroids, ketorolac, acetaminophen, benzodiazepines, or opioids had no measurable effect of serum SAA concentrations. No significant correlations were observed between SAA levels at 24 hours or 7 days, and APACHE II scores at 1 hour and 24 hours, or hospital or ICU length of stay. Furthermore, SAA levels at any measured time point were not associated with discharge disposition or hospital readmission rates.
Normalized Dynamics of Inflammatory Markers Reveal Distinct Time-Course Patterns
To better characterize the temporal dynamics and interplay between inflammatory markers, values for each analyte were normalized using Z-scores. This approach revealed distinct time-course patterns across the markers. Both PCT and IL-6 exhibited an early peak at 24 hours postoperatively, with PCT showing relatively modest dynamic range overall. CRP levels rose at 24 hours and remained elevated through 7 days before returning to near baseline by 3 months. Notably, SAA closely mirrored CRP’s trajectory. In contrast, HBP followed a delayed pattern, with its peak occurring at 7 days, when levels of other markers were already in decline (Figure 2), underscoring its unique time-course profile.
To further investigate whether early inflammatory responses could predict recovery trajectories, we analyzed the distribution of perioperative inflammatory markers. Because HBP, SAA, IL-6, and CRP exhibited nonparametric distributions (Figure 4), they were included in an unsupervised clustering analysis, whereas PCT, which showed limited variability and fewer outliers, was excluded. When the acute response underwent cluster analysis, it demonstrated five distinct cluster centers (Figure 5A–B): Cluster #1 (ALL↑; Modest elevation in all markers), Cluster #2 (Marked IL-6 response), Cluster #3 (Moderate CRP increase with HBP decline), Cluster #4 (Moderate IL-6 increase with HBP decline), and Cluster #5 (Decrease in both CRP and SAA). These clusters were largely similar in baseline demographics and clinical characteristics (see Table 1), except for Cluster #2, which differed on specific variables. However, their perioperative and postoperative biomarker trajectories showed clear distinctions (Figure 6), suggesting heterogeneous immunological recovery profiles despite comparable baseline features. The analysis of normalized values of PCT, IL-6, CRP vs SAA or HBP demonstrated distinctive abnormalities in the time course. All values were normalized to Z-score Distribution of the markers among the patient showed significant heterogeneity in all of them except procalcitonin (A). Utilizing remaining markers, 5 centers of clustering were identified at 24 hours mark (B) Trajectories of the inflammatory markers expressed as Z-scores across five clusters. In cluster #2, the dynamics of IL-6 exceeded the scale by 24 hours


Discussion
The principal finding is that serum amyloid A (SAA) and heparin-binding protein (HBP) follow distinct perioperative trajectories after cardiac surgery, diverging from canonical inflammatory markers (IL-6, CRP, PCT). SAA mirrored CRP, with a rapid postoperative rise and sustained elevation, consistent with an acute-phase response. By contrast, HBP showed a delayed, biphasic pattern, with no early increase, peaking at day 7 and normalizing by 3 months. This temporal dissociation suggests that HBP reflects later-stage immunological or tissue-repair processes not captured by conventional markers. Because most patients recovered smoothly, the observed markers may indicate a new equilibrium or incomplete recovery.
The perioperative evolution of serum HPB in this study was marked by a delayed increase at 7 days, followed by a decline below baseline levels at 3 months. Although earlier studies at earlier time points demonstrated similar findings and cross-validated our results, this is a novel finding: persistent alterations in HBP persist even at a 3-month observation period.41-43 This biphasic pattern represents a novel finding that extends current understanding. We can only speculate on the origin of the initial HBP spike. It is accepted that serum HBP is released by activated neutrophils, suggesting that the absence of an early peak and subsequent depletion at three months may reflect decreased long-term neutrophil activation. 45 The delayed peak at 7 days may instead originate from macrophage and monocyte activity, an alternative and often underrecognized source of HBP. 53 Unlike neutrophils, monocytes and macrophages exhibit longer-lived activation and turnover following surgery, which may explain the observed temporal divergence. Such a shift would alter the secretion patterns of other cytokines, which we did not measure. Furthermore, other tissues, such as the heart and lung, have been implicated as sources of HBP. 41 Endothelium could be a significant source, and vasculitis is quite common in the aftermath of cardiac surgery.20,44,45 As injury and stress to these organs are significant during the perioperative period, they may contribute to elevated serum HBP levels. The 3-month decline in HBP remains less well understood. Serum HBP levels varied substantially among individuals, a pattern consistent with prior research.38,40,43,44,51 This variability may be driven by inherited differences or by perioperative factors not fully captured in our dataset (e.g., heparin or protamine dose, changes in CBP hardware, diuretic use perioperatively). While anticoagulation therapy (e.g., for DVT or PE) could theoretically influence HBP levels, these conditions were present in only a tiny minority of patients. Moreover, the use of surgical heparin is highly standardized, making it less likely to account for the observed variability. Furthermore, we could not control the use of protamine or other heparin-neutralizing agents, which may have indirect effects on serum HBP levels. An alternative explanation for the observed depletion of HBP at three months is prolonged deactivation or phenotype switching of monocytes toward an M2-like state during the healing phase. 53 Though an attractive hypothesis, our methodology was not designed to assess markers of different monocyte phenotypes. Persistence of HBP may reflect other perioperative inflammatory complications (pericarditis) or ongoing vascular remodeling, but our observational cohort study did not collect these data. The clinical implications of these biphasic HBP dynamics remain uncertain, as this study was not powered to explore clinical outcomes. Nevertheless, one might speculate that the peak in HBP at 7 days could contribute to increased vascular permeability and fluid accumulation mechanisms reminiscent of the capillary leak seen in sepsis. 39 Further research is warranted to clarify its relevance in conditions characterized by prolonged inflammation or vascular dysfunction, such as chronic anticoagulation, extracorporeal support, or the presence of heparin-coated implants.37,50,54 The clinical significance of HBP changes needs to be defined as incomplete recovery or the emergence of a novel post-operative homeostasis. Establishing the long-term trajectory and functional significance of HBP will be critical in understanding its role in surgical recovery and its potential as a biomarker or therapeutic target. Perioperative conditions, including those that determine the extent of peri-surgical stress, did not correlate with the dynamics of HBP and SAA. It is possible that surgical insult may be severe enough to induce maximal response initially. Alternatively, some suggest that direct injury to the heart is the primary source of insult. 21 We also did not measure reperfusion injury.22,26 Therefore, lack of correlation may stem from the fact that we did not capture perioperative factors affecting SAA and HBP. Finally, we could account for interference for hardware coated with heparin. 54 However, we demonstrated a relationship between SAA, HBP, and other classical inflammatory factors, as described previously.17,40,46
Our study demonstrated that SAA levels remained consistently elevated throughout the entire observation period, including at 3-months post-surgery. To our knowledge, this is the first study to document such prolonged elevations of SAA in the context of elective cardiac surgery, thereby expanding existing knowledge on SAA beyond its established role in sepsis-related inflammation. 35 This persistent elevation aligns with the concept that SAA is part of the acute-phase response to tissue injury; however, its sustained presence long after the resolution of acute inflammation suggests a potential role in longer-term recovery processes.46,48,55,56 Unlike CRP, a prototypical pentraxin that typically normalizes within 30 days postoperatively, SAA appears to follow a different trajectory.31,35 Although both proteins belong to the same family of acute-phase reactants, their biological functions are distinct, which may explain their differing perioperative dynamics.7,8,11,17,31,35 This divergence raises the possibility that SAA reflects not only inflammation but also ongoing tissue remodeling, immunomodulation during recovery or new balance after surgery.35,46,47,55 Alternatively, undetected pathogen-driven responses or unmeasured perioperative factors may have contributed to its sustained elevation. Glucocorticoid signaling represents a plausible influence, given its regulatory role in SAA expression; however, endogenous steroid levels were not assessed, and the impact of exogenous steroid administration could be determined from available data but their biological impact is unknown. Despite its high serum abundance and presumed protective or regulatory functions, the physiological role of SAA remains incompletely characterized.46-48 Its broad expression and involvement in multiple pathways suggest it may participate in nonspecific or systemic responses. Notably, elevated SAA levels have been associated with outcomes in patients undergoing coronary angiography or experiencing acute coronary syndromes; however, these findings require further replication and validation.46-48
The extended dynamics of some markers observed in our cohort challenge the conventional assumption that surgical recovery concludes within 28–30 days. The extended observed patterns may reflect a delayed or incomplete return to pre-surgical homeostasis, thereby challenging the conventional assumption that recovery is largely achieved within 28 days. Alternatively, they may indicate that perioperative stress induces a sustained shift toward a new physiological equilibrium rather than a simple reversion to baseline. Both scenarios may exist, even though their clinical impact is unclear despite evidence of their prognostic value in sepsis.35,38,48
The perioperative trajectories of classical inflammatory markers in our study were largely consistent with previously published findings, particularly during the acute postoperative period. 35 As expected, PCT exhibited a transient elevation, peaking early and returning to baseline within 7 days.12,13,18,20 Both CRP and IL-6 remained elevated during the early recovery phase but normalized by 3 months, reflecting their roles in the sustained but resolving immune response associated with tissue repair and healing.7,10-12,15,24 Overall, the behavior of these classical markers met expectations based on their well-established roles in postoperative inflammation. The correlation between CRP and SAA observed in our data mirrors previous reports describing similar patterns between CRP and other members of the pentraxin family, such as pentraxin 3.17,35 CRP and SAA, while functionally distinct, appear to be tightly interconnected within the acute inflammatory response. These possibilities raise important questions regarding the biological and clinical significance of prolonged SAA elevation in the postoperative setting. It remains unclear whether such persistence represents ongoing subclinical inflammation, an adaptive response, or a marker of altered healing trajectories. Addressing these uncertainties will require well-designed mechanistic and longitudinal studies capable of capturing dynamic changes over time and linking them to meaningful clinical outcomes. Such efforts will help clarify their potential role in guiding postoperative monitoring, risk stratification, and clinical decision-making, thereby improving their translational relevance in surgical care. 46
An intriguing finding of this study was the heterogeneity of inflammatory responses revealed by cluster analysis, which identified distinct trajectories among the five markers. Notably, SAA and HBP demonstrated divergent dynamics compared to the classical markers, which appeared largely redundant, particularly in the early postoperative period. These results highlight the value of multiplexed inflammatory profiling. Our findings underscore the need for expanded dynamic range in future cartridge designs to more accurately capture the full spectrum of inflammatory marker concentrations during acute illness. Interestingly, while short-term clustering patterns highlighted variability in inflammatory responses, differences between clusters diminished over the long term. This suggests that while acute inflammatory phase dynamics may reflect individualized immunological responses, they may converge during recovery, a finding that warrants further exploration.
This study has several limitations. First, we did not include detailed data on the perioperative administration of heparin and protamine, two medications known to influence HBP levels.48,50,53-56 Although we recorded the use of other drugs such as corticosteroids, opioids, and electrolytes, their effects on inflammatory markers may vary. Nonetheless, the high degree of standardization in perioperative care likely contributed to reduced variability in biomarker expression. 57 We were also very conservative in drawing conclusions from observed association, considering the pilot nature of the study. For example, we observe some effect of acetaminophen on some markers. We decided ot downplay this association and re-address it in other studies, considering that we may not capture all drug use. Acetaminophen has been shown to suppress neutrophil oxidative burst and extracellular trap formation via antioxidant mechanisms, indicating a modest inhibitory and modulatory effect on innate immune function. This finding should be addressed in a more robust study. Significant variability may be introduced by patients’ pre-existing health status, affecting CRP and inflammation in cardiac surgery settings. 58 Our study was underpowered to detect clinically significant associations with outcomes, largely due to a lower incidence of perioperative complications.38,41,42,51 While our observed reference ranges aligned with previously published data, inconsistencies across studies likely reflect platform-dependent differences in assay performance.38,41,42 Importantly, this study was not designed to establish clinical outcomes but rather to extend the temporal window of biomarker assessment and to compare the perioperative dynamics of both classical and novel inflammatory markers. The relatively low rate of acute complications in our cohort would require a different study design, likely larger and event-enriched, to allow meaningful outcome-based inference. Furthermore, while we observed prolonged alterations in markets such as HBP and SAA, the clinical relevance of these findings remains uncertain. For example, persistent depletion of HBP may theoretically be linked to complications such as prolonged edema, coagulation abnormalities, fibrosis, increased susceptibility to infection, or even neoplastic recurrence.50,59 However, these associations remain speculative, as the causal versus associative role of HBP is not yet defined. We also did not analyze genetic variants of SAA, which may affect individual trajectories. 48 The ability to measure multiple biomarkers simultaneously at the point of care may offer synergistic diagnostic and prognostic insights, especially in complex perioperative settings.10,31 However, a notable technical limitation of this approach was the analytes’ large dynamic range, which occasionally exceeded the measurement capabilities of the point-of-care platform. In such cases, manual sample dilution was required to introduce the risk of values falling outside the device’s optimal detection range.
This study has several notable strengths. It includes a relatively large cohort of patients undergoing elective cardiac surgery, an important factor given the known heterogeneity in individual inflammatory responses. The longitudinal design allowed for intra-individual comparisons over time, incorporating preoperative baseline levels to improve the interpretation of postoperative dynamics. Additionally, the study population was relatively homogenous, and both operative and postoperative care were highly standardized, including consistent use of cardiopulmonary bypass equipment and protocols. 54 This level of standardization reduces confounding and increases the internal validity of the findings. Biomarker measurements were conducted using the commercial platform, which has previously been validated against ELISA-based methods.41,51 The similarity of our results to prior studies supports the reliability and external validity of our dataset.
Importantly, this study contributes several novel insights. Most significantly, the prolonged elevations and late-phase alterations in SAA and HBP suggest that the commonly accepted 30-day “recovery period” after surgery may reflect an administrative rather than a physiological threshold. These findings challenge conventional timelines for postoperative recovery and call for a reevaluation of how long-term inflammation is monitored and interpreted after cardiac surgery. While our study was not powered to assess clinical outcomes, particularly given the low incidence of complications, this does not diminish the potential relevance of the observed biomarker trajectories. Rather, the absence of immediate clinical correlates emphasizes the need for future, larger-scale studies to determine whether prolonged inflammatory responses are simply features of normal recovery or predictors of delayed complications or adverse outcomes.
Conclusion
SAA and HBP follow different perioperative patterns than classical markers like IL-6, CRP, and PCT. Unlike these traditional markers, SAA and HBP remain abnormal for up to three months after surgery. This suggests that full immunological recovery may take longer than 30 days, and highlights the value of SAA and HBP in monitoring extended or subtle inflammation after cardiac surgery.
Supplemental Material
Supplemental Material - Longitudinal Analysis of Heparin-Binding Protein (HBP) and Serum Amyloid a Protein (SAA) Versus Interleukin 6 (IL-6), C-Reactive Protein (CRP), and Procalcitonin (PCT) During Both the Acute Postoperative Period and Recovery at Three Months From Non-emergent Cardiac Surgery
Supplemental Material for Longitudinal Analysis of Heparin-Binding Protein (HBP) and Serum Amyloid a Protein (SAA) Versus Interleukin 6 (IL-6), C-Reactive Protein (CRP), and Procalcitonin (PCT) During Both the Acute Postoperative Period and Recovery at Three Months From Non-emergent Cardiac Surgery by Krzysztof Laudanski, Ahmed Sayed Ahmed, Mohamed A. Mahmoud, Hossam Gad, Benjamin R.E. Harris, Ryan Smith, Dandan Zhu, Abdelhamed Elgazar, Anil Vasishta, Gajic Ognjen, Daniel A. Diedrich, Juan Crestanello in Clinical Medicine Insights: Cardiology
Footnotes
Acknowledgments
KL would like to acknowledge the participation of the nursing staff of HVICU at the Penn Presbyterian Medical Center and several members of the Cardiac Anesthesiology Division at the Department of Anesthesiology and Critical Care who made sample collection possible.
Ethical Considerations
The study was approved by the Institutional Review Board at the University of Pennsylvania (#815686).
Consent to Participate
All participants were provided informed consent during the study.
Author Contributions
Conceptualization, K.L.; methodology, K.L.; validation, K.L.; formal analysis, K.L., A.S.A., M.A.M., H.G., B.H., O.G., J.C., A.V.; investigation, K.L., O.G., J.C.; resources, K.L., O.G., J.C.; writing—original draft preparation, K.L.; writing—review and editing, K.L., A.S.A., M.A.M., D.Z., H.G., B.H., O.G., J.C., A.V., R.S.; visualization, K.L., A.S.A., M.A.M., H.G., D.Z., B.H., O.G., J.C., A.V., R.S.; supervision, K.L.; project administration, K.L.; funding acquisition, K.L.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This grant was funded by the Alzheimer’s Disease Core Center (National Institutes of Health - National Institute on Aging), grant number P30 AG10124 and NIGMS NIH, grant number K23 GM120630, and KL’s own funds.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors upon reasonable request.
Author’s Statement
All authors reviewed the final version of the manuscript and agreed to its publication.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.